
Abstract
Background
Gastrointestinal duplications are uncommon occurring in 1 in 5000 live births. Small intestine is commonly involved, while appendicular duplications are extremely rare. Vitelline duct anomalies arise due to failure of involution of the omphalomesenteric duct. Their spectrum ranges from a simple umbilical sinus to completely patent omphalomesenteric fistulae. We report here a rare association of complete appendico-cecal duplication with patent vitello-intestinal duct (PVID).
Case presentation
A 14-year-old girl who presented with complaints of scant, foul smelling, and feculent discharge from umbilicus intermittently since birth was evaluated and diagnosed to have a patent vitello-intestinal duct. At laparotomy, a patent vitello-intestinal tract opening unusually at the ileo-cecal junction was noted. In addition, an appendico-cecal duplication cyst bearing an appendix on the mesenteric side and a 4-cm long orthotopic appendix on the native cecum was found with the duplex cecum sharing a common wall and blood supply. The terminal ileum with the duplication and patent vitello-intestinal duct were excised in toto, and an end-to-end ileo-ascending anastomosis was done. The child is well at 1 year follow-up.
Conclusion
A complete appendico-cecal (Type C) duplication with ectopically inserted patent vitello-intestinal duct is reported here as an unusual association, discussing its management and the probable disarray in the embryological development.
Similar content being viewed by others


Background
Gastrointestinal duplications are rare congenital anomalies which occur in 1 per 5000 live births [1]. They are characterized by intimate attachment to the alimentary tract, presence of well-developed smooth muscle coat, and epithelial lining resembling some part of the alimentary tract. Small bowel is the commonest site for duplications. Appendicular duplications are rarer, albeit the fact that appendix is a commonly encountered organ in day-to-day surgical practice.
Vitelline duct anomalies arise due to failure of involution of the omphalomesenteric duct [2]. The spectrum of these anomalies is wide and may vary from the commonly encountered Meckel’s diverticulum to completely patent omphalomesenteric fistulae.
We report here a rare occurrence of complete appendiculo-cecal duplication with patent vitello-intestinal duct (PVID) having an ectopic insertion at the ileo-cecal junction.
Case presentation
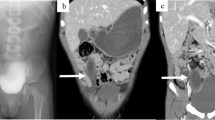
A 14-year-old girl was admitted with complaints of passage of scant, foul smelling, and often-feculent discharge from umbilicus on and off since birth. There was no history of fever, abdominal distension, or bowel/ bladder disturbances. General physical examination was unremarkable. Local examination revealed a soft, non-tender abdomen, vertical slit umbilicus with scant, feculent discharge. Blood investigations were normal. Abdominal ultrasound showed a hypoechoic tract between the umbilicus and small intestinal bowel loops suggestive of vitello-intestinal fistula (Fig. 1).

Sonographic appearance of vitello-intestinal duct
With a provisional diagnosis of patent vitello-intestinal duct, she was taken up for exploration by a limited infra-umbilical incision. At laparotomy, a patent vitello-intestinal tract was noted, extending from the umbilicus to the ileo-cecal junction. In addition, a 4 × 5 cm cystic appendico-cecal duplication cyst bearing a 3-cm-long appendix was noted on the mesenteric side, along with a 4-cm-long orthotopic appendix on the native cecum. Both cecum shared a common wall and blood supply and communicated with ascending colon distally (Fig. 2).

Intra-operative finding
The terminal 7 cm of the ileum with the duplicated cyst and patent vitello-intestinal duct were excised in toto. Bowel continuity was restored by end-to-end ileo-ascending anastomosis (Fig. 3). She had an uneventful postop recovery and is well at follow-up (1 year). Histopathologic examination was congruous with the gross findings (Figs. 4 and 5).

Excised specimen showing patent vitello-intestinal tract (black arrow), terminal ileum (white arrow), native appendix with cecum (tip of hemostat) alongside duplicated cecum and appendix sharing common wall

Histopathology of duplex appendix

Histopathology of vitello-intestinal duct showing colonic mucosa and a patent lumen
Discussions
Small intestine harbors duplications commonly, with appendicular duplication being extremely rare, accounting for 0.4% of all gastrointestinal duplications and affecting 1 of 12,500 patients [3]. Its incidence was first reported by Collins in his study of over 50,000 necropsy specimens [4]. Complete patency of the vitello-intestinal duct is also equally rare (0.0067%) [5]. In most cases, the finding is incidental and predominant in infants or small children. Appendicular duplications were first classified by Cave [6] in 1936, modified by Wallbridge and Waugh [7] in 1962, and finally revised by Biermann [8] in 1993. Type A occurs when two appendices partially or completely arise from a common cecal base and is not associated with other congenital anomalies. Type B has four subtypes and involves one appendix in the normal location and the second appendix in an ectopic site [9]. Type B1 has the second appendix located on the cecum just superior to the ileo-cecal valve (also called the “avian” or “bird” type as it simulates natural anatomical arrangement in birds); in type B2, the duplex appendix is on one of the taenia of the cecum. It is along the taenia of the hepatic flexure and splenic flexure of the colon in type B3 and type B4 respectively. Type C involves duplication of the cecum, with each cecum bearing an appendix. Types B and C can be associated with other gastrointestinal and genitourinary anomalies. The recently described horseshoe anomaly of the appendix is considered type D anomaly [10].
Most duplications present in infancy or early childhood, although late presentations are reported [11]. Signs and symptoms are related to location, type, size, and the presence of ectopic gastric mucosa [12]. Clinical findings in patients with duplication include recurrent abdominal pain, vomiting, abdominal distention, intestinal obstruction, palpable abdominal mass, failure to thrive, constipation, and occasionally bleeding from ectopic gastric mucosa [13]. Duplication cysts can sometimes be detected incidentally. Patent vitello-intestinal remnants often present with features of intestinal obstruction and discharge per umbilicus or may be asymptomatic [14]. Our patient presented primarily with features of patent vitello-intestinal tract that was confirmed by ultrasound, but appendico-cecal duplication was an unexpected intra-operative surprise. Nevertheless, ultrasound remains a preferred investigation for evaluating suspected gastro-intestinal duplications, which present as cystic abdominal masses [15]. This helps in pre-operative counseling of patient caregivers about the possible need for intestinal resection.
The treatment of choice for appendicular duplication is total surgical excision [16], to prevent complications. Type A duplication can be treated with a simple appendicectomy of both appendix. This avoids diagnostic confusion, should the pathology recur in the other appendix in future. Type B duplications are also amenable to appendectomy of the involved appendix. However, type C duplications with a shared blood supply and common wall require a limited resection of the duplex cecum with appendix and ileo-colic anastomosis to restore intestinal continuity. As most lesions are small and do not require long intestinal resections, total cyst excision with limited resection of the adjacent intestinal segment is preferred.
The anatomical curiosity of this case lies in the fact that these anomalies are very rare in an organ commonly affected with inflammatory pathology (< 100 complete appendix duplications reported till date) [17]. There is an isolated report of appendicular duplication associated with Meckel’s diverticulum [18] with an uncertain suggestion towards the embryological aberration by the authors. One of Cave’s theories on the pathogenesis of duplex appendix that appendicular duplication is only incidental to a more general affection of the primitive midgut [19] probably explains the rare association noted in our case and may warrant future studies in the embryology of these anomalies.
Conclusions
A complete appendico-cecal (type C) duplication with patent vitello-intestinal duct having an ectopic insertion at ileo-cecal junction is a unique association not thus far reported in literature. Embryology of the anomaly is indistinct; however, the management is simple with a predictable outcome.
Availability of data and materials
Not applicable
Abbreviations
- PVID:
-
Patent vitello-intestinal duct
References
Currie AB, Hemalatha VH, Doraiswamy NV. Duplications of the alimentary tract. J R Coll Surg Edinb. 1978;23(6):347–54.
Moore TC. Omphalomesenteric duct malformations. Seminars in Pediatric Surgery. 1996;5(2):116–23.
Kjossev KT, Losanoff JE. Duplicated vermiform appendix. Br J Surg. 1996;83:1259.
Collins DC. A study of 50,000 specimens of the human vermiform appendix. Surg Gynecol Obstet. 1955;101:437–45.
Elebute EA, Ransome-Kuti O. Patent vitello-intestinal duct with ileal prolapse. Archives of Surgery. 1965;91(3):456–60. https://doi.org/10.1001/archsurg.1965.01320150086013.
Cave AJE. Appendix vermiformis duplex. J Anatomy. 1936;70(Pt 2):283–92.
Wallbridge PH. Double appendix. British J Surg. 1963;50:346–7.
Biermann R. Appendix duplex. Eine Pathologische Raritat. 1993;64:1059–61.
Bender E, Schmidt S. Type B2 appendiceal duplication with appendicitis: a case report. Int J Surg. 2002;3:2.
Drino RD, Kotjelnikov B, Aksamija G. Rare anomalies in the development of the appendix. Acta Chir Iugosl. 1991;38(1):103–11.
Kim EP, McClenathan JH. Unusual duplication of appendix and cecum: extension of the Cave-Wallbridge classification. J Pediatr Surg. 2001 Sep;36(9):E18. https://doi.org/10.1053/jpsu.2001.26400.
Temiz A, Oğuzkurt P, Ezer SS. Different clinical presentations, diagnostic difficulties, and management of cecal duplication. Journal of Pediatric Surgery. 2013;48(3):550–4. https://doi.org/10.1016/j.jpedsurg.2012.07.048.
Kumar A, Kumar P, Chand K. Intestinal Duplication with ectopic gastric mucosa diagnosed by Meckel’s diverticulum scan. Iran J Nucl Med. 2017;25(47):73–6.
Lund DP. Alimentary tract duplications. In: Grosfeld JL, O’Neill JA, Fonkalsrud EW, Coran AG, editors. Pediatric surgery. 6th ed. Philadelphia: Mosby-Elsevier; 2006. p. 1389–98. https://doi.org/10.1016/B978-0-323-02842-4.50091-7.
Nebot CS, Salvador RL. Enteric duplication cysts in children: varied presentations, varied imaging findings. Insights Imaging. 2018;9(6):1097–106. https://doi.org/10.1007/s13244-018-0660-z.
Iyer CP, Mahour GH. Duplications of the alimentary tract in infants and children. J Pediatr Surg. 1995;30(9):1267–70. https://doi.org/10.1016/0022-3468(95)90482-4.
Modi H, Kosmin M. A case of a duplicated vermiform appendix associated with a Meckel’s diverticulum. Gastroenterology Today. 2008;18(4):114–5.
Panda SK, Prasad C, Tirkey R, Rajesh V, Mishra J, Dora RK. Unusual association of Meckel’s diverticulum with double appendix – a rare finding. International Journal of Surgery Case Reports. 2014;5(11):879–81. https://doi.org/10.1016/j.ijscr.2014.09.009.
Canbay E, Akman E. Appendix perforation in appendix duplication in a man: a case report. J Med Case Reports. 2011;5(1):162. https://doi.org/10.1186/1752-1947-5-162.
Acknowledgements
Not applicable
Funding
None
Author information
Authors and Affiliations
Contributions
RKR and PK were involved directly in patient care, surgery, collection of investigation reports/images, and drafting of the manuscript. JC performed the histological examination of the resected specimen and contributed to the writing of the manuscript. SAM played a major role in assimilating and the critical review of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Institutional Ethics Review Board (IERB)/Institutional Ethics committee (IEC) clearance granted vide IEC No-146/2021
Consent for publication
Written informed consent was obtained from the parent (father) of the patient for publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rajkiran Raju, S., Prasanna Kumar, A.R., Shubha, A.M. et al. “Type C appendicular duplication with patent vitello-intestinal duct—an unforeseen association”—a case report. Ann Pediatr Surg 17, 58 (2021). https://doi.org/10.1186/s43159-021-00127-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43159-021-00127-2