
Abstract
Background
Patients with renal failure suffer from fluid overload which is a risk factor for mortality and morbidity. Therefore, fluid status assessment in patients on regular hemodialysis is very important. Dry weight assessment by clinical parameters is not always reliable. We evaluate the role of inferior vena cava ultrasound in estimating fluid overload in regular hemodialysis patients.
Results
A total of 45 persons, 30 end-stage renal disease patients on regular hemodialysis in group A (18 men and 12 women) and 15 healthy persons in group B (10 men and 5 women), were included in the study. The patients in group A ages ranged from 29 to 70 years with a mean of 48.38 ± 12.70 years and in group B ages ranged from 25 to 55 years with a mean of 34.93 ± 8.26. By clinical methods, the mean dry weight was 68.37 kg (68.37 ± 10.42). After HD mean, IVCe decreased from 2.01 ± 0.29 to 1.79 ± 0.22 cm (P < 0.001) similarly, mean IVCi decreased from 0.99 ± 0.48 to 0.64 ± 0.39 cm (P < 0.001). Changes in IVCD were significantly correlated with alterations in body weight following dialysis (P < 0.001). The IVC-CI increased significantly after dialysis (P < 0.001). IVCD and its IVC-CI reflected alterations in fluid status (P < 0.001). Considering the clinical parameters of fluid status, following HD mean, heart rate increased from 81.80 ± 5.15 beats per minute to 89.87 ± 6.42, (P < 0.001), systolic blood pressure decreased from 130 ± 18.43 mmHg to 113.33 ± 15.27 (P < 0.001), and diastolic blood pressure decreased from 80.17 ± 10.12 mmHg to 71.50 ± 9.29 (P < 0.001).
Conclusion
It was found a significant correlation between IVCD and IVC-CI with ultrafiltration of hemodialysis. Thus, IVC ultrasound can be used in dry weight assessment in ESRD patients on regular HD by measurement of IVCD and IVC-CI before and after hemodialysis.
Similar content being viewed by others

Background
Sixty years ago, Belding Scribner developed a blood access device which is used for repeated hemodialysis and became known as the Scribner shunt [1]. The development of the Scribner shunt opened the door for the creation of grafts and fistulas [2, 3]. One of the vital functions of the kidney is the regulation of fluid homeostasis [4]. Patients with renal failure suffer from fluid overload which is a risk factor for mortality and morbidity [5, 6]. So, accurate assessment of fluid status in hemodialysis patients is very important and represents a big challenge as the achievement of euvolemia is dependent on the skills of the treating physician. Dry weight definition is “the lowest post-dialysis weight at which patients are vitally stable with minimal symptoms of hypervolemia or hypovolemia” [7]. Overestimation of dry weight may lead to chronic fluid overload, edema, hypertension, and cardiac complications [8], while underestimation may lead to hypovolemia followed by complications like hypotension, nausea, headache, and muscle cramps [9]. Clinical parameters (heart rate, blood pressure, venous congestion, and lower limb edema) are not specific for fluid assessment and not always reliable. Therefore, optimal estimation of fluid status should include a combination of clinical and technical assessment methods [10]. Central venous pressure (CVP) [11], lung ultrasound [12], inferior vena cava (IVC) ultrasound [13], bio-impedance spectroscopy (BIS), and levels of atrial natriuretic peptide [14] can be used in the fluid status assessment. Recently, IVC ultrasound machines are available everywhere and can be easily used as it is considered a non-invasive evaluation method [15]. It can be very helpful in fluid management in the perioperative period, in trauma resuscitation, and ICU patients [16]. In this study, we used ultrasound to measure inferior vena cava diameter (IVCD) during inspiration (IVCi) and expiration (IVCe) in ESRD patients on regular hemodialysis before and after dialysis.
Aim
This study aims to evaluate the role of IVC collapsibility index and diameter measured by ultrasound in estimating fluid overload in regular hemodialysis patients to get the ideal dry weight.
Methods
Study design
A controlled cross-sectional study was conducted between 5 January and 15 March 2021.
Study area and population
The study was carried out at the dialysis unit of the Internal Medicine department, in cooperation with the Radiology department, Faculty of Medicine, Bab Al Shaeria University hospitals. The study was conducted on 45 persons classified into two groups as follows:
-
Group A: 30 end-stage renal disease patients, on regular hemodialysis receiving 3 sessions per week, 4 h for each session, with age over 18 years.
-
Group B: 15 healthy persons with no history of any disease that affects IVC diameter and with age over 18 years.
All patients participating in this study were recruited according to the following criteria
Inclusion criteria
-
1.
End-stage renal disease patients on regular hemodialysis, with age over 18 years
-
2.
Healthy persons with no history of any disease that affects IVC diameter (hear failure, liver cirrhosis) and with age over 18 years
Exclusion criteria
-
1.
Patients refused to be included in this study
-
2.
Patients with criteria of heart failure
-
3.
Patients with liver cirrhosis
-
4.
COPD patients
-
5.
Obese (BMI ≥ 30)
All patients were subjected to the following:
-
1.
Full history taking
-
2.
Full clinical examination
-
3.
Weight and height measurement
-
4.
Dry weight assessment by clinical parameters: symptoms, weight, blood pressure, heart rate, and lower limb edema before and after HD
-
5.
Echocardiography to exclude heart failure
-
6.
Abdominal ultrasound to exclude liver cirrhosis
-
7.
Chest x-ray
-
8.
Inferior vena cava diameter (IVCD) measurement by ultrasound before and after hemodialysis
-
9.
Calculation of Kt/v
-
10.
Laboratory investigations: complete blood count (CBC), kidney functions (serum urea and serum creatinine before and after HD), blood chemicals (serum Na, Ca, K), and liver functions (albumin, PT)
For normal group:
-
1.
Full history talking
-
2.
Full clinical examinations
-
3.
Weight and height measurement
-
4.
Measurement of inferior vena cava diameter (IVCD) by ultrasound
Laboratory investigations: complete blood count (CBC), kidney functions (serum urea and serum creatinine), blood chemicals (serum Na, Ca, K), and liver functions
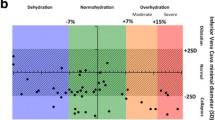
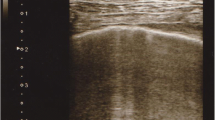
IVCD was measured 1.5 cm below the diaphragm in the hepatic segment in the supine position. IVCD was measured during normal inspiration and expiration. IVC diameter at inspiration ranges from 0 to 14 mm at rest and expiratory diameter of 15 to 20 mm at rest. IVC collapsibility index (IVC-CI) is defined as (IVCe − IVCi)/ IVCe [17].
Statistical analysis
Data were handled using SPSS software version 20. We presented the qualitative data as frequencies and percentages and quantitative data as mean, standard deviation, range, and median. To compare two groups of quantitative data, we used independent t test and paired t test. We used the ROC curve to compare between variables. We used the following criteria to determine the P value.
Significance level:
-
P value ≤ 0.05: significant
-
P value ≤ 0.001: highly significant
-
P value > 0.05: insignificant
Results
Considering demographic data, a total of 45 persons were included the study and were classified in two groups:
-
Group [A]: 30 ESRD on regular HD in (18 men and 12 women)
-
Group [B]: 15 healthy persons in group B (10 men and 5 women)
Ages in group [A] ranged between 29 and 70 years with a mean of 48.38 ± 12.704 years.
Ages in group [B] ranged between 25 and 55 years with a mean of 34.93 ± 8.268 years.
The mean dry weight for group [A] was 68.37 kg (68.37 ± 10.424).
The mean weight for group [B] was 70.67 Kg (70.67 ± 7.669) (Table 1).
Considering IVC parameters, in group [A] before hemodialysis, the mean of IVCe was 2.013 ± 0.298, the mean of IVCi was 0.99 ± 0.487, and the mean of IVC-CI was 0.527 ± 0.189, while in group [B], the mean of IVCe was 1.68 ± 0.174, the mean of IVCi was 0.8 ± 0.141, and the mean of IVC-CI was 0.525 ± 0.054 (Table 2).
Following ROC curve, the difference in IVCi and IVC-CI of both groups was not significant (P > 0.05). However, the difference in IVCe was significant (P < 0.05). The area under the ROC curve of IVCe was significantly higher than 0.5 concluding that the expiratory IVC could differentiate between HD patient and normal one (Fig. 1).

Comparison between IVC parameters in both groups
After HD mean, IVCe decreased from 2.013 ± 0.298 to 1.797 ± 0.226 cm (P < 0.001), mean IVCi decreased from 0.99 ± 0.487 to 0.643 ± 0.391 cm (P < 0.001), while mean IVC-CI increased from 0.527 ± 0.189 to 0.652 ± 0.187 (P < 0.001) (Table 3). Changes in IVCD were significantly correlated with alterations in body weight following dialysis (P < 0.001) . IVCD and its IVC CI reflected alterations in fluid status.
Following the ROC curve, the differences in IVCe and IVC-CI before and after HD sessions were significant (P < 0.05). The area under the ROC curves of the IVCe and IVC-CI were significantly higher than 0.5 concluding that IVCe and IVC-CI could identify the efficacy of ultrafiltration among HD patients (Fig. 2).

Comparison between IVC parameters before and after HD
Regarding the clinical parameters of fluid status, following HD mean, heart rate increased from 81.80 ± 5.15 beats per minute to 89.87 ± 6.42, (P < 0.001), systolic blood pressure decreased from 130 ± 18.43 mmHg to 113.33 ± 15.27 (P < 0.001), and diastolic blood pressure decreased from 80.17 ± 10.12 mmHg to 71.50 ± 9.29 (P < 0.001) (Table 4).
According to the dry weight method, 22 patients were hypervolemic, 6 were euvolemic, and 2 were hypovolemic before dialysis, and after dialysis, 7 were still hypervolemic, 21 were euvolemic, and 2 were hypovolemic. According to the IVC-CI, 16 were hypervolemic, 8 euvolemic, and 6 hypovolemic before dialysis. After dialysis, 7 were hypervolemic, 5 euvolemic, and 18 were hypovolemic. Thus, there were a significant number of patients who became hypovolemic after dialysis according to the IVC-CI.
Test result of the ROC curve. Comparison between IVC parameters in both groups
Test result variable(s) | Area | Std. error | P value | 95% confidence interval | |
|---|---|---|---|---|---|
Lower bound | Upper bound | ||||
IVCe before | 0.831 | 0.061 | 0.00 | 0.711 | 0.951 |
IVCi before | 0.56 | 0.087 | 0.516 | 0.39 | 0.73 |
C.I. before | 0.466 | 0.091 | 0.709 | 0.287 | 0.644 |
Discussion
The results in our study suggest that clinical parameters are not always reliable and not specific for fluid status assessment. Hypovolemic complications such as dizziness, headache, and muscle cramps result from the underestimation of dry weight. In extreme cases, intradialytic hypotension is common which endangers perfusion to vital organs. In our patients, hypovolemic symptoms occurred in fifteen instances. After dialysis, the patients’ blood pressure is expected to increase (paradoxical hypertension) or to decrease (depending on the degree of hypovolemia) compared to pre-dialysis blood pressure with a rise in heart rate which is an indicator of hypovolemia [18]. On the other hand, overestimation of the dry weight may cause chronic fluid overload and complications such as hypertension and congestive heart failure [19]. Therefore, optimal estimation of fluid status should include a combination of clinical and technical assessment methods. One of these methods is the central venous pressure measurement but is considered an invasive method for evaluation and cannot be used routinely [20]. Another method is lung ultrasound but is not accurate and has some limitations [21]. Bio-impedance and levels (BIS) of atrial natriuretic peptide are available but require special machines and are not very accurate [22, 23]. At the same time, ultrasound machines are available and can be easily used to measure IVCD in hospitals during inspiration and expiration [24]. Previous studies in adults and children have used IVCD to estimate the intravascular volume in HD patients and to correlate well the ultrafiltration [25, 26]. This study has been done to evaluate the role of IVCD and CI in regular hemodialysis patients compared with healthy individuals. IVCe, IVCi, and IVC-CI were measured before and after HD and were correlated well with the amount of ultrafiltration achieved via dialysis.
In our study, IVCD decreased significantly following dialysis and correlated well with the changes in weight, and IVC-CI increased significantly after ultrafiltration. We have taken IVC-CI < 0.40 as hypervolemic, IVC-CI > 0.40 to < 0.75 as euvolemic, and IVC-CI > 0.75 as hypovolemic. When the patients’ fluid status was classified according to the IVC-CI, 18 (60 % of patients) were hypovolemic, while 7 patients were hypervolemic and only 5 patients were euvolemic after the dialysis session.
Test result of the ROC curve. Comparison between IVC parameters before and after HD
Test result variable(s) | Area | Std. error | P value | 95% confidence interval | |
|---|---|---|---|---|---|
Lower bound | Upper bound | ||||
C.I. | 0.747 | 0.063 | 0.001 | 0.623 | 0.871 |
IVCe | 0.254 | 0.063 | 0.001 | 0.130 | 0.378 |
IVCi | 0.532 | 0.079 | 0.668 | 0.377 | 0.687 |
Conclusion
IVC ultrasound can be used in dry weight assessment in ESRD patients on regular HD by measurement of IVCD and IVC-CI. It was found a significant correlation between IVCD and IVC-CI with ultrafiltration. Traditional methods based on clinical parameters are not always reliable and not specific for fluid status assessment. Thus, using IVC parameters before and after hemodialysis could be very useful in the estimation of fluid status to get the ideal dry weight.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- IVC:
-
Inferior vena cava
- IVC-CI:
-
Inferior vena cava collapsibility index
- CVP:
-
Central venous pressure
- ESRD:
-
End-stage renal disease
- HD:
-
Hemodialysis
- IVCD:
-
Inferior vena cava diameter
- BMI:
-
Body mass index
- IVCe:
-
Inferior vena cava expiratory
- IVCi:
-
Inferior vena cava inspiratory
- COPD:
-
Chronic obstructive lung disease
- BIS:
-
Bio-impedance spectroscopy
- ICU:
-
Intensive care unit
References
Himmelfarb J, Ikizler TA (2010) Hemodialysis. New Engl J Med 363(19):1833–1845. https://doi.org/10.1056/NEJMra0902710
Rose DA, Sonaike E, Hughes K (2013) Hemodialysis access. Surg Clin 93(4):997–1012. https://doi.org/10.1016/j.suc.2013.05.002
Murea M, Geary RL, Davis RP, Moossavi S (2019) Vascular access for hemodialysis: a perpetual challenge. Semin Dial 32(6):527–534. https://doi.org/10.1111/sdi.12828
Chambers D, Huang C, Matthews G (2019) Renal regulation of water and electrolyte balance. In: Basic Physiology for Anaesthetists. Cambridge University Press, Cambridge, pp 318–328. https://doi.org/10.1017/9781108565011.072
Zoccali C, Moissl U, Chazot C, Mallamaci F, Tripepi G, Arkossy O, Wabel P, Stuard S (2017) Chronic fluid overload and mortality in ESRD. J Am Soc Nephrol 28(8):2491–2497. https://doi.org/10.1681/ASN.2016121341
Onofriescu M, Siriopol D, Voroneanu L, Hogas S, Nistor I, Apetrii M et al (2015) Overhydration, cardiac function and survival in hemodialysis patients. PloS one 10(8):e0135691. https://doi.org/10.1371/journal.pone.0135691
Huang SHS, Filler G, Lindsay R, McIntyre CW (2015) Euvolemia in hemodialysis patients: a potentially dangerous goal? Semin Dial 28(1):1–5. https://doi.org/10.1111/sdi.12317
Agarwal R (2010) Hypervolemia is associated with increased mortality among hemodialysis patients. Hypertens J 56(3):512–517. https://doi.org/10.1161/HYPERTENSIONAHA.110.154815
Pirkle JL Jr, Comeau ME, Langefeld CD, Russell GB, Balderston SS, Freedman BI, Burkart JM (2018) Effects of weight-based ultrafiltration rate limits on intradialytic hypotension in hemodialysis. Hemodial Int 22(2):270–278. https://doi.org/10.1111/hdi.12578
Dekker MJ, Kooman JP (2018) Fluid status assessment in hemodialysis patients and the association with outcome: review of recent literature. Curr Opini Nephrol Hypertens 27(3):188–193. https://doi.org/10.1097/MNH.0000000000000409
Marik PE (2010) Hemodynamic parameters to guide fluid therapy. Transfus Altern Transfus Med 11(3):102–112. https://doi.org/10.1111/j.1778-428X.2010.01133.x
Vitturi N, Dugo M, Soattin M, Simoni F, Maresca L, Zagatti R, Maresca MC (2014) Lung ultrasound during hemodialysis: the role in the assessment of volume status. Int Urol NephrolJ 46(1):169–174. https://doi.org/10.1007/s11255-013-0500-5
Shrestha SK, Ghimire A, Ansari SR, Adhikari A (2018) Use of handheld ultrasound to estimate fluid status of hemodialysis patients. Nep Med J 1(2):65–69. https://doi.org/10.3126/nmj.v1i2.21584
Ko H, Jayasekara R, Grech C (2019) Effectiveness of bioimpedance spectroscopy on dry weight (DW) measurement in haemodialysis patients: a systematic review. Renal Soc Aus J 15(2):53–63. https://doi.org/10.33235/rsaj.15.2.53-63
Marik P, Lemson J (2014) Fluid responsiveness: an evolution of our understanding. Brit J Anaesthesia 112(4):617–620. https://doi.org/10.1093/bja/aet590
Kalantari K, Chang JN, Ronco C, Rosner MH (2013) Assessment of intravascular volume status and volume responsiveness in critically ill patients. Kidney Int J 83(6):1017–1028. https://doi.org/10.1038/ki.2012.424
Seyal MS (2009) The Textbook of Emergency Cardiovascular Care and CPR. JAMA 301(20):2162. https://doi.org/10.1001/jama.2009.731
Reeves PB, Mc Causland FR (2018) Mechanisms, clinical implications, and treatment of intradialytic hypotension. Clin J Am Soc Nephrol 13(8):1297–1303. https://doi.org/10.2215/CJN.12141017
Arkouche W, Giaime P, Mercadal L (2013) Fluid overload and arterial hypertension in hemodialysis patients. Nephrol Ther 9(6):408–415. https://doi.org/10.1016/j.nephro.2013.04.004
Thanakitcharu P, Charoenwut M, Siriwiwatanakul N (2013) Inferior vena cava diameter and collapsibility index: a practical non-invasive evaluation of intravascular fluid volume in critically-ill patients. J Med Assoc 96(Suppl 3):S14–S22
Lichtenstein DA (2014) Lung ultrasound in the critically ill. Ann Intensive Care 4(1):1–12. https://doi.org/10.1186/2110-5820-4-1
Sivalingam M, Vilar E, Mathavakkannan S, Farrington K (2015) The role of natriuretic peptides in volume assessment and mortality prediction in haemodialysis patients. BMC Nephrol J 16(1):1–10. https://doi.org/10.1186/s12882-015-0212-4
Merhametsiz O, Oguz E, Yayar O, Bektan B, Canbakan B, Ayli D (2015) Bioimpedance spectroscopy method to determine hypervolemia in maintenance hemodialysis patients. Hippokratia 19(4):324–331
Zhang Z, Xu X, Ye S, Xu L (2014) Ultrasonographic measurement of the respiratory variation in the inferior vena cava diameter is predictive of fluid responsiveness in critically ill patients: systematic review and meta-analysis. Ultrasound Med Biol 40(5):845–853. https://doi.org/10.1016/j.ultrasmedbio.2013.12.010
Kaptein MJ, Kaptein JS, Oo Z, Kaptein EM (2018) Relationship of inferior vena cava collapsibility to ultrafiltration volume achieved in critically ill hemodialysis patients. Int J Nephrol Renovasc 11:195–209. https://doi.org/10.2147/IJNRD.S165744
Torterüe X, Dehoux L, Macher M-A, Niel O, Kwon T, Deschênes G, Hogan J (2017) Fluid status evaluation by inferior vena cava diameter and bioimpedance spectroscopy in pediatric chronic hemodialysis. BMC Nephrol J 18(1):1–7. https://doi.org/10.1186/s12882-017-0793-1
Acknowledgements
Great thanks to all participants in this work, supervisors, all authors, and our colleges in the Nephrology department in our hospital for their effort. Special thanks to Dr. Mahmoud Hagag for his great guidance and advice.
Funding
We did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
EAM and MAEA carried out the idea as well as performing the surgeries; MAM performed ultrasound for patients and healthy groups; MAH did the literature search, drafted the manuscript, and designed the figures. All authors discussed the results and commented on the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the local research ethical (Committee of Internal Medicine Department and Committee of Faculty of Medicine, Al Azhar University, Egypt, registration number Med_00000126 August 2020 (telephone, fax: + 0020224020184, http://www.medicineazhar.edu.eg) .(All patients included in this study gave written informed consent to participate in this research.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hafiz, M.A.E.H., Mohamed, E.A., Mohamed, M.A.E.N. et al. Inferior vena cava diameter and collapsibility index as a marker of fluid status in regular hemodialysis patients. Egypt J Intern Med 33, 43 (2021). https://doi.org/10.1186/s43162-021-00072-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-021-00072-x