
Abstract
Introduction
Recent studies regarding the infrapatellar fat pad (IPFP) mainly focus on the roles of the cells derived from the IPFP. There have been few clinical or epidemiological studies reporting on the association between the IPFP and knee osteoarthritis (OA). Our objective is to generate hypotheses regarding the associations between IPFP maximum area and knee OA measures in older adults.
Methods
A total of 977 subjects between 50 and 80 years of age (mean, 62.4 years) participated in the study. Radiographic knee osteophyte and joint space narrowing (JSN) were assessed using the Osteoarthritis Research Society International atlas. T1- or T2-weighted fat suppressed magnetic resonance imaging (MRI) was utilized to assess IPFP maximum area, cartilage volume, cartilage defects, and bone marrow lesions (BMLs). Knee pain was assessed by self-administered Western Ontario McMaster Osteoarthritis Index (WOMAC) questionnaire.
Results
After adjustment for potential confounders, IPFP maximum area was significantly associated with joint space narrowing (odds ratio (OR): 0.75, 95% confidence interval (CI): 0.62 to 0.91 (medial), 0.77, 95% CI: 0.62 to 0.96 (lateral)) and medial osteophytes (OR: 0.52, 95% CI: 0.35 to 0.76), knee tibial and patellar cartilage volume (β: 56.9 to 164.9 mm3/cm2, all P <0.001), tibial cartilage defects (OR: 0.58, 95% CI: 0.41 to 0.81 (medial), 0.53, 95% CI: 0.40-0.71 (lateral)), any BMLs (OR: 0.77, 95% CI: 0.63 to 0.94), and knee pain on a flat surface (OR: 0.79, 95% CI: 0.63 to 0.98). IPFP maximum area was negatively, but not significantly, associated with femoral cartilage defects, lateral tibiofemoral BMLs, and total knee pain or other knee pain subscales.
Conclusion
IPFP maximum area is beneficially associated with radiographic OA, MRI structural pathology and knee pain on a flat surface suggesting a protective role for IPFP possibly through shock absorption. Consequently, we must pay special attention to IPFP in the clinical settings, avoiding resection of normal IPFP in knee surgery.
Similar content being viewed by others

Introduction
Osteoarthritis (OA), the most prevalent form of arthritis, is a common cause of chronic disability in older adults[1]. It can affect one or more joints of the body but is most common in the knees[2]. Traditionally, it is characterized by loss of articular cartilage and formation of osteophytes; however, evidence has emerged that OA involves the entire joint tissues, including the menisci, ligaments, subchondral bone, capsule, synovium, and periarticular muscle[2, 3]. Although the pathogenesis of knee OA is not fully elucidated, both mechanical and metabolic factors play roles in the progression of this disease[1, 2]. Age[4], female sex[5], and body mass index (BMI)[6] are well-known risk factors for knee OA.
Infrapatellar fat pad (IPFP), an intracapsular but extrasynovial structure[7], is situated in the knee under the patella, between the patellar tendon, femoral condyle and tibial plateau[8], and is structurally similar to subcutaneous adipose tissue[9]. Recent studies[10, 11] mainly focus on the roles of the cells derived from IPFP, such as inflammatory cells and substance P nerve cells in OA, and consider IPFP as an active joint tissue in the initiation and progression of knee OA[8], as inflammatory cells from IPFP can produce inflammatory mediators, which are able to influence the cartilage and synovium metabolism, and substance P nerve could be an important source of pain in knee OA. IPFP is commonly resected during knee surgery; however, IPFP locates so closely to cartilage and bone surface that it may reduce the impact loading and absorb forces generated through the knee joint. So far, there have been few clinical or epidemiological studies[12] reporting the association between IPFP and knee OA measures, so the role of IPFP in knee OA is largely unknown.
Clinical features (such as joint pain) and joint structural abnormalities such as joint space narrowing (JSN), osteophytes, loss of cartilage volume, cartilage defects and bone marrow lesions (BMLs) are usually used to assess development/progression of knee OA[13]. The aim of this study was, therefore, to generate hypotheses regarding the associations between symptoms, joint structural abnormalities and IPFP area in older adults.
Methods
Subjects
This study was conducted as part of the Tasmanian Older Adult Cohort (TASOAC) study, an ongoing prospective, population-based study aimed at identifying the environmental, genetic, and biochemical factors associated with the development and progression of OA (assessed by both radiography and magnetic resonance imaging (MRI)). Subjects (n = 1,100) between the age of 50 and 80 years were randomly selected from the roll of electors in southern Tasmania (population, 229,000), a comprehensive population listing with an equal number of men and women. The overall response rate was 57%. Institutionalized persons and subjects with contraindications to MRI were excluded. The study was approved by the Southern Tasmanian Health and Medical Human Research Ethics Committee, and written informed consent was obtained from all participants. Self-report of diseases including asthma, cardiovascular disease, diabetes, and rheumatoid arthritis was recorded by questionnaire.
Anthropometrics and joint pain assessment
Height was measured to the nearest 0.1 cm (with shoes, socks, and headgear removed) using a stadiometer. Weight was measured to the nearest 0.1 kg (with shoes, socks, and bulky clothing removed) by using a single pair of electronic scales (Delta Model 707, Seca, Hamburg, Germany) that were calibrated using a known weight at the beginning of each clinic. BMI (weight (kg)/height (m2)) was also calculated. Total body and trunk fat were measured by a Hologic dual-energy x-ray absorptiometry (DXA) scanner (Hologic Corp., Waltham, MA, USA).
The assessment of knee pain (on a flat surface, going up/down stairs, at night, sitting/lying, and standing upright) was self-administered, using the Western Ontario McMaster Osteoarthritis Index (WOMAC) with a 10-point scale from 0 (no pain, stiffness, or functional problems) to 9 (most severe)[14]. Each compartment of joint pain was summed to create a total pain score (0 to 45), and the presence of knee pain was defined as a total score or a subscale score ≥1[15, 16].
Lower-limb muscle strength and knee radiographic assessments
We used dynamometry to measure lower-limb muscle strength twice, and took the mean as the final result, as previously described[17, 18]. A standing anteroposterior semiflexed view of the right knee with 15 degrees of fixed-knee flexion was performed in all subjects, and radiographs were individually assessed for JSN and osteophytes on a scale of 0 to 3 (0 = normal and 3 = most severe) using the Osteoarthritis Research Society International (OARSI) atlas developed by Altman et al.[19]. We summed the osteophyte and JSN scores as the knee total radiographic OA (ROA) score; an ROA score ≥1 was used to define the presence of knee ROA, as previously described[20].
Magnetic resonance imaging assessment
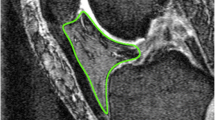
MRI scans of the right knees were performed at baseline. Knees were imaged in the sagittal plane on a 1.5-T whole-body magnetic resonance unit (Picker, Cleveland, OH, USA) with the use of a commercial transmit-receive extremity coil. The following image sequences were used: (1) a T1-weighted fat saturation three-dimensional gradient recall acquisition in the steady state; flip angle 30 degrees; repetition time 31 msecs; echo time 6.71 msec; field of view 16 cm; 60 partitions; 512 × 512 matrix; acquisition time 11 minutes 56 sec; one acquisition. Sagittal images were obtained at a partition thickness of 1.5 mm and an in-plane resolution of 0.31 × 0.31 (512 × 512 pixels), and (2) a T2-weighted fat saturation two-dimensional fast spin echo, flip angle 90°, repetition time 3,067 ms, echo time 112 ms, field of view 16 cm, 15 partitions, 256 × 256-pixel matrix; sagittal images were obtained at a slice thickness of 4 mm with a interslice gap of 1.0 mm.IPFP was measured by manually drawing disarticulation contours around the IPFP boundaries (Figure 1) on a section-by-section T2-weighted MR image, using the software program Osiris (University of Geneva). The maximum area was selected to represent the IPFP size. One observer graded the IPFP area on all MRI scans. The intraclass correlation coefficient (ICC) was 0.96 for intra-observer reliability (measured in 40 images by one observer), and inter-observer reliability was 0.92 (measured in 40 images by two observers).

Measurement of infrapatellar fat pad area. The areas of infrapatellar fat pad were measured by manually drawing disarticulation contours around the infrapatellar fat pad boundaries on a section-by-section T2-weighted magnetic resonance imaging. The maximum area was selected to represent the infrapatellar fat pad area.
Knee cartilage volume was determined on T1-weighted MR images with image processing on an independent work station, as previously described[17, 18, 21]. The total cartilage volume was divided into patellar, medial and lateral tibial cartilage volume by manually drawing disarticulation contours around the cartilage boundaries, section by section, which were then re-sampled for the final three-dimensional rendering[17, 18]. The coefficients of variation (CVs) for this method in our hands were 2.1% to 2.6%[17, 18].
Cartilage defects (0 to 4 scale) were assessed at the medial tibial, medial femoral, lateral tibial, lateral femoral, and patellar sites using T1-weighted images as previously described[22, 23] and were further confirmed using T2-weighted images as follows: grade 0 = normal cartilage; grade 1 = focal blistering and intracartilaginous low-signal intensity area with an intact surface; grade 2 = irregularities on the surface or bottom and loss of thickness <50%; grade 3 = deep ulceration with loss of thickness >50%; grade 4 = full-thickness chondral wear with exposure of subchondral bone. The presence of cartilage defect was defined as a cartilage defect score ≥2 at one site. Intraobserver reliability was 0.89 to 0.94 and interobserver reliability was 0.85 to 0.93[22, 24]. Subchondral BMLs were defined as discrete areas of increased signal adjacent to the subcortical bone at the medial and lateral tibia and femur on T2-weighted MR images using a semiquantitative (0 to 3 scale) scoring system. The intraobserver reliability ranged between 0.89 to 1.00, as previously described[25]. Tibial plateau bone area was determined by manually measuring on axial T1-weighted MR images, as previously described[20].
Patellofemoral synovitis was graded semiquantitatively from 0 to 3 in terms of the signal alterations in IPFP on T2-weighted MR images at the superior edge of the fat pad adjacent to the patella[26]. Intraobserver reliability was assessed in 40 subjects with an ICC of 0.91.
Serum biomarker measurements
Serum levels of leptin, IL-6 and TNF-α were measured in first 193 subjects as described previously[27, 28].
Data analysis
Partial correlation analyses were used to examine the associations between knee cartilage volume and IPFP area, and between total tibial bone area and IPFP area. Multivariable linear regression was used to analyze the associations of IFPF area (the dependent variable) with an independent variable (age, sex, height, weight, BMI, body fat, trunk fat, leg muscle strength, patellofemoral synovitis, leptin, IL-6 or TNF-α) after adjustment for the following covariates except itself: age, sex, height (not for BMI), weight (not for BMI, fat measures), tibial bone size, disease status (diabetes, cardiovascular diseases, asthma, rheumatoid arthritis) and ROA. Univariable and multivariable linear regression analyses were used to examine the associations between knee cartilage volume/total BML score (the dependent variable) and IPFP area (the independent variable) before and after adjustment for age, sex, height, weight, tibial bone size, patellofemoral synovitis and disease status, and further ROA. Univariable and multivariable binary logistic regression analyses were used to examine the associations between IPFP area (the independent variable) and a dependent variable (knee cartilage defects, knee JSN, osteophytes, tibial or femoral BMLs, or WOMAC knee pain) before or after adjustment for the same covariates. Interactions between sex or ROA and IPFP area were investigated by regressing cartilage volume (or others, for example, BMLs) on a binary (0/1) term for sex (or ROA) within IPFP, and assessed by testing the statistical significance of the coefficient of a (sex × IPFP) or a (ROA × IPFP) product term.
Adjustments for multiple testing on regression results were undertaken using the Hochberg method[29]. A P-value <0.05 (2-tailed) or a 95% CI not including the null point (for linear regression) or 1 (for logistic regression) was considered as statistically significant. All statistical analyses were performed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
A total of 977 subjects between 50 and 80 years of age (mean, 62.4 years) participated in the present study. There were no significant differences in demographic factors (age, sex, and BMI) between these participants and those excluded (n = 123) (data not shown). Characteristics of the subjects are presented in Table 1. The mean IPFP area was 7.59 cm2 (SD 1.18, range 4.56 to 12.14). There was a positive association (partial r = 0.26, P <0.001) between total tibial bone area and IPFP area, so all subsequent analyses were adjusted for tibial bone area.
In multivariable analyses, IPFP area was significantly and positively associated with age (β: 1.58, 95% CI: 0.80, 2.35), height (β: 6.42, 95% CI: 5.46, 7.38), weight (β: 0.90, 95% CI: 0.47, 1.34), and negatively associated with female sex (β: -42.59, 95% CI: -59.13, -26.04) after adjustment for covariates. IPFP area was neither associated with BMI, body fat, trunk fat, leg muscle strength and patellofemoral synovitis, nor with leptin, IL-6 and TNF-α (data not shown).
Table 2 describes the associations between IPFP area and radiographic OA, JSN, and osteophytes. In univariable analyses, IPFP area was significantly and negatively associated with prevalence of radiographic OA, but inconsistently associated with JSN and osteophytes. After adjustment for age, sex, height, weight, tibial bone size, patellofemoral synovitis and disease status, larger IPFP area was significantly associated with reduced radiographic OA, medial JSN, lateral JSN and medial tibiofemoral osteophytes. The association between IPFP area and lateral tibiofemoral osteophytes was consistent but not significant in the multivariable analyses. The changes in results from univariable to multivariable analyses were mainly affected by adjustment for tibial bone area.
There was a positive association (partial r = 0.20, P <0.001) between total cartilage volume and IPFP area. IPFP area was significantly associated with cartilage volume in all sites in adjusted analyses; and the associations decreased in magnitude by 17 to 35% but remained significant after further adjustment for radiographic OA (all P <0.001, Table 3). Moreover, though IPFP area was positively associated with cartilage defects at some sites, larger IPFP area was significantly associated with reduced medial and lateral tibial cartilage defects after adjustment for covariates particularly tibial bone size, and these associations became more evident after further adjustment for radiographic OA (all P <0.01, Table 3). The associations of IPFP area with femoral and patellar cartilage defects were negative but did not reach significance (Table 3).
IPFP area was positively associated with BMLs in univariable analyses; however, in multivariable analyses, particularly after adjustment for tibial bone area, larger IPFP area was associated with reduced BMLs in all compartments, where increasing per-cm2 area was significantly associated with 30% and 17% reduced odds of presence of BMLs at medial femoral and any compartments, respectively. When further adjusted for radiographic OA, the significant associations remained, and the associations with medial tibiofemoral and medial tibial BMLs became significant (Table 4). IPFP area was negatively but non-significantly associated with lateral tibiofemoral BMLs in multivariable analyses (Table 4). The association between IPFP area and total BML scores became negatively significant after adjustment for covariates and remained significant after further adjustment for radiographic OA (Table 4).
IPFP area was not significantly associated with total knee pain and pain subscales in univariable analyses; however, IPFP area was significantly and negatively associated with pain when walking on a flat surface and going up/down stairs in multivariable analyses, and remained significant for pain when walking on a flat surface after further adjustment for radiographic OA (P <0.05, Table 5). IPFP area was not associated with other pain subscales and total knee pain score in multivariable analyses (Table 5).
There were no significant interactions between sex and IPFP area or between radiographic OA and IPFP area on the outcomes (cartilage volume, cartilage defects, BMLs) (data not shown) so male and female subjects or participants with and without radiographic OA were combined for analyses. The results remained largely unchanged when subjects with rheumatoid arthritis were excluded for analyses (data not shown). All associations (except the association with knee pain) remained significant after adjustment for multiple comparisons (data not shown).
Discussion
To our knowledge, this cross-sectional study is the first to report the significant associations between IPFP area and clinical and structural abnormalities of the knee joint in older people. We found consistent evidence that IPFP area was beneficially associated with radiographic OA, knee structural abnormalities and pain. This was independent of patellofemoral synovitis, body size, tibial bone area and other covariates, suggesting IPFP area has an important protective role in knee OA.
In a previous study, Chuckpaiwong et al.[12] measured IPFP volume using MRI in a cohort of 15 control subjects and 15 knee OA subjects, and reported that BMI was not significantly associated with IPFP volume in either the control or the OA group, and age was significantly and positively associated with IPFP volume in the OA group and the whole cohort. Our findings on age and BMI were consistent with this study, but we found that weight and height, measures of body size rather than obesity status, were significantly and positively associated with IPFP area. Furthermore, we found that women had a smaller IPFP area than men, and a larger tibial bone area (a measure of knee size) was associated with greater IPFP area, providing support for the construct validity of IPFP area measurement. All these factors (except for BMI) were used as adjusting variables in our analyses.
Body mass and/or fat are considered strong risk factors for knee OA. However, the role of regional fat is much less clear. The major adipose tissue in the knee joint is IPFP, and in vitro and animal studies have reported that IPFP can produce inflammatory cytokines and adipokines that may have detrimental effects on cartilage in knee OA[30–32]; in contrast, a meeting abstract reported that in mice, although high-fat diet increased IPFP volume, the adipocytes in the IPFP did not become hypertrophic. IPFP adipocytes may be protected from obesity-induced macrophage infiltration and inflammation, suggesting that IPFP is not a source of microphage-mediated inflammation in a diet-induced obese model of early-onset knee OA[33]. A recent study reported that medium conditioned by IPFP from end-stage OA inhibited nitric oxide (NO) production as well as matrix metalloproteinase (MMP)-1, MMP-3 and collagen type II gene expression, and thus may contribute to the inhibition of cartilage catabolism[34]. Considering the intra-articular position of the IPFP with a flexible and displaceable structure[7], IPFP is likely to absorb force and reduce overloading of the knee joint, and have a protective effect on the knee.
Chuckpaiwong et al.[12] reported that there was no difference in IPFP volume between control and OA groups, possibly due to a small sample size. In contrast, we found that IPFP area was significantly and beneficially associated with cartilage volume and cartilage defects in the current study. Additionally, IPFP area was associated with decreased presence of JSN, an indirect estimate of cartilage loss on radiography, in both medial and lateral tibiofemoral compartments. While these data are cross-sectional, they provide very consistent evidence in support of a protective effect of local joint fat on articular cartilage, which is opposite to the effects of systematic fat[35]. We found that IPFP area was not associated with systematic fat mass, and metabolic and inflammatory biomarkers, all of which were associated with increased knee symptoms and cartilage loss[15, 27, 28, 36]. This suggests that systemic metabolic changes do not necessarily affect the size of IPFP.
The commonest subchondral bone abnormalities in knee OA are osteophytes and BMLs. Both are associated with knee pain[37], cartilage defects and cartilage loss[38], and need for total knee replacement[39]. In this study we reported that osteophytes and BMLs were negatively associated with IPFP area, particularly in the medial compartment. These findings further support that IPFP is protective against knee structural changes in OA.
Abnormalities of some joint structures, such as subchondral bone, capsule, ligaments, meniscus and synovium, have been associated with knee pain. It has been suggested that the sensory nerves located in these joint tissues can release substance P, calcitonin gene-related peptide (CGRP), neuropeptide Y and vasoactive intestinal peptide (VIP) into the local microenvironment, which act as the signals of pain[40]. IPFP has been regarded as an important source of pain in knee OA as it contains substance P nerve[8]; however, the association between IPFP and knee pain has not been clarified, though a previous study reported that IPFP volume was not associated with knee pain[12]. Our current study demonstrated that the IPFP area was associated with decreased presence of knee pain when walking on a flat surface and, and to a lesser extent, pain when walking upstairs/downstairs, which is opposite to what was expected, thus it had a protective effect on mechanical knee pain, which is biologically plausible.
The reasons underlying the protective effects of IPFP on joint structures and symptoms are unclear. It may be that some biochemical factors secreted from IPFP are protective, because it has been shown that medium conditioned by OA IPFP inhibits catabolic processes in cartilage[34]; it may most likely be due to the shock-absorbing nature of IPFP. As we know, biomechanical factors, especially abnormal mechanical stress/loading, play an important role in the initiation and progression of OA[41]. IPFP may have the same function as meniscus that can reduce mechanical overloading (especially in knee flexion) and absorb shock (an alteration in the environment of the joint, which can lead to cartilage degradation) through the joint. Additionally, IPFP, having the same anatomical location as the patellar ligament around the joint, may reduce instability and injury to the joint, and thus prevent the onset and progression of OA. Based on these finding, we conclude that IPFP, especially its size, plays a beneficial rather than detrimental role in the initiation or progression of OA. In the clinical setting, the IPFP is often deliberately partially or totally resected for clear visualization of the joint for the surgeons. This study suggests this may be deleterious.
The main strength of this study is that we selected participants randomly from the community, with a large sample size, and obtained both structural and symptomatic measurements. This study has several potential limitations. First, this study measured IPFP area on two-dimensional T2-weighted MRI, rather than IPFP volume on three-dimensional T1-weighted MRI. However, the boundary of IPFP on two-dimensional T2-weighted MRI is clearer than that on three-dimensional T1-weighted MRI; also IPFP area was highly correlated to IPFP volume in our analysis (r = 0.87) (unpublished data). IPFP volume measurement is also time-consuming. We did not measure IPFP quality, such as edema and fibrosis, which may be associated with the progression of OA. Second, measurement error may influence results. However, all measures were highly reproducible suggesting this is unlikely. Third, a large number of statistical tests have been performed, which may induce false positive results due to multiple testing; however, almost all significant associations remained after adjustment for multiple comparisons. Though the associations between IPFP area and knee pain did not pass the Hochberg correction, the consistent associations with weight-bearing knee pain subscales (walking on a flat surface and going up/down stairs) suggest the findings are biologically plausible, and may not be false positives. Last, the cross-sectional nature of this study precludes any inference about cause and effect relationships. Longitudinal studies are needed to address causality.
Conclusions
In conclusion, IPFP maximum area is beneficially associated with radiographic OA, MRI structural pathology and knee pain on a flat surface, suggesting a protective role for IPFP, possibly through shock absorption. Consequently, we must pay special attention to IPFP in the clinical setting, avoiding resection of normal IPFP in knee surgery.
Abbreviations
- BMI:
-
body mass index
- BML:
-
bone marrow lesion
- CV:
-
coefficient of variation
- IL-6:
-
interleukin-6
- IPFP:
-
infrapatellar fat pad
- JSN:
-
joint space narrowing
- LTF:
-
lateral tibiofemoral
- MRI:
-
magnetic resonance imaging
- MTF:
-
medial tibiofemoral
- OA:
-
osteoarthritis
- OARSI:
-
Osteoarthritis Research Society International
- ROA:
-
radiographic osteoarthritis
- TF:
-
tibiofemoral
- TNF-α:
-
tumor necrosis factor-α
- WOMAC:
-
Western Ontario McMaster Osteoarthritis Index.
References
Loeser RF: Aging and osteoarthritis. Curr Opin Rheumatol. 2011, 23: 492-496.
Hunter DJ, Felson DT: Osteoarthritis. BMJ. 2006, 332: 639-642.
Poole AR: Osteoarthritis as a whole joint disease. HSS J. 2012, 8: 4-6.
Felson DT: Epidemiology of hip and knee osteoarthritis. Epidemiol Rev. 1988, 10: 1-28.
Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G: A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthr Cartil. 2005, 13: 769-781.
Ding C, Cicuttini F, Scott F, Cooley H, Jones G: Knee structural alteration and BMI: a cross-sectional study. Obes Res. 2005, 13: 350-361.
Saddik D, McNally EG, Richardson M: MRI of Hoffa’s fat pad. Skeletal Radiol. 2004, 33: 433-444.
Clockaerts S, Bastiaansen-Jenniskens YM, Runhaar J, Van Osch GJ, Van Offel JF, Verhaar JA, De Clerck LS, Somville J: The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: a narrative review. Osteoarthr Cartil. 2010, 18: 876-882.
Vahlensieck M, Linneborn G, Schild H, Schmidt HM: Hoffa’s recess: incidence, morphology and differential diagnosis of the globular-shaped cleft in the infrapatellar fat pad of the knee on MRI and cadaver dissections. Eur Radiol. 2002, 12: 90-93.
Distel E, Cadoudal T, Durant S, Poignard A, Chevalier X, Benelli C: The infrapatellar fat pad in knee osteoarthritis: an important source of interleukin-6 and its soluble receptor. Arthritis Rheum. 2009, 60: 3374-3377.
Gandhi R, Takahashi M, Virtanen C, Syed K, Davey JR, Mahomed NN: Microarray analysis of the infrapatellar fat pad in knee osteoarthritis: relationship with joint inflammation. J Rheumatol. 2011, 38: 1966-1972.
Chuckpaiwong B, Charles HC, Kraus VB, Guilak F, Nunley JA: Age-associated increases in the size of the infrapatellar fat pad in knee osteoarthritis as measured by 3 T MRI. J Orthop Res. 2010, 28: 1149-1154.
Ding C, Zhang Y, Hunter D: Use of imaging techniques to predict progression in osteoarthritis. Curr Opin Rheumatol. 2013, 25: 127-135.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW: Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988, 15: 1833-1840.
Stannus OP, Jones G, Blizzard L, Cicuttini FM, Ding C: Associations between serum levels of inflammatory markers and change in knee pain over 5 years in older adults: a prospective cohort study. Ann Rheum Dis. 2013, 72: 535-540.
Antony B, Jones G, Venn A, Cicuttini F, March L, Blizzard L, Dwyer T, Cross M, Ding C: Association between childhood overweight measures and adulthood knee pain, stiffness and dysfunction: a 25-year cohort study. Ann Rheum Dis. 2013, doi:10.1136/annrheumdis-2013-204161
Ding C, Cicuttini F, Scott F, Glisson M, Jones G: Sex differences in knee cartilage volume in adults: role of body and bone size, age and physical activity. Rheumatology (Oxford). 2003, 42: 1317-1323.
Jones G, Glisson M, Hynes K, Cicuttini F: Sex and site differences in cartilage development: a possible explanation for variations in knee osteoarthritis in later life. Arthritis Rheum. 2000, 43: 2543-2549.
Altman RD, Hochberg M, Murphy WA, Wolfe F, Lequesne M: Atlas of individual radiographic features in osteoarthritis. Osteoarthr Cartil. 1995, 3: 3-70.
Jones G, Ding C, Scott F, Glisson M, Cicuttini F: Early radiographic osteoarthritis is associated with substantial changes in cartilage volume and tibial bone surface area in both males and females. Osteoarthr Cartil. 2004, 12: 169-174.
Ding C, Cicuttini F, Blizzard L, Jones G: Smoking interacts with family history with regard to change in knee cartilage volume and cartilage defect development. Arthritis Rheum. 2007, 56: 1521-1528.
Ding C, Garnero P, Cicuttini F, Scott F, Cooley H, Jones G: Knee cartilage defects: association with early radiographic osteoarthritis, decreased cartilage volume, increased joint surface area and type II collagen breakdown. Osteoarthr Cartil. 2005, 13: 198-205.
Ding C, Cicuttini F, Scott F, Cooley H, Boon C, Jones G: Natural history of knee cartilage defects and factors affecting change. Arch Intern Med. 2006, 166: 651-658.
Bennell KL, Bowles KA, Payne C, Cicuttini F, Williamson E, Forbes A, Hanna F, Davies-Tuck M, Harris A, Hinman RS: Lateral wedge insoles for medial knee osteoarthritis: 12 month randomised controlled trial. BMJ. 2011, 342: d2912-
Zhai G, Blizzard L, Srikanth V, Ding C, Cooley H, Cicuttini F, Jones G: Correlates of knee pain in older adults: Tasmanian Older Adult Cohort Study. Arthritis Rheum. 2006, 55: 264-271.
Roemer FW, Guermazi A, Zhang Y, Yang M, Hunter DJ, Crema MD, Bohndorf K: Hoffa’s Fat Pad: evaluation on unenhanced MR images as a measure of patellofemoral synovitis in osteoarthritis. AJR Am J Roentgenol. 2009, 192: 1696-1700.
Stannus O, Jones G, Cicuttini F, Parameswaran V, Quinn S, Burgess J, Ding C: Circulating levels of IL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults. Osteoarthr Cartil. 2010, 18: 1441-1447.
Stannus OP, Jones G, Quinn SJ, Cicuttini FM, Dore D, Ding C: The association between leptin, interleukin-6, and hip radiographic osteoarthritis in older people: a cross-sectional study. Arthritis Res Ther. 2010, 12: R95-
Hochberg Y: A sharper Bonferroni procedure for multiple tests of significance. Biometrika. 1988, 75: 800-802.
Ushiyama T, Chano T, Inoue K, Matsusue Y: Cytokine production in the infrapatellar fat pad: another source of cytokines in knee synovial fluids. Ann Rheum Dis. 2003, 62: 108-112.
Clockaerts S, Bastiaansen-Jenniskens YM, Feijt C, De Clerck L, Verhaar JA, Zuurmond AM, Stojanovic-Susulic V, Somville J, Kloppenburg M, van Osch GJ: Cytokine production by infrapatellar fat pad can be stimulated by interleukin 1beta and inhibited by peroxisome proliferator activated receptor alpha agonist. Ann Rheum Dis. 2012, 71: 1012-1018.
Klein-Wieringa IR, Kloppenburg M, Bastiaansen-Jenniskens YM, Yusuf E, Kwekkeboom JC, El-Bannoudi H, Nelissen RG, Zuurmond A, Stojanovic-Susulic V, Van Osch GJ, Toes RE, Loan-Facsinay A: The infrapatellar fat pad of patients with osteoarthritis has an inflammatory phenotype. Ann Rheum Dis. 2011, 70: 851-857.
Chang W, DeMoe C, Kent C, Kovats S, Garteiser P, Doblas S, Towner R, Griffin TM: Infrapatellar fat pad hypertrophy without inflammation in a diet-induced mouse model of obesity and osteoarthritis. Osteoarthr Cartil. 2011, 19: 66-
Bastiaansen-Jenniskens YM, Clockaerts S, Feijt C, Zuurmond AM, Stojanovic-Susulic V, Bridts C, de Clerck L, DeGroot J, Verhaar JA, Kloppenburg M, van-Osch GJ: Infrapatellar fat pad of patients with end-stage osteoarthritis inhibits catabolic mediators in cartilage. Ann Rheum Dis. 2012, 71: 288-294.
Ding C, Stannus O, Cicuttini F, Antony B, Jones G: Body fat is associated with increased and lean mass with decreased knee cartilage loss in older adults: a prospective cohort study. Int J Obes. 2012, 37: 822-827.
Ding C, Parameswaran V, Cicuttini F, Burgess J, Zhai G, Quinn S, Jones G: Association between leptin, body composition, sex and knee cartilage morphology in older adults: the Tasmanian older adult cohort (TASOAC) study. Ann Rheum Dis. 2008, 67: 1256-1261.
Javaid MK, Kiran A, Guermazi A, Kwoh CK, Zaim S, Carbone L, Harris T, McCulloch CE, Arden NK, Lane NE, Felson D, Nevitt M, ABC Health Study: Individual magnetic resonance imaging and radiographic features of knee osteoarthritis in subjects with unilateral knee pain: the health, aging, and body composition study. Arthritis Rheum. 2012, 64: 3246-3255.
Dore D, Martens A, Quinn S, Ding C, Winzenberg T, Zhai G, Pelletier JP, Martel-Pelletier J, Abram F, Cicuttini F, Jones G: Bone marrow lesions predict site-specific cartilage defect development and volume loss: a prospective study in older adults. Arthritis Res Ther. 2010, 12: R222-
Dore D, Quinn S, Ding C, Winzenberg T, Zhai G, Cicuttini F, Jones G: Natural history and clinical significance of MRI-detected bone marrow lesions at the knee: a prospective study in community dwelling older adults. Arthritis Res Ther. 2010, 12: R223-
McDougall JJ: Arthritis and pain. Neurogenic origin of joint pain. Arthritis Res Ther. 2006, 8: 220-
Guilak F, Fermor B, Keefe FJ, Kraus VB, Olson SA, Pisetsky DS, Setton LA, Weinberg JB: The role of biomechanics and inflammation in cartilage injury and repair. Clin Orthop Relat Res. 2004, 423: 17-26.
Acknowledgements
We especially thank the participants who made this study possible, and we gratefully acknowledge the role of the staff and volunteers in collecting the data, particularly research nurses C Boon and P Boon. R Warren assessed MR images and Dr G Zhai scored bone marrow lesions. Dr V Srikanth and Dr H Cooley assessed radiographs. This study was supported by the National Health and Medical Research Council of Australia; Arthritis Foundation of Australia; Tasmanian Community Fund; Masonic Centenary Medical Research Foundation, Royal Hobart Hospital Research Foundation, and University of Tasmania Institutional Research Grants Scheme. G Jones is supported by a National Health and Medical Research Council Practitioner Fellowship. D Aitken is supported by a National Health and Medical Research Council Early Career Fellowship. C Ding is supported by an Australian Research Council Future Fellowship.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
CD had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. CD carried out the study design, participated in the acquisition, analysis and interpretation of data, manuscript preparation, and statistical analysis. WH participated in the acquisition, analysis and interpretation of data, manuscript preparation, and statistical analysis. SC participated in the acquisition of data, manuscript preparation, and statistical analysis. ZL participated in the analysis and interpretation of data, manuscript preparation, and statistical analysis. XJ participated in the acquisition, analysis and interpretation of data, and manuscript preparation. XW participated in the acquisition of data, manuscript preparation, and statistical analysis. BA participated in the acquisition, analysis and interpretation of data, and manuscript preparation. YC participated in the acquisition of data, manuscript preparation, and statistical analysis. DA participated in the acquisition of data, and manuscript preparation. FC participated in the study design, and manuscript preparation. GJ participated in the study design, acquisition, analysis and interpretation of data, and manuscript preparation. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Han, W., Cai, S., Liu, Z. et al. Infrapatellar fat pad in the knee: is local fat good or bad for knee osteoarthritis?. Arthritis Res Ther 16, R145 (2014). https://doi.org/10.1186/ar4607
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar4607