
Abstract
Background
Inflammatory bowel disease is a chronic inflammatory disorder of the gastrointestinal tract and includes ulcerative colitis and Crohn’s disease. Inflammatory bowel disease has always seemed to be rare in the Middle East and Northern Africa. In this study, we explored the clinical characteristics of inflammatory bowel disease patients in our center.
Methods
This retrospective study was conducted on patients with an established diagnosis of inflammatory bowel disease over 10 years from September 2009 to September 2019 who were referred to our inflammatory bowel disease center. Clinical information was obtained from medical records and patient interviews. We included all patients in whom the diagnosis of ulcerative colitis or Crohn’s disease was confirmed by clinical, laboratory, endoscopic, and histological examination over a 10-year period from 2009 to 2019.
Results
Our study had one hundred and sixty-nine inflammatory bowel disease patients; one hundred and thirty-six ulcerative colitis patients and the remaining thirty-three patients had Crohn’s disease. The main presenting symptom was bloody diarrhea (78 patients) representing 46.2% of the patients in our study. The majority of ulcerative colitis patients (55.9%) had moderate disease (Truelove & Witts score), while the majority of Crohn’s disease patients (66.7%) had moderate to severe disease (Crohn’s Disease Activity Index).
Conclusions
The prevalence of inflammatory bowel disease is still low in Egypt despite the rising curve of newly diagnosed cases.
Similar content being viewed by others


Background
Inflammatory bowel disease (IBD) is a chronic inflammatory disorder of the gastrointestinal tract and includes ulcerative colitis (UC) and Crohn’s disease (CD) [1]. They mainly affect young populations, altering their quality of life and increasing morbidity, compared to the general population [2]. The etiology and pathogenesis of IBD are still poorly understood. The pathogenesis of IBD involves genetic factors and environmental factors [1].
IBD was first recognized in European countries during the industrial revolution. The incidence and prevalence of IBD significantly increased in the twentieth century [3]. IBD occurs with different frequencies around the world. The countries reporting the highest incidence of UC are the USA, the UK, and Sweden [4].
IBD has always seemed to be rare in the Middle East and Northern Africa. In Mediterranean countries, the prevalence of UC was estimated at 5/100000 in urban areas [5].
In a recent review of the natural history of IBD, it was noted that as countries become westernized, the incidence of UC increases first followed by CD [6]. Both diseases have emerged in countries in which they had rarely been previously reported, including Japan, South Korea, India, Iran, Lebanon, Thailand, the French West Indies, and North Africa [7]. In these countries, the occurrence of UC preceded that of CD by approximately 10 years. The overall incidence of IBD can be broken down into several geographic zones: those with a high incidence, those with a moderate incidence, those with a low incidence 15 years ago but with a consistently increasing incidence, and those with an unknown incidence [6].
In this study, we studied the sociodemographic and clinical characteristics of patients diagnosed with CD and UC in the Tropical Medicine Department of Ain Shams University Faculty of Medicine.
Methods
As we are lacking the data regarding IBD patients in addition to the absence of solid databases to follow up the patients in Egypt as well as most African countries. This study aimed to identify the sociodemographic and clinical characteristics of IBD patients in our country.
Our department’s gastroenterology center serves patients from all parts of Egypt. We considered patients with chronic diarrhea, bleeding per rectum, recurrent abdominal pain or discomfort, melena, weight loss, and/or perianal fistula or abscess. The diagnosis was established by clinical, laboratory, and radiological findings and endoscopic and histopathological criteria.
This retrospective study was conducted on patients with an established diagnosis of IBD over the 10 years from September 2009 to September 2019 who were referred to our IBD center. The following data were collected at index presentation for assessment: demographical data, occupation and the impact of the disease, criteria of activity, area of residency, symptoms (diarrhea, weight loss, abdominal pain, and blood in the stool), family history of IBD, smoking history, extraintestinal manifestations (EIMs), the use of corticosteroids at the time of presentation, and the subsequent decision of treatment by azathioprine, or monoclonal antibodies against tumor necrosis factor (anti-TNF), or colectomy. Clinical information was obtained from medical records including the patients’ interviews at their index presentation. We included all patients in whom the diagnosis of UC or CD was confirmed by clinical, laboratory, endoscopic, and histological examination over a 10-year period from 2009 to 2019.
As infection is an important cause of deterioration in our patients even being confused with the activity of the disease and also Egypt is in a region endemic for many parasitic infections, so stool analysis was performed for all our patients at index presentation.
CD was diagnosed if there were histopathologic findings suggestive of Crohn’s disease (non-caseating granuloma) in patients with skip lesions; a cobblestone appearance; mucosal ulceration; or aphthous lesions at endoscopy, deep inflammation or chronic terminal ileal inflammation, with or without radiologic evidence of stricturing disease, fistulizing disease, or existence of recurrent perianal disease (abscess, fistula), were also included in the diagnosis. Endoscopic and histopathological examinations were performed by 2 senior experts.
UC was diagnosed when there was evidence of superficial inflammation, crypt abscesses, and cryptitis in diffuse mucosal disease of the colon extending from the rectum to different proximal extensions. For cases of UC, the Truelove classification was used to assess severity, and the Montreal classification was used to assess the extent of the disease.
A diagnosis of IBD was established according to the corresponding criteria. Endoscopic grades were assigned according to the Mayo score as (1) mild activity (erythema, decreased vascular pattern, and mild friability), (2) moderate activity (marked erythema, lack of vascular pattern, friability, and erosions), and (3) severe activity, spontaneous bleeding, and large ulcerations). The histopathological findings included the following: vascular congestion, crypt abscesses, mucin depletion, cellular infiltrate, cryptitis, and crypt branching.
The activity of the disease (whether UC or CD) was determined according to the patient’s condition when first presented to our center (index presentation). The relatively simple Harvey-Bradshaw score [8] (Table 1) and the more complicated Crohn's Disease Activity Index [9] (CDAI) (Table 2) were used to assess the disease activity of CD patients at their index presentation. The CDAI is the sum of 8 components calculated online depending on the evaluation within one previous week of the number of liquid or soft stools, daily abdominal pain, patient well-being, complications, use of antidiarrheal, hematocrit, body weight. The Montreal classification [10] (Table 3) and endoscopic grades assessed the activity as follows: (1) inactive (the vascular pattern is only slightly distorted and there is, fine granularity without friability or epithelial defects); (2) mildly active (there is unequivocal erythema, either focal or confluent, and some friability without epithelial necrosis); (3) moderately active (a few aphthoid erosions or small ulcers are noted); or (4) severe (ulcers are larger and more numerous). The histopathological findings included the following: cellular infiltrate, focal inflammation, microfistulization, non-caseating granulomas, cobblestoning, and lymphoid hyperplasia.
Results
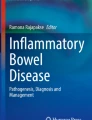
This retrospective study was conducted on patients with an established diagnosis of IBD over 10 years from September 2009 to September 2019 who were referred to our IBD unit at Tropical Medicine Department, Ain Shams University Hospitals. The total number of IBD patients was 169 patients, 136 of them were UC patients (80.5%) and the other 33 patients (19.5%) were diagnosed to have Crohn’s disease. The number of new patients received by our unit each year during the time period of the study is shown in Fig. 1.

The number of new patients per year (2009–2019)
Females were slightly more than males (53.8% vs 46.2%). The age of patients ranged between 9 and 76 years. The basic demographic characteristics of our patients are shown in Table 4 and Fig. 2. The clinical picture of the patients ranged between diarrhea, bleeding, and abdominal pain, with the majority of the patients having no extraintestinal manifestations at index presentation as in Table 5.

The body mass index of the patients at diagnosis
Exploration of the patients’ blood investigations at index presentation showed mostly normal laboratory markers except for anemia and elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) (Table 6). Most of our patients (95.3%) had stool examination free from parasites, with only 4.7% of the patients having Entamoeba histolytica cysts (Fig. 3).

Percentage of the patients with parasites in their stool analysis
Macroscopic and microscopic appearance of the disease (Tables 7 and 8)
All of our patients naturally had undergone colonoscopy at or around the time of presentation with biopsies taken for histopathological examination. As for UC patients, the most frequent endoscopic finding was a loss of vascular pattern (89.7%), while aphthous ulcers were the commonest finding in CD patients (60.6%). Histopathological examination showed that aggregation of polymorph nuclear leucocytes (PMN), cryptitis, infiltration of the lamina propria, and depletion of goblet cells were the most common microscopic findings. Only a minority of patients (4.1%) had dysplasia with no patients showing any evidence of malignancy fortunately.
Ulcerative colitis patients
Our records showed 136 patients with UC; the site of the colon most affected was recto-sigmoid (36.8%), with the main presenting symptom being bloody diarrhea (52.9%) (Table 9). The activity of the disease at index presentation was evaluated by Truelove & Witts criteria and by Mayo score (Figs. 4 and 5).

Degree of severity of ulcerative colitis (Truelove & Witts score) at index presentation

Degree of severity of ulcerative colitis (Mayo score) at index presentation
Crohn’s disease patients
For patients affected by CD, the main site of affection was the ileum (48.5%), and abdominal pain was the most common presentation (42.4%) (Table 10). Crohn’s Disease Activity Index was used to assess the disease activity at index presentation (Fig. 6).

Degree of severity of Crohn’s disease (Crohn’s Disease Activity Index) at index presentation
Discussion
The current study included (169) Egyptian patients similar to another study from Egypt reflecting a relatively small prevalence of the disease, probably due to a lack of awareness of the disease [11]. The number of newly confirmed cases of IBD in our unit during the 10-year period of the study generally shows a rising trend with a sharper rise at the beginning with the cases rising in a less acute manner in later years. The mean age at diagnosis for the patients in this study was 33.5 years with similar results reported in other studies from India, Brazil, and Iran [12,13,14,15].
As for the gender differences in IBD prevalence, our study showed a male to female ratio of 1:1.16, indicating a lack of difference in IBD prevalence between both genders which was similarly reported by Esmat and colleagues [11], regarding UC patients with a higher male predominance in CD patients (2.6:1). Other studies have reported a higher female predominance in both UC & CD [13, 16], while others showed a similar prevalence in both genders [15, 17]. The prevalence of UC was much higher in our study than CD; (4:1.12). This was also reported by Darakhshan and colleagues [18] who found a higher prevalence of UC (6.2:1) and studies in Brazil with a lower incidence of UC (2~1.7:1) [19].
The body mass index (BMI) of the patients in our study was mainly among overweight (46.2%) and average weight (43.8%) groups. Slightly different results were reported by Mentella and colleagues [20] where 49% of the patients had average weight and 25.7% were overweight, which was also stated in other studies [21] that reported a percentage of 20–40% of overweight patients among IBD adult patients. There was no apparent correlation between smoking and IBD in our study as 142 patients (84%) were non-smokers at the time of diagnosis, with the remaining patients being smokers or ex-smokers, which is different from the findings in previous studies showing that smoking was protective against UC [22]. However, it is similar to findings in other studies done in Arabs [11, 23] and Asians [24].
The main presentation in our study was diarrhea & bleeding per rectum in 46.2% of patients followed by bleeding per rectum alone (24.9%) and diarrhea alone (17.8%). This is similar to the study of Esmat and colleagues [11] where rectal bleeding and diarrhea were the main presenting symptoms in UC patients and diarrhea was the main presentation of CD patients. This was also reported in a study from Iran [15] as bloody diarrhea was the main presenting symptom (97.9%) in their cohort though abdominal pain was the second main presentation (71.4%) where it was the main presenting symptom in only 11% of patients in the current study. Their findings were also different from another study in Iran [18] which stated that the main presenting symptoms of their patients were diarrhea, bleeding, and bloody diarrhea. Abdominal pain was also the main presentation in another study [23] which could be explained by the fact that it was done on patients with CD only with no UC patients included, which is in fact similar to the 33 patients with CD in our study whose main presentation was abdominal pain (42.4%).
The laboratory parameters of our patients showed only mild anemia with a mean hemoglobin of 10.9 gm/dl, with the rest of the parameters being mainly normal. This is quite similar to the average level of hemoglobin in the study of Esmat and colleagues [11] which was 11 gm/dl. The median ESR was 30 mm in the 1st hour and that is slightly similar also to the findings in the study of Esmat and colleagues [11], where the mean ESR in the 1st hour was 36 in UC patients and 49.5 in CD patients.
In our study, most of the patients with UC had a disease affecting the rectosigmoid colon (36.8%), while pancolitis and extensive colitis were presented equally, each in 17.2% of the patients. Similar results were reported by Mostafa and colleagues [25], where most of the patients (50%) had proctosigmoiditis. This is quite different from another study in Egypt [11] which reported that 65.2% of patients had left-sided colitis, 18.5% of patients had proctosigmoiditis, and 16.3% had pancolitis.
The presentations of the disease in the current study showed that the most common activity at index presentation in UC patients is the moderate form (55.9%) followed by the severe form according to the Truelove & Witts score. Using the Mayo score in stratification regarding the disease activity in presentation, the severe form had the highest percentage of the included patients (41.9%) which could be related to built-in differences in criteria for evaluation of both scores and could also be due to the fact that we are a tertiary center receiving complicated patients from other hospitals and centers all over the country.
Crohn’s disease group of patients were mainly at moderate to severe form followed by mild form (66.7%) and (33.3%) respectively. This is matched with another Egyptian study that showed 50% of patients presented with the moderate form of the disease [11].
Thirty-two patients were treated by biological therapies. Twenty-two of them were ulcerative colitis (16.17%) patients and the other ten were Crohn’s disease (30.3%) patients. These percentages are comparable to those recorded by a Danish study which stated the use of biologics in 28.5% of CD patients and 11.3% of UC patients [26]. That retrospective study included more than 30 thousand patients during 12 years which may reflect the difference in the prevalence of IBD there and in Egypt. It also shows the relatively late use of biologics in Egypt with the standard treatment for severe cases limited to intravenous steroids, and surgery in non-responding cases.
Infliximab was the most commonly used biologic followed by adalimumab. These choices are of course influenced by financial issues, insurance coverage, and availability.
Surgical intervention in the current study was decided in 20 patients; 8 of them were UC and 12 of them were CD which is more than those reported by Esmat and colleagues [11] that were 11 patients only (4 UC and 7 CD), with a comparable percentage of the total number of patients who needed surgical intervention in UC in relation to CD patients’ total number who needed surgical intervention.
As a matter of fact, the findings from recent reviews on IBD patients in Africa and the Middle East [27,28,29] are quite similar to the findings from our study regarding the percentage of smokers, the percentage of female patients, and the proctosigmoid distribution of UC in the majority of their patients, with only slight differences with some of the studies included in these reviews related to the severity of the disease as most of their studies showed a predominance of mild activity of IBD in contrast to our study where the majority of UC and CD patients were moderate to severe which again could be related to the fact that we are a tertiary center dealing with more complicated cases. It is worth noting that in two of these reviews [27, 29] the information related to Egyptian patients was derived from only one study [11], indicating the need for a population-based IBD registry and multicenter studies to pinpoint the real situation of IBD in Egypt which will be surely reflected upon the public awareness of the disease and national health plans.
Conclusion
The prevalence of inflammatory bowel disease is still low in Egypt despite the rising curve of newly diagnosed cases. Further large-scale multicenter studies are needed to obtain accurate figures regarding the IBD pattern and prevalence in Egypt.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- BMI:
-
Body mass index
- CRP:
-
C-reactive protein
- CD:
-
Crohn’s disease
- CDAI:
-
Crohn’s Disease Activity Index
- ESR:
-
Erythrocyte sedimentation rate
- EIMs:
-
Extraintestinal manifestations
- IBD:
-
Inflammatory bowel disease
- PMN:
-
Polymorph nuclear leucocytes
- TNF:
-
Tumor necrosis factor
- UC:
-
Ulcerative colitis
References
Pierik M, Yang H, Barmada MM, et al. (2005) The IBD international genetics consortium provides further evidence for linkage to IBD4 and shows gene-environment interaction. Inflamm Bowel Dis 11(1): 1-7.
Molodecky NA, Kaplan GG (2010) Environmental risk factors for inflammatory bowel disease. Gastroenterol Hepatol (N Y) 6:339–346
Molodecky NA, Soon S, Rabi DM et al (2012) Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 142(1):46–54
Ehlin AG, Montgomery SM, Ekbom A et al (2003) Prevalence of gastrointestinal diseases in two British national birth cohorts. Gut 52:1117–1121
Tezel A, Dökmeci G, Eskiocak M et al (2003) Epidemiological features of ulcerative colitis in Trakya, Turkey. J Int Med Res 31:141–148
Cosnes J, Gower-Rousseau C, Seksik P et al (2011) Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 140:1785–1794
Sood A, Midha V, Sood N et al (2003) Incidence and prevalence of ulcerative colitis in Punjab, North India. Gut 52:1587–1590
Harvey RF, Bradshaw JM (1980) A simple index of Crohn’s-disease activity. The Lancet 315:514
Best WR, Becktel JM, Singleton JW et al (1976) Development of a Crohn’s Disease Activity Index. National Cooperative Crohn’s Disease Study. Gastroenterology 70:439–444. 1248701
Silverberg MS, Satsangi J, Ahmad T et al (2005) Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol 19(Suppl A):5A–36A
Esmat S, El Nady M, Elfekki M et al (2014) Epidemiological and clinical characteristics of inflammatory bowel diseases in Cairo, Egypt. World J Gastroenterol 20:814
Kedia S, Ahuja V (2017) Epidemiology of inflammatory bowel disease in India: the great shift east. Inflamm Intest Dis 2:102–115
Makharia GK, Ramakrishna BS, Abraham P et al (2012) Survey of inflammatory bowel diseases in India. Indian J Gastroenterol 31(6):299–306
Martins AL, Volpato RA, da Penha Z-GM (2018) The prevalence and phenotype in Brazilian patients with inflammatory bowel disease. BMC Gastroenterol 18:87
Zobeiri M, Bashiri H, Askari L et al (2017) Epidemiologic characteristics of patients with inflammatory bowel disease in Kermanshah, Iran. Middle East J Dig Dis 9(3):164
Ng SC, Zeng Z, Niewiadomski O et al (2016) Early course of inflammatory bowel disease in a population-based inception cohort study from 8 countries in Asia and Australia. Gastroenterology 150(1):86–95
Ng SC, Tang W, Ching JY et al (2013) Incidence and phenotype of inflammatory bowel disease based on results from the Asia-pacific Crohn’s and colitis epidemiology study. Gastroenterology 145(1):158–165
Darakhshan F, Khojeini EV, Balaii H et al (2008) Epidemiology of inflammatory bowel disease in Iran: a review of 803 cases. Gastroenterol Hepatol Bed Bench 1(1):19–24
Quaresma AB, Kaplan GG, Kotze PG (2019) The globalization of inflammatory bowel disease: the incidence and prevalence of inflammatory bowel disease in Brazil. Curr Opin Gastroenterol 35(4):259–264
Mentella MC, Scaldaferri F, Pizzoferrato M et al (2019) The Association of disease activity, BMI and phase angle with vitamin D deficiency in patients with IBD. Nutrients 11(11):2583
Gupta N, DeRoche K, Arroyo-Mercado F et al (2019) 2929 Correlation of body mass index (BMI) and C-reactive protein (CRP) with inflammatory bowel disease progression in an urban, Afro-Caribbean population. Am J Gastroenterol 114:S1596–S1597
Lakatos PL, Vegh Z, Lovasz BD et al (2013) Is current smoking still an important environmental factor in inflammatory bowel diseases? Results from a population-based incident cohort. Inflamm Bowel Dis 19(5):1010–1017
Siddique I, Alazmi W, Al-Ali J et al (2012) Clinical epidemiology of Crohn’s disease in Arabs based on the Montreal classification. Inflamm Bowel Dis 18(9):1689–1697
Ray G (2016) Inflammatory bowel disease in India-past, present and future. World J Gastroenterol 22(36):8123
Mostafa EF, Metwally A, Hussein SA (2018) Inflammatory bowel diseases prevalence in patients underwent colonoscopy in Zagazig University Hospitals. Afro-Egyptian J Infect Endemic Dis 8(2):81–87
Alulis S, Vadstrup K, Borsi A et al (2020) Treatment patterns for biologics in ulcerative colitis and Crohn’s disease: a Danish Nationwide Register Study from 2003 to 2015. Scand J Gastroenterol 55(3):265–271
Mosli M, Alawadhi S, Hasan F et al (2021) Incidence, prevalence, and clinical epidemiology of inflammatory bowel disease in the Arab World: a systematic review and meta-analysis. Inflammatory Intestinal Diseases 6:123–131
Rajbhandari R, Blakemore S, Gupta N et al (2020) Crohn’s disease in low and lower-middle income countries: a scoping review. World J Gastroenterol 26(43):6891
Sharara AI, Al Awadhi S, Alharbi O et al (2018) Epidemiology, disease burden, and treatment challenges of ulcerative colitis in Africa and the Middle East. Expert Review Gastroenterol Hepatol 12(9):883–897
Acknowledgements
Assistant lecturers and residents of Inflammatory bowel diseases unit, Tropical Medicine Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the Declaration of Helsinki 1975, as revised in 2000 and in accordance with the Faculty of Medicine, Ain shams University ethical committee standards.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shamkh, M.A.A., Sakr, M.A., Abd Alaty, W.H. et al. A decade of inflammatory bowel disease: a single center experience in Egypt. Egypt J Intern Med 34, 22 (2022). https://doi.org/10.1186/s43162-022-00115-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-022-00115-x