
Abstract
Background
Renal tubulointerstitial fibrosis is a structural marker and prominent pathological characteristic of chronic progressive kidney disease, fibroblast growth factor-2 (FGF2) is a key fibrogenic cytokine that is likely to be involved in the pathogenesis of renal fibrosis, kidney injury molecule-1 (KIM-1) is one of the most promising, early biomarkers of renal disease, either acute or chronic, due to its translatability between preclinical and clinical trials. It is believed that this molecule participates in the process of both kidney injury and healing.
Methods
We prospectively enrolled a cohort study of eighty adult patients who had glomerular diseases (with glomerular filtration rate (GFR) > 30 ml/min/m2); serum level of FGF-2 and KIM-1 was measured at the same time of renal biopsy and was correlated with the degree of interstitial renal fibrosis.
Results
We found a significant positive correlation between FGF-2 and KIM-1 and the degree of interstitial renal fibrosis, albumin, and creatinine (P≤ 0.001), and a negative significant correlation with GFR and proteinuria. there is a positive significant correlation between serum KIM-1 and FGF-2 and hypertension with a significant P value (<0.001) that serum KIM-1 has sensitivity 90% and specificity of 95% and serum FGF-2 has sensitivity 95% and specificity 95% for detection of interstitial renal fibrosis.
Conclusions
Serum FGF-2 and KIM-1 seem to be a non-invasive novel biomarker of interstitial renal fibrosis in glomerulonephritis patients. It may become a useful biomarker without the need for the invasive maneuver of the renal biopsy. FGF-2 and KIM-1 are expected to be therapeutic targets for kidney injury.
Similar content being viewed by others

Background
Renal tubulointerstitial fibrosis is a structural marker and prominent pathological characteristic of chronic progressive kidney disease, and the degree of tubulointerstitial scarring is an excellent prognostic marker for end-stage renal disease [1].
Deposition of extracellular matrix components and interstitial fibroblast accumulation are two main features of tubulointerstitial fibrosis [2]. Numerous studies have provided experimental evidence that tubuloepithelial cell plasticity and interstitial fibroblast proliferation contribute to the accumulation of interstitial fibroblasts in the renal parenchyma [3].
A key role in tubulointerstitial fibrosis is the tubular epithelial-to-mesenchymal transition (EMT), or transdifferentiation of tubular epithelial cells into myofibroblasts, which are the cells responsible for the secretion and accumulation of extracellular matrix components [4].
Fibroblast growth factor-2 (FGF2) is a key fibrogenic cytokine that is likely to be involved in the pathogenesis of renal fibrosis. FGF2 displays a potent capacity to induce tubuloepithelial cell plasticity and promote renal fibroblasts proliferation, and its expression is significantly increased in human kidney disease with marked fibrosis [1].
FGF-2 protein was isolated from the kidney in 1985. Floege et al. reported FGF2 immunostaining in Bowman’s capsule, the glomerular, mesangium, blood vessels, and the interstitium, as well as some tubules in rats, FGF-2 was synthesized by mesangial cells in vitro and in vivo [5].
Kidney injury molecule-1 (KIM-1) protein is a membrane receptor for human hepatitis A virus (HHAV) and T cell immunoglobulin and mucin domain containing 4 (TIMD 4). KIM-1 is one of the most promising, early biomarkers of renal disease, either acute or chronic, due to its translatability between preclinical and clinical trials. It is believed that this molecule participates in the process of both kidney injury and healing, although the precise mechanism of restoration of tubular integrity after injury still remains unclear [6].
It has been proposed that there may be a novel role for chronic KIM-1 expression in the pathogenesis of renal fibrosis through activation of the innate immune system and leukocyte recruitment. Humphreys et al. suggested that persistent KIM-1 expression is a maladaptive process through chronic uptake of cell toxic components from the tubular lumen, promoting chronic inflammation and ultimately renal fibrosis, making KIM-1 a potential novel therapeutic target in fibrosis in general diseases [7].
The aim of our study is to evaluate the significance of serum FGF2 and KIM-1 to detect the degree of histopathological interstitial renal fibrosis in glomerulonephritis patients; in a trial to use serum FGF-2 and KIM-1 level as a non-invasive marker of interstitial renal fibrosis to avoid renal biopsy and its possible subsequent complications.
Methods
We prospectively enrolled a cohort study of eighty adult patients who had glomerular diseases (with glomerular filtration rate> 30 ml/min/m2) at Kasr Alainy Hospital (Cairo, Egypt). The study population was chosen for which blood samples and renal biopsy were collected; this was performed between April 2019 and September 2020. Exclusion criteria included patients less than 18 years or more than 60 years, chronic infections other than viral ones, malignancy, acute kidney injury, obstructive nephropathy, diabetis, chronic kidney disease (GFR <30ml/min/m2), and end-stage renal disease patients (ESRD). All patients gave their written informed consent.
Biochemical and biomarkers’ measurements
Blood samples for complete blood picture, serum level of total calcium and phosphorous, serum albumin, Na, K, serum urea, creatinine, fasting blood sugar. Immune profile (ANA, ADNA, C3, and C4), virology (HCV Ab, HBsAg, and HIVAb), urine analysis, and 24-h urinary protein were done. Serum FGF-2 and KIM-1 level were measured with ELISA test for quantitative detection; at the same time, renal biopsies were obtained. The serum samples for FGF-2 and KIM-1were allowed clotting in a serum separator tube (about 4 h) at room temperature. Centrifuged at approximately 1000×g for 15 min, and were stored at −20°C. Serum FGF-2 was assayed using ELISA kit (Bioassay technology lab) cat no: E10055Hu.CHINA and serum KIM-1 was assayed using ELISA kit (Bioassay technology lab) cat no: E10099Hu.CHIN. Estimated glomerular filtration rate was calculated with a shortened version of the modification of diet in renal disease (MDRD: (GFR (ml/min/1.73 m2) = 186 × Scr (mg/dl)–1.154 × Age–0.203 × 0.742 (if female) × 1.210 (if black)), we classify the GFR in to 3 stages according to KDIGO guidelines (stage 1 GFR ≥90 ml/min/1.73 m2, stage 2 GFR 60–89 ml/min/1.73 m2, stage 3a 45–59 ml/min/1.73 m2, stage 3b 30–44 ml/min/1.73 m2.
Renal biopsies (tru cut needle)
Two cores were obtained under ultrasound guidance, using an 18G semi-automatic biopsy gun with pre and post-procedure precautions.
Material preparation
One core was formalin-fixed, processed in alcohol, cleared in xylene, and incubated in paraffin blocks. Three sets of slides were prepared from serial cuts (3 μ thick); stained with hematoxylin/eosin, Masson’s trichrome, and periodic acid–Schiff.
The other core was frozen sectioned then treated with polyclonal Rabbit antibodies against anti-Human (IgA, IgM, IgG, C3, and C1q) using immunofluorescence technique.
Histopathological examination
All slides were examined under light microscope by two pathologists who were blinded about the results of the serum FGF-2 and KIM-1 level to evaluate the presence of the following: (a) interstitial fibrosis/tubular atrophy, (b) glomerular sclerosis, and (c) chronic arteriopathy viz. arterial intimal fibrosis.
The extent of interstitial fibrosis/tubular atrophy was evaluated according to Banff code score [% of cortex with fibrosis: mild: 6–25%, moderate: 26–50% and sever : > 50%] [5].
Outcome measures
The primary outcome is to detect the significance of serum FGF-2 and KIM-1 as a biomarker of interstitial renal fibrosis in glomerulonephritis patient, and the second outcome is to detect the relation between both FGF-2 and KIM-1 with other parameters such as creatinine, GFR, albumin, proteinuria, and between FGF-2 and KIM 1.
Statistical methods
Data were coded and entered using the statistical package SPSS (Statistical Package for the Social Sciences) version 24. Data was summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Mann-Whitney test [6]. Correlations between quantitative variables were done using the Spearman correlation coefficient [6]. P values less than 0.05 were considered as statistically significant.
Results
Out of 80 CKD patients included, males were 41 (51.2%), females were 39 (48.8%), 42 patients are hypertensive (52.2%), 5% are HBs Ag positive, 7.5% are HCV Ab positive, all are HIV negative, ANA is positive in 33.8% of the patients, anti-DNA positive in 33.8% of the patients, while C3 is consumed in 38.8% of the patients and C4 is consumed in 31.2% of the patients (Table 1).
The degree of interstitial renal fibrosis was normal in 25%, mild in 15%, moderate in 28.7, and severe in 27.5% according to histopathological classification (Table 1).
The GFR was measured by MDRD: according to exclusion criteria we have 22 patients in stage 1 (27.5%), 14 patients in stage2 (17.5%), 17 patients in stage 3A (21.3%), and 27 patients in stage 3B (33.8%) (Tables 1, 2, 3, 4, 5 and 6).
Eighty non-diabetic patients with glomerulonephritis indicated for renal biopsy with mean age 29.7, creat 1.5 mg/ml, urea 58.4 mg/ml, FBS 93.87 mg/dl, serum Na 134.9 mg/dl, serum K 4.45 mg/dl, seum albumin 2.48 g, proteinuria 3.95 g/24 h, serum Ca 8.01 mg/dl, serum phosphorous 4.49 mg/dl, GFR 65.49 min/ml/h, the mean degree of fibrosis is 18%, the mean KIM-1 is 39.95 pg/ml, and FGF-2 is 47.9ng/ml (Table 3).
Our study show a positive correlation between serum KIM-1 with FGF-2, degree of fibrosis, albumin, and serum creatinine with a significant P value (<0.001), it also shows a negative correlation between serum KIM-1 with GFR and Proteinuria with a significant P value (<0.001) (Figs. 1, 2, 3, 4, 5, and 6).

Correlation between serum KIM-1 and FGF-2

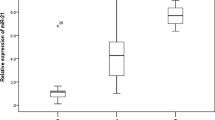
Correlation between serum KIM-1 and degree of fibrosis

Correlation between serum KIM-1 and GFR

Correlation between serum KIM-1 and proteinuria

Correlation between serum KIM-1 and serum albumin

Correlation between serum KIM-1 and serum creatinine
Our study shows a positive correlation between serum FGF-2 and degree of fibrosis, albumin, and serum creatinine with a significant P value (<0.001), it also shows a negative correlation between serum FGF-2 with GFR and proteinuria with a significant P value (<0.001) (Figs. 7, 8, 9, 10, and 11; Table 4).

Correlation between FGF-2 and degree of fibrosis

Correlation between FGF-2 and GFR

Correlation between FGF-2 and proteinuria

Correlation between FGF-2 and serum albumin

Correlation between FGF-2 and serum creatinin
In our study, there is a positive significant correlation between serum KIM-1 and FGF-2 and hypertension with significant P value (<0.001) (Figs. 12, 13, 14, 15 and 16; Table 5).

Correlation between serum KIM-1 and stages of GFR as it shows a positive correlation with stages of GFR with significant P value

Correlation between serum KIM-1 and stages of GFR as it shows a positive correlation with stages of GFR with significant P value

Receiver operating characteristic curves (ROC) curve for detection of interstitial renal fibrosis: ROC curve show sensitivity and specificity of FGF-2 and KIM-1 for detection of interstitial renal fibrosis

Receiver operating characteristic curves( ROC) curve for detection of advanced renal injury stage 3. It shows ROC curve show sensitivity and specificity of FGF-2 and KIM-1 for detection of advanced stage 3 renal injury

a Marked interstitial fibrosis in chronic interstitial nephritis Masson trichome stain −×100. b Moderate interstitial fibrosis in a case of membranous nephropathy with secondary FSGS, JMS stain −×100. c Focal mild interstitial fibrosis in case of active MPGN with crescents, PAS stain −×100
Our study shows that serum KIM-1 has sensitivity of 90% and specificity of 95% with a significant P value (<0.001) for detection of interstitial renal fibrosis and also serum FGF-2 has a sensitivity of 95% and specificity of 95% with a significant P value (<0.001) for detection of interstitial renal fibrosis (Fig. 14; Table 6)
Our study shows that serum KIM-1 has a sensitivity of 95.5% and specificity of 97.2% with a significant P value (<0.001) for detection of advanced stage 3 renal injury and also serum FGF-2 has a sensitivity of 90.9% and specificity of 97.2% with significant P value (<0.001) for detection of advanced stage 3 renal injury (Figs. 15 and 16).
Discussion
Chronic progressive renal disease is accompanied by changes in the tubule-interstitium irrespective of the primary renal disease. The irreversible loss of kidney function prevents the body from eliminating the waste and need for dialysis or organ transplantation [1].
Regardless of etiology, tubulointerstitial changes consist of interstitial inflammation followed by fibrosis, tubular atrophy, and dilation, so the mechanism responsible for chronic renal failure is tubulointerstitial fibrosis, which is the process of progressive scarring of the interstitial space caused by myofibroblasts [8].
A mechanism that contributes to the increase of myofibroblasts in the interstitium during renal fibrosis is the epithelial–mesenchymal transition of proximal tubular cells. These cells lose their identity as epithelial cells and differentiate into myofibroblasts by pro-fibrotic stimuli as FGF-2 [9].
Kidney injury molecule-1 is an epithelial cell adhesion molecule that is induced in damaged tubular epithelial cells undergoing dedifferentiation and proliferation, and the role of KIM-1 as a biomarker, we can hypothesize that KIM-1 may play a protective role in the initial stage of kidney injury, and in the later stage, it may play a damaging role due to the excessive cell proliferation caused by the KIM-1–induced renal repair [10].
In our study, we evaluate the significance of serum FGF-2 and KIM-1 levels to detect the degree of interstitial renal fibrosis in 80 Egyptian patients with glomerulonephritis ( GFR > 30 ml/min/h).
In our study, we found a positive correlation between Kim-1 and degree of renal fibrosis with a significant P value (<0.001). This result agreed with Van Timmeren MM. et al. [11] which concluded that expression of KIM-1 is associated with renal fibrosis and inflammation. The elevation of KIM-1 was confirmed in kidney biopsy tissue collected from patients with kidney disease. KIM-1 was expressed at the luminal side of dedifferentiated proximal tubules in areas of fibrosis and inflammation and correlated positively with kidney damage and negatively with renal function.
Also, Humphreys et al. created a genetic model in mice, demonstrated that chronic KIM-1 expression led to inflammation, tubule interstitial fibrosis, characterized by elevated monocyte chemotactic protein-1 (MCP-1) levels, and increased MCP-1-dependent macrophage chemotaxis. He found that KIM-1-positive tubule interstitium contained abundant interstitial smooth muscle actin-positive myofibroblasts. Activation and proliferation of fibroblasts and myofibroblasts result in the excessive synthesis of extracellular matrix, eventually leading to fibrosis [7].
Benjamin et al. [12] hypothesized that KIM-1 might regulate kidney inflammation and fibrosis when its expression is prolonged because (a) it is upregulated very early after kidney injury and is thus poised to serve as a sentinel of damage; (b) it is expressed in chronic fibrosing kidney disease, where it colocalizes with areas of fibrosis and inflammation .
Nogare AL. et al. found that KIM-1 protein expression was increased in biopsies with interstitial fibrosis and tubular atrophy (IF/TA) compared with biopsies showing acute calcineurin inhibitor nephrotoxicity (CIN) (p <0.05) in renal transplant patients. Significant correlations were found between KIM-1 protein and mRNA levels in tissue and IF/TA, which shows its potential as a biomarker of injuries that can trigger graft fibrosis [13].
In our study, we found a positive significant correlation between KIM-1 and GFR and serum creatinine, this was agreed with Venkata S. et al. [14] that concluded that Blood KIM-1 levels were also elevated in patients with CKD of various etiologies. In a cohort of patients with type 1 diabetes and proteinuria, serum KIM-1 level at baseline strongly predicted rate of eGFR loss and risk of ESRD during 5–15 years of follow-up.
In our study, we found positive significant correlation between FGF-2 and degree of interstitial renal fibrosis, this was agreed with lui et al, 2010 whoconcluded that Fibroblast growth factor-2 (FGF2) is a key fibrogenic cytokine that is likely to be involved in the pathogenesis of renal fibrosis. FGF2 displays a potent capacity to induce tubulo-epithelial cell plasticity and promote renal fibroblasts proliferation, and its expression is significantly increased in human kidney disease with marked fibrosis (3).
Zhuo Xu and Chunsun Dai [15] demonstrated in this study that FGF/FGFR2 signaling in fibroblasts plays an important role in promoting fibroblast proliferation and activation, which aggravates renal interstitial fibrosis.
Also, Frank et al. [16] have demonstrated that FGF-2 is expressed in interstitial fibroblast-like cells and that it is robustly upregulated within these and tubular epithelial cells in human kidney fibrosis. However, FGF-2 does not seem to play a role in interstitial matrix production may have a critical role in fibroblast proliferation and myofibroblast formation.
Valentina et al. [17] report that fibroblast growth factor-2 (FGF-2) is an important trigger of epithelial-mesenchymal transition (EMT). It reduces the expression of cytokeratin and E-cadherin in the proximal tubular epithelium, so it induces epithelial-mesenchymal transition (EMT) of proximal tubular epithelial cells (PTECs) into myofibroblasts lead to end-stage renal disease.
In our study, we found a significant correlation between serum KIM-1 and FGF-2 and incidence of hypertension with a significant P value (<0.001), this finding is consistent with Alfonso et al,2012 who report that urinary KIM-1 and NGAL was elevated in a patient with chronic renovascular hypertension and systemic hypertension [18]. And also, Milica Bozic et al. [19] report that FGF-2 levels are associated with atherosclerosis progression in CKD. This effect is independent of other parameters known, such as age, the degree of renal function, the levels of cholesterol, and smoking status. Therefore, FGF-2 could be considered as a marker and potential target in atherosclerosis progression leading to increased incidence of cardiovascular disease as hypertension.
While our results showed a direct relation between serum KIM-1 and creatinine (p< 0.001)(r=0.776), Peter Egli et al. [20] concluded that among young and healthy adults, plasma levels of KIM-1 were independently associated with systolic and diastolic BP and KIM-1 was not associated with renal function, suggesting that KIM-1 may increase only after prolonged injury leading to substantial kidney damage.
In our study, we found a negative significant correlation between serum FGF-2 and KIM-1 and GFR, as serum FGF-2 and KIM-1 was increased gradually with the decline of GFR and increase in stages 3B other than any stage, Our study shows that serum KIM-1 has sensitivity 90% and specificity 95% with a significant P value (<0.001) for detection of interstitial renal fibrosis and also serum FGF-2 has sensitivity 95% and specificity 95% with significant P value (<0.001) for detection of interstitial renal fibrosis.
Our study shows that serum KIM-1 has a sensitivity of 95.5% and specificity of 97.2% with a significant P value (<0.001) for detection of advanced stage 3 renal injury and also serum FGF-2 has a sensitivity of 90.9% and specificity of 97.2% with significant P value ( <0.001) for detection of advanced stage 3 renal injury.
Conclusions
In our study, we evaluated the performance of serum levels of FGF-2 and KIM-1 as a novel biomarker for the assessment of interstitial renal fibrosis in glomerulonephritis. The AUC-ROC value for serum FGF-2 was AUC=0.98 P<0.0001 with a sensitivity of 95% and specificity of 95% for detection degree of fibrosis. The AUC-ROC value for serum KIM-1 was AUC=0.949 P<0.0001 with a sensitivity of 90% and specificity of 95% for detection of the degree of fibrosis.
We therefore propose that serum FGF-2 and KIM-1 levels may be considered as a good marker to assess the degree of interstitial renal fibrosis without proceeding with subcutaneous renal biopsy.
Currently, the pathological diagnosis is the gold standard for the evaluation of the kidney. However, it is highly recognized that there is a need for the development of accurate non-invasive biomarkers to uncover, prognosticate and guide therapy without the need for invasive and risky methods.
Limitations of this study included:
-
1.
The relatively small number of patients studied that may decrease the statistical power and reproducibility of results.
-
2.
Lack of follow-up of patients to determine the disease progression and measure the serum FGF-2 and KIM-1 level afterwards.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CIN:
-
Calcineurin inhibitor nephrotoxicity
- EMT:
-
Epithelial-to-mesenchymal transition
- ESRD:
-
End-stage renal disease patients
- FGF-2:
-
Fibroblast growth factor-2
- FSGS:
-
Focal segmental glomerular sclerosis
- GFR:
-
Glomerular filtration rate
- HHVD:
-
Human hepatitis A virus
- IF/TA:
-
Interstitial fibrosis and tubular atrophy
- KIM-1:
-
Kidney injury molecule-1
- MCD:
-
Minimal change disease
- MDRD:
-
Modification of diet in renal disease
- PTECs:
-
Proximal tubular epithelial cells
- TIMD4:
-
T cell immunoglobulin and mucin domain containing 4
References
Guan X, Nie L, He T, Yang K, Xiao T, Wang S, Huang Y, Zhang J, Wang J, Sharma K, Liu Y, Zhao J (2014) Klotho suppresses renal tubulo-interstitial fibrosis by controlling basic fibroblast growth factor-2 signalling. J Pathol 234:560–572
Yang J, Liu Y (2001) Dissection of key events in tubular epithelial to myofibroblast transition and its implications in renal interstitial fibrosis. Am J Pathol 159:1465–1475
Liu Y (2010) Newinsights into epithelial–mesenchymal transition in kidneyfibrosis. J Am Soc Nephrol 21:212–222
Piera-Velazquez S, Li Z, Jimenez SA (2011) Role of endothelial-mesenchymal transition (EndoMT) in the pathogenesis of fibrotic disorders. Am. J. Pathol. 179(3):1074–1080
Floege J, Eng E, Lindner V, Young BA, Reidy MA, Johnson RJ (1992) Rat glomerular mesangial cells synthesize basic fibroblast growth factor: Release, upregulated synthesis, and mitogenecity in mesan gial proliferative glomerulonephritis. J Clin Invest 90:2362–2369
Nogare AL, Veronese FV, Carpio VN, Montenegro RM, Pedroso JA, Pegas KL, Gonçalves LF, Ceratti R (2015) Kidney injury molecule-1 expression in human kidney transplants with interstitial fibrosis and tubular atrophy. BMC Nephrology 16:19. https://doi.org/10.1186/s12882-015-0011-y
Humphreys BD, Xu F, Sabbisetti V, Grgic I, Naini SM, Wang N (2013) Chronic epithelial kidney injury molecule-1 expression causes murine kidney fibrosis. J Clin Invest 123:4023–4035
Hewitson TD (Jun 2009) Renal tubulointerstitial fibrosis: common but never simple. Am. J. Physiol. Renal Physiol. 296(6):F1239–F1244
Piera-Velazquez S, Li Z, Jimenez SA (2011) Role of endothelial-mesenchymal transition (EndoMT) in the pathogenesis of fibrotic disorders. Am. J. Pathol 179(3):1074–1080
Han WK, Bailly V, Abichandani R, Thadhani R, Bonventre JV (2002) Kidney Injury Molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 62:237–244
Van Timmeren MM., Van den Heuvel MC. And Bailly V. 2007. Tubular kidney injury molecule-1 (KIM-1) in human renal disease. J Pathol. 212:209-217
Benjamin D. Humphreys, Fengfeng Xu, Venkata Sabbisetti, Ivica Grgic, Said Movahedi Naini, Ningning Wang, Guochun Chen, Sheng Xiao, Dhruti Patel, Joel M. Henderson, Takaharu Ichimura, Shan Mou, Savuth Soeung, Andrew P. McMahon, Vijay K. Kuchroo, Joseph V. Bonventre (2013) Chronic epithelial kidney injury molecule-1expression causes murine kidney fibrosis J Clin Invest. 123(9):4023–4035. doi:https://doi.org/10.1172/JCI45361
Nogare AL, Veronese FV, Carpio VN, Montenegro RM, Pedroso JA, Pegas KL, Gonçalves LF, Manfro RC (2015) Kidney injury molecule-1 expression in human kidney transplants with interstitial fibrosis and tubular atrophy. BMC Nephrol 16:19
Sabbisetti VS, Waikar SS, Antoine DJ, Smiles A, Wang C, Ravisankar A, Ito K, Sharma S, Ramadesikan S, Lee M, Briskin R, De Jager PL, Ngo TT, Radlinski M, Dear JW, Park KB, Betensky R, Krolewski AS, Bonventre JV (2014) Blood Kidney Injury Molecule-1 Is a Biomarker of Acute and Chronic Kidney Injury and Predicts Progression to ESRD in Type I Diabetes. J Am SocNephrol. 25(10):2177–2186
Xu Z, Dai C (2017) Ablation of FGFR2 in FibroblastsAmeliorates Kidney Fibrosis after Ischemia/Reperfusion Injury in Mice. Kidney Dis 3:160–170
Strutz F, Zeisberg M, Hemmerlein B, Sattler B, Hummel K, Becker V, Muller G (2000) Basic fibroblast growth factor expression is increased in human renal fibrogenesis and may mediate autocrinefibroblast proliferation. Kidney International 57:1521–1538
Masola V, Zaza G, Secchi MF, Gambaro G, Lupo A, Onisto M (2014) Heparanase is a key player in renal fibrosis by regulating TGF-βexpression and activity. Biochimica et Biophysica Acta 1843:2122–2128
Eirin A, Gloviczki ML, Tang H, Rule AD, Woollard JR, Lerman A, Textor SC, Lerman LO (2012) Chronic renovascular hypertension is associated with elevated levels of neutrophil gelatinase-associated lipocalin. Nephrol Dial Transplant 27:4153–4161
Bozic M, Betriu A, Bermudez-Lopez M, Ortiz A, Fernandez E, Valdivielso JM (2018) Association of FGF-2 Concentrations with Atheroma Progression in Chronic Kidney Disease Patients. Clin J Am Soc Nephrol 13:577–584
-Peter Egli, Stefanie Aeschbacher, Matthias Bossard, Lucien Eggimann, Laura Bargetzi, Joel Estis, John Todd, Martin Risch, Lorenz Risch and David Conen. (2016). Relationship of kidney injury molecule-1 with estimated glomerular filtration rate and blood pressure in the general population. American Heart Association – Scientific Sessions. New Orleansincluded in the study.”
Funding
No funding
Author information
Authors and Affiliations
Contributions
Dr. Amr Mohamed shaker is the corresponding author, who create the idea of the research and design the work and also write the manuscript, he took the renal biopsy from the patient after taking consent. Dr. Nehal Kamal Rakha who collected and analyzed the data. Dr. Amal Mohamed Rashad and Dr. Tarek Ramzy who are responsible for the result and analysis of the lab work. DR. Wael Mostafa Hamza who is responsible for reading the renal biopsy and interpreting the data of biopsy. Dr. Mohamed Mostafa ElKhatib who designed the idea and supervise and revise all the analysis and interpretation of the data. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee at which the studies were conducted (no number only acceptance) (date of acceptance Novomber 2017). Informed consent was obtained from all individual participants included in the study.
Consent for publication
Patients signed informed consent regarding publishing their data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shaker, A.M., Rakha, N.K., El-Shehaby, A.M.R. et al. The significance of fibroblast growth factor-2 and kidney injury molecule-1 as biomarker of interstitial renal fibrosis in glomerulonephritis. Egypt J Intern Med 34, 28 (2022). https://doi.org/10.1186/s43162-022-00112-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-022-00112-0