
Abstract
Background
In recent years, public awareness of healthy diets has significantly increased, leading to a rise in the consumption of nutritional supplements. Among these, omega-3 fatty acids have become particularly popular. n − 3 polyunsaturated fatty acids (PUFAs) are widely distributed in marine and terrestrial environments. The primary sources of marine n − 3 fatty acid supplements are oily fish, such as anchovies, sardines and mackerel. Recently, they have drawn considerable attention for their potential therapeutic benefits in treating a range of illnesses, including cancer, neurological disorders, cardiovascular diseases, immunological and reproductive diseases, respectively.
Main text
This study explores the many activities of n − 3 PUFAs, highlighting their importance in cellular processes that include signaling pathways, cell membrane integrity and structural maintenance. These fatty acids significantly regulate important physiological functions including the neurological system, blood pressure control, hematopoiesis, glucose metabolism and inflammatory responses. The latter highlights the wide therapeutic range of n − 3 PUFAs is especially notable considering the implications for controlling inflammatory disorders. Furthermore, the chemistry and dietary sources of omega-3 fatty acids are clarified in this review, which also sheds light on the complex molecular pathways that support the therapeutic efficacy of these fats and their bioavailability. The most recent information on the FDA's approval of omega-3 oils for use in formulation development highlights the compounds' adaptability and potential influence on the development of novel medications.
Conclusion
A thorough analysis of omega-3 polyunsaturated fatty acids reveals both their remarkable therapeutic potential against a variety of diseases and their essential place in a normal diet. This study adds to the increasing amount of data that supports the use of n − 3 PUFAs in preventative and therapeutic approaches that are meant to improve human health and well-being by clarifying their mechanisms of action and emphasizing their applicability in formulation and development.
Similar content being viewed by others


Background
The interaction of genetics, environment and nature is the foundation for all health and disease. Nutrition is an environmental factor of major importance. The dietary environment in which humans currently reside differs from the existing genetic makeup. Studies on the evolutionary aspects of diet indicate the major changes, particularly in the intake of essential fatty acids and antioxidant content. Dietary habits and lifestyle parameters in today’s modern society have been characterized by.
-
(1)
An increase in energy intake in comparison to energy expenditure.
-
(2)
An increased intake of dietary saturated fat, omega-6 fatty acids and trans fatty acids than that of omega-3 fatty acids.
-
(3)
Diet with less content of complex carbohydrates and fiber.
-
(4)
Diet with more proportions of cereal grains than of fruits and vegetables.
-
(5)
Reduced intake of protein, antioxidants and calcium.
The rise in trans-fatty acids is toxic to human health because it prevents omega-6 and omega-3 fatty acids from desaturating and elongating. As a result, there is less arachidonic acid, eicosapentaenoic acid and docosahexaenoic acid available for use in human metabolism. The last 150 years in particular have seen dramatic changes in dietary consumption that have been linked to several malignancies related to the breast [1], colon [2] and prostate [3] as well as chronic disorders including atherosclerosis, essential hypertension, obesity, diabetes, arthritis and other autoimmune diseases. Chronic illness is caused by interactions between genetically regulated biochemical processes sedentary lifestyles and toxic drug exposure, in addition to food [4].
The initial evidence of the health benefits of omega-3 fatty acids, namely eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), came from Greenland Eskimos, who consumed a diet heavy in fish and had low rates of multiple sclerosis, asthma, type I diabetes mellitus and coronary heart disease. Numerous studies have shown that omega-3 fats are necessary for the body to synthesize cell membranes in the body and their impact on the function of cell receptors in these membranes. They function as the basic component of hormones that regulate clotting, inflammation, and the contraction and relaxation of arterial walls. Moreover, they can attach to cell receptors that regulate genetic activity. These benefits include the prevention of heart disease and stroke, the management of lupus, eczema, rheumatoid arthritis and the function of omega-3 fats as preventive agents against cancer and other illnesses [5,6,7].
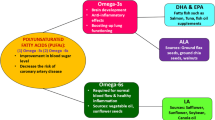
High polyunsaturated fatty acids (PUFAs) include alpha-linolenic acid (ALA), docosahexaenoic acid (DHA), eicosapentaenoic acid (EPA) and n − 3 fatty acids. These PUFAs are identified chemically by the presence of a double bond that is three atoms away from the terminal methyl group as displayed in Fig. 1. The presence of multiple double bonds (polyunsaturation) is a key feature of these fatty acids [8]. The carbon chains of omega-3 fatty acids include bends or kinks due to their special structure, which includes many double bonds. In contrast to saturated fats, which have no double bonds and form solid structures, unsaturated fats are more fluid and flexible due to these kinks that keep the fatty acids from packing closely together. The capacity of this fluidity to provide appropriate membrane permeability and receptor activation is essential to the operation of cell membranes. Omega-3 fats are plentiful; plants contain ALA, while fish and algae have DHA and EPA. Plant oils containing alpha-lipoic acid (ALA) are commonly found in walnuts, edible seeds, flaxseeds and hempseed oil [6]. Mammals must get omega-3 fatty acid from food as they are unable to synthesize it. Therefore, the term "essential for diet" refers to omega-3 fatty acids [9].

Structural classification of omega-3 fatty acid
Main text
Omega-3 fatty acids types
The two primary forms of omega-3 fats that are vital to human health are EPA and DHA. Since the body cannot generate ALA, it is regarded as an essential fat that is necessary for proper human growth and development. It can be converted into EPA and DHA at a limited rate [7, 10].
Sources of omega-3
Foods rich in ALA include flaxseed, soybean and canola oils from plant oils, walnuts and chia seeds. Fish like salmon, mackerel, tuna, herring and sardines contain higher amounts of EPA and DHA. Some foods fortified with DHA and other omega-3 s include specific brands of yogurt, eggs, milk, juices, soya beverages and Algae oils. Dietary supplements containing re-esterified triglycerides, natural triglycerides, free fatty acids and phospholipids are rich sources of DHA [11,12,13]. Omega-3 source from natural and dietary supplements is represented in Fig. 2A and B, respectively [14, 15].

Different sources of omega-3 fatty acid from A natural sources, B dietary supplements
Synthesis of omega-3
ALA is the most basic omega-3 fatty acid (18:3n − 3). With the help of delta-15 desaturase, the n − 6 fatty acid linoleic acid (18:2n − 6) is converted into α-linolenic acid by desaturation. Humans are unable to produce α-linolenic acid because they lack the enzyme delta-15 desaturase. On the other hand, plants can generate α-linolenic acid since they contain delta-15 desaturase. Desaturation mostly happens at carbon atoms lower than carbon 9 (counting from the carboxyl carbon). Figure 3 represents the schematic pathway for the synthesis of omega-3 oils.

Synthesis of omega-3 fatty acids
The hormonal balance, end-product feedback inhibition and nutritional state influence the activities of the delta-6 and delta-5 desaturases. To convert EPA to DHA (22:6n − 3), two carbons must be added to EPA to form DHA (22:5n − 3, or DPA). To make 24:5n-3, EPA needs two extra carbons added to it. This protein is subsequently transferred from the endoplasmic reticulum to peroxisomes, where restricted β-oxidation removes two carbons to form DHA [16].
Therapeutic health benefits of omega-3
Scientific, clinical and industry experts are well aware of the health advantages of omega-3 fatty acids; studies on nearly every bodily system and a wide range of illnesses are shown in Fig. 4. They have an impact on how cell receptors in these membranes function and are essential for the construction of cell membranes throughout the body. Additionally, they operate as a precursor to the synthesis of hormones that regulate blood clotting, artery wall contraction and relaxation, and inflammation. Moreover, they can attach to cell receptors that control genetic activity. These advantages of omega-3 fats make them possibly protective against rheumatoid arthritis, lupus, eczema, heart disease, stroke and cancer, among other disorders [7].

Health benefits of omega-3 in various diseases
Mechanism of omega-3 fatty acids
Omega-3 fatty acids (OM3FAs) are thought to increase lipo-protein-lipase (LPL) expression, increase fatty acid beta-oxidation, suppress lipogenic gene expression and affect total body lipid accretion, though the precise mechanism of action is still unclear [17,18,19]. This occurs at the cellular level as a result of omega-3 fatty acid capacity to bind to peroxisome proliferator-activated receptors (PPARs), which are transcription factors that alter the expression of genes related to energy balance [20, 21]. PPARs control the metabolism of glucose and fatty acids that alter the basal metabolism of cells [22].
The biochemical process by which the body breaks down fat and converts it into energy is called beta-oxidation. OM3FAs primarily work on acetyl-CoA carboxylase and carnitine acetyltransferase 1 (CAT 1) to increase the rate of beta-oxidation, which lowers the body's amount of triacyl glycerides [17, 18]. Through the carnitine-acylcarnitine translocation, carnitine acetyltransferase modifies fatty acid substrates that facilitate its movement through the inner mitochondrial membrane. It is then converted into acyl-CoA, a precursor substrate employed in several metabolic pathways to produce ATP. Additionally, EPA catalyzes the formation of malonyl CoA, a potent CAT1 inhibitor, acetyl-CoA carboxylase that decreases feedback inhibition; hence, beta-oxidation is indirectly increased [18, 20].
By activating AMPK/SIRT, which is crucial for cell maintenance and repair, OM3FAs provide favorable antineoplastic effects for the treatment of breast cancer, colorectal cancer, leukemia, gastric cancer, pancreatic cancer, esophageal cancer, prostate cancer, head cancer, neck cancer and lung cancer [23,24,25]. OM3FAs’ anti-inflammatory properties benefit the treatment of brain disease, cancer, diabetes, rheumatoid arthritis and irritable bowel syndrome. In high-fat tissues such as the brain, the presence of DHA in phospholipid membranes provides a stabilizing and protective impact that contributes to preserving the integrity of neural tissues and cell membranes, thereby improving cognitive function in conditions of Alzheimer's disease and dementia [26,27,28].
The pathophysiology of proliferative and degenerative retinal illnesses is linked to variables and processes that are targeted by long-chain polyunsaturated fatty acids (LCPUFAs) for their anti-angiogenic, anti-vaso proliferative and neuroprotective properties. DHA and EPA are also essential components of retinal cell membranes that help in neovascular and cell survival, thus preventing macular degeneration [29].
Table 1 summarizes the mechanism and receptors involved in offering health benefits in various disease conditions.
Effects of omega-3 supplements on health outcomes
The meta-analysis by Shichun et al. (2022), which included 14 clinical RCTs with a total of 135,291 subjects, found that participants who consumed omega-3 supplements showed a significant reduction in major adverse cardiovascular events (MACEs), cardiovascular death and myocardial infarction (MI) [48]. Similarly, a randomized controlled trial by Dong et al. (2022), part of the VITAL trial, found that participants who consumed omega-3 supplements showed a significant reduction in markers of inflammation compared to the placebo group. This study investigated the effects of Vitamin D3 and marine omega-3 fatty acids on systemic inflammatory biomarkers over four years. These findings underscore the potential health benefits of omega-3 supplementation in reducing both cardiovascular events and inflammation [49].
Stability problem
Foods high in polyunsaturated fatty acids impose a major issue concerning stability that affects their shelf life, consumer acceptability, functioning, safety and nutritional value. The occurrence of fatty acid oxidation notably the aldehydes such as malondialdehyde (MDA) and 4-hydroxy-2-nonenal (4-HNE) that crosslink to proteins and bind covalently to nucleic acids has been linked to the aging process, mutagenesis and development of cancer. Lipid oxidation is accelerated by surface area, heating, irradiation, light and oxygen availability, and other factors, which reduce product stability and shelf life [50].
Oxidation of omega-3 long-chain PUFA occurs in three phases
Initiation phase
Formation of free radicals: Unsaturated fatty acids react with pro-oxidants, including lipoxygenases, singlet oxygen and transition metals, especially iron, to generate lipid radicals, which take out one hydrogen atom.
Propagation phase
-
Oxygen attack The lipid radical reacts with oxygen to form a peroxyl radical (LOO).
-
Chain reaction The peroxyl radical abstracts a hydrogen atom from another lipid molecule, generating another lipid radical and propagating the chain reaction.
-
Hydroperoxide formation The abstracted hydrogen atom combines with oxygen to form a hydroperoxide (LOOH), the primary oxidation product.
Termination phase
-
Radical scavenging Two radicals can combine, terminating the chain reaction. Alternatively, antioxidants can scavenge radicals, preventing further propagation.
Secondary reactions
Hydroperoxides can undergo further decomposition, leading to a complex mixture of volatile and non-volatile secondary oxidation products containing various functional groups like hydroxy, aldehyde, epoxy and ketone. The degree of oxidation is influenced by intrinsic factors such as fatty acid composition, endogenous iron and extrinsic factors such as pH, temperature, oxygen availability, etc. [50].
Approaches to enhance the stability of omega-3 oil
Encapsulation
The n − 3 PUFAs are highly unsaturated, which makes them extremely prone to oxidation. This can lead to the generation of harmful hydroperoxides, off-flavors and a reduced shelf life of the product. Microencapsulating the lipid that has to be preserved is one such approach to prevent oxidation that can prevent or postpone the oxidation of polyunsaturated fatty acids while shielding them from light and heat damage. To improve the preservation of oils, encapsulating agents such as plant gums, modified starch, gelatine, milk protein or dextrin, and modified cellulose have been used. Techniques used for encapsulation are spray-drying, freeze-drying and double coating [50].
Stabilization of foods containing omega-3 LC-PUFAs through modified atmospheric packaging
Omega-3 LC-PUFA is highly susceptible to physical and chemical alterations as a result of light exposure and temperature variations. Modified environment packaging, [MAP], is a commonly used technology to increase the quality and shelf life of perishable omega-3 LC-PUFA-containing products [51].
Applications of omega-3 oil in formulation and development
Bioavailability challenges
Incorporating omega-3 into formulation presents unique challenges due to its high lipophilic properties that limit dispersion and absorption in the human body. Additionally, omega-3 s are susceptible to oxidation which can lead to undesirable flavors and reduced health benefits. Due to its poor oral bioavailability, a high dose needs to be administered for its therapeutic benefits which affect consumer acceptance because of unpleasant fishy taste and odor. To overcome these challenges, scientists have developed various formulation strategies. The bioavailability profile of SEEDS and normal fish oil is illustrated in Fig. 5.

Bioavailability profile of SEEDS and normal fish oil [52]
Advanced delivery systems
In a randomized, double-blind study conducted by Kristen E. Bremmell et al., Aqua Celle, a patented self-micro-emulsifying delivery system (SMEDS), demonstrated an increase in total absorption of omega-3 (EPA and DHA) sixfold when compared to non-emulsified omega 3 oil attributed to Aqua Celle’s emulsifying properties. By employing surfactants and co-surfactants, SMEDS disperse omega-3 s into an aqueous phase forming stable emulsions. These emulsions enhance bioavailability by facilitating intestinal uptake and potentially bypassing the need for dietary fat for optimal absorption [52].
Self-nanoemulsifying drug delivery systems (SNEDDS) to enhance DHA bioavailability were investigated by Alhakamy Na et al. to overcome the limit imposed due to its poor solubility. The optimum droplet size of 111.5 nm, and zeta potential − 23.53 mV enhanced absorption and stability of the formulation. SNEDDS administration resulted in a 3.32-fold increase in DHA plasma levels in comparison to that of the aqueous dispersion, highlighting the efficacy of this delivery approach [53].
Microencapsulation techniques can prevent oxidation of omega-3 fatty acids, increase their shelf life and mask unpleasant flavors. It also provides an effective method for stabilizing and improving the administration of bioactive ingredients. Spray drying and complex coacervation processes are the most popular commercial approaches for microencapsulation. A study by Natalia Castejon et al. examined the effects of the microencapsulation process on the composition of fatty acids and reported that microencapsulated omega-3 lipids with particle sizes ranging from 1.5 to 30 μm showed significant potential for enhancement of bioavailability [54].
Omega-3 oils are susceptible to oxidation and microbial attack which reduces their oral bioavailability. The study by Hamed et al. presents a promising strategy of combining rosemary in microcapsule to stabilize against both oxidation and microbes. Maltodextrin and arabic gum are used as wall material for microcapsule formation. These advancements in formulation unlock the potential of omega-3 oils for functional food and nutraceutical applications [55].
Flaxseed oil, water, sucrose ester as an emulsifier, and antioxidants were combined to develop a unique stabilized emulsified formulation that contained micronutrients and omega-3 fatty acid (omega-3 FA). The stability of the formulations was confirmed using the emulsion stability index, dilution test and freeze–thaw methods. According to OECD criteria, an acute oral toxicity assessment demonstrated the formulations' safety. The created product shows promise for improving the nutritive content and bioavailability of omega-3 FA in the food and nutraceutical sectors [56].
To treat hyperlipidemia, omega-3 fatty acid-based nanostructured lipid carriers of atorvastatin (AT) were developed and assessed through in vitro and in vivo research. Nanolipid carriers (NLC) were formulated by the melt emulsification ultrasonication technology using stearic acid, omega-3 fatty acid as solid and liquid lipid, respectively, Tween 80, poloxamer 188 as surfactant and co-surfactant soya-lecithin. The MTT assay findings demonstrated compatibility with L929 (mouse fibroblast) cell lines, and NLCs had a sustained pattern of drug release. Research on the anti-hyperlipidemic effect of oral treatment revealed a substantial drop in blood LDL and TG levels [57].
FDA approval for safe use of omega 3 oils
There should be fats and oils in a suitable, well-balanced diet. Consuming the right kind and quantity of fat or oil is crucial for maintaining good health and preventing sickness. According to the US Food and Drug Administration's Dietary Guidelines, “20–35 percent of the daily calories should come from dietary fats.” A valid health claim for EPA and DHA-containing conventional foods and dietary supplements was recognized by the FDA in 2004. According to this health claim, “consumption of EPA and DHA omega-3 fatty acids may reduce the risk of coronary heart disease”; however, the evidence is supportive rather than convincing. Additionally, the FDA states that dietary supplement labels cannot suggest a daily dose of EPA and DHA greater than 2 g. According to the 2005 Dietary Guidelines, a healthy diet should contain fewer than 10% of calories from saturated fats and less than 300 mg of cholesterol daily. The Dietary Guidelines also stress that sources of polyunsaturated and monounsaturated fatty acids, such as fish, nuts and vegetable oils, should account for the majority of dietary fats and oils. Food producers are looking for many more chances to include omega-3 in their formulas as customers continue to demand more nutrient-dense goods [58].
Over the last 20 years, the FDA and other international regulatory bodies have assessed some DHA or DHA-rich oil sources for the possible inclusion of DHA in foods intended for human consumption. GRN 137 is one of the pertinent US GRAS notifications (FDA, 2008). Every GRAS notification included details and data from clinical studies to substantiate the suggested DHA constituents' safety for use in food intended for human consumption.
The FDA has approved the use of certain qualified health claims on the ability of foods and dietary supplements containing the omega-3 fatty acids, EPA and DHA, to lower blood pressure and lower the risk of hypertension and coronary heart disease. The ruling was issued in response to a petition that was brought in 2014 by the Global Organization for EPA and DHA Omega-3 (GOED) [59].
To lower the incidence of cardiovascular events in some patients with or at high risk for cardiovascular disease (CVD), the FDA authorized a new use for icosapent ethyl (Vascepa), a medication that is a highly refined version of eicosapentaenoic acid (EPA), an omega-3 fatty acid found in fish. The EPA/DHA brand-name Epanova from AstraZeneca and two generic versions, which all target hypertriglyceridemia (triglyceride levels of 500 mg/dL or greater), were authorized by the FDA. The FDA authorized two generic omega-3 EPA/DHA medications: Teva Pharmaceuticals' Omtryg (ANDA #091028) and TRYGG Pharma AS's Omtryg (NDA #204977), which is jointly owned by Lindsay Goldberg LLC and Aker BioMarine ASA [60].
It is not advised for nursing mothers to use DHA or EPA supplements, nevertheless, as these supplements can be extremely concentrated (up to six to fourteen times serum levels), with just 200–300 mg of DHA needed daily.
Omega-3 interactions with medications
Fish oil and other omega-3 dietary supplements interact with prescription drugs leading to adverse effects and hence should be consumed in consultation with a physician.
Ex: Coumadin, or warfarin, and comparable anticoagulants: Even though it seems to be less effective than aspirin, fish oil can show antiplatelet effects when taken in large doses. When used with warfarin, fish oil may cause longer clotting times, as seen by a higher international normalized ratio (INR). However, studies reported that dosages of 3–6 g/day of fish oil do not affect patients' anticoagulant status and the risk of hemorrhage that is clinically meaningful [61, 62].
Omega-3 deficiency
Dermatitis and rough scaly skin can result from a lack of critical fatty acids, specifically omega-3 s or omega-6 s. A deficiency of omega-3 fatty acids leads to a decrease in the concentration of DHA in the plasma and tissue. However, there are no established DHA or EPA cutoff doses beyond which functional endpoints related to immunological response, brain or visual function, or both are compromised [7].
Half-life
Maximum EPA and DHA plasma concentrations have been reported five to nine hours on oral administration, but unnoticeable until two weeks of regular dosage. The half-life of EPA is 37 h and that of DHA is 48 h when given repeatedly [62].
Omega-3 intakes
Based on data from the National Health and Nutrition Examination Survey (NHANES) conducted in 2011–2012, the majority of American adults and children ingest the recommended quantities of omega-3 fatty acids, or ALA. The average daily intake of ALA from food is 1.55 g for men and 1.32 g for females among children and teenagers aged 2–19. The average daily intake of ALA from food for adults (20 years of age and older) is 2.06 g for men and 1.59 g for women. The quantity of DHA and EPA that are obtained by food consumption makes up relatively little of the total daily intake of omega-3 fatty acids (approximately 40 mg for children and teenagers and around 90 mg for adults) [7].
Conclusion
The search for nutrients and supplements that can enhance health and quality of life is becoming more popular. Supplements and dietary plans like n − 3 PUFAs can lead to maximum therapeutic benefits, improved healing, lower risk of disease and elite performance in competition. ALA, EPA and DHA are the three primary forms of omega-3 fatty acids, which are a family of vital lipids that may be gained from food. Strategic dietary interventions and targeted supplementation with purified n − 3 PUFAs offer promising adjuvant therapeutic modalities for managing various chronic conditions. Their modulatory effects on inflammatory pathways, lipid profiles and cellular signaling mechanisms suggest potential applications in mitigating autoimmune disorders, neurodegenerative diseases, certain cancers and cardiovascular risk factors. Additionally, evidence points toward neuroprotective and vision-preserving properties, broadening the scope of their potential pharmacological interventions. Future research should focus on dose optimization, personalized treatment plans and robust clinical trials to fully elucidate the therapeutic potential of Omega-3 PUFAs. This review underscores the pharmacological potential of omega-3 and its vital role in providing optimal health.
Availability of data and materials
Not applicable.
Abbreviations
- EPA:
-
Eicosapentaenoic acid
- DHA:
-
Docosahexaenoic acid
- ALA:
-
Alpha-linolenic acid
- PUFAs:
-
High polyunsaturated fatty acids
- OM3FAs:
-
Omega-3 fatty acids
- LPL:
-
Lipo-protein-lipase
- PPARs:
-
Peroxisome proliferator-activated receptors
- CAT 1:
-
Carnitine acetyl transferase 1
- GPRs:
-
G Protein-coupled receptors
References
Theinel MH, Nucci MP, Alves AH, Dias OFM, Mamani JB, Garrigós MM, Oliveira FA, Rego GNA, Valle NME, Cianciarullo G, Gamarra LF (2023) The effects of omega-3 polyunsaturated fatty acids on breast cancer as a preventive measure or as an adjunct to conventional treatments. Nutrients 15:1310. https://doi.org/10.3390/nu15061310
Sharifi E, Yazdani Z, Najafi M, Hosseini-khah Z, Jafarpour A, Rafiei A (2022) The combined effect of fish oil containing omega-3 fatty acids and Lactobacillus plantarum on colorectal cancer. Food Sci Nutr 10:4411–4418. https://doi.org/10.1002/fsn3.3037
Liang P, Henning SM, Guan J, Grogan T, Elashoff D, Cohen P, Aronson WJ (2020) Effect of dietary omega-3 fatty acids on castrate-resistant prostate cancer and tumor-associated macrophages. Prostate Cancer Prostatic Dis 23:127–135. https://doi.org/10.1038/s41391-019-0168-8
Simopoulos AP (2008) The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med 233:674–688. https://doi.org/10.3181/0711-MR-311
Ratanabanangkoon P, Guzman H, Almarsson O, Berkovitz D, Tokarcyzk S, Straughn AB, Chen H (2008) A high-throughput approach towards a novel formulation of fenofibrate in omega-3 oil. Eur J Pharm Sci 33:351–360. https://doi.org/10.1016/j.ejps.2008.01.005
Elagizi A, Lavie CJ, O’Keefe E, Marshall K, O’Keefe JH, Milani RV (2021) An update on omega-3 polyunsaturated fatty acids and cardiovascular health. Nutrients 13:204. https://doi.org/10.3390/nu13010204
The Nutrition Source. Omega-3 fatty acids: an essential contribution [Internet]. 2023 [cited 2024 Jun 27]. Available from: https://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/fats-and-cholesterol/types-of-fat/omega-3-fats/
Djuricic I, Calder PC (2021) Beneficial outcomes of omega-6 and omega-3 polyunsaturated fatty acids on human health: an update for 2021. Nutrients 13:2421. https://doi.org/10.3390/nu13072421
Wikipedia contributors. Omega-3 fatty acid [Internet]. Wikipedia. 2024 [cited 2024 Jun 27]. Available from: https://en.wikipedia.org/wiki/Omega-3_fatty_acid
Tur JA, Bibiloni MM, Sureda A, Pons A (2012) Dietary sources of omega 3 fatty acids: public health risks and benefits. Br J Nutr 107:S23–S52. https://doi.org/10.1017/S0007114512001456
Office of Dietary Supplements. Omega-3 fatty acids [Internet]. [Cited 2024 Jun 27]. Available from: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/
Miller MR, Nichols PD, Carter CG (2008) Omega 3 Oil sources for use in aquaculture—alternatives to the unsustainable harvest of wild fish. Nutr Res Rev 21:85–96. https://doi.org/10.1017/S0954422408102414
Davidson MH, Kling D, Maki KC (2011) Novel developments in omega-3 fatty acid-based strategies. Curr Opin Lipidol 22:437–444. https://doi.org/10.1097/MOL.0b013e32834bd642
Ms FH. 12 foods that are very high in omega-3 [Internet]. Healthline (2023) Available from: https://www.healthline.com/nutrition/12-omega-3-rich-foods#1.-Mackerel-(4,580-mg-per-serving)
Cunningham E (2012) Are krill oil supplements a better source of n-3 fatty acids than fish oil supplements. J Acad Nutr Diet 112:344. https://doi.org/10.1016/j.jand.2011.12.016
Calder PC (2013) Omega-3 polyunsaturated fatty acids and inflammatory processes: nutrition or pharmacology. Br J Clin Pharmacol 75:645–662. https://doi.org/10.1111/j.1365-2125.2012.04374.x
Backes J, Anzalone D, Hilleman D, Catini J (2016) The clinical relevance of omega-3 fatty acids in the management of hypertriglyceridemia. Lipids Health Dis 15:118. https://doi.org/10.1186/s12944-016-0286-4
Noreen EE, Sass MJ, Crowe ML, Pabon VA, Brandauer J, Averill LK (2010) Effects of supplemental fish oil on resting metabolic rate, body composition, and salivary cortisol in healthy adults. J Int Soc Sports Nutr. https://doi.org/10.1186/1550-2783-7-31
Bays HE, Tighe AP, Sadovsky R, Davidson MH (2008) Prescription omega-3 fatty acids and their lipid effects: physiologic mechanisms of action and clinical implications. Expert Rev Cardiovasc Ther 6:391–409. https://doi.org/10.1586/14779072.6.3.391
Logan SL, Spriet LL (2015) Omega-3 fatty acid supplementation for 12 weeks increases resting and exercise metabolic rate in healthy community-dwelling older females. PLoS ONE 10:e0144828. https://doi.org/10.1371/journal.pone.0144828
Seo T, Blaner WS, Deckelbaum RJ (2005) Omega-3 fatty acids: molecular approaches to optimal biological outcomes. Curr Opin Lipidol 16:11–18. https://doi.org/10.1097/00041433-200502000-00004
Kota B, Huang T, Roufogalis B (2005) An overview on biological mechanisms of PPARs. Pharmacol Res 51:85–94. https://doi.org/10.1016/j.phrs.2004.07.012
Nabavi SF, Bilotto S, Russo GL, Orhan IE, Habtemariam S, Daglia M, Devi KP, Loizzo MR, Tundis R, Nabavi SM (2015) Omega-3 polyunsaturated fatty acids and cancer: lessons learned from clinical trials. Cancer Metastasis Rev 34:359–380. https://doi.org/10.1007/s10555-015-9572-2
Ishihara T, Yoshida M, Arita M (2019) Omega-3 fatty acid-derived mediators that control inflammation and tissue homeostasis. Int Immunol 31:559–567. https://doi.org/10.1093/intimm/dxz001
Svensson RU et al (2016) Inhibition of acetyl-CoA carboxylase suppresses fatty acid synthesis and tumour growth of non-small-cell lung cancer in preclinical models. Nat Med 22:1108–1119. https://doi.org/10.1038/nm.4181
Chew EY, Clemons TE, Agrón E, Launer LJ, Grodstein F, Bernstein PS (2015) Effect of omega-3 fatty acids, lutein/zeaxanthin, or other nutrient supplementation on cognitive function. JAMA 314:791. https://doi.org/10.1001/jama.2015.9677
Lim W, Gammack J, Van Niekerk J, Dangour A (2005) Omega 3 fatty acid for the prevention of dementia. In: Lim W-S (ed) Cochrane database syst rev. John Wiley & Sons Ltd, Chichester, UK. https://doi.org/10.1002/14651858.CD005379
Tully AM, Roche HM, Doyle R, Fallon C, Bruce I, Lawlor B, Coakley D, Gibney MJ (2003) Low serum cholesteryl ester-docosahexaenoic acid levels in Alzheimer’s disease: a case–control study. Br J Nutr 89:483–489. https://doi.org/10.1079/BJN2002804
SanGiovanni JP, Chew EY (2005) The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog Retin Eye Res 24:87–138. https://doi.org/10.1016/j.preteyeres.2004.06.002
Sakamoto A, Saotome M, Iguchi K, Maekawa Y (2019) Marine-derived omega-3 polyunsaturated fatty acids and heart failure: current understanding for basic to clinical relevance. Int J Mol Sci 20:4025. https://doi.org/10.3390/ijms20164025
Nodari S, Metra M, Milesi G, Manerba A, Cesana BM, Gheorghiade M, Dei Cas L (2009) The role of n-3 PUFAs in preventing the arrhythmic risk in patients with idiopathic dilated cardiomyopathy. Cardiovasc Drugs Ther 23:5–15. https://doi.org/10.1007/s10557-008-6142-7
London B, Albert C, Anderson ME et al (2007) Omega-3 fatty acids and cardiac arrhythmias: prior studies and recommendations for future research. Circulation. https://doi.org/10.1161/CIRCULATIONAHA.107.712984
Albert CM (1998) Fish consumption and risk of sudden cardiac death. JAMA 279:23. https://doi.org/10.1001/jama.279.1.23
AbuMweis S, Jew S, Tayyem R, Agraib L (2018) Eicosapentaenoic acid and docosahexaenoic acid containing supplements modulate risk factors for cardiovascular disease: a meta-analysis of randomised placebo-control human clinical trials. J Hum Nutr Diet 31:67–84. https://doi.org/10.1111/jhn.12493
Zhang AC, Singh S, Craig JP, Downie LE (2020) Omega-3 fatty acids and eye health: opinions and self-reported practice behaviors of optometrists in Australia and New Zealand. Nutrients 12:1179. https://doi.org/10.3390/nu12041179
Bhargava R, Pandey K, Ranjan S, Mehta B, Malik A (2023) Omega-3 fatty acids supplements for dry eye—Are they effective or ineffective. Indian J Ophthalmol 71:1619–1625. https://doi.org/10.4103/IJO.IJO_2789_22
McDaniel JC, Rausch J, Tan A (2020) Impact of omega-3 fatty acid oral therapy on healing of chronic venous leg ulcers in older adults: Study protocol for a randomized controlled single-center trial. Trials 21:93. https://doi.org/10.1186/s13063-019-3970-7
Coderre TJ (2008) Spinal cord mechanisms of hyperalgesia and allodynia. The senses: a comprehensive reference. Elsevier, Netherlands, pp 339–380. https://doi.org/10.1016/B978-012370880-9.00168-7
Silva RV, Oliveira JT, Santos BLR, Dias FC, Martinez AMB, Lima CKF, Miranda ALP (2017) Long-chain omega-3 fatty acids supplementation accelerates nerve regeneration and prevents neuropathic pain behavior in mice. Front Pharmacol. https://doi.org/10.3389/fphar.2017.00723
Unda SR, Villegas EA, Toledo ME, AsisOnell G, Laino CH (2020) Beneficial effects of fish oil enriched in omega-3 fatty acids on the development and maintenance of neuropathic pain. J Pharm Pharmacol 72:437–447. https://doi.org/10.1111/jphp.13213
Galan Arriero I, Serrano-Munoz D, Gómez-Soriano J, Goicoechea C, Taylor J, Velasco A (2017) The role of omega-3 and omega-9 fatty acids for the treatment of neuropathic pain after neurotrauma. Biochim et Biophys Acta (BBA) - Biomembranes 1859:1629–1635. https://doi.org/10.1016/j.bbamem.2017.05.003
NaPier Z, Kanim LEA, Arabi Y, Salehi K, Sears B, Perry M et al (2019) Omega-3 fatty acid supplementation reduces intervertebral disc degeneration. Med Sci Monit 25:9531–9537. https://doi.org/10.12659/MSM.918649
Chong EW-T (2008) Dietary ω-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration. Arch Ophthalmol 126:826. https://doi.org/10.1001/archopht.126.6.826
Ishak WMW, Katas H, Yuen NP, Abdullah MA, Zulfakar MH (2019) Topical application of omega-3-, omega-6-, and omega-9-rich oil emulsions for cutaneous wound healing in rats. Drug Deliv Transl Res 9:418–433. https://doi.org/10.1007/s13346-018-0522-8
Garcia Lopez S, Villanueva Arriaga RE, Nájera Medina O, Rodríguez López CP et al (2016) one month of omega-3 fatty acid supplementation improves lipid profiles, glucose levels and blood pressure in overweight schoolchildren with metabolic syndrome. J Pediatr Endocrinol Metab. https://doi.org/10.1515/jpem-2015-0324
Bernardi JR, Escobar RS, Ferreira CF, Silveira PP (2012) Fetal and neonatal levels of omega-3: effects on neurodevelopment, nutrition, and growth. Sci World J. https://doi.org/10.1100/2012/202473
Nevins JEH, Donovan SM, Snetselaar L, Dewey KG, Novotny R (2021) Omega-3 fatty acid dietary supplements consumed during pregnancy and lactation and child neurodevelopment: a systematic review. J Nutr 151:3483–3494. https://doi.org/10.1093/jn/nxab238
Shen SC, Gong C, Jin KQ, Zhou L, Xiao Y, Ma L (2022) Omega-3 fatty acid supplementation and coronary heart disease risks: a meta-analysis of randomized controlled clinical trials. Front Nutr. https://doi.org/10.3389/fnut.2022.809311
Dong Y, Zhu H, Chen L, Huang Y, Christen W, Cook NR, Copeland T, Mora S, Buring JE, Lee IM, Costenbader KH, Manson JAE (2022) Effects of vitamin D3 and marine omega-3 fatty acids supplementation on biomarkers of systemic inflammation: 4-year findings from the VITAL randomized trial. Nutrients. https://doi.org/10.3390/nu14245307
Arab-Tehrany E, Jacquot M, Gaiani C, Imran M, Desobry S, Linder M (2012) Beneficial effects and oxidative stability of omega-3 long-chain polyunsaturated fatty acids. Trends Food Sci Technol 25:24–33. https://doi.org/10.1016/j.tifs.2011.12.002
Jensen HA, Sørensen A-DM, Hansen LT, Bøknæs N, Mejlholm O, Jacobsen C (2023) Effect of artificial light on the lipid oxidation of whole, cooked Northern shrimp (Pandalus borealis) during frozen storage. Food Chemistry Advances 3:100369. https://doi.org/10.1016/j.focha.2023.100369
Bremmell KE, Briskey D, Meola TR, Mallard A, Prestidge CA, Rao A (2020) A self-emulsifying omega-3 ethyl ester formulation (AquaCelle) significantly improves eicosapentaenoic and docosahexaenoic acid bioavailability in healthy adults. Eur J Nutr 59:2729–2737. https://doi.org/10.1007/s00394-019-02118-x
Alhakamy NA, Aldawsari HM, Hosny KM, Ahmad J, Akhter S, Kammoun AK, Alghaith AF, Asfour HZ, Al-Rabia MW, Md S (2020) Formulation design and pharmacokinetic evaluation of docosahexaenoic acid containing self-nanoemulsifying drug delivery system for oral administration. Nanomater Nanotechnol 10:184798042095098. https://doi.org/10.1177/1847980420950988
Castejon N, Luna P, Senorans FJ (2021) Microencapsulation by spray drying of omega-3 lipids extracted from oilseeds and microalgae: effect on polyunsaturated fatty acid composition. LWT 148:111789. https://doi.org/10.1016/j.lwt.2021.111789
Hamed S, Elshafei K, El-Sayed H, Abo-Elwafa G, Afifi S, Zahran H (2020) Formulation of multi-functional omega-3 oil rich microcapsules by spray drying methodology. Egypt J Chem. https://doi.org/10.21608/ejchem.2020.43946.2891
Jagtap AA, Badhe YS, Hegde MV, Zanwar AA (2021) Development and characterization of stabilized omega-3 fatty acid and micronutrient emulsion formulation for food fortification. J Food Sci Technol 58:996–1004. https://doi.org/10.1007/s13197-020-04614-z
Sreedhar R, Kumar VS, Bhaskaran Pillai AK, Mangalathillam S (2019) Omega-3 fatty acid based nanolipid formulation of atorvastatin for treating hyperlipidemia. Adv Pharm Bull 9:271–280. https://doi.org/10.15171/apb.2019.031
Oklahoma State University. Foods, health and omega-3 oils [Internet] (2017) Available from: https://extension.okstate.edu/fact-sheets/foods-health-and-omega-3-oils.html
GRAS Notice 000732: Docosahexaenoic acid oil produced in Schizochytrium sp. | FDA [Internet]. Available from: https://www.fda.gov/media/112824
Harvard Health (2020) FDA approves fish oil-based drug for heart attack and stroke prevention [Internet]. Harvard Health. Available from: https://www.health.harvard.edu/heart-health/fda-approves-fish-oil-based-drug-for-heart-attack-and-stroke-prevention
Grebow J (2020) FDA approves three more omega-3 drugs. Is this good or bad news for supplements? Nutr Outlook [Internet]. 2020 Nov 15. Available from: https://www.nutritionaloutlook.com/view/fda-approves-three-more-omega-3-drugs-good-or-bad-news-supplements
Wachira JK, Larson MK, Harris WS (2014) n-3 Fatty acids affect haemostasis but do not increase the risk of bleeding: clinical observations and mechanistic insights. Br J Nutr 111:1652–1662. https://doi.org/10.1017/S000711451300425X
Acknowledgements
The authors express their gratitude to KLE College of Pharmacy, Belagavi, for providing a conducive study environment and ongoing encouragement.
Funding
This review did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the review, for collection of data, and while manuscript preparation. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
Authors do not have any conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Patted, P.G., Masareddy, R.S., Patil, A.S. et al. Omega-3 fatty acids: a comprehensive scientific review of their sources, functions and health benefits. Futur J Pharm Sci 10, 94 (2024). https://doi.org/10.1186/s43094-024-00667-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-024-00667-5