
Abstract
Background
Hoffa's fat pad is an intra-capsular extra-sinovial structure of the knee joint that has a significant biomechanical and metabolic role, minimizing the influence of stresses created by loading and generating cytokines. Changes in its size can lead to variations in the homeostasis of the knee in elderly patients. This work intends to assess the dimensional variations of Hoffa's fat pad associated to aging in both sexes, using MRI sagittal sequences acquired from the OAI (Osteoarthritis Initiative) database.
Methods
We examined the Hoffa's fat pad sagittal thickness in 217 men and women with knee osteoarthritis who were grouped into four age groups for the study: 40–49; 50–59; 60–69; and 70–80. 3T sagittal IW 2D TSE Fat-suppressed MRI sequences, taken from the OAI (Osteoarthritis Initiative) database, were examined.
Results
Hoffa’s fat pad thickness was shown to differ significantly between groups in both men and women, decreasing in the older individuals' groups (R = − 0.46; p 0.0001). By dividing the patients into ten-year age groups and by sex, the thickness of both the right knee and the left knee was examined. In fact, the average thickness of Hoffa's fat pad of the right knee was reported to be, in males, 33.6+/− 3 mm in subjects aged between 40 and 49 years, 31+/− 2.4 mm for patients aged between 50 and 59, 30.3 ± 1.8 mm in the group between 60 and 69 years and 28.7+/− 1.8 mm between 70 and 80 years. In women the values obtained were the following: 29+/− 1.6 mm between 40 and 49 years; 28.9+/− 2.6 mm in the group between 50 and 59 years, 25.3+/− 1.9 mm for patients aged 60 and 69 years and 26+/− 2 mm between 70 and 80 years. Similar results were obtained for the left knee.
Conclusions
Hoffa’s fat pad gradually thins with aging in both male and female patients with knee osteoarthritis, and this can be detected by evaluating the thickness of the fat pad on sagittal MRI sequences.
Similar content being viewed by others


Background
The knee is the most commonly afflicted peripheral joint by OA, resulting in progressive loss of function, discomfort, stiffness, and persistent impairment [1].
The frequency of OA of the knee rises with aging and it is higher in people aged 70 to 74 [2, 3].
Hoffa’s fat pad, also known as infrapatellar fat pad (IPFP), is a distinctive intra-articular, though extra-synovial, structure of the knee, that is situated near to the synovium [4, 5].
IPFP is anatomically made up of subcutaneous fat-like adipose tissue [6] and it has a significant biomechanical function in minimizing the effects of load-generated pressures on the knee joint [7, 8].
In recent years, IPFP has emerged as having a new role in knee osteoarthritis (OA). Knee osteoarthritis, in fact, can be considered a disease of the entire joint, involving not only cartilage but also the meniscus, the subchondral bone, the synovial membrane and the infrapatellar fat pad [9].
For these reasons, morphological measurements of IPFP have recently sparked interest in scientific study as prospective biomarkers for investigating the physiology of healthy tissues, structure–function interactions, and size changes associated with obesity and OA. In some papers, larger IPFP sizes have been linked to decreased knee pain and a lower risk of cartilage deterioration [10]. Indeed, there are correlations between quantitative cartilage and Hoffa's fat pad morphological alterations, implying that IPFP volume is deleterious to cartilage deterioration. However, a larger amount of IPFP was seen in persons with symptomatic and radiographic OA of the knee compared to asymptomatic controls with no radiographic evidence of OA [11].
MRI is a fundamental tool for the study of knee osteoarthritis, and in particular, for the quantitative and qualitative evaluation of the Hoffa fat pad, as it has signal characteristics that differentiate it from adjacent structures.
Indeed, IPFP signal intensity in MRI in OA patients was found to be substantially connected with knee structural abnormalities (such as knee cartilage volume) [12, 13]. A study on the elderly before the onset of knee OA discovered that changes in IFP signal intensity were related to the abnormal structure of the knee joint and clinical symptoms cross-sectionally and longitudinally, implying that IFP signal intensity is an important imaging marker of knee OA.
Given the link between IPFP volume and knee OA, an age-related joint illness, this study aims to use sagittal MRI sequences to assess the dimensional changes of the Hoffa fat pad to aging in both sexes.
Methods
Data source and subjects
Data used in this paper were obtained from the Osteoarthritis Initiative (OAI) database. OAI is a multi-center, longitudinal cohort study on knee OA carried out by four American sites (the Ohio State University, Memorial Hospital of Rhode Island, the University of Pittsburgh, University of Maryland and Johns Hopkins University) which recruited patients between February 2004 and May 2006 (Fig. 1).

Infrapatellar fat pad in the knee joint
In this study, 217 patients (108 men and 109 women) between the ages of 40 and 79 were divided into four groups according to their decade of age (40–49 years; 50–59 years; 60–69 years; 70–79 years), and the sagittal thickness of the Hoffa's fat pad was examined in each group.
Image acquisition and analysis
Images were acquired using a 3T Magnetom Trio magnet (Siemens Healthcare Erlangen, Germany) and a quadrature knee coil. The thickness of IPFP was determined using a sagittal intermediate-weighted fat-suppressed turbo spin-echo sequence, IW TSE (time of repetition = 3200 ms, time of echo = 30 ms, slice thickness 3.0 mm; in plane resolution 0.36 mm × 0.36 mm). To get the optimum contrast between the IPFP and surrounding tissue in each image, brightness, intensity, contrast, and gray value restrictions were adjusted.
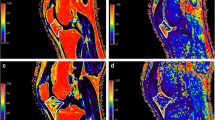
The maximal sagittal thickness (depth) of IPFP, from the anterior to posterior surface, was manually measured for each patient, both for the right knee and for the left knee, drawing a line perpendicular to the patellar tendon, as published in our previous work [14] (Figs. 2, 3).

MRI image of Infrapatellar fat pad in the knee joint

Measurement of IPFP sagittal thickness (for this figure, all the authors Giovanni Ricatti, Nicola Veronese, Ilaria Gangai, Mariateresa Paparella, Valentina Testini, Giuseppe Guglielmi have given the permission to publish this figure for both the print and online format. This figure is present in the article Ricatti G, Veronese N, Gangai I, Paparella M, Testini V, Guglielmi G. Hoffa's fat pad thickness: a measurement method with sagittal MRI sequences. Radiol Med. 2021 Jun;126(6):886–893. https://doi.org/10.1007/s11547-021-01345-9. Epub 2021 Mar 27. PMID: 33,772,711; PMCID: PMC8154775
Two distinct blinded observers with a combined 3 years of experience conducted all of these measurements; the intra-observer and inter-observer reliability were assessed in our prior study [14].
Statistical analysis
After ensuring that the continuous variables were normal, they were evaluated in terms of means and standard deviation (SD). For categorical relative frequencies (%) were reported. For examining probable gender associations, parametric univariate tests (p-values referenced to Fisher exact for frequencies and t-test for means) were performed. In order to assess whether IPFP sagittal thickness, across all participants (men and women), was related to age we used an ANOVA (Analysis of Variance) test, while the p-values were reported as p for trend.
Finally, the association between age and IPFP sagittal thickness was analyzed using a simple linear correlation analysis.
All analyses were performed using the SPSS 20.0 for Windows (SPSS Inc., Chicago, Illinois). All statistical tests were two-tailed, and statistical significance was assumed for a p-value < 0.05.
Results
Overall, 217 individuals (108 males and 109 females) aging a mean of 57.3 years (SD: 10.4; range: 40–79) were included. The subjects performed MRI of both knees.
Hoffa's fat pad thickness was observed to differ significantly between males and females for both knees, being significantly higher in males compared to females (p < 0.0001).
Table 1 shows the mean thickness of Hoffa's fat pad by gender: at the right knee, in males, this parameter was 33.62 ± 3.00 mm in subjects aged between 40 and 49 years vs. 28.67 ± 1.76 mm in those aging more than 70 years (p for trend < 0.0001). A similar finding was present for left knee. In females aged between 40 and 49 years, the mean thickness of Hoffa’s fat pad was 29.00 ± 1.64 mm vs. 25.96 ± 1.96 mm in females older than 70 years. A similar trend was observed for left knee (Table 1).
Using a linear correlation analysis, increasing age was associated with a significant decline in mean thickness of Hoffa's fat pad at both knees (R = -0.46; p < 0.0001).
Discussion
Knee osteoarthritis is a complex, painful and disabling pathology. Although patient education, exercises, a change in lifestyle and analgesics should all be included in the initial course of treatment, total joint replacement with an arthroplasty is currently the only successful option for patients with clinically disabling knee osteoarthritis [15]. Since the life expectancy of the population is constantly increasing, the prevalence of knee osteoarthritis is also destined to grow in the next years, as this disease is closely related to aging [16]. Therefore, the understanding of the etiopathogenesis of OA and in particular of the pain mechanisms represents a priority objective for identifying new therapeutic targets, in particular in order to manage pain induced by knee osteoarthritis. It is understood that Hoffa's fat pad serves as a local source of inflammatory mediators, including a range of cytokines and adipokines, including leptin and adiponectin [17,18,19,20,21].
It was also observed that patients with advanced OA had a high degree of fibrosis of Hoffa's body, a process related to the fact that fibrosis can aid repair in the healing process of tissues after injury [22]. Indeed, some studies have evaluated the possible correlation in the increase in IPFP fibrosis and the degree of joint damage [21, 23].
Furthermore, the activation of the inflammatory process also plays an essential role in painful symptoms: in fact, patients with KOA (knee osteoarthritis) who have an increased IPFP volume tend to have symptomatic OA [24, 25]. In individuals with KOA, particular cartilage autoantigens produced can activate immune cells, which then secrete a variety of cytokines and adipokines in response to the local inflammatory state [26].
MRI is essential for getting quantitative information on IPFP in patients with OA, providing direct proof of IPFP involvement in the etiology of KOA.
With our study, we would like to demonstrate a correlation between dimensional variations of the IPF and aging. Moreover, also another study showed a decrease in IPFP volume in moderate and end-stage OA compared to controls as well as a difference in IPFP hypointense signal [36]. Surprisingly, no variation in suprapatellar fat pad was identified between groups, suggesting IPFP's unique involvement in OA [27]. Additionally, it appears that a higher maximum sagittal cross-sectional area of the Hoffa's fat pad is beneficial for avoiding structural alterations and knee pain [25, 28, 29].
However, this constitutes only a starting point for further assessments that may be addressed in the future in other studies, such as the relationship between the serum level of cytokines and adipokines and the size and signaling characteristics of IPFP in MRI; how the characteristics of IPFP in MRI are correlated with the symptoms of OA, even after drug therapy; how MRI features of IPFP can represent an early marker of OA development.
The role of MRI is and will therefore be fundamental not only for the diagnosis of osteoarthritis, but also for the follow-up during therapy and for the prevention of the pathology, being able to also use it as a screening in patients at risk.
Limitations of this study are that it is the retrospective, the limited number of operators (only 2); moreover, the study only included patients with knee osteoarthritis; consequently, it could be valuable in future studies to compare the dimensional variations of Hoffa's fat pad between osteoarthritic and healthy patients.
Conclusions
The study shows that with aging Hoffa’s fat pad, for both male and female patients affected by knee osteoarthritis, undergoes a progressive thinning, detectable by measuring its thickness on sagittal MRI sequences.
This work represents a start point for further studies in the future: the mechanisms underlying the role of Hoffa's fat pad in the symptoms of knee osteoarthritis and in the degenerative processes of articular cartilage; the association between serum levels of various adipokines and the properties of Hoffa's fat pad as measured by MRI; how the characteristics of Hoffa's fat pad on MRI change after therapeutic interventions for osteoarthritis; whether the characteristics of Hoffa's fat pad can be used as a biomarker for imaging of knee osteoarthritis in general; and whether local fatty tissues in other joints are related to joint pain.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- OAI:
-
Osteoarthritis initiative
- OA:
-
Osteoarthritis
- IPFP:
-
Infrapatellar fat pad
- TSE:
-
Turbo spin echo
- KOA:
-
Knee osteoarthritis
References
Hussain SM, Neilly DW, Baliga S, Patil S, Meek R (2016) Knee osteoarthritis: a review of management options. Scott Med J 61(1):7–16
Michael JW, Schlüter-Brust KU, Eysel P (2010) The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arztebl Int 107(9):152–162
de Lange-Brokaar BJ, Ioan-Facsinay A, van Osch GJ, Zuurmond AM, Schoones J, Toes RE, et al. Synovial inflammation, immune cells and their cytokines in osteoarthritis: a review. Osteoarthritis Cartilage 2012;20:1484e99.
Saddik D, McNally EG, Richardson M. MRI of Hoffa’s fat pad. Skeletal Radiol 2004;33:433e44.
Gallagher J, Tierney P, Murray P, O’Brien M (2005) The infrapatellar fat pad: anatomy and clinical correlations. Knee Surg Sports Traumatol Arthrosc 13:268–272
Clockaerts S, Bastiaansen-Jenniskens YM, Runhaar J, Van Osch GJ, Van Offel JF, Verhaar JA, et al. The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: a narrative review. Osteoarthritis Cartilage 2010;18:876e82.
Han W, Cai S, Liu Z, Jin X, Wang X, Antony B, Cao Y, Aitken D, Cicuttini F, Jones G, Ding C (2014) Infrapatellar fat pad in the knee: Is local fat good or bad for knee osteoarthritis? Arthritis Res Ther 16:R145
Maurel B, Le Corroller T, Cohen M, Acid S, Bierry G, Parratte S, Flecher X, Argenson JN, Petit P, Champsaur P (2010) Infrapatellar fat pad: anterior crossroads of the knee. J Radiol 91:841–855
Belluzzi E, Stocco E, Pozzuoli A, Granzotto M, Porzionato A, Vettor R, De Caro R, Ruggieri P, Ramonda R, Rossato M, Favero M, Macchi V (2019) Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. Biomed Res Int 31(2019):6390182
Masaki T, Takahashi K, Hashimoto S, Ikuta F, Watanabe A, Kiuchi S, Okuaki T, Mochizuki Y, Takai S (2019) Volume change in infrapatellar fat pad is associated not with obesity but with cartilage degeneration. J Orthop Res 37(3):593–600
Sallie M Cowan, Harvi F Hart et al. Infrapatellar fat pad volume is greater in individuals with patellofemoral joint osteoarthritis and associated with pain. Rheumatol Int. 2015;35(8):1439–42.
Han W, Aitken D, Zheng S, Wluka A et al (2019) Association between quantitatively measured infrapatellar fat pad high signal-intensity alteration and magnetic resonance imaging-assessed progression of knee osteoarthritis. Arthritis Care Res 71:638–646
Wang K, Ding C, Hannon MJ, Chen Z, Kwoh CK, Lynch J et al (2018) Signal intensity alteration within infrapatellar fat pad predicts knee replacement within 5 years: data from the osteoarthritis initiative. Osteoarthritis Cartilage 26:1345–1350
Ricatti G, Veronese N et al (2021) Hoffa’s fat pad thickness: a measurement method with sagittal MRI sequences. Radiol Med (Torino) 126:886–893
Khan M, Adili A, Winemaker M, Bhandari M (2018) Management of osteoarthritis of the knee in younger patients. CMAJ 190(3):E72–E79
Felson DT (1988) Epidemiology of hip and knee osteoarthritis. Epidemiol Rev 10:1–28
Hui W, Litherland GJ, Elias MS, Kitson GI, Cawston TE, Rowan AD, Young DA (2012) Leptin produced by joint white adipose tissue induces cartilage degradation via upregulation and activation of matrix metalloproteinases. Ann Rheum Dis 71:455–462
Klein-Wieringa IR, Kloppenburg M, Bastiaansen-Jenniskens YM, Yusuf E, Kwekkeboom JC, El-Bannoudi H, Nelissen RGHH, Zuurmond A, Stojanovic-Susulic V, Van Osch GJVM, Toes REM, Ioan-Facsinay A (2011) The infrapatellar fat pad of patients with osteoarthritis has an inflammatory phenotype. Ann Rheum Dis 70:851–857
Gandhi R, Takahashi M, Virtanen C, Syed K, Davey JR, Mahomed NN (2011) Microarray analysis of the infrapatellar fat pad in knee osteoarthritis: relationship with joint inflammation. J Rheumatol 38:1966–1972
Eymard F, Pigenet A, Citadelle D, Tordjman J, Foucher L, Rose C, Flouzat Lachaniette CH, Rouault C, Clément K, Berenbaum F, Chevalier X, Houard X (2017) Knee and hip intra-articular adipose tissues (IAATs) compared with autologous subcutaneous adipose tissue: a specific phenotype for a central player in osteoarthritis. Ann Rheum Dis 76(6):1142–1148. https://doi.org/10.1136/annrheumdis-2016-210478
Chang J, Liao Z, Lu M, Meng T, Han W, Ding C (2018) Systemic and local adipose tissue in knee osteoarthritis. Osteoarthritis Cartilage 26(7):864–871. https://doi.org/10.1016/j.joca.2018.03.004
Ioan-Facsinay A, Kloppenburg M (2013) An emerging player in knee osteoarthritis: the infrapatellar fat pad. Arthritis Res Ther 15(6):225. https://doi.org/10.1186/ar4422.PMID:24367915
Ioan-Facsinay A, Kloppenburg M (2017) Osteoarthritis: inflammation and fibrosis in adipose tissue of osteoarthritic joints. Nat Rev Rheumatol 13(6):325–326. https://doi.org/10.1038/nrrheum.2017.53
Chuckpaiwong B, Charles HC, Kraus VB, Guilak F, Nunley JA (2010) Age-associated increases in the size of the infrapatellar fat pad in knee osteoarthritis as measured by 3T MRI. J Orthop Res 28:1149–1154
Pan F, Han W, Wang X, Liu Z, Jin X, Antony B, Cicuttini F, Jones G, Ding C (2015) A longitudinal study of the association between infrapatellar fat pad maximal area and changes in knee symptoms and structure in older adults. Ann Rheum Dis 74:1818–1824
Zeng N, Yan ZP, Chen XY, Ni GX (2020) Infrapatellar fat pad and knee osteoarthritis. Aging Dis 11(5):1317–1328
Fontanella CG, Belluzzi E, Rossato M, Olivotto E, Trisolino G, Ruggieri P, Rubini A, Porzionato A, Natali A, De Caro R, Vettor R, Ramonda R, Macchi V, Favero M (2019) Quantitative MRI analysis of infrapatellar and suprapatellar fat pads in normal controls, moderate and end-stage osteoarthritis. Ann Anat 221:108–114. https://doi.org/10.1016/j.aanat.2018.09.007
Cowan SM, Hart HF, Warden SJ, Crossley KM (2015) Infrapatellar fat pad volume is greater in individuals with patellofemoral joint osteoarthritis and associated with pain. Rheumatol Int 35:1439–1442
Teichtahl AJ, Wulidasari E, Brady SRE, Wang Y, Wluka AE, Ding C, Giles GG, Cicuttini FM (2015) A large infrapatellar fat pad protects against knee pain and lateral tibial cartilage volume loss. Arthritis Res Ther 17:318
Acknowledgements
None.
Funding
The authors received no financial sponsors or other funding for this research.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material collection was performed by VT, GR and MTP. Data analysis was performed by NV. All authors (VT, NV, GR, MTP and GG) participated in the writing of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent to publish was obtained from study participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Testini, V., Veronese, N., Ricatti, G. et al. Dimensional changes of Hoffa’s fat pad related to aging: evaluation by MRI. Egypt J Radiol Nucl Med 55, 15 (2024). https://doi.org/10.1186/s43055-023-01177-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01177-9