
Abstract
Background
Autoimmune thyroiditis (AIT) is the most common thyroid pathology in pediatric patients among which Hashimoto’s thyroiditis has the highest prevalence. Along with size, measuring mechano-acoustic tissue elasticity is evolving as an important parameter in the evaluation of diffuse thyroid pathology. This study aims to investigate the role of shear wave elastography (SWE) in the diagnosis of autoimmune thyroid disease (AITD) in the pediatric population and also compare the elasticity between them and healthy individuals.
Results
This case–control analytical study was carried out on 64 pediatric subjects ranging in age from 7 to 17 years. All the cases were diagnosed as AIT by anti-thyroid antibodies, and their thyroid function was evaluated by thyroid hormones. We performed thyroid Ultrasonography and Shear wave elastography. Patients with AIT had significantly higher elasticity values (35.6 kPa, IQR 8.43–103.7 kPa) than the control group (9.35 kPa, IQR 5.73–13.21 kPa). There was no correlation of elasticity values of thyroid gland in patients with AIT with autoantibodies and thyroid function test, respectively. The cutoff value for elasticity was 12.317 kPa with sensitivity and specificity of 96.9% and 100%, respectively.
Conclusions
SWE is a highly sensitive imaging method integrating routine ultrasonography in the diagnosis of AITD which estimates the extent of fibrosis in numerical value.
Similar content being viewed by others


Background
Autoimmune thyroiditis (AIT) is the commonest pediatric thyroid pathology. It entails glandular lymphocytic infiltration and consequently fibrosis which may alter tissue elasticity [1] There are many autoimmune diseases that are associated with autoimmune thyroiditis other than Hashimoto’s thyroiditis (HT) and Graves’ disease including; pernicious anemia, systemic or ocular myasthenia, immune thrombocytopenia, Addison's disease, type 1 insulin-dependent diabetes mellitus and vitiligo [2].
Elastography is an evolving imaging tool quantitatively evaluating the elasticity of the tissues, with additive diagnostic value to the routine ultrasound assessments for thyroid pathologies being focal or diffuse [3].
Shear wave elastography through measuring the propagation speed of its waves within certain tissues can reflect their stiffness [4] and represent it in unit measurements as kilopascals or meters per second [5]. Operator dependability, when compared with strain Elastography, is lower ensuring more accurate information on tissue elasticity [6].
Methods
Study population
Over a 6 months period, we prospectively evaluated 64 patients, 32 with autoimmune thyroiditis (AIT) (5 males and 27 females) and 32 healthy volunteers (9 males and 23 females), ranging in age from 7 to 17 years. Patients were diagnosed by the treating endocrinologist as well as the patient’s clinical and laboratory records. This was done after approval from the institutional review board. Written consent was taken before performing sonoelastography. Our control group subjects were recruited from patients performing radiological examinations for various complaints other than thyroid-related diseases. We excluded patients who underwent thyroid surgery or fine needle biopsy in the previous 6 months for possible alterations in the parenchyma of the thyroid gland.
Clinical examination
Detailed history of chief complaints, the onset of symptoms, associated autoimmune diseases and family history of any thyroid diseases were taken.
Laboratory investigations
Results of anti-thyroid peroxidase (TPOAb) and/or antithyroglobulin (TGAb), and other specific antibodies according to autoimmune diseases, along with Thyroxine (T4), Tri-iodothyronine (T3), thyroid-stimulating hormone (TSH) are obtained.
Imaging
The examination was performed with the patients in a supine position having their necks extended by a pillow. The subjects were advised not to move and swallow during the examination. Ultrasound Sonography system (Toshiba APLIO 400) was used to perform thyroid ultrasonography and shear wave elastography using linear wave transducer (frequency 7–14 MHz).
Ultrasound
During dedicated ultrasound examination of the thyroid gland, dimensions and volumes of the gland were calculated by using the formula width (cm) × length (cm) × depth (cm) × 0.523. The assessment of parenchymal pathologies altering gland’s echogenicity was decided upon by comparing the gland’s echogenicity to that of strap muscles, and we also reported the degree of heterogeneity, thyroiditis foci, and pseudo-nodular appearance.
Shear wave elastography (SWE)
SWE software was activated. In split-screen mode, the 2-dimensional SWE map of both thyroid lobes was examined. We obtained three measurements in the longitudinal plane for each lobe using a 3 mm rounded ROI, measurements were represented in kPa. The mean stiffness values in each lobe were calculated as the average of the three measurements. We were keen to exclude the main carotid artery from the 2-dimensional SWE map to avoid pulsation artifact.
Detailed sonographic and elastographic evaluation of thyroid gland was interpreted on basis of the following findings (Figs. 1, 2,3,4,5 and 6):
-
Dimensions of both thyroid lobes: length, width and depth
-
Echotexture: Homogeneous or heterogeneous parenchymal interface
-
Nodules present or absent
-
Vascularity of the thyroid gland: whether normal or increased or decreased.
-
Elasticity of both thyroid lobes.

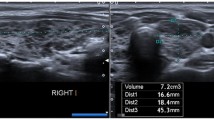
Thyroid ultra-sound of a 9 years female with history of neck swelling since 4 years with positive TPOAb and TGAb, T4 1.1 and TSH 0.07 diagnosed as Hashimoto’s thyroiditis under medication with tab eltroxin showing heterogeneous texture of both thyroid lobes with multiple scattered hypoechoic micronodules and hyperechoic septations

Elastography of right thyroid gland measuring elasticity (33.7, 30.9 and 23.2 kPa

Thyroid Ultrasound of a 13 years old female with history of neck swelling since 4 years, positive TPOAb and TGAb, T4 1.6, T3 3.1 and TSH 6.8 under medication with tab. Carbimazole and diagnosed as Grave’s disease. The gland shows increased size of right lobe with coarse echotexture, hyperechoic septations giving pseudonodular appearance with few scattered micro hypoechoic nodules and increased vascularity

SWE of right thyroid lobe showing three measurements of elasticity 66.1, 61.8 and 54.3 kPa

a Gray scale findings in an 8-year-old female with positive anti-thyroglobulin and anti-microsomal antibodies, showing inhomogeneous increased echogenicity with hyperechoic septations of both thyroid lobes. b SWE showing three measurements of elasticity (36.3, 24.3 and 23.47 kPa) of right thyroid lobe in longitudinal plane

a Gray scale ultrasound of the thyroid gland, in an 8-year-old female with history of Crohn’s disease and neck swelling for 2 years. TPO-Ab positive and TG-Ab borderline, diagnosed as Hashimoto’s thyroiditis. The gland is of homogeneous hyperechoic echotexture with normal dimensions of both glands and vascularity. b ,c SWE of thyroid glands measuring elasticity of both thyroid glands (b) right thyroid lobe (15.7, 14.3 and 9.5 kPa) c left thyroid lobe (8.1,8.1 and 10.4 kPa)
Statistical analysis
Descriptive statistical analysis was carried out in the present study using SPSS version 22. Descriptive data statistics which included the mean, median, SD and range were calculated. Kolmogorov–Smirnov test was used to analyze a range of variables. The Mann–Whitney U test was used for comparison between patients with autoimmune-related thyroid disease and control. The analysis of correlation was evaluated with the spearman correlation test. ROC curve was plotted for elasticity values and the optimum elasticity cutoff value was determined. Sensitivity, Specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.
Results
This case–control analytical study included a total of 64 patients (32 patients with autoimmune thyroiditis (AIT) and 32 healthy volunteers without any known thyroid pathologies).
Healthy control group
The mean and median age of the healthy control group were 10.56 ± 2.39 years and 10 years (range 7–16 years), respectively. The number of male and female was 9 and 23, respectively. Table 1 presents a descriptive analysis of age, volume, and elasticity in healthy control.
Autoimmune thyroiditis (AIT) patient group
The mean and median age of the Autoimmune thyroiditis (AIT) group were 11.31 ± 2.77 years and 11 years (range 7–17 years), respectively. The number of male and female was 5 and 27, respectively. Descriptive analysis of age, volume and elasticity in AIT Table 2 presents descriptive analysis of age, volume, and elasticity in AIT.
Correlation between elasticity, autoimmune antibodies, and thyroid hormones:
The correlation between elasticity values and auto-antibodies [anti thyroid peroxidase (TPOAb) and anti-thyroglobulin (TGAb) levels] in AIT groups were non-significant (p > 0.05), as given in Table 3. Also, there was no significant correlation between elasticity values and thyroid function test (T4 & TSH) in children with AIT, i.e., their p-value > 0.05, as given in Table 4.
Comparison of elasticity values between healthy and AIT groups:
In children with autoimmune thyroiditis, thyroid SWE (Fig. 2) values were significantly greater than those of healthy children (p-value < 0.05, n1 = n2 = 32, Ustat = 12, Ucritical = > 172, Ustat < Ucritical), as given in Table 5
ROC curves analysis:
ROC curve analysis of the SWE values of AIT was calculated; kPa is given in Fig. 7.The maximum area under the curve(AUC) for the mean elasticity value of both lobes in AIT was 0.978(95% confidence interval).The cutoff value with the highest diagnostic accuracy for elasticity value was 13.217 kPa; Sensitivity, Specificity, positive predictive value (PPV),and negative predictive value (NPV) were 96.9%, 100%, 100% and 96.9%, respectively with diagnostic accuracy of 98%, as given in Table 6

ROC curve showing the optimal SWE cutoff value for autoimmune thyroiditis
Discussion
Diffuse thyroid disease in the pediatric population can lead to gross metabolic abnormalities affecting development and growth rendering early accurate diagnosis mandatory [7]. Traditionally the diagnosis is achieved by clinical examination, thyroid hormones levels, and thyroid ultrasonography [8]. Thyroid ultrasound is pivotal to the assessment of the gland’s echogenicity, volume, and vasculature as well as any related or surrounding abnormality [9]. SWE is a recent ultra-sound-based elastography method with the ability to quantitatively evaluate thyroid gland stiffness using the concept of strain elastography [10]. Any diffuse thyroid disease with its disease-related histological changes, e.g., follicular cell hyperplasia, lymphocytic infiltration, and colloid accumulation will change the glandular elastic properties, and if these histological changes proceed for a longer time, fibrosis, septations, and focal nodularity may evolve [11].
In the present study, we attempted to perform conventional thyroid Ultrasound to patients with autoimmune thyroiditis and normal participants calculating the gland’s volume and examining its parenchyma for echogenicity, the extent of heterogeneity, and pseudo-nodular appearance. Regarding the volume of the thyroid gland, we observed patients with AIT had significantly higher total thyroid volume (10.88 ml; IQR 0.6–22.47 ml) than control subjects (5 ml; IQR 2.87–7.87 ml). This matched the results of a previous retrospective study done by Kandemirli et al. [12] whose study population’s total thyroid volume with AIT was significantly higher than that of the healthy control group (HT group:9.73 ml; IQR 5.31–16.73 ml, control subjects: 4.11 ml; IQR 2.42–5.72 ml).
Ultrasonography is a widely used imaging tool in the diagnosis and follow-up of AIT. Its reported common findings of glandular heterogeneity, hypoechogenicity, and lobulated outline though specific are hardly sensitive [13]. The AIT disease-related histological changes including lymphocytic infiltration and interstitial fibrosis [14] consequently lead to parenchymal stiffness when compared to healthy thyroid tissue which will be invariably reflected in elasticity values [15]. In our study, elasticity mean values are higher in patients with autoimmune thyroiditis as compared to normal subjects in the same age group. Our reported mean elasticity value of the healthy control group was 9.35 ± 1.63 kPa (5.7–13.21 kPa) and the AIT group was 35.63 ± 20.30 kPa (8.43–103.7 kPa) which was close to the elasticity values of Kara et al. [16] who studied 149 participants ranging from 8 to 60 years showing the result of mean elasticity value in patient with AIT to be 25.01 ± 10.53 kPa (10.72–68.27 kPa). The elasticity values were also close to many other studies [17,18,19,20,21].
Kandemirli et al. [12] studied 59 patients diagnosed with HT and 26 healthy volunteers without any thyroid-related disorders, they used a scoring system based on gray-scale ultrasonographic findings subdividing patients with Hashimoto thyroiditis into three categories as follows: focal thyroiditis (grade 1), diffuse thyroiditis (grade2), and fibrotic thyroid gland (grade 3). Based on elasticity values, grade 3 patients had the highest and the most significant elasticity values (19.7 kPa; IQR 17.8–21.5 kPa) when compared to the patients with grade 2 (15.5 kPa; IQR 14.5–17.8 kPa) and grade 1 thyroiditis (12.8 kPa; IQR 11.9–13.1 kPa). Vlad et al. [21] also studied 104 patients the mean elasticity value in patients with AIT was found to be 26.2 ± 10.8 kPa with SWEmax 52.4 ± 24.6Kpa. In our study, the SWE of thyroid gland in children with AIT was found to be 35.63 ± 20.3; IQR 8.43–103.7 kPa which is consistent with the values of Ruchala et al. [17] which had reported having baseline thyroid stiffness in chronic autoimmune thyroiditis(CAT) to be 36.15 ± 18.7 kPa.
In healthy children our mean SWE was found to be 9.35 ± 1.63 kPa; IQR 5.73–13.21 kPa which is the approximate SWE postulated by Bhatia et al. [22] (9.0 ± 4.0 kPa).
In the study conducted by Kandemirli et al. [12] they reported no significant correlation between SWE and TGOAb in patients with HT. Our study also showed a negative correlation between SWE, TPOAb and TGAb. In concordance with Kara et al. [16], our study showed no positive correlation between SWE and TFT(TSH & T4) as well.
The cutoff value of elasticity in our study was 12.317 kPa with sensitivity, specificity, and accuracy rates of 96.9%, 100% and 98%, respectively. The cutoff value with the highest diagnostic accuracy for elasticity value in the study conducted by Fukuhara [19] was 12.3 kPa with reported sensitivity, specificity, and accuracy rates of 87.4%, 78.7% and 85.1%, respectively.
In our study, we were dependent on clinical examination, ultrasound findings, and laboratory tests, to diagnose AIT rather than tissue biopsy which we consider a limitation, this being rather controversial as any fine needle biopsy or surgery would have altered the gland parenchyma. In addition, most of our patients were under medication with Eltroxin and some of them were on the carbimazole medication. We considered this irrelevant guided by previous studies which reported no significant elasticity changes when comparing treated and non-treated patients [18, 23]. We also ignored age-related changes having a rather narrow age group; this was decided upon because previous studies documented statistically insignificant changes with narrow age gaps [24].
Conclusions
SWE is a useful and highly sensitive imaging method that complements routine ultrasonography examination in children with autoimmune thyroid disease by providing objective numerical values and estimating the degree of fibrosis. However, further studies are recommended to seek out the conventional reference values per age groups in the pediatric population. Larger cohorts in the Egyptian population are needed to compare the elasticity values of normal and pathologic tissues.
Availability of data and materials
Data available within the article or its supplementary materials.
Abbreviations
- AIT:
-
Autoimmune thyroiditis
- SWE:
-
Shear wave elastography
- AITD:
-
Autoimmune thyroid disease
- TPOAb:
-
Anti-thyroid peroxidase
- TGAb:
-
Antithyroglobulin
References
Palabıyık FB, İnci E, Çakır EDP, Hocaoğlu E (2019) Evaluation of normal thyroid tissue and autoimmune thyroiditis in children using shear wave elastography. J Clin Res Pediatric Endocrinol 11(2):132–139. https://doi.org/10.4274/jcrpe.galenos.2018.2018.0137
Biró E, Szekanecz Z, Dankó K, Kiss E, Szabó NA, Szűcs G, Zeher M, Bodolay E, Szegedi G, Bakó G, Czirják L (2006) Association of systemic and thyroid autoimmune diseases. Clin Rheumatol 25(2):240
Uysal E, Öztürk M (2019) Quantitative assessment of thyroid glands in healthy children with shear wave elastography. Ultrasound Q 35(3):297–300
Hermana J, Sedlackovab Z, Vachutk J (2017) Shear wave elastography parameters of normal soft tissues of the neck. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 161(3):320–325
Öztürk M, Çaliskan E, Bayramoglu Z, Adaletli I (2018) Quantitative assessment of palatine tonsils in healthy children and adolescents with shear-wave elastography. Ultrasound Q 34(4):213–218
Bilgici MC, Sağlam D, Delibalta S, Yücel S, Tomak L, Elmalı M (2018) Shear wave velocity of the healthy thyroid gland in children with acoustic radiation force impulse elastography. J Med Ultrason 45(1):75–80
Brown RS, Huang S (2005) The thyroid and its disorders. In: Brooks CG, Clayton PE, Brown RS (eds) Brooks pediatric clinical endocrinology, 5th edn. Blackwell Publishing, Massachusetts, pp 218–253
Sporea I, Sirli R, Bota S, Vlad M, Popescu A, Zosin I (2012) ARFI elastography for the evaluation of diffuse thyroid gland pathology: Preliminary results, world. J Radiol 4:174–178. https://doi.org/10.4329/wjr.v4.i4.174
Pishdad P, Pishdad GR, Tavanaa S, Pishdad R, Jalli R (2017) Thyroid Ultrasonography in differentiation between graves’ disease and hashimoto’s thyroiditis. J Biomed Phys Eng 7:21–26
Sun J, Cai J, Wang X (2014) Real-time ultrasound elastography for differentiation of benign and malignant thyroid nodules: a meta-analysis. J Ultrasound Med 33(3):495–502. https://doi.org/10.7863/ultra.33.3.495
Perez-Montiel MD, Suster S (2008) The spectrum of histologic changes in thyroid hyperplasia: a clinicopathologic study of 300 cases. Hum Pathol 39(7):1080–1087. https://doi.org/10.1016/j.humpath.2007.12.001
Kandemirli SG, Bayramoglu Z, Caliskan E, Sari ZN, Adaletli I (2018) Quantitative assessment of thyroid gland elasticity with shear-wave elastography in pediatric patients with Hashimoto’s thyroiditis. J Med Ultrason 45(3):417–423
Hekimoglu K, Donmez FY, Arslan S, Ozdemir A, Demir C, Yazici C (2015) The role of shear wave elastography in the diagnosis of chronic autoimmune thyroiditis. Med Ultrason 17(3):322–326
Caturegli P, De Remigis A, Rose NR (2014) Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmun Rev 13(4–5):391–397
Arda K, Ciledag N, Aktas E, Arıbas BK, Köse K (2011) Quantitative assessment of normal soft-tissue elasticity using shear-wave ultrasound elastography. Am J Roentgenol 197(3):532–536
Kara T, Ateş F, Durmaz MS et al (2020) Assessment of thyroid gland elasticity with shear-wave elastography in Hashimoto’s thyroiditis patients. J Ultrasound 23:543–551
Ruchala M, Szczepanek-Parulska E, Zybek A, Moczko J, Czarnywojtek A, Kaminski G, Sowinski J (2012) The role of sonoelastography in acute, subacute and chronic thyroiditis: a novel application of the method. Eur J Endocrinol 166(3):425
Ruchała M, Szmyt K, Sławek S, Zybek A, Szczepanek-Parulska E (2014) Ultrasound sonoelastography in the evaluation of thyroiditis and autoimmune thyroid disease. Endokrynol Pol 65(6):520–531
Fukuhara T, Matsuda E, Izawa S, Fujiwara K, Kitano H (2015) Utility of shear wave elastography for diagnosing chronic autoimmune thyroiditis. J Thyroid Res 1:2015
Hekimoglu K, Donmez FY, Arslan S, Ozdemir A, Demir C, Yazici C (2015) The role of shear wave elastography in the diagnosis of chronic autoimmune thyroiditis. Med Ultrason 17(3):322–326
Vlad M, Golu I, Bota S, Vlad A, Timar B, Timar R, Sporea I (2015) Real-time shear wave elastography may predict autoimmune thyroid disease. Wien Klin Wochenschr 127(9):330–336
Bhatia K, Tong CS, Cho CC, Yuen EH, Lee J, Ahuja AT et al (2012) Reliability of shear wave ultrasound elastography for neck lesions identified in routine clinical practice. Ultraschall Med 33:463–468
Palabıyık FB, İnci E, Çakır EDP, Hocaoğlu E (2019) Evaluation of normal thyroid tissue and autoimmune thyroiditis in children using shear wave elastography. J Clin Res Pediatric Endocrinol 11(2):132–139. https://doi.org/10.4274/jcrpe.galenos.2018.2018.0137
Ceyhan Bilgici M, Saglam D, Delibalta S, Yücel S, Tomak L, Elmalı M (2001) Shear wave velocity of the healthy thyroid gland in children with acoustic radiation force impulse elastography. J Med Ultrason 45(2018):75–80
Acknowledgements
We acknowledge all patients who were involved in the study.
Funding
No source of funds.
Author information
Authors and Affiliations
Contributions
SM and WA have designed this study together. SB and KM contributed to the data collection, SB and SM contributed to data analysis. SB contributed to data processing. SM and WA shared together in writing the manuscript. ALL authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This study was approved by the Ethical Research Committee of Faculty of Medicine Cairo University in Egypt. The ethics committee reference number is not available. A written consent was taken from the legal guardians of all patients accepting to participate in our research work.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declared that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kamel, S.M., ElKhashab, K.M., Bhagat, S. et al. Shear wave elastography as a quantitative method for thyroid gland elasticity assessment in pediatrics patients with autoimmune-related thyroid disease, diagnostic utility and laboratory correlation. Egypt J Radiol Nucl Med 53, 189 (2022). https://doi.org/10.1186/s43055-022-00882-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00882-1