
Abstract
Background
Hepatoblastoma (HB) is the most frequent malignant liver tumor in infants and young children. While it is rare, the brain seems to be the most habitual site of non-pulmonary metastasis.
Case presentation
In this report, we present the case of a 13-month-old girl followed for metastatic hepatoblastoma in the lung. She was brought to the emergency department with tonic–clonic seizure, and a brain CT scan revealed a single intra-parenchymal metastasis.
Conclusions
In children with a history of hepatoblastoma, the development of neurologic symptoms should prompt cerebral imaging, to exclude the presence of cerebral metastases.
Similar content being viewed by others


Background
Hepatoblastoma (HB) is the most frequent primary malignancy of the liver in pediatric patients under 3 years of age, accounting for 1% to 2% of all malignancies in this population, with an incidence rate of 1.5 to 5 cases per 1 million infants [1, 2]. Tumor metastases are a major obstacle to the development of effective treatments for HB patients; they usually affect the lungs; brain metastases are extremely rare [3].
Zhi et al. [4] reported that 132 of 316 infants with HB developed distant metastases, 80% of them lung metastases, followed by 6% intracranial metastases, 4.5% bone metastases, 3% diaphragm metastases, 3% right atrium metastases and 3% pleura metastases.
Our objective is to demonstrate the indications of brain imaging in hepatoblastoma and to illustrate the radiological features of cerebral metastasis as an unusual presentation of HB through our case.
Case presentation
A 13-month-old girl without any previous history presented with an abdominal distention. Clinical examination reveals a patient with hemodynamic and respiratory stability presenting a significant abdominal mass on palpation. A CT scan of the chest, abdomen, and pelvis identified a single mass of the liver involving segments IV-V-VI and VIII with irregular contours and heterogeneous enhancement, associated with pulmonary metastases (Fig. 1). The serum alpha-fetoprotein (AFP) was measured at 60,150 ng/mL. A liver biopsy confirmed the diagnosis of hepatoblastoma stage IV, and the patient underwent palliative chemotherapy.

Axial abdomen CT before (A) and after contrast (B) revealed a large hepatic mass involving segments IV-V-VI and VIII. The mass displayed irregular contours and heterogeneous enhancement, with delineated areas of necrosis (indicated by the yellow arrow). It measured 120 × 90 mm axial diameters. Axial chest CT in a lung window (C, D) revealed the presence of multiple pulmonary nodules (indicated by the red arrow), indicating lung metastases
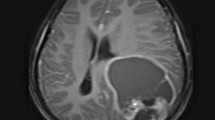
After one year, the child presented to the emergency department with tonic–clonic seizure without localizing signs. A CT scan of the brain before and after contrast revealed a solitary supratentorial hemorrhagic mass located in the right frontal lobe. The mass displayed heterogeneous enhancement, causing regional edema and was identified as a brain metastasis (Fig. 2).

Axial and coronal brain CT before (A, C) and after contrast (B, D) showed a solitary supratentorial hemorrhagic mass located in the right frontal lobe, with heterogeneous enhancement, causing regional edema without mass effect
Methylprednisolone and anticonvulsants were initiated, and the possibility of providing palliative care with cranial radiation was considered. However, three days after admission, the patient experienced a cardiorespiratory arrest.
Discussion
Primary tumors of the liver are rare in infancy. HB is the commonest and has a diverse clinical appearance [5]. AFP is a tumoral marker for HB, at the moment of diagnosis and during follow-up. Age and imaging are also important in classifying risk groups and determining long-term survival rates. Furthermore, biopsy plays a significant role in confirming the histology of the tumor [4].
International pediatric liver tumor organizations such as SIOPEL, COG, and CHIC recommend abdominal CT scan or MRI liver-specific contrast imaging for PRETEXT staging in patients with suspected HB [6]. This classification describes 4 stages based on the anatomical lesions of the liver and the implication of other structures. Depending on tumor stage and metastatic status, there are several treatment options, including chemotherapy, chemoembolization, resection of the tumor, metastasectomy, radio-frequency ablation, and liver transplantation [7].
Our patient had hepatoblastoma stage IV with pulmonary metastases, and she underwent palliative chemotherapy.
The metastatic site of hepatoblastoma is usually the lungs. Lung metastases detected at diagnosis are one of the most reliable prognostic indicators of poor outcome in patients diagnosed with hepatoblastoma [8]. Extra-pulmonary metastases to the brain, abdomen, and bones are uncommon in patients with hepatoblastoma. Children with hepatoblastoma with distant metastases have a poor prognosis at diagnosis and even worse if they recur [9].
Brain metastases rarely occur in children with hepatoblastoma; few cases have been reported worldwide. Rai and Feusner [1] conducted an extensive review of the literature to identify such patients and examine the different therapies used to treat them. They identified 39 patients. All patients had neurological symptoms at the time of diagnosis of brain metastasis such as hemiparesis, acute headache, generalized tonic–clonic seizures or partial seizures. Although extensive demographic information was reported for only 19 of these patients, it is noteworthy that 24% (4/17) were aged more than 4 years at the time of the initial primary tumor diagnosis, one third was stage IV at original HB diagnosis, and 63% (7/11) had evidence of lung metastases (at initial diagnosis or at recurrence) before brain metastases occurred. Based on the limited published data on this uncommon condition and the known association of worse prognosis with older age at diagnosis, they suggest additional brain imaging of older patients when they present for pulmonary relapse evaluation even if they are neurologically asymptomatic, with the objective of early detection and surgical resection of these lesions.
In addition, if a child with HB presents with neurological disorders, brain imaging, preferably MRI, should be done to rule out the presence of brain metastases [3].
Several previous authors described isolated cases of hemorrhagic parenchymal metastases in patients with HB [10]. Among them, both Kabudi and colleagues and Roberson et al. [11, 12] described these metastatic lesions as dense enhancement on MRI, consistent with the extreme cellularity of these tumors. Porto and colleagues [13] described an imaging pattern of a recurrent hemorrhagic lesion with little or no associated enhancement resembling a cavernous malformation.
In our case, the brain CT scan showed a solitary supratentorial hemorrhagic mass located in the right frontal lobe, with heterogeneous enhancement.
Based on the risk of bleeding and the clinical benefit associated with surgery, surgery on a single massive hemorrhagic lesion should be considered even in chemotherapy-sensitive tumors. Brain irradiation, which is a common treatment for adults with multiple metastases, is generally not recommended for young children due to concerns about its effects. However, the poor prognosis in these cases often necessitates the use of radiotherapy. Among the children, only one survived for an extended period. This child had a single recurrent brain metastasis, which was successfully treated through a combination of multiple surgical resections, chemotherapy, and radiotherapy [12].
Conclusions
In conclusion, in children known to have HB, the appearance of neurological complaints should prompt brain imaging studies to rule out the possibility of intracranial spread of the tumor. However, routine cerebral imaging screening is not indicated because of the cost and rarity of brain metastases in HB.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HB:
-
Hepatoblastoma.
- CT:
-
Computed Tomography
- MRI:
-
Magnetic Resonance Imaging
- AFP:
-
Alpha-fetoprotein
- PRETEXT:
-
PRE-Treatment EXTent of tumor
References
Rai P, Feusner JH (2016) Cerebral metastasis of hepatoblastoma: a review. J Pediatric Hematol Oncol 38(4):279–282
Ranganathan S, Lopez-Terrada D, Alaggio R (2020) Hepatoblastoma and pediatric hepatocellular carcinoma: an update. Pediatr Dev Pathol 23(2):79–95
Habchi SBLAN, Djaafer KBM (2021) Brain metastases in hepatoblastoma a case report. Clin Case Rep Clin Study, 3(3)
Zhi T, Zhang WL, Zhang Y, Hu HM, Huang DS (2021) Clinical characteristics and prognostic factors of hepatoblastoma in 316 children aged under 3 years—a 14-year retrospective single-center study. BMC Pediatr 21(1):1–11
Barragan V, Escudero MC, Jimenez IC, Correa C, Luengas JP (2022) Bone metastases in hepatoblastoma, an unusual presentation. Case report and review of the literature. Radiol Case Rep 17(11):4272–4275
Roebuck DJ, Olsen Ø, Pariente D (2006) Radiological staging in children with hepatoblastoma. Pediatr Radiol 36(3):176–182. https://doi.org/10.1007/s00247-005-0029-6
Hu HM, Zhang WL, Wang YZ, Zhang Y, You Y, Fan L et al (2020) Treatment outcomes for hepatoblastoma children with pulmonary metastasis and extrapulmonary involvement: experience of 36 cases at a single institution. Transl Cancer Res 9(10):6402–11
Brown J, Perilongo G, Shafford E, Keeling J, Pritchard J, Brock P et al (2000) Pretreatment prognostic factors for children with hepatoblastoma-results from the International Society of Paediatric Oncology (SIOP) Study SIOPEL 1. Eur J Cancer 36:1418–1425
Park SM, Choe BK, Kim YH, Kim HS, Kwon TC, Lee HJ (2006) A case of recurrent hepatoblastoma: lung, heart and brain metastasis. Clin Exp Pediat 49(6):691–695
Amans MR, Phillips CD (2012) Hepatoblastoma metastatic to brain mimicking intracranial hemorrhage: case report and literature review. Radiol Case Rep 7(2):611
Kebudi R, Ayan I, Görgün O et al (2005) Brain metastasis in pediatric extracranial solid tumors: survey and literature review. J Neurooncol 71:43–48
Robertson PL, Muraszko KM, Axtell RA (1997) Hepatoblastoma metastatic to brain: prolonged survival after multiple surgical resections of a solitary brain lesion. J Pediatr Hematol Oncol 19:168–171
Porto L, Jarisch A, Zanella F et al (2010) The role of magnetic resonance imaging in children with hematogenous brain metastases from primary solid tumors. Pediatr Hematol Oncol 27:103–111
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics committee approval for this study was approved by the Ethics Committee for Biomedical Research Casablanca, Morocco, in accordance with the Declaration of Helsinki, under reference 17/15. Written informed consent was obtained for all patients. Anonymity and confidentiality were respected for all participants.
Consent for publication
Yes, I have the consent of the patient's parent.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Houssaini, M.S., Akammar, A., Mourabiti, A.Y. et al. Cerebral metastasis of Hepatoblastoma: a case report and literature review. Egypt J Radiol Nucl Med 54, 220 (2023). https://doi.org/10.1186/s43055-023-01149-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01149-z