
Abstract
Background
On mammography many cancers may be missed even in retrospect either due to the breast density, the small size of the tumor or the subtle signs of cancer that are imperceptible. We aimed to compare the sensitivity of artificial intelligence (AI) to that of digital mammography in the detection of different types of breast cancer. Also, the sensitivity of AI in picking up the different breast cancer morphologies namely mass, pathological calcifications, asymmetry, and distortion was assessed. Tissue biopsy and pathology were used as the standard reference. The study included 123 female patients with 134 proved carcinoma. All patients underwent digital mammogram (DM) examination scanned with artificial intelligence algorithm.
Results
AI achieved higher sensitivity than mammography in detecting malignant breast lesions. The sensitivity of AI was 96.6%, and false negative rate was 3.4%, while mammography sensitivity was 87.3% and false negative rate 12.7%. Our study showed AI performed better than mammography in detecting ductal carcinoma in situ and invasive lobular carcinoma with sensitivity (100% and 96.6%) vs (88.9% and 82.2%) respectively. AI was more sensitive to detect cancers presented with suspicious mass 95.2% vs 75%, suspicious calcifications 100% vs 86.5% and asymmetry and distortion 100% vs 84.6%, than mammography.
Conclusions
AI showed potential values to overcome mammographic limitations in the detection of breast cancer even those with challenging morphology as invasive lobular carcinoma, ductal carcinoma in situ, tubular carcinoma and micropapillary carcinoma.
Similar content being viewed by others

Background
In 2018, an estimated 2.1 million cases of breast cancer were diagnosed around the world, with an estimated 630,000 breast cancer related deaths. Countries with low human developmental index show a greater incidence of cases among premenopausal women [1].
Mammography is the first tool for detection and diagnosis of breast cancer. It’s readily available and cost effective. Unfortunately, mammography being a two-dimensional imaging tool has its well-established limitations. Tissue superimposition may mimic or mask an underlying lesion. This is especially evident in premenopausal women who have dense breasts [2].Recent advances in AI hold a great promise not only for detection of breast cancer, but for risk assessment, diagnosis, prognosis and monitoring response to therapy [3]. AI can be used as an independent preliminary reader of mammographic images, with near human reader accuracy. By doing so it can help save time and effort of radiologists and reduce false positive results [4].
The main aim of the current study was to assess the sensitivity of screening or diagnostic mammograms aided by artificial intelligence in detecting the different histologic types of breast cancer. Also, the sensitivity of artificial intelligence in detecting different cancer morphology was estimated.
Methods
The study was prospectively carried out on 123 female patients with 134 pathologically proven malignant breast lesion, during the period from December 2020 to June 2021. Eleven cases showed bilateral carcinomas and 30 patients showed multiple masses (multifocal, n = 24 and multicentric, n = 6).
Inclusion criteria: patients presented for either screening or diagnostic mammogram and were pathologically proven to have breast carcinoma.
Exclusion criteria: patients with proven benign masses or benign masses on follow up, patients on chemotherapy or after breast surgery and pregnant patients (contraindicated for mammography).
All patients underwent baseline examination of digital mammogram (DM). Ultrasound guided biopsy was performed for the included lesions. Image interpretation was carried out by two radiologists with at least 15 years of experience in breast imaging. Image interpretation was at individual sessions and readers were blinded about the pathology of the included masses. Diagnosis was achieved by consensus.
The results of AI & DM were correlated to the pathology as the standard reference.
Breast Mammography: was performed by digital mammography, (manufacture: Amulet Innovality, Fujifilm Gobal company, Japan). Mammography machines were supported with a “Bellus” workstation of resolution five megapixels. Standard two views were taken for each breast in the medio-lateral and cranio-caudal positions. On average the total dose for a typical mammogram with 2 views of each breast was about 0.4 millisieverts (mSv). Breast ultrasound (US): was performed to characterize mammographic abnormalities into pure cystic, solid or complex, verify benign abnormalities and for guiding biopsy. HS60 Samsung ultrasound, Korea, 2019 device equipped with a linear probe of 9–13 MHz was used. All the real-time scanning was performed by a radiologist with at least 15 years of experience in breast ultrasound. Artificial intelligence images were generated from mammographic images by (Lunit INSIGHT MMG, Korea, version 2019) for Fujifilm digital mammography system. This AI software generates score (susceptibility of malignancy) from < 10 to 100%, below 10% considered “Low” scoring (No registered scoring percentage). For an input mammogram image (i.e., one of the four views), the AI algorithm provides pixel-level abnormality scores as a heat map and a representative abnormality score, which is the maximum of the pixel-level abnormality scores. The abnormality scores are floating-point values between 0 and 100. Sensitivity and specificity were calculated with the cutoff threshold of 10% (i.e., if the abnormality score is ≥ 10%, then positive; otherwise, negative). The statistical material and methods: Data were coded and entered using the statistical package for the Social Sciences (SPSS) 22nd edition, continuous variables were presented in mean ± SD and were compared using Mann Whitney U test, and Kruskal Wallis test. Categorical variables were presented in frequency ad percentage and paired variables were compared using McNamara test. Spearman correlation test was used to correlate two continuous variables.
Results
The patients’ age ranged between 32 to 80 years old (mean age was 53.6 ± SD 12.0 years old).
Most of the patients had a mammographic breast density of “ACR b” (59.7%) and “ACR c” (32.1%).
The pathological entities of the included carcinoma: IDC (n = 91), ILC (n = 29), DCIS (n = 9), and other rare forms as micropapillary carcinoma, borderline phyllodes tumor and tubular cribriform carcinoma (n = 5) where, IDC (68%) was the most prevalent pathology.
Sensitivity according to pathological type of cancer
Cancer was detected at the right breast in 87 (65%) and at the left side in 47 (35%). According to pathological type of breast cancer, mammography demonstrated a sensitivity of 89% in detecting IDC, 82.2% in detecting ILC, 88.9% in detecting DCIS and 80% in detecting other histopathological types of breast cancer, as shown in Table 1.
AI system demonstrated a sensitivity of 96.7% in detecting IDC, 96.6% in detecting ILC, 100% for detection of DCIS, and 80% for detection of other malignant types, as shown in Table 2.
Overall, the AI system demonstrated 96.6% sensitivity and 3.4% false negative rate, whereas mammography demonstrated 87.3% sensitivity and 12.7% false negative rate in detection of different types of breast cancer. False negative results on AI were 3 cases: 1 case of IDC, 1 case of ILC, and 1 case of borderline phyllodes carcinoma (Table 3).
Sensitivity according to lesion morphology
Suspicious findings on mammography and AI imaging were categorized into either a suspicious mass, suspicious calcifications, asymmetry and distortion. The sensitivity of the digital mammography in detecting suspicious mass was 84.6%, in detecting asymmetry and distortion was 75% and in detecting calcification was 86.5%. The sensitivity of AI in the detection of suspicious calcifications was 100%, suspicious mass was 95.2%, while the asymmetry and distortion were 100% (Table 4).
Discussion
Early detection of breast cancer through screening is the most effective method for reducing cancer related morbidity and mortality. Despite its benefits, mammography has limited sensitivity especially in dense breasts. Among the recent advances aiming to combat the limitations of mammography is the use of AI [5].
In 1990s, CAD (computer aided detection) was introduced to increase radiologists accuracy in detection and diagnosis of breast cancer. But no true clinical benefit was achieved as a result. Eversince, there has been an ongoing research to develop more advanced technology, such as deep learning. Deep learning models are not limited by the human understanding of what a breast cancer looks like, but rather teach themselves what to look for after being exposed to multiple examples of normal and pathological images [6].
In the current work, AI achieved higher sensitivity than mammography in detecting the different types of malignant breast lesions and the commonest carcinoma was IDC (68%), Fig. 1.

Screening mammogram of a 60-year-old female patient. A Digital mammography cranio-caudal views of both breasts. Left breast upper outer focal area of increased density and distortion (arrow). B AI heatmap showed left breast upper outer high intense color hue of 91% score of malignancy suspicion. C On ultrasound, a small indistinct solid mass was detected. Wire localization and excision biopsy revealed IDC. Localization of the disease was more feasible by the aid of the AI and the suspicion of malignancy was confirmed
The sensitivity of AI was 96.6%, and false negative rate 3.4%, while mammographic sensitivity was 87.3% and false negative rate 12.7%. AI performed better than mammography in detecting different histopathological types of breast malignancy namely DCIS, IDC and ILC with sensitivity (100%, 96.7%, 96.6%) vs (88.9%, 89%, 82.2%) respectively. While in other rare types of breast malignancy (micropapillary carcinoma, borderline phyllodes tumor and tubular cribriform carcinoma), both AI and mammography showed the same sensitivity 80%.
The current results were consistent with multi-institutional studies such as the one performed by Kim et al. [7] in South Korea, the USA, and the UK. They reported that AI standalone sensitivity in the three validation datasets was 91%. Another retrospective study based on the screening programe in Western Australia reported that AI based systems outperfomed human radiologists with 14.2% increase in senitivity [8].
Close results were attained by Ribli et al. [9] where the AI emloyed system achieved AUC = 0.95, (95 percentile interval: 0.91 to 0.98, estimated from 10,000 bootstrap samples). Meanwhile, Watanabe et al. [10] reported that with the aid of an AI system, the cancer detection rate among radiologists increased from an average of 51% to 62%.
Our findings are also agreeing with smaller scale studies [11,12,13,14,15,16]. Rodriguez-Ruiz et al. [17] in 2019, performed a study on 240 mammograms (100 cancers, 40 leading to false-positive recalls, 100 normal) reported that sensitivity increased with AI support to 86% vs 83% with mammography alone. Other study by Pacilè et al. [12] in 2020, which was carried out on 240 participants, also reported that average sensitivity of radiologists was increased by 0.033 when using AI support (P = 0.021). Sasaki et al. [13] also suggested that AI can increase the sensitivity of human readers from 89 to 96%.
Although several studies discussed the role of AI in cancer detection among screening mammograms, few studies addressed its significance in detecting different types of cancer and their different mammographic appearances. Our study showed that AI was more sensitive to detect cancers with suspicious mass 95.2% vs 75%, suspicious calcifications 100% vs 86.5% and asymmetry and distortion 100% vs 84.6%, than mammography.
This study results went with Kim et al. [7] who reported AI sensitivity in detecting soft tissue lesions (mass, asymmetry and distortion) to be 89.8% vs 71.6% for reading mammograms by unassissted radiologists. Also in their study the AI showed better sensitivity than radiologists in detecting microcalcifications (87.6% vs 71.4%).
Another study also suggested that in malignant cases, AI performed better than mammography in both mass detection and calcifications. (84.1–86.1% vs 77.5–77.9%) [18]. Furthermore, in Conant et al. study [14], sensitivity of AI in cases with only calcifications was 100% and was 88% in cases with soft-tissue densities with or without calcifications.
The AI system employed in the current study showed 100% senitivity in detection of DCIS. This could be explained through the pathological nature of DCIS where calcification is a prominent feature [19]. Our study showed ability of AI to detect pathological calcification at a sensitivity rate of 100%.
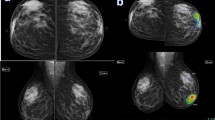
In mammographic imaging, ILC doesn’t always present as a mass. It may have vague appearances in the form of architectural distortion, asymmetry, or even breast size discrepencies, making it one of the most missed pathological types of cancer on mammography (up to 30% of missed cancers). Mammographic sensitivity in detecting ILC ranges from 86 to 100% in fatty breasts down to 45–68% in extremely dense breasts [19]. It was found in the current study that AI can overcome the limitations of mammography in cases of ILC, Fig. 2. It shows better sensitivity than mammography in detecting that type of carcinoma (96.7% vs 89%).

A 43-year-old female patient presenting with mastalgia. A, B Digital mammography in cranio-audal and mediolateral oblique views respectively of both breasts. They show extremely dense breasts (ACR d) with asymmetries and subtle distortions (arrows). C AI: showing right breast large UOQ suspicious area with 92% score of malignancy. The left breast also shows UOQ as well as retro areolar suspicious areas, with 89% score of malignancy. Both breast lesions elicit red and green heat maps which reflected high probability of malignancy on the color-coded scale. Ultrasound guided True-cut biopsy was performed and revealed bilateral ILC. In this case AI was able to illustrate the disease bilaterality and multicentricity on the left side which was not evident on mammography
The applied color hue provided by the AI scanning delineated the full extent of the disease not just targeted the site of the abnormality on the mammogram [20]. Such criteria helped to determine the multifocal or multicentric distribution of the included carcinomas, Figs. 2 and 3.

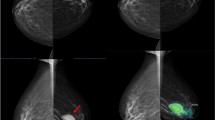
A 58-year-old female patient with left breast proved micropapillary carcinoma. A Digital mammography of the left breast. There is focal large circumscribed mass in the lower inner quadrant and related indistinct asymmetrical densities. B Ultrasound image showed purely solid mass. C Contrast enhnaced mammogram of the left breast showed rim enhancement of the mass suggestive of being malignant and suspicious enhancment of the related asymmetries (i.e. likely multifocal carcinoma). D AI- scanned four images mammogram that represent high intensity red color hue that involved the mass and the nearby minions comparable to the features at the contrast enhanced mammogram with definite cancer suggestion of high scoring percentage of 98%. In this case, the AI detected the carcinoma and also the satellites were marked by the color hue giving the exact dimensions of the disease
Regarding the histopathological types of breast cancer, this work was consistent with a study performed by Lang et al. [4]. In agreement with our results, AI showed high sensitivity in detecting both IDC, ILC, and DCIS. The AI in their study missed three tubular carcinoma, two IDC and one ILC. Our results reflected more or less similar findings, as in the current work the AI algothrium missed three cases of IDC, one case of ILC, and one case of borderline phyllodes carcinoma.
However, the AI algorithm sometimes underestimate breast lesions that lack the morphologic features of malignancy on the mammogram. As a result, no demarcation by the color hue was noted at the heatmap images and the given abnormality scoring for the breast showed accordingly a “Low” scoring, Fig. 4. To get the best performance of AI in correlation with mammogram; complementary ultrasound is mandatory to decrease the incidence of false negative results in case of diagnostic mammogram or screening mammogram with high breast density [21].

Screening mammogram of a 45-year-old female patient with left breast proved invasive ductal carcinoma. A Digital mammography medio-lateral and cranio-caudal views of both breasts. There is a left breast axillary tail tiny lobulated mass (arrow). B AI- scanned four images mammogram that showed no color demarcation and “Low” scoring percentage. C Ultrasound image showed tiny lobulated solid mass in plane with the breast tissue. The detected left breast mass showed no suspicion of malignancy and was false negative by the sono-mammogram and AI
Lang et al. [4] and our study both showed 100% sensitivity in detection of DCIS, which highlights AI’s advantage in detection of pathological microcalcifications.
This study has some limitations. It is limited by the relatively small sample size. We did not study the interaction of a human interpreter with AI algorithm results and how AI will affect radiologists’ final assessment. The used AI algorithm does not take into account clinical factors such as symptoms or family history, which may limit comprehensive analysis.
Conclusions
AI showed promising aspects in detection of different histopathological types of breast cancer. It showed the potential to overcome mammographic limitations with certain challenging malignant pathologies as invasive lobular carcinoma, ductal carcinoma in situ, tubular carcinoma and micropapillary carcinoma.
Availability of data and materials
The corresponding author is responsible for sending the used data and materials upon request.
Change history
06 September 2022
A Correction to this paper has been published: https://doi.org/10.1186/s43055-022-00884-z
Abbreviations
- AI:
-
Artificial intelligence
- DM:
-
Digital mammography
- SD:
-
Standard deviation
- ACR:
-
American College of Radiology
- IDC:
-
Invasive duct carcinoma
- ILC:
-
Invasive lobular carcinoma
- DCIS:
-
Duct carcinoma Insitu
- DBT:
-
Digital breast tomosynthesis
- CAD:
-
Computer aided detection
- USA:
-
United status of Amercia
- UK:
-
United Kingdom
- AUC:
-
Area under the curve
References
Heer E, Harper A, Escandor N et al (2020) Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Heal 8(8):e1027–e1037
Steinhof-Radwańska K, Lorek A, Holecki M et al (2021) Multifocality and multicentrality in breast cancer : comparison of the efficiency of mammography, contrast-enhanced spectral mammography, and magnetic resonance imaging in a group of patients with primarily operable breast cancer. Curr Oncol 28(5):4016–4030
Bi WL, Hosny A, Schabath MB et al (2019) Artificial intelligence in cancer imaging: clinical challenges and applications. CA Cancer J Clin 69(2):127–157
Lång K, Dustler M, Dahlblom V et al (2021) Identifying normal mammograms in a large screening population using artificial intelligence. Eur Radiol 31(3):1687–1692
Schaffter T, Buist DSM, Lee CI et al (2020) Evaluation of combined artificial intelligence and radiologist assessment to interpret screening mammogram. JAMA Netw Open 3(3):e200265
Franceschini G, Mason EJ, Orlandi A et al (2021) How will artificial intelligence impact breast cancer research efficiency? Expert Rev Anticancer Ther 21(10):1067–1070
Kim HE, Kim HH, Han BK et al (2020) Changes in cancer detection and false-positive recall in mammography using artificial intelligence: a retrospective, multireader study. Lancet Digit Health 2(3):e138–e148
Marinovich MK, Wylie E, Lotter W et al (2021) Artificial intelligence (AI) to enhance breast cancer screening: protocol for population-based cohort study of cancer detection”. BMJ Open 12(1):e054005
Ribli D, Horváth A, Unger Z et al (2018) Detecting and classifying lesions in mammograms with deep learning. Sci Rep 8(1):4165
Watanabe AT, Lim V, Vu HX et al (2019) Improved cancer detection using artificial intelligence: a retrospective evaluation of missed cancers on mammography. J Digit Imaging 32(4):625–637
Rodríguez-Ruiz A, Krupinski E, Mordang JJ et al (2019) Detection of breast cancer with mammography: effect of an artificial intelligence support system. Radiology 290(3):305–314
Pacilè S, Lopez J, Chone P et al (2020) Improving breast cancer detection accuracy of mammography with the concurrent use of an artificial intelligence tool. Radiol Artif Intell 2(6):e190208
Sasaki M, Tozaki M, Rodríguez-Ruiz A et al (2020) Artificial intelligence for breast cancer detection in mammography: experience of use of the ScreenPoint Medical Transpara system in 310 Japanese women. Breast Cancer 27(4):642–651
Conant EF, Toledano AY, Periaswamy S et al (2019) Improving accuracy and efficiency with concurrent use of artificial intelligence for digital breast tomosynthesis. Radiol Artif Intell 1(4):e180096
Pinto MC, Rodriguez-Ruiz A, Pedersen K et al (2021) Impact of artificial intelligence decision support using deep learning on breast cancer screening interpretation with single-view wide-angle digital breast tomosynthesis. Radiology 300(3):529–536
van Winkel SL, Rodríguez-Ruiz A, Appelman L et al (2021) Impact of artificial intelligence support on accuracy and reading time in breast tomosynthesis image interpretation: a multi-reader multi-case study. Eur. Radiol 31(11):8682–8691
Rodriguez-Ruiz A, Lång K, Gubern-Merida A et al (2019) Stand-alone artificial intelligence for breast cancer detection in mammography: comparison with 101 radiologists. J Natl Cancer Inst 111(9):916–922
Kim EK, Kim HE, Han K et al (2018) Applying data-driven imaging biomarker in mammography for breast cancer screening: preliminary study. Sci Rep 8(1):1–8
Weaver O, Yang W (2020) Imaging of breast cancers with predilection for nonmass pattern of growth: invasive lobular carcinoma and DCIS-does imaging capture it all? AJR Am J Roentgenol 215(6):1504–1511
Mansour S, Kamal R, Hashem L et al (2021) Can artificial intelligence replace ultrasound as a complementary tool to mammogram for the diagnosis of the breast cancer? Br J Radiol 94:20210820
Mansour S, Kamel R, Marey A et al (2022) Discrimination between phyllodes tumor and fibro-adenoma: Does artificial intelligence-aided mammograms have an impact? Egyptian Journal of Radiology and Nuclear Medicine 53(57):1–13
Funding
No source of funding.
Author information
Authors and Affiliations
Contributions
MS is the guarantor of integrity of the entire study. KR and MS contributed to the study concepts and design. MS, RM, SP, MA, AB, TS and AH contributed to the literature research. MS, RM, AH and AB contributed to the clinical studies. MS, AB, TS and AH, contributed to the experimental studies/data analysis. MS and AH contributed to the statistical analysis. MS, AB, and AH contributed to the manuscript preparation. MS, AB, and AH contributed to the manuscript editing. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of the Radiology Department of El Kasr ElAiny Hospital, Cairo University which is an academic governmental supported highly specialized multidisciplinary Hospital. A waiver of informed consent was obtained.
Committee’s reference number
Not applicable.
Consent for publication
All patients included in this research were legible, above 16 years of age. The study was waived to get written informed consent from the included patients.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the names have been updated.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Raafat, M., Mansour, S., Kamal, R. et al. Does artificial intelligence aid in the detection of different types of breast cancer?. Egypt J Radiol Nucl Med 53, 182 (2022). https://doi.org/10.1186/s43055-022-00868-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00868-z