
Abstract
Background
This study aims to investigate the association between bony morphological features and ACL injury and to identify potential risk factors for the identification and prevention of ACL injuries. The study used knee MRIs to examine the distal femoral and proximal tibia morphology of 500 patients aged 19–50, including 250 cases with an injured ACL and 250 controls with a non-injured ACL. Previous literature has shown that ACL injuries are a common occurrence in sports and can have serious long-term consequences. Several risk factors have been identified, including anatomical variations in the bony structures of the knee. However, the relationship between bony morphology and ACL injury is not well understood, and there is a need to investigate the potential role of these factors in the identification and prevention of ACL injuries. This study was necessary because of the high incidence of ACL injuries and the potential long-term consequences, such as osteoarthritis, associated with this injury. By identifying potential risk factors, such as bony morphological features, it may be possible to develop targeted prevention strategies to reduce the incidence of ACL injuries. The study also adds to the existing literature by providing new insights into the relationship between bony morphology and ACL injury, and by identifying specific parameters that can be used to predict ACL injury.
Results
There was a significant difference in bony morphology between ACL-injured and non-injured patients. The most convincing parameters of femur and tibia were notch width index (NWI), medial tibial plateau depth (MTPD), and lateral tibial plateau slope (LTPS). A significantly smaller intercondylar notch was seen in the injured patients (mean 17.25 mm) than in controls (mean 18.41 mm) (p < 0.001, unpaired t test). The findings indicate that among all the features assessed, the medial tibial plateau depth (MTPD) stands out as the most statistically significant with an odds ratio of 2.4, and it demonstrates a substantial association.
Conclusions
ACL-injured patients have a narrower NWI, shallower MTPD, and steeper LTPS, which appear to be associated with ACL injury. Identifying the cut-off values for these parameters can help predict ACL injury.
Similar content being viewed by others

Background
Anterior cruciate ligament (ACL) is the most injured ligament in the knee; ACL injuries occur frequently in both athletes and non-athletes. In the USA, the prevalence of ACL injury is 1 in 3000, and approximately 250,000 injuries occur every year [1]. A significant number of studies have been carried out to identify the predisposing factors of ACL injuries of which age, sex, and anatomical factors are notable [2,3,4,5]. Studies have shown that female adolescents participating in jumping/landing sports are at a substantially higher risk of ACL injury compared to their male counterparts, with a fourfold to sixfold increased risk [6, 7]. The passage of the Educational Assistance Act, Title IX, led to a significant increase in female participation in high school sports, increasing nearly ninefold from 0.3 million to 2.8 million. However, this increase in participation has also resulted in a rise in ACL injuries among female athletes. Significant disparity exists in understanding risk factors; however, three major factors, namely anatomical, hormonal, and neuromuscular hold ground in this gender disparity [8]. Thigh length, height, and femoral NW variations can also predispose to ACL injury as shown in various studies [2].
Recent studies have highlighted a growing body of evidence indicating that abnormal biomechanics in the lower limbs during injury-prone movements, such as jump sports, deceleration, lateral pivoting, and landing sports, may be a contributing factor to ACL injuries in females [8,9,10,11]. The most effective imaging technique for assessing knee and ACL injuries is magnetic resonance imaging (MRI), which has been demonstrated to have high sensitivity and specificity [12]. Although several studies have emphasized the importance of a narrow NW, typically observed in females, in relation to ACL injury, there is still no unanimous agreement on this theory, as some studies have presented conflicting results [13,14,15,16].
The purpose of this study was to evaluate multiple bony morphological features observed on MRI in patients with and without ACL injury. The objectives were achieved by measuring anatomic variables of proximal tibia and distal femur and assessing these parameters to determine whether they are risk factors for ACL injury.
Methods
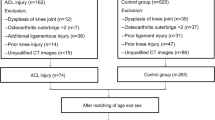
This is a retrospective, unmatched case–control, single-centre study conducted on 500 patients, consisting of 250 with ACL injury and 250 controls who underwent MRI of the knee between January 2018 and January 2022. The sample size of study was calculated from expected proportions and assumed odds ratio from similar studies from past. Non-injured ACL patients were defined as having intact posterolateral and anteromedial bundles with normal signal. The ACL-injured patients were defined as having discontinuity of fibres resulting in partial or complete tear. ACL injury at all sites such as mid substance, femoral, and tibial attachments including avulsion injuries was included. Traumatic patients with significantly displaced fractures that limited accurate measurements were excluded. Unfortunately, surgical or arthroscopic correlation was not performed to confirm final diagnosis. Patients included were aged between 19 and 50 years to ensure skeletal maturation and to avoid degenerative changes that may be common in the non-included age group.
The study group was divided into 2 groups wherein the first group consisted of 250 individuals diagnosed with ACL injuries including non-traumatic (please refer definition of ACL injury as mentioned above) on MRI knee scans. The other group (controls) consisted of 250 individuals who were not found to have any ACL injury on MRI. Post-operative, degenerative, inflammatory, infective, or haemophilic arthritic and traumatic patients with displaced or depressed fractures causing difficulty in bony measurements were deliberately excluded from study as these conditions affect normal anatomic configuration and true measurements of the parameters.
Patient demographics and clinical history were compiled from the electronic patient records of the hospital. This study protocol was approved by the Scientific and Ethical Committee of the Institute. Informed consent was obtained from all individual participants included in study. The confidentiality was strictly maintained regarding all personal details of the participants and information related to the study.
All the patients included in the study underwent a standard MRI knee scan on a 1.5 T Siemens Avanto or a 3 T Vida Scanner. MRI protocol adequacy to diagnose ACL injury was audited, modified/rectified to standard before starting study. All images were acquired, while patient was in supine position with knee flexed to a 10-degree angle. Axial, coronal, and sagittal planes of T1 and proton density fat-saturated (PDFS) sequences were used to diagnose ACL injury and to measure bony parameters. Picture archiving and communication system imaging software was used to retrieve MRI images and assess the various morphometric parameters using built-in measurement tools. Diagnosis of ACL injury on MRI and bony measurements was strictly done by one radiologist to avoid interobserver variability and bias arising from it.
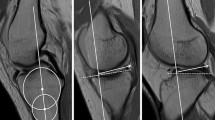
To evaluate the femoral measurements, coronal and axial PDFS sequences were used. The bicondylar width and NW were calculated at the level of popliteal groove on the coronal PDFS (Fig. 1a). NWI was determined by dividing the notch width by the bicondylar width at the same level. Notch entrance width was calculated on the axial PDFS at the level of femoral epicondyles (Fig. 1b). For tibial measurements, sagittal reconstructed images of T1 were used. The posterior tibial slopes (MTPS and LTPS) were calculated (Fig. 2A). A longitudinal axis was first created at the mediolateral centre of the medial tibial plateau in the sagittal plane. A tangent was then drawn on this image to the tibial plateau, connecting the peak anterior and posterior cortical edges. The slope of the line, which extended through these two points, represented the MTPS and was measured relative to the axis perpendicular to the longitudinal axis of the tibia. Similarly, the LTPS was derived. Tibial axis was generated with double circle method. Finally, the MTPD measurement was calculated by drawing a line that connected the peak anterior and posterior points of the medial plateau to a line drawn tangentially to the deepest point of the medial plateau and measuring the maximum vertical distance between the two parallel lines (Fig. 2B).

Distal femoral measurements. a Coronal—notch width (red), bicondylar width (blue). b Axial—notch entrance width (orange)

A Tibial measurements—a Double circle method to determine true tibial longitudinal axis(green). b Calculated lateral tibial plateau inclination angle (red) perpendicular to longitudinal axis. B Tibial measurements—a medial tibial inclination angle (red) perpendicular to tibial longitudinal axis(green) and b medial tibial plateau depth (blue)
Data analysis was done using the SPSS (Statistical Package for the Social Science) Version 28 for windows. Continuous imaging metrics were compared using independent sample t test. Chi-square test was used to compare the difference of qualitative/categorical variables in 2 groups. Data were not normally distributed as determined by the Shapiro–Wilk test, and therefore, nonparametric Mann–Whitney U test was used to ascertain the statistical significance between cases and controls. A logistic regression was performed with injury/no injury (i.e. cases and controls as the outcome variable). The independent variables with a p value < 0.1 in univariate analysis were entered in the model, and univariate odds ratio was calculated by drawing receiver operative characteristics curves (ROCs).
Results
This study looked at 250 people with injured ACLs and compared their bone structure to that of 250 people with healthy ACLs. The two groups were not matched in terms of age and gender, but both were predominantly male (Table 1). The study found several differences between the bone structures of the two groups (Table 2). It is important to note that the relationship of absolute measurements with injury has been examined without reference to overall patient size or weight, except for the consideration of sex differences. The notch width index (NWI) is perhaps the only measure in this study that takes into account the size of the individual.
First, the injured ACL group had a significantly smaller intercondylar notch width (mean 17.25 mm vs. 18.41 mm, p < 0.001) as well as a significantly smaller notch width index (mean 0.25 mm vs. 0.27 mm, p < 0.001) compared to the healthy group. In contrast, the injured ACL group had a significantly larger combined femoral condylar width (mean 51.02 mm vs. 49.43 mm, p < 0.001) compared to the healthy group. There were no significant differences at notch entrance width.
In terms of tibial parameters, the study found that MTPD was significantly shallower in the injured ACL group compared to the healthy group (mean 2.46 mm vs. 2.76 mm, p < 0.001). LTPS was significantly steeper in the injured ACL group compared to the healthy group (mean 6.05 degrees vs. 5.0 degrees, p < 0.001). There were no significant differences at MTPS.
There exist significant bony differences between males and females, with females typically exhibiting smaller bony parameters when compared to males (Table 3a). A logistic regression model (Table 3b) was used to calculate the odds ratio with regard to bony parameters. If the odds ratio for ACL injury is greater than 1 and the lower and upper confidence intervals are also greater than 1, then we can conclude that there is a statistically significant association between a higher notch width and an increased likelihood of ACL injury. Specifically, there is a 1.24-fold increase in the odds of ACL injury associated with smaller notch width and a 1.74-fold increase in odds for ACL injury associated with a shallower MPTD.
The study also used box plots (Fig. 3) and area under the curve (AUC)–receiver operating characteristics (ROC) curves (Figs. 4, 5, 6, 7) to determine thresholds for significant parameters. An ROC curve was generated using the sensitivity and specificity values for the outcome of ACL injury (yes/no). Using Medcalc software, the curve was plotted with sensitivity on the y-axis and 100—specificity on the x-axis. The cut-off value for a particular imaging parameter was calculated based on its sensitivity and specificity for diagnosing the presence of ACL injury. Area under the ROC curve (AUC) is a measure of how well a parameter can distinguish between the two groups, with an AUC of 1.0 indicating perfect discrimination and 0.5 indicating chance discrimination.

Box plot data presentation showing striking differences between injured and non-injured ACL for various bony parameters from top NW, NWI, MTPD, and LTPS
For NW, the AUC was 0.64, which is considered a moderate level of discrimination. The cut-off value for NW was 16.4 mm, and at this value, the sensitivity was 41.2% (meaning that 41.2% of ACL-injured patients had NW values above the cut-off) and the specificity was 84.8% (meaning that 84.8% of non-injured patients had NW values below the cut-off) (Fig. 4 and Table 4). Similar results were found for NWI (AUC of 0.69) and LTPS (AUC of 0.66), with cut-off values of 0.26 and 6.7 degrees, respectively (Figs. 5, 6 and Tables 5, 6). MTPD had an AUC of 0.61, which is considered poor discrimination. The cut-off value for MTPD was 2.83 mm, with a sensitivity of 78.4% and a specificity of 44.4% (Fig. 7 and Table 7).

Receiver operating characteristic curve for notch width parameter with high specificity as represented in table (aDeLong et al. 1988; bBinomial exact)

Receiver operating characteristic curve for notch width index parameter with high sensitivity as represented in table (aDeLong et al. 1988; b Binomial exact)

Receiver operating characteristic curve for LTPS parameter with high specificity as represented in table (aDeLong et al., 1988; bBinomial exact)

Receiver operating characteristic curve for MTPD parameter with high sensitivity as represented in table (aDeLong et al. 1988; b Binomial exact)
Overall, the study found that NW, NWI, MTPD, and LTPS were the most promising parameters for distinguishing between ACL-injured and non-injured patients and suggests that certain bone structure differences may be associated with an increased risk of ACL injury, particularly in females. The findings indicate that among all the features assessed, the medial tibial plateau depth (MTPD) stands out as the most statistically significant. With an odds ratio of 2.4, it demonstrates a substantial association.
However, further research is needed to confirm these findings and determine how these bone structure differences may contribute to ACL injury risk.
Discussion
Anterior cruciate ligament (ACL) injuries are the most common outcome of knee injuries [17], and the development of preventative methods to avoid them has become a matter of prime importance. The risk of early osteoarthrosis and the added effects on quality of life make these injuries particularly concerning for athletes, as they may have serious consequences on their career [18].
Numerous studies have investigated the underlying anatomical determinants of ACL injury using various imaging techniques. Anderson et al. used computed tomography data to compare and investigate bone morphology between ACL-injured and non-injured patients and found differences in certain morphological variables between men and women [15, 19]. Similarly, other studies have utilized MRI scans and radiography to identify risk factors for ACL injury [20,21,22]. Domzalski et al. found that a narrower intercondylar notch was correlated with a higher probability of ACL rupture in a young population [23, 24]. Park et al. identified NW and medial condyle width as important risk factors for ACL injuries in men, while notch width, medial-to-lateral ratio, and notch width index showed greater significance in women [25, 26]. A meta-analysis by Zeng et al. found that having a smaller notch width index increases the risk of ACL injury [27]. A study by Bayer S et al. talks about the knee morphological risk factors of ACL injury [28] and another by Iriuchisima T et al. talks about the influence of the variance in width between the tibial spine and femoral intercondylar notch on the occurrence of ACL injury [29]. A recent meta-analysis by Renato Andrade et al. found that notch morphology such as smaller NWI and increased tibial slopes put the individual at higher risk of injuring the ACL [30].
In our study, we examined bony morphology differences between ACL-injured and non-injured patients using MRI scans. We found that smaller NW and NWI were risk factors for ACL injury. Women with smaller NW were found to be at higher risk compared to men. Our results were consistent with those of previous studies [24, 25, 27].
Another anatomical factor that has been linked to ACL injury is tibial slope. O'Malley et al. found a considerable connection between a higher posterior tibial slope and ACL injury [31], and Webb et al. discovered that an increased tibial slope increased the risk of ACL injury following ACL reconstruction [32]. However, the relationship between ACL damage and tibial slope has been the subject of much debate and research [32, 33]. Dare et al. found that lateral tibial slope was strongly linked to a higher incidence of ACL injuries in paediatric and teenage patients [34]. Although some studies have found a correlation between ACL injury and tibial slope, the results have been inconsistent and debatable [34, 35].
From a biomechanical perspective, an increased tibial slope may provide more translational force, which could lead to an increase in the tibia’s anterior motion. It is well established that the ACL plays a significant role in limiting anterior tibial mobility. As a result, an increased tibial slope may cause an increase in ACL tension or possibly an ACL rupture [36, 37]. In our study, we found that MTPD and LTPS were significant risk factors for ACL injury, and we established cut-off values for potential risk factors. Although our study did not find significant differences in medial tibial plateau slope between cases and controls, we did find high specificity of LTPS and high sensitivity of MTPD for ACL injury.
In conclusion, the development of preventative methods to avoid ACL injuries is essential for athletes and individuals who engage in activities that may put them at risk of knee injuries. Anatomical factors such as NW, NWI, and tibial slope have been identified as significant risk factors for ACL injury. Future research should focus on developing preventative measures that take these risk factors into account to reduce the incidence of ACL injuries in at-risk population.
This study, much like the recent study conducted by Ashwini T et al. [38], has identified a correlation between narrow femoral intercondylar notch, low notch index, shallow medial tibial plateau, and steep posterior tibial slopes with ACL injury within the studied population. Specifically, a narrow intercondylar notch (< 16 mm), low NI (< 0.26), shallow MTPD (< 2.8 mm), and steep tibial slopes (LTPS 6.3 degrees) were found to be factors that predispose individuals to ACL injury. MRI scans that show these characteristics may suggest a higher risk of ACL injury and prompt the need for strategic modifications in biomechanical movement or training to help prevent injury. This information can be valuable to orthopaedic doctors when counselling patients, implementing preventive measures, and adjusting post-operative rehabilitation protocols.
There are certain limitations to our study that should be noted. First, the ACL injury diagnosis was not confirmed using arthroscopy or surgery. Furthermore, our study only included a mature skeleton population and did not examine adolescents, which may be an important consideration when generalizing our findings to the wider population. Lastly, while the thickness of the individual bundle is an important parameter, our study only focused on bony morphology.
Conclusions
This study provides evidence that bony morphological features, specifically NWI, MTPD, and LTPS, are associated with ACL injury and can be used for the identification and prevention of ACL injuries. The results suggest that individuals with a narrower NWI, shallower MTPD, and steeper LTPS are at increased risk of ACL injury.
The findings of this study have important implications for the field of sports medicine and orthopaedics. Identifying individuals at higher risk of ACL injury based on their bony morphology could help with targeted prevention strategies such as modifying training programs, using braces or other protective equipment, and recommending surgical interventions. The study by Mather, Richard C. et al. [39] underscores the economic burden associated with ACL tears and highlights the importance of prioritizing injury prevention and effective treatment approaches to minimize both individual and societal costs. Furthermore, understanding the relationship between bony morphology and ACL injury may help guide surgical interventions and post-operative rehabilitation to prevent re-injury and optimize outcomes.
This study adds to the existing literature by providing new insights into the relationship between bony morphology and ACL injury and identifying specific parameters that can be used to predict ACL injury. The findings of this study have the potential to improve clinical decision-making and ultimately lead to better outcomes for individuals at risk of ACL injury.
Availability of data and materials
The data that support the findings of this study are not openly available due to sensitivity and are available from the corresponding author, [Sagar Maheshwari], upon reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- NWI:
-
Notch width index
- MTPD:
-
Medial tibial plateau depth
- LTPS:
-
Lateral tibial plateau slope
- SPSS:
-
Statistical package for the social science
- AUC:
-
Area under curve
References
Lesic A, Bumbasirevic M (1999) The clinical anatomy of cruciate ligaments and its relevance in anterior cruciate ligament (ACL) reconstruction. Folia Anat 27:1–11
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P, Taylor DC et al (2003) Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 west point cadets. Am J Sports Med 31:831–842. https://doi.org/10.1177/03635465030310061801
Söderman K, Alfredson H, Pietilä T, Werner S (2001) Risk factors for leg injuries in female soccer players: a prospective investigation during one out-door season. Knee Surg Sports Traumatol Arthrosc 9:313–321. https://doi.org/10.1007/s001670100228
Chaudhari AM, Zelman EA, Flanigan DC, Kaeding CC, Nagaraja HN (2009) Anterior cruciate ligament-injured subjects have smaller anterior cruciate ligaments than matched controls: a magnetic resonance imaging study. Am J Sports Med 37:1282–1287. https://doi.org/10.1177/0363546509332256
Si HB, Zeng Y, Shen B, Yang J, Zhou ZK, Kang PD et al (2015) The influence of body mass index on the outcomes of primary total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 23:1824–1832. https://doi.org/10.1007/s00167-014-3301-1
National Federation of State High School Associations. NFHS 2002–2003 high school athletics participation survey. Indianapolis: National Federation of High School Associations.
Chia L et al (2022) Non-contact anterior cruciate ligament injury epidemiology in team-ball sports: a systematic review with meta-analysis by sex, age, sport, participation level, and exposure type. Sports Med 52:2447–2467. https://doi.org/10.1007/s40279-022-01697-w
Hewett TE (2000) Neuromuscular and hormonal factors associated with knee injuries in female athletes. Strategies for intervention. Sports Med 29(5):313–327. https://doi.org/10.2165/00007256-200029050-00003. (PMID: 10840866)
Hewett TE, Paterno MV, Myer GD (2002) Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop 402:76–94
Hewett TE, Stroupe AL, Nance TA, Noyes FR (1996) Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med 24:765–773
McLean SG, Neal RJ, Myers PT, Walters MR (1999) Knee joint kinematics during the sidestep cutting maneuver: potential for injury in women. Med Sci Sports Exerc 31:959–968
Lee K, Siegel MJ, Lau DM, Hildebolt CF, Matava MJ (1999) Anterior cruciate ligament tears: MR imaging-based diagnosis in a pediatric population. Radiology 213:697–704
van Eck CF, Martins CA, Vyas SM, Celentano U, van Dijk CN, Fu FH (2010) Femoral intercondylar notch shape and dimensions in ACL-injured patients. Knee Surg Sports Traumatol Arthrosc 18:1257–1262. https://doi.org/10.1007/s00167-010-1135-z
Anderson AF, Anderson CN, Gorman TM, Cross MB, Spindler KP (2007) Radiographic measurements of the intercondylar notch: Are they accurate? Arthroscopy 23:261–688
Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB (1987) Analysis of the intercondylar notch by computed tomography. Am J Sports Med 15:547–552. https://doi.org/10.1177/036354658701500605
Yellin JL et al (2021) Narrow notch width is a risk factor for anterior cruciate ligament injury in the pediatric population: a multicenter study. Arthrosc Sports Med Rehabil 3(3):e823–e828. https://doi.org/10.1016/j.asmr.2021.01.024
Bahr R, Krosshaug T (2005) Understanding injury mechanisms: a key component of preventing injuries in sport. Br J Sports Med 39:324–329
Lohmander LS, Östenberg A, Englund M, Roos H (2004) High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum 50:3145–3152
Anderson AF, Anderson CN, Gorman TM, Cross MB, Spindler KP (2007) Radiographic measurements of the intercondylar notch: are they accurate? Arthroscopy. 23:261–8
Görmeli CA, Görmeli G, Öztürk BY et al (2015) The effect of the intercondylar notch width index on anterior cruciate ligament injuries: a study on groups with unilateral and bilateral ACL injury. Acta Orthop Belg 81:240–244. https://doi.org/10.1177/2325967114S00204
Sonnery-Cottet B, Archbold P, Cucurulo T, Fayard JM, Bortolletto J, Thaunat M (2011) The influence of the tibial slope and the size of the intercondylar notch on rupture of the anterior cruciate ligament. J Bone Joint Surg Br 93:1475–1478. https://doi.org/10.1302/0301-620X.93B11.26905
Hirtler L, Röhrich S, Kainberger F (2016) The femoral intercondylar notch during life: an anatomic redefinition with patterns predisposing to cruciate ligament impingement. AJR Am J Roentgenol. 207:1–10. https://doi.org/10.2214/AJR.16.16015
Ghandour TM, Abdelrahman AA, Talaat AM, Ghandour AM, Al Gazzar HY (2015) New combined method using MRI for the assessment of tibial plateau slope and depth as risk factors for anterior cruciate ligament injury in correlation with anterior cruciate ligament arthroscopic findings: does it correlate? Egypt Orthop J 50:171–177. https://doi.org/10.4103/1110-1148.177928
Domzalski M, Grzelak P, Gabos P (2010) Risk factors for anterior cruciate ligament injury in skeletally immature patients: analysis of intercondylar notch width using magnetic resonance imaging. Int Orthop 34:703–707
Park JS, Nam DC, Kim DH, Kim HK, Hwang SC (2012) Measurement of knee morphometrics using MRI: a comparative study between ACL-injured and non-injured knees. Knee Surg Relat Res 24:180–185
Vrooijink SHA, Wolters F, Van Eck CF, Fu FH (2011) Measurements of knee morphometrics using MRI and arthroscopy: a comparative study between ACL-injured and non-injured subjects. Knee Surg Sports Traumatol Arthrosc Off J ESSKA 19(Suppl 1):S12–S16
Zeng C, Gao SG, Wei J, Yang TB, Cheng L, Luo W et al (2013) The influence of the intercondylar notch dimensions on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 21:804–815. https://doi.org/10.1007/s00167-012-2166-4
Bayer S, et al. Knee Morphological Risk Factors of ACL Injury: A Systematic Review. JBJS 2020
Iriuchisima T, et al. The Occurrence of ACL injury Influenced by the Variance in Width between the Tibial Spine and Femoral Intercondylar Notch. Knee Surg. Sports Traumatol. Arthrosc. 2020
Andrade R et al (2016) Notch morphology is a risk factor for ACL injury: a systematic review and meta-analysis. J ISAKOS 1(2):70–81. https://doi.org/10.1136/jisakos-2015-000030
O’Malley MP, Milewski MD, Solomito MJ, Erwteman AS, Nissen CW (2015) The association of tibial slope and anterior cruciate ligament rupture in skeletally immature patients. Arthroscopy 31:77–82. https://doi.org/10.1016/j.arthro.2014.07.019
Webb JM, Salmon LJ, Leclerc E, Pinczewski LA, Roe JP (2013) Posterior tibial slope and further anterior cruciate ligament injuries in the anterior cruciate ligament-reconstructed patient. Am J Sports Med 41:2800–2804. https://doi.org/10.1177/0363546513503288
Alentorn-Geli E, Pelfort X, Mingo F, Lizano-Díez X, Leal-Blanquet J, Torres-Claramunt R et al (2015) An evaluation of the association between radiographic intercondylar notch narrowing and anterior cruciate ligament injury in men: The notch angle is a better parameter than notch width. Arthroscopy 31:2004–2013. https://doi.org/10.1016/j.arthro.2015.04.088
Dare DM, Fabricant PD, McCarthy MM, Rebolledo BJ, Green DW, Cordasco FA et al (2015) Increased lateral tibial slope is a risk factor for pediatric anterior cruciate ligament injury: An MRI-based case-control study of 152 patients. Am J Sports Med 43:1632–1639. https://doi.org/10.1177/0363546515579182
Wordeman SC, Quatman CE, Kaeding CC, Hewett TE (2012) In vivo evidence for tibial plateau slope as a risk factor for anterior cruciate ligament injury: a systematic review and meta-analysis. Am J Sports Med 40:1673–1681. https://doi.org/10.1177/0363546512442307
Wang YL, Yang T, Zeng C, Wei J, Xie DX, Yang YH et al (2017) Association between tibial plateau slopes and anterior cruciate ligament injury: a Meta-analysis. Arthroscopy 33:1248–59.e4. https://doi.org/10.1016/j.arthro.2017.01.015
Dejour H, Bonnin M (1994) Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg Br 76:745–749
Ashwini T et al (2018) MRI correlation of anterior cruciate ligament injuries with femoral intercondylar notch, posterior tibial slopes and medial tibial plateau depth in the indian population. Int J Anat Radiol Surg 7(3):1–6. https://doi.org/10.7860/IJARS/2018/36086:2397
Mather RC et al (2013) Societal and economic impact of anterior cruciate ligament tears. J Bone Joint Surg 95(19):1751–1759. https://doi.org/10.2106/JBJS.L.01705
Acknowledgements
Thank you Dr Amitava Banerjee, Professor and head of Preventive Medicine, for study inputs and Dr Sudhir Jadhav and Shrivallabh Sane for helping with statistical analysis. Thank you Mr Dan Boyd and Ms Laura Swanton for reviewing the manuscript as native English speakers.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
SGM is main and corresponding author who has major contribution for diagnosing ACL injury measuring parameters, data entry, and writing manuscript. RK has developed study design. PL has done data stratification of MRI knees. JT has contributed basic data analysis and arranged statistician. RA contributed to the form of data presentation. MA selected important tables and arranged sequentially. TT has helped with arranging statistician for advanced tests. DB helped with study proforma questions. SK helped main author for manuscript writing and review of the literature. HN described result analysis section. SR helped in interpretation of ROC curve table data. ME drew few animations to figures. SV helped with authors guideline for writing manuscript. All authors read and approved the final manuscript after revision.
Corresponding author
Ethics declarations
Ethics approval and consent to participate.
Patient demographics and clinical history were compiled from the electronic patient records of the hospital. This study protocol was approved by the Scientific and Ethical Committee of the Institute (Reference: DYPV/EC/290/2019). Informed consent was obtained from all individual participants included in study. The confidentiality was strictly maintained regarding all personal details of the participants and information related to the study.
Consent for publication
Informed consent was obtained from all individual participants included in study. The confidentiality was strictly maintained regarding all personal details of the participants and information related to the study.
Competing interests
All financial and non-financial competing interests must be declared in this section. See our editorial policies for a full explanation of competing interests. If you are unsure whether you or any of your co-authors have a competing interest, please contact the editorial office. Please use the authors’ initials to refer to each authors’ competing interests in this section. If you do not have any competing interests, please state “The authors declare that they have no competing interests” in this section.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Maheshwari, S.G., Kuber, R., Lamghare, P. et al. Anterior cruciate ligament (ACL) injury: correlation with MRI morphometry. Egypt J Radiol Nucl Med 54, 130 (2023). https://doi.org/10.1186/s43055-023-01073-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01073-2