
Abstract
Background
Some important hematological indices implement acute phase reactions. They can be used to assess disease activity and therapeutic response in many inflammatory conditions. This work aimed to determine whether different hematological indices can be used to assess disease activity and therapeutic response in patients with ankylosing spondylitis (AS) on biological drugs.
Patients and methods
Ninety-seven AS patients and a similar number of controls were involved in the current study. The Ankylosing Spondylitis Disease Activity Score (ASDAS) was used to assess the disease activity. Different complete blood count parameters and indices were assessed.
Results
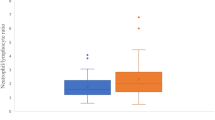
There was a significant difference between the patients and controls as regards mean corpuscular volume, mean corpuscular hemoglobin, red blood cells count, red cell distribution width, mean platelet volume, platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII). Moreover, there was a statistical correlation between ASDAS on one side and hemoglobin (Hb), hematocrit (HTC), lymphocyte count, neutrophil-to-lymphocyte ratio (NLR), PLR, and SII on the other side. When the patient group was divided into 2 subgroups according to ASDAS, with patients with inactive and low disease activity in one subgroup and those with very high and high disease activity in another subgroup, there was a significant difference as regards Hb, HTC, mean corpuscular hemoglobin concentration, NLR, PLR, SII, and also ESR and CRP levels. Moreover, there was a significant correlation between PLR and SII levels on one side and ESR on the other side.
Conclusion
Hematological indices such as PLR, NLR, and SII might be potential markers for follow-up of disease activity and therapeutic response in AS patients treated with biological therapy. This emphasizes the significance of a comprehensive approach for AS patient assessment and follow-up of therapeutic drugs, considering inflammatory markers, hematological indices, and disease activity scores.
Similar content being viewed by others


Background
Ankylosing spondylitis (AS) is a chronic inflammatory illness that has a prevalence rate between 0.1 and 1.4% worldwide [1]. AS typically affects the axial spine and sacroiliac joints, although it can also impact peripheral joints and entheses [2,3,4]. Progressive spine stiffness and persistent back pain are two of the most common clinical signs and symptoms of AS, while there is a wide variety of other manifestations as well. AS can lead to peripheral arthritis, enthesitis, dactylitis, and postural problems that result from reduced spinal movement [5, 6]. Along with skeletal involvement, AS can also present with extra-articular symptoms such as psoriasis (10%), acute anterior uveitis (25–35% of cases), and inflammatory bowel disease (IBD), which affects about 50% of cases [7]. The systemic inflammation caused by AS disease pathophysiology increases the risk of cardiovascular disease. Patients may also encounter pulmonary problems, such as restrictive pulmonary illnesses [8].
Although the pathogenic mechanism of AS is still unclear, several theories regarding the initial process have been suggested. One of them is a direct inference from “self–nonself” immunology that suggests a molecular mimicry between the foreign and self-peptide causing autoinflammation to certain arthritogenic peptides [9]. Other hypotheses propose that AS results from the conformational flexibility of the major risk gene, human leukocyte gene-B27 (HLA-B27). An error-prone folding mechanism in some HLA-B27 alleles might lead to endoplasmic reticulum stress, which in turn triggers the release of cytokines. Altered HLA-B27 molecules can activate the immune system through natural killer cells, killer immunoglobulin-like receptors expressed on CD4 + T cells, and the intrinsic HLA monitoring receptor [10].
To evaluate the activity of AS disease, the SpondyloArthritis international Society (ASAS) membership chose ASDAS with C-reactive protein (CRP) as the best method of assessment and ASDAS with erythrocyte sedimentation rate (ESR) as the alternative form. In addition to the CRP or ESR score, this index also includes four other self-reported items: back pain, peripheral pain or swelling, length of morning stiffness, and patient global assessment of disease activity [11, 12].
Although CRP and ESR levels are commonly used to assess disease activity in many rheumatic conditions, they are insufficient due to their limited specificity and sensitivity [13].
A complete blood count (CBC) is a low-cost, easy, and relatively sensitive clinical indicator of inflammatory response. CBC components, namely platelets, lymphocytes, and neutrophils, are affected by inflammation and immunological responses. These cells are powerful effectors in the inflammatory response. Essential alterations that take place in the peripheral blood in reaction to inflammation include anemia, leukocytosis, and thrombocytopenia [14, 15]. Additionally, the platelet-to-lymphocyte ratio (PLR) and the neutrophil-to-lymphocyte ratio (NLR) are two essential hematological indices that monitor acute phase responses [16,17,18].
Therefore, measuring disease activity in AS is critical not only for a better understanding of the pathophysiology of AS and predicting prognosis but also for monitoring the response to therapeutic drugs. To the best of our knowledge, this is, so far, the first study to investigate the value of hematological markers in a unique group of AS patients treated with biological therapy. This study aimed to determine whether different hematological indices can be used to assess disease activity and therapeutic response in patients with AS on biological drugs.
Patients and methods
Study design
The study design is as follows: observational (cross-sectional) study. A convenient sample of patients was recruited from the outpatient clinic of the rheumatology department.
Study setting and sampling
The study was conducted on 97 AS patients and a similar number of controls. All AS patients were diagnosed according to the Assessment of SpondyloArthritis international Society classification criteria for spondylarthritis [19].
Exclusion criteria
All patients with other inflammatory, autoimmune, infectious diseases, diabetes mellitus, malignancies, pregnancy, liver or kidney diseases were excluded. Newly diagnosed AS patients and those on biologics for less than 3 months were also excluded.
Calculation of sample size
Based on the results of a previous study [20], the mean ± SD of NLR in AS patients was 2.25 ± 0.89, and for the healthy control group, it was 1.72 ± 0.52. To detect the difference between groups with a power of 80%, a level of significance of 5%, and an effect size of 0.67, a total sample size of 72 participants was needed, at ≥ 36 participants for each study group. The sample size was calculated by G*Power (version 3.1.9.2; Germany).
Methodology
All patients were subjected to a full medical history and clinical examination. Disease activity was assessed using ASDAS [11]. Back pain, peripheral pain/swelling, duration of morning stiffness, and patient global assessment were all assessed on a numerical rating scale (from 0 to 10) according to the following formula:
The 3 cut-offs, selected to separate disease activity states, were as follows: < 1.3 between “inactive disease” and “low disease activity” < 2.1 between “low disease activity” and “high disease activity” and > 3.5 between “high disease activity” and “very high disease activity.”
Laboratory investigations
Venous blood was collected from all participants who did not exhibit any clinical symptoms of fever or infection.
A CBC using the Sysmex XT1800i apparatus was done, from which the following data were collected: red blood cell count (RBCs), hemoglobin level (Hb), red cell distribution width (RDW), white blood cell count (WBCs), absolute neutrophil and lymphocyte count, platelet count, and markers of platelet activation (mean platelet volume (MPV) and platelet distribution width (PDW)) [21]. By dividing the absolute count of neutrophils by the absolute count of lymphocytes, NLR was calculated. PLR was also calculated by dividing the absolute platelet count by the absolute lymphocytic count [22]. The systemic immune-inflammation index (SII) was calculated as the product of the platelet and neutrophil counts divided by the lymphocyte count [23, 24]. ESR [25] and CRP [26] were measured immediately.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences SPSS 22.0 software (IBM Microsoft). Quantitative data normality was tested by Kolmogorov’s test. Qualitative variables were presented using numbers and percent; the chi-square test was used for analysis. Numerical variables were expressed as medians (IQR), and the Mann–Whitney U test was used for comparison between groups. Spearman’s correlation analysis was used to evaluate the relation between laboratory parameters and clinical variables. A P-value (< 0.05) was adopted as the level of significance.
Results
Ninety-seven AS patients and a similar number of matched controls were included in the current study. The demographical and clinical characteristics of the study groups are shown in Tables 1 and 2. The median age of the AS patients was 42 years, and the percentage of males in the AS disease group was 86.6% with age- and sex-matched controls. The median disease duration of the patients was 8 years. As regards the extra-articular manifestations of AS, 7 patients had uveitis and 8 patients had colitis. Eighty-four (86.6%) patients were HLA-B27 positive. Fifty-three (54.6%) patients used NSAIDs, while only 3 (3.1%) patients were on steroids. Six patients were on mesalamine, and only one patient used MTX. As regards ASDAS, 8 patients had inactive disease while 20 had VHDA, with nearly equal numbers of LDA and HAD (35, 34, respectively). Thirty-eight patients were on adalimumab, 29 on golimumab, 21 on secukinumab, and 9 patients on etanercept. Table 2 presents the laboratory findings of the studied groups. There was a significant difference between the patients and controls as regards MCV, MCH, RDW, RBCs, MPV, PLR, and SII. Moreover, there was a statistical correlation between ASDAS on one side and Hb, HTC, lymphocyte count, NLR, PLR, and SII on the other side (Table 3). When the patient group was divided into 2 subgroups based on ASDAS, with patients with inactive and LDA in one subgroup and those with HAD and VHDA in another subgroup, there was a significant difference as regards Hb, HTC, MCHC, NLR, PLR, SII, ESR, and CRP levels. Moreover, there was a significant correlation between PLR and SII levels on one side and ESR on the other side (Table 4).
Discussion
The etiopathogenesis of spondyloarthropathy is caused by the interplay of genetic, immunomodulatory, and ethnic factors. There are still many unanswered questions about these complex relationships, one of which is how the severity of the illness is influenced by the peak of the inflammatory state [27, 28]. To evaluate the degree of disease activity and patients’ responses to biological treatment, ESR, CRP, and other disease activity scores have been widely used [29, 30]. Nevertheless, monitoring the course of the AS disease necessitates the development of further novel biomarkers, especially in patients treated with biological drugs. Since different hematological markers can be easily obtained from CBC, these markers seem promising for evaluating disease activity in AS patients, aiming for optimal management. Combined hematological indices of inflammation, particularly NLR, PLR, and SII, are widely used with favorable results in various diseases. Additionally, the prognosis and severity of several inflammatory disorders can be predicted by the CBC parameters and the ratios between them [31, 32].
The demographic data of the patients in this study revealed no significant difference when compared to the healthy control group. This demonstrated that the patients were correctly matched to the control group, and confounding variables that could have influenced the results were avoided.
RDW and MPV represent the degree of heterogeneity in circulating erythrocyte volume and platelet count, which are altered by inflammatory conditions [33]. Many studies have been conducted on the connections between MPV, RDW, platelet count, and other hematological parameters in rheumatic disorders; nevertheless, conflicting results have been reported [34]. In the current work, there was a statistically significant difference between the patients and controls as regard to MCV, MCH, RDW, RBCs, MPV, PLR, and SII, with decreased levels of MPV, PLR, SII, and red blood cell parameters except for RDW, which was increased in the patient group. Anemia is a common manifestation of the chronic inflammation process and has also been observed in individuals with axial SpA. The mechanism behind it is thought to be related to the inhibitory effects of cytokine secretion. TNF-α has the potential to inhibit erythropoietin’s actions on hematopoietic stem and progenitor cells [35]. Since all the recruited patients were on biological treatment, with their marvelous anti-inflammatory effect, for at least 3 months and that nearly 44% of them were either in remission or low disease activity, it was expected that the PLR and SII might be of normal levels. On the other hand, the results of Liang T et al. [36] reported that the levels of PLR were significantly higher in the AS group than in the non-AS group. This discrepancy may be due to patient selection criteria. Melek Sezgin et al. [37] observed that RDW was more significant in AS patients than in controls. The impact of anemia rather than a true inflammatory index might be the reason for the elevated RDW. Consistent with the results of the present study, several studies [38,39,40,41,42] reported no significant difference in NLR between AS patients and healthy controls; however, comparable findings were reported by Bozan et al. [43]. This may be the result of various treatment strategies and methods used to choose AS patients for various research projects.
Moreover, there was a statistical correlation (P < 0.01) between ASDAS on one side and Hb, HTC, lymphocyte count, NLR, PLR, and SII on the other side. Similarly, Liang T. et al. [36] and Sariyildiz A. et al. [20] found a correlation between PLR, activity indices, and disease severity. Additionally, Wu J. et al. [13] and Sariyildiz A. et al. [20] reported a correlation between SII and disease activity.
Regarding NLR, numerous studies [38, 44, 45] have reported a relationship between AS disease activity indices and NLR. Others, such as Al-Osami et al. [46] and Inal et al. [38], observed no correlation. Currently, CBC indices such as NLR and PLR are commonly used as indicators of inflammation. Previous studies have shown that they are associated with a variety of autoimmune disorders [47,48,49]. Additionally, SII can better reflect the body’s balance of inflammation and immunity than NLR or PLR alone because it incorporates the three properties of neutrophils, lymphocytes, and PLTs. This allows SII to represent numerous inflammatory and immunological pathways in the body [50]. Previous researches [51,52,53] have observed a relationship between SII and many other rheumatologic disease activities, such as rheumatoid arthritis, vasculitis, and Behcet disease.
The current study showed that RBCs parameters, NLR, PLR, SII, ESR, and CRP levels were significantly higher in AS patients with higher disease activity. The persistent inflammation that is seen in individuals with high disease activity can help to explain this observation. Similarly, Liang T et al. [36] found a correlation between PLR and NLR on one side and disease activity grading on the other side. Moreover, they observed that PLR was associated with the severity of AS and may be used independently to diagnose AS. Also, Al-Osami et al. [46] found that NLR and PLR were significantly higher in the AS patients with active disease compared to those with inactive disease, even though there was no significant difference in the same parameters between AS patients and healthy controls. Inal et al. [38] and Kucuk et al. [45] also reported the same finding as regards NLR and PLR. Furthermore, Wu J et al. [13] reported that patients with active AS had significantly higher NLR, SII, and PLR levels than those in remission. The increase in SII level may be due to the increase in neutrophils, together with thrombocytosis and lymphopenia caused by an immune-inflammatory response.
Moreover, there was a significant correlation between PLR and SII levels on one side and ESR on the other. This emphasizes the importance of these indices for monitoring the inflammatory process in AS patients, particularly when combined with acute phase reactants such as ESR.
Conclusions
Hematological indices such as PLR, NLR, and SII might be potential markers for follow-up of disease activity and therapeutic response in AS patients treated with biological therapy. This emphasizes the significance of a comprehensive approach for AS patient assessment and follow-up of therapeutic drugs, considering inflammatory markers, hematological indices, and disease activity scores.
Availability of data and materials
Available.
Abbreviations
- AS:
-
Ankylosing spondylitis
- ASDAS:
-
Ankylosing Spondylitis Disease Activity Score
- CBC:
-
Complete blood count
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- LDA:
-
Low disease activity
- HAD:
-
High disease activity
- MPV:
-
Mean platelet volume
- MCV:
-
Mean corpuscular volume
- MCH:
-
Mean corpuscular hemoglobin
- MCHC:
-
Mean corpuscular hemoglobin concentration
- NLR:
-
Neutrophil-to-lymphocyte ratio
- PLR:
-
Platelet-to-lymphocyte ratio
- PDW:
-
Platelet distribution width
- SII:
-
Systemic immune-inflammation index
- VHDA:
-
Very high disease activity
References
Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD et al (2014) Global prevalence of ankylosing spondylitis. Rheumatology 53(4):650–7
Fakhreldin S, Abdallah MM, Al-Tohamy MY, Zayed HS (2020) Bone mineral density in ankylosing spondylitis: relation to disease activity, functional capacity, spinal mobility and radiological damage. Egypt Rheumatol 42(4):297–301
Garcia-Montoya L, Gul H, Emery P(2018). Recent advances in ankylosing spondylitis: understanding the disease and management. F1000Res. 21;7:F1000 Faculty Rev-1512.
Houzou P, Koffi-Tessio VE, Oniankitan S, Sossou K, Fianyo E, Tagbor KC et al (2022) Clinical profile of ankylosing spondylitis patients in Togo. Egypt Rheumatol 44(1):1–4
Mauro D, Thomas R, Guggino G, Lories R, Brown MA, Ciccia F (2021) Ankylosing spondylitis: an autoimmune or autoinflammatory disease? Nat Rev Rheumatol 17(7):387–404
Sieper J, Braun J, Dougados M, Baeten D (2015) Axial spondyloarthritis. Nat Rev Dis Prim 1:15041
Bengtsson K, Forsblad-d’Elia H, Deminger A, Klingberg E, Dehlin M, Exarchou S et al (2021) Incidence of extra-articular manifestations in ankylosing spondylitis, psoriatic arthritis and undifferentiated spondyloarthritis: results from a national register-based cohort study. Rheumatology 60(6):2725–34
Helon K, Wisłowska M, Kanecki K, Goryński P, Nitsch-Osuch A, Bonek K (2024) Time trend analysis of comorbidities in ankylosing spondylitis: a population-based study from 53,142 hospitalizations in Poland. J Clin Med 13(2):602
Galal S, Hassan RM, Labib HSA (2023) Association of vascular endothelial growth factor serum levels with ankylosing spondylitis in Egyptian patients. Egypt Rheumatol Rehabil 50:13
Xiong Y, Cai M, Xu Y, Dong P, Chen H, He W, Zhang J (2022) Joint together: the etiology and pathogenesis of ankylosing spondylitis. Front Immunol 13:996103
Lukas C, Landewe R, Sieper J, Dougados M, Davis J, Braun J et al (2009) Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann Rheum Dis 68(1):18–24
Van der Heijde D, Lie E, Kvien TK, Sieper J, van den Bosch F, Listing J et al (2009) ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann Rheum Dis 68(12):1811–8
Wu J, Yan L, Chai K (2021) Systemic immune-inflammation index is associated with disease activity in patients with ankylosing spondylitis. J Clin Lab Anal 35(9):e23964
Cetinkaya E, Senol K, Saylam B, Tez M (2014) Red cell distribution width to platelet ratio: new and promising prognostic marker in acute pancreatitis. World J Gastroenterol 20(39):14450–4
Siyan X, Xuejie Ch (2019) Red blood cell distribution width-to-platelet ratio as a disease activity-associated factor in systemic lupus erythematosus. Medicine 97(39):e12342
Zhou Z, Chen H, Ju H, Sun M, Jin H (2020) Platelet indices in patients with chronic inflammatory arthritis: a systematic review and meta-analysis. Platelets 31(7):834–44
Khaled SAA, NasrEldin E, Makarem YS, Mahmoud HFF (2020) Value of platelet distribution width and mean platelet volume in disease activity score of rheumatoid arthritis. J Inflamm Res 13:595–606
Olumuyiwa-Akeredolu O, Page MJ, Soma P, Pretorius E (2019) Platelets: emerging facilitators of cellular crosstalk in rheumatoid arthritis. Nat Rev Rheumatol 15(4):237–248
Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos-Vargas R et al (2009) The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis 68(2):1–44
Sariyildiz A, Benlidayi IC, Turk I, Acemoglu SSZ, Unal I (2023) Evaluation of the relationship between blood cell markers and inflammation, disease activity, and general health status in ankylosing spondylitis. Rev Assoc Med Bras (1992) 69(10):e20230722
Gulati GL, Hyland LJ, Kocher W, Schwarting R (2002) Changes in automated complete blood cell count and differential leukocyte count results induced by storage of blood at room temperature. Arch Pathol Lab Med 126(3):336–42
Lee YH (2018) Association between the neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio and rheumatoid arthritis and their correlations with the disease activity: a meta-analysis. J Rheum Dis 25(3):169
Li M, Li Z, Wang Z, Yue C, Hu W, Lu H (2022) Prognostic value of systemic immune-inflammation index in patients with pancreatic cancer: a meta-analysis. Clin Exp Med 22(4):637–46
Hu T, Wang J, Xiao R, Liao X, Liu M, Sun Z (2022) Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: a systematic review and meta-analysis. Front Cardiovasc Med 8(9):933913
Bull BS, Caswell M, Ernst E, Joe JM, Kallner A, Koepke JA et al (1993) ICSH recommendations for measurement of erythrocyte sedimentation-rate. J Clin Pathol 46(3):198–203
Bíró A, Rovó Z, Papp D, Cervenak L, Varga L, Füst G et al (2007) Studies on the interactions between C-reactive protein and complement proteins. Immunology 121(1):40–50
Sharip A, Kunz J (2020) Understanding the pathogenesis of spondyloarthritis. Biomolecules 20(10):1461
Colbert RA, Tran TM, Layh-Schmitt G (2014) HLA-B27 misfolding and ankylosing spondylitis. Mol Immunol 57(1):44–51
Lippi G, Mattiuzzi C, Cervellin G (2016) Learning more and spending less with neglected laboratory parameters: the paradigmatic case of red blood cell distribution width. Acta Biomed 87(3):323–8
Agrawal P, Tote S, Sapkale B (2024) Diagnosis and treatment of ankylosing spondylitis. Cureus 16(1):e52559
Hao X, Li D, Wu D, Zhang N (2017) The relationship between hematological indices and autoimmune rheumatic diseases (ARDs), a meta-analysis. Sci Rep 7(1):10833
Taha SI, Samaan SF, Ibrahim RA, Moustafa NM, El-Sehsah EM, Youssef MK (2022) Can complete blood count picture tell us more about the activity of rheumatological diseases? Clin Med Insights Arthritis Musculoskelet Disord 15(15):11795441221089182
Kisacik B, Tufan A, Kalyoncu U, Karadag O, Akdogan A, Ozturk MA et al (2008) Mean platelet volume (MPV) as an inflammatory marker in ankylosing spondylitis and rheumatoid arthritis. Joint Bone Spine 75(3):291–4
Fatma A, Salwa G, Menna E, Alshymaa F (2023) Impact of biological and non-biological treatment on hematological indices in patients with ankylosing spondylitis and psoriatic arthritis. Egypt Rheumatol Rehabil 50:14
Grigorakaki C, Morceau F, Chateauvieux S, Dicato M, Diederich M (2011) Tumor necrosis factor alpha-mediated inhibition of erythropoiesis involves GATA-1/GATA-2 balance impairment and PU.1 over-expression. Biochem Pharmacol 82(2):156–66
Liang T, Chen J, Xu G, Zhang Z, Xue J, Zeng H et al (2021) Platelet-to-lymphocyte ratio as an independent factor was associated with the severity of ankylosing spondylitis. Front Immunol 5(12):760214
Sezgin M, Tecer D, Kanık A, Kekik FS, Yeşildal E, Akaslan E et al (2017) Serum RDW and MPV in ankylosing spondylitis: can they show the disease activity? Clin Hemorheol Microcirc 65(1):1–10
Ee Inal, Sunar I, Sarataş Ş, Eroğlu P, Inal S, Yener M (2015) May neutrophil- lymphocyte and platelet lymphocyte ratios indicate disease activity in ankylosing spondylitis? Arch Rheumatol 30(2):130–7
Mercan R, Bitik B, Tufan A, Bozbulut UB, Atas N, Ozturk MA et al (2016) The association between neutrophil lymphocyte ratio and disease activity in rheumatoid arthritis and ankylosing spondylitis. J Clin Lab Anal 30(5):597–601
ÖzŞahin M, Demirin H, Uçgun T, Ermis F (2014) Neutrophil-lymphocyte ratio in patients with ankylosing spondylitis. Abant Med J 3(1):16–20
Boyraz I, Koç B, Boyacı A, Tutoğlu A, Sarman H, Ozkan H (2014) Ratio of neutrophil/lymphocyte and platelet/ lymphocyte in patient with ankylosing spondylitis that are treating with anti-TNF. Int J Clin Exp Med 7(9):2912–5
Boyraz I, Onur Caglar S, Erdem F, Yazici M, Yazici S, Koc B et al (2016) Assessment of relation between neutrophil lympocyte, platelet lympocyte ratios and epicardial fat thickness in patients with ankylosing spondylitis. Med Glas (Zenica) 13(1):14–17
Bozan N, Alpaycı M, Aslan M, Cankaya H, Kıroglu AF, Turan M et al (2016) Mean platelet volume, red cell distribution width, platelet-to-lymphocyte and neutrophil-to-lymphocyte ratios in patients with ankylosing spondylitis and their relationships with high-frequency hearing thresholds. Eur Arch Otorhinolaryngol 273(11):3663–72
Coşkun BN, Öksüz MF, Ermurat S, Tufan AN, Oruçoğlu N, Doğan A et al (2014) Neutrophil lymphocyte ratio can be a valuable marker in defining disease activity in patients who have started anti-tumor necrosis factor (TNF) drugs for ankylosing spondylitis. Eur J Rheumatol 1(3):101–5
Kucuk A, Uslu AU, Ugan Y, Bagcaci S, Karahan AY, Akarmut A, Sahin A, Kucuksen S (2015) Neutrophil-to-lymphocyte ratio is involved in the severity of ankylosing spondylitis. Bratisl Lek Listy 116(12):722–5
Al-Osami MH, Awadh NI, Khalid KB, Awadh AI (2020) Neutrophil/lymphocyte and platelet/lymphocyte ratios as potential markers of disease activity in patients with ankylosing spondylitis: a case-control study. Adv Rheumatol 60(1):13
Gao MZ, Huang YL, Wu XD, Xu QW, Ji R, Gu B et al (2018) Red blood cell distribution width and neutrophil to lymphocyte ratio are correlated with disease activity of dermatomyositis and polymyositis. J Clin Lab Anal 32(1):e22209
Pan L, Du J, Li T, Liao H (2017) Platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio associated with disease activity in patients with Takayasu’s arteritis: a case-control study. BMJ Open 7(4):e014451
Wu Y, Chen Y, Yang X, Chen L, Yang Y (2016) Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were associated with disease activity in patients with systemic lupus erythematosus. Int Immunopharmacol 36:94–99
Hu B, Yang XR, Xu Y, Sun YF, Sun C, Guo W et al (2014) Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res 20(23):6212–22
Satis S (2021) New inflammatory marker associated with disease activity in rheumatoid arthritis: the systemic immune-inflammation index. Curr Health Sci J 47(4):553–7
Kim Y, Choi H, Jung SM, Song JJ, Park YB, Lee SW (2019) Systemic immune-inflammation index could estimate the cross-sectional high activity and the poor outcomes in immunosuppressive drug-naïve patients with antineutrophil cytoplasmic antibody-associated vasculitis. Nephrol (Carlton) 24(7):711–7
Tanacan E, Dincer D, Erdogan FG, Gurler A (2021) A cutoff value for the systemic immune-inflammation index in determining activity of Behçet disease. Clin Exp Dermatol 46(2):286–91
Acknowledgements
None.
Funding
This study has no funding sources.
Author information
Authors and Affiliations
Contributions
All authors have contributed to designing the study, collecting and analyzing, interpretation of data, and preparing and revising the manuscript. Design of the study: MA, ZS, AI. Recruitment of patients: MA, AI. Data collection: MA, AI, AE. Randomizing: MA, HA, AI, AE. Assessment: MA, AI. Statistical analysis and data interpretation: HA, AE. Manuscript preparation: MA, HA, AI, AE. Manuscript revision: MA, ZS, AI. All co-authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We confirm none of the present study’s procedures had violated the principles stated by the latest version of declaration of Helsinki. The current study was approved by the local ethical committee at Kafrelsheikh University with the approval code KFSIRB200-160. All patients and controls were recruited to participate and provided detailed information about the study, and those who agreed to be involved in the study were included. We confirm that the manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ibrahim, A.M., El-Nahal, A.S., Ahmed, H.A. et al. Hematological indices: potential markers of disease activity in ankylosing spondylitis patients treated with biological drugs. Egypt J Intern Med 36, 74 (2024). https://doi.org/10.1186/s43162-024-00337-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-024-00337-1