
Abstract
Background
Enteric duplication is a congenital disease that occurs throughout the entire gastrointestinal tract. Although it may sometimes cause intestinal volvulus, a few reports have described cases of enteric duplication twisted on itself. We experienced a rare pediatric case of long-segment tubular ileal duplication showing torsion. Torsion of enteric duplication is extremely rare. We herein report a pediatric case showing unusual torsion of ileal duplication requiring emergency surgery.
Case presentation
A 3-year-old boy presented with abdominal pain and vomiting. Contrast-enhanced computed tomography (CT) revealed a cystic luminal structure with a blind end and fluid collection in the pelvic cavity. CT also showed no findings of ileus or intestinal dilatation except for a cystic luminal structure. The preoperative diagnosis was torsion of Meckel’s diverticulum. The patient underwent emergent explorative diagnostic laparoscopy. As a result, a necrotic luminal structure and bloody ascites were recognized, and small-scale laparotomy was performed. Long-segment ileal duplication was recognized. The long-segment tubular ileal duplication shared the anti-mesenteric side of the intestinal wall along one-third of its length. The residual two-thirds of its length was free from the ileum and its blind end was twisted in a manner that looked similar to Meckel’s diverticulum. Normal ileum and the duplication, including the twisted necrotic portion, were resected, and ileal anastomosis was performed. The postoperative course was uneventful. A pathological examination confirmed the definitive diagnosis of enteric duplication.
Conclusions
We reported the unusual presentation of intestinal duplication mimicking torsion of Meckel’s diverticulum. Enteric duplication shows various clinical symptoms and presentations. We must understand that the classification of digestive enteric duplication is diverse with a variety of associated clinical symptoms.
Similar content being viewed by others


Background
Enteric duplication is a congenital disease that occurs throughout the entire gastrointestinal tract. Although it may cause intestinal volvulus, there are few reports of enteric duplication itself being twisted.
We herein report a pediatric case in which the diverticulum-like site of tubular intestinal duplication was twisted and necrotic. Torsion of enteric duplication is extremely rare, and this case is reported along with a review of the literature.
Case presentation
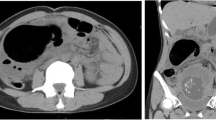
A 3-year-old boy presented with complaints of acute abdominal pain. The patient had visited the primary care pediatric clinic the day after the onset and been diagnosed with viral gastroenteritis and received medication conservatively. However, the abdominal pain persisted, so the patient was referred by his primary care physician to the previous local hospital. An abdominal X-ray did not show dilation of intestine and findings of ileus (Fig. 1a). The patient underwent contrast-enhanced computed tomography (CT), which revealed a cystic lesion similar to the structure of the gastrointestinal tract and ascites retention in the abdominal cavity (Fig. 1b, c). The patient was therefore transferred to our hospital for acute abdomen. He had a fever and showed abdominal distension and tenderness with peritoneal signs in the right lower abdomen. Blood sampling showed an elevated white blood cell count and CRP (Table 1).

Abdominal X-ray and contrast-enhanced CT. a An abdominal X-ray did not show dilation of intestine and findings of ileus. b, c From the right middle abdomen to the bottom of the pelvis, we detected a gastrointestinal-like lesion (arrow) that was blind with fluid retention inside
We reviewed the contrast-enhanced CT findings again. There were no findings of ileus or intestinal dilatation except for the cystic luminal structure. The blood supply of the entire gastrointestinal tract was also preserved, except for the cystic luminal structure. Based on the clinical symptoms and these imaging findings, the preoperative diagnosis was torsion of Meckel’s diverticulum.
We decided to perform exploratory laparoscopic inspection to obtain a definitive diagnosis. Exploratory laparoscopy revealed that the dark-colored twisted cystic luminal structure was located at the right lower abdomen, and its root seemed to be continuous with the small intestine (Fig. 2a). After releasing the 720° clockwise twisting, the cystic luminal structure was confirmed to have branched off of the small intestine. However, the connected formation was not that of Meckel’s diverticulum, but rather duplication.

Intraoperative findings. a A strangulated necrotic tubular structure was recognized to demonstrate torsion. Its root was continuous with the intestinal tract and was twisted. b, c Intestinal duplication was found along the normal intestinal tract. It shared a wall with the small intestine and ran in parallel for 15 cm, but its anal side showed a diverticulum-like form (arrow) and was twisted
Small-scale laparotomy using the umbilical trocar wound was then performed to clarify the pathophysiological mechanism. The entire small intestine was extracted through the wound retractor. A long segment of tubular ileal duplication was recognized at 120 cm from the oral side of the ileocecal region (Fig. 2b). The long-segment tubular ileal duplication shared the anti-mesenteric side of the intestinal wall along one-third of its length. The residual two-thirds of its length was free from the ileum and twisted in a manner similar to Meckel’s diverticulum. Thin pedicle-like structure was recognized at the root of duplication cyst. Blood supply was thought to be kept by both thin pedicle and intramural blood flow. The diverticulum-like part was necrotic due to the twisting (Fig. 2c). The intraoperative diagnosis was torsion of intestinal duplication. The duplicated portion was resected along with the normal ileum, and intestinal anastomosis was performed with one layer. An abdominal drain was not placed, and the wound was closed in layers.
The excised specimen is shown in Fig. 3a. The pathological findings revealed that the luminal structure shared a muscular layer with the normal ileum and had an inner surface covered with intestinal epithelium, which was compatible with intestinal duplication, as shown in Fig. 3b and c.

Excised specimen and pathological findings. a, b The overall picture of the intestinal duplication, partially protruding like a diverticulum and showing necrosis due to twisting. b The inner surface of the intestinal duplication was covered with intestinal mucosa. (arrow). c Hematoxylin–eosin staining of resected specimen. The inner surface of the intestinal duplication was covered with intestinal epithelium (arrow)
The postoperative course was uneventful, and the patient left our hospital on postoperative day 14. He showed no adverse events in 3 years of follow-up.
Discussion
The term enteric duplication was first used by Fitz [1], but was not widely used until it was popularized by Ladd in the 1930s [2], with further classifications by Gross in the 1950s [3]. The reported incidence is 1:4.500 births, and most duplications are recognized in children (antenatally or within first 2 years of life), with fewer than 30% of all duplications diagnosed in adults. Approximately 75% of duplications have been reported to be located within the abdominal cavity, whereas the remaining cases are intrathoracic (20%) or thoracoabdominal (5%). Although the exact etiology is unknown, several theories have been proposed, including a split notochord (currently the most favored), partial twinning, persistent embryological diverticula and aberrant luminal re-canalization. Other rare causes include intrauterine trauma and hypoxia [4, 5].
Many authors have reported variable clinical presentations depending on the location, size and other factors, such as the presence of ectopic mucosa, communication with adjacent bowel or inflammation. Infants and neonates sometimes show abdominal pain, nausea, vomiting, bleeding, abdominal distension, abdominal mass, obstruction and intussusception. Some duplication cysts may remain asymptomatic until adulthood [6].
Duplication can sometimes cause intestinal volvulus, but there have been a few reports in which the enteric duplication itself became twisted. A search on PubMed for the period 1950–2021 using "enteric duplication", "volvulus" and "torsion" as search words revealed four cases of volvulus of the enteric duplication itself. Table 2 shows the five total cases of volvulus of the enteric volvulus itself, including our present case [7,8,9,10]. The patient age ranged from 1 to 53 years old. The main complaint was abdominal pain in all cases, and biliary vomiting was also observed in cases 1 and 2. Imaging revealed dilation of the small intestine and cystic structures. The size varied from 10 to 70 cm. In case 1, the duplicated colonic segment demonstrated torsion over the partially duplicated appendix. Cases 2 and 3 involved a completely isolated duplication cyst in the ileal mesentery, and Case 4 involved tubular intestinal duplication contralateral to the mesentery, similar to our case.
In general, intestinal duplication is located on the mesenteric side and shares a smooth muscle wall with the adjacent gastrointestinal tract. Because the enteric duplication is fixed between the mesentery and the adjacent intestinal tract, it seems difficult to twist. However, in Case 1, the colon duplication was attached to the periphery of the appendix duplication. In addition, the duplication was only in contact with the mesentery with a thin stalk-like structure in Cases 2 and 3. In Cases 4 and 5, diverticulum-like intestinal duplication protruded from the opposite side of the mesentery.
The twisting is considered to be due to the enteric duplication having a structure with good mobility. Ladd et al. proposed a concept of three characteristics: (1) a well-developed smooth muscle coat; (2) mucosal lining found within some portion of the alimentary tract; and (3) contiguity to any segment of the alimentary tract [2]. It is also said that the enteric duplication is usually located on the mesenteric side. However, in recent years, there have been reports of varied cases, such as those that are isolated and those that occur on the opposite side of the mesentery.
The broadly accepted classification of intestinal duplication consists of five types: intestinal membrane type, intestinal wall cyst type, extra-intestinal cyst type, extra-intestinal tubular type and solitary type [11]. The prevalence of gastrointestinal duplication varies, but it is more common in the ileum and ileocolic segment than in other sites. Intestinal duplication is usually cystic or tubular in nature and often continuous with the regular bowel wall, and it shares the muscle and mucosal layer [12]. Li et al. classified enteric duplication into two types according to the pattern of the vascular supply in relation to the duplication and involved bowel [13]. The authors noted that duplications of small intestine have a relatively independent vascular supply and can be resected without the adjacent bowel. Our case seems to be a pattern (Type1c) in which the duplication is located on one side of the mesentery as described by long li et al. Blood perfusion of the conjoined segment was supplied from thin pedicle of the mesentery and those of the residual two-thirds segment was supplied from intramural blood flow. Hung et al. also suggested broad variations in the current anatomical classification [10]. Understanding the different potential forms of enteric duplication can help diagnose enteric duplication based on clinical symptoms and imaging findings.
Our case shared characteristics with the long-segment tubular type and was located at the anti-mesenteric side, and two-thirds of it was also free from the adjacent bowel. The free side had a blind end and the complete structure of the intestinal wall, so the duplication might have had some degree of motility. As a result, torsion would have been able to be induced that mimicked torsion of Meckel’s diverticulum around the root on the free side without the involvement of the mesentery.
Conclusions
We experienced a rare case in which a portion of intestinal duplication located on the anti-mesenteric side protruded with a diverticulum shape and had become twisted. We should consider enteric duplication when encountering cases of cystic lesions presenting with twisting mimicking torsion of Meckel’s diverticulum. Enteric duplication can present with a variety of clinical symptoms.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Fitz RH. Persistent omphalomesenteric remains: their importance in the causation of intestinal duplication, cyst formation and obstruction. Am J Med Sci. 1884;88:30–57.
Ladd WE, Gross RE. Surgical treatment of duplications of the alimentary tract enterogenous cysts, enteric cysts or ileum duplex. Surg Gynecol Obstet. 1940;70:295–307.
Gross RE. Duplications of the alimentary tract. In: The Surgery of Infancy and Childhood. 1953;221–245.
Schalamon J, Schleef J, Hollwarth ME. Experience with gastro-intestinal duplications in childhood. Langenbecks Arch Surg. 2000;385:402–5.
Merrot T, Anastasescu R, Pankevych T, Tercier S, Garcia S, Alessandrini P, et al. Duodenal duplications. Clinical characteristics, embryological hypotheses, histological findings, treatment. Eur J Pediatr Surg. 2006;16:18–23.
Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics. 1993;13:1063–680. https://doi.org/10.1148/radiographics.13.5.8210590.
Sharma S, Yadav AK, Mandal AK, Zaheer S, Yadav DK, Samie A. Enteric duplication cysts in children: a clinicopathological dilemma. J Clin Diagn Res. 2015;9:EC08-11. https://doi.org/10.7860/JCDR/2015/12929.6381.
Oğuzkurt P, Oğuzkurt L, Kayaselcuk F, Oz S. An unusual cause of acute abdomen: torsion of colonic duplication over a duplicated appendix. Pediatr Surg Int. 2004;20:722–3. https://doi.org/10.1007/s00383-004-1283-7.
Xiao-Ming A, Jin-Jing L, Li-Chen H, Lu-Lu H, Xiong Y, Hong-Hai Z, et al. A huge completely isolated duplication cyst complicated by torsion and lined by 3 different mucosal epithelial components in an adult: a case report. Medicine (Baltimore). 2018;97: e13005. https://doi.org/10.1097/MD.0000000000013005.
Huang ZH, Wan ZH, Vikash V, Vikash S, Jiang CQ. Report of a rare case and review of adult intestinal duplication at the opposite side of mesenteric margin. Sao Paulo Med J. 2018;136:89–93. https://doi.org/10.1590/1516-3180.2017.0184030817.
Fuyou H, Hong Y, Yan S. The diagnosis and classification of intestinal duplication (in Chinese). Chinese J. Pediatr. Surg. 1997; 18: 91–93. Available from: http://eng.med.wanfangdata.com.cn/PaperDetail.aspx?qkid=xrwk&qcode=xrwk199702010#.
Sinha A, Ojha S, Sarin YK. Completely isolated, noncontiguous duplication cyst. Eur J Pediatr Surg. 2006;16:127–9.
Li L, Zhang JZ, Wang YX. Vascular classification for small intestinal duplications: experience with 80 cases. J Pediatr Surg. 1998;33:1243–5. https://doi.org/10.1016/s0022-3468(98)90159-2.
Acknowledgements
We thank Mr. Brian Quinn for his comments and help with the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. MM drafted the manuscript. MM, CK, KY and TK performed the surgery. MM, KS, MM, TH and WY collected the data and references. TK and SI gave the advice for manuscript brush-up. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval was obtained from the appropriate ethics review board of our institution. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study; patient anonymity has been preserved, and personal information has been protected.
Consent for publication
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical concerns.
Competing interests
The authors have no conflicts of interest to report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matsukubo, M., Muto, M., Kedoin, C. et al. An unusual presentation of intestinal duplication mimicking torsion of Meckel’s diverticulum: a rare report of a pediatric case. surg case rep 8, 53 (2022). https://doi.org/10.1186/s40792-022-01409-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-022-01409-6