
Abstract
Background
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) has always been a problem solver in troublesome breast lesions. Despite its many advantages, the encountered low specificity results in unnecessary biopsies. Diffusion-weighted MRI (DW-MRI) is a well-established technique that helps in characterizing breast lesions according to their water diffusivity. So this work aimed to assess the diagnostic performance of DW-MRI in troublesome breast lesions and see if it can replace DCE-MRI study.
Results
In our prospective study, we included 86 patients with mammography and/or ultrasound-detected 90 probably benign or probably malignant (BIRADS 3 or 4) breast lesions. Among the studied cases, 49/90 lesions were benign, and 41/90 were malignant. Combined analysis of morphological and kinetic findings in DCE-MRI had achieved the highest sensitivity of 95.1%. DW-MRI alone was less sensitive (73.2%) yet more specific (83.7%) than DCE-MRI (77.6%). Diagnostic accuracy of DCE-MRI was higher (85.6%) as compared to DW-MRI which was (78.9%).
Conclusion
DCE-MRI is the cornerstone in the workup of troublesome breast lesions. DW-MRI should not be used as supplementary tool unless contrast administration is contraindicated. Combining both DCE-MRI and DW-MRI is the ultimate technique for better lesion evaluation.
Similar content being viewed by others


Background
Breast cancer has been recently known as a heterogeneous group of diseases in regard to the biological makeup that is reflected on their treatment and clinical outcome [1]. Therefore, it has become clear that the traditional reliance on morphology alone does not suffice in the adequate classification of a disease that shows significant inter- and intratumoral differences [2].
Non-invasive functional magnetic resonance imaging (MRI) is used to obtain information about the microstructure as well as the biologic environment of a tumor. The concept of angiogenesis in the detection of tumor enhancement has long been employed in distinguishing malignant from benign tumors [3]. Dynamic contrast-enhanced MRI (DCE-MRI) is a dynamic investigation that allows tracking of enhancement in different types of tissues where malignant cells will usually show rapid uptake and washout while normal glandular tissue will demonstrate slow progressive kinetics [4].
However, despite its many advantages including high image quality and high sensitivity which surpasses that of mammography and ultrasound [5], it has been shown that a major disadvantage of MRI is its low specificity [6].
In the hope of adding further functional information about tumor cells that will aid in better differentiation between benign and malignant tumors, more techniques have been developed including diffusion-weighted imaging (DWI) and its derived measurement, including apparent diffusion coefficient (ADC), which has been under a lot of study [7].
Diffusion-weighted MRI (DW-MRI) is sensitive to characteristics often disrupted in malignant breast tissues, such as cell organization, density, extracellular space, and cell membrane permeability, which may help to better discriminate between different types of breast lesions [8].
There are currently two approaches to the utilization of breast MRI, and both aim for different objectives: one is the employment of various techniques to gain as much biological information about the tumor as possible, and the other aims at decreasing the complexity in both attaining and interpreting the images taking care not to compromise on the importance of functional imaging. Research has been undergoing between the former, the parametric MRI, and the latter, the abbreviated MRI [9].
So this work aimed to assess the diagnostic performance of DW-MRI in troublesome breast lesions and see if it can replace DCE-MRI study.
Methods
This study was a prospective analysis, approved by the ethics committee at our institute during the period from January 2018 to July 2020.
Patient population
This study included 86 patients with 90 probably benign or probably malignant (BIRADS 3 and 4) breast lesions detected on the initial mammography and/or breast ultrasound (US). They were referred from the multidisciplinary team for further lesion characterization by DCE-MRI and DW-MRI. The diagnostic indication for MRI in this study was better lesion characterization thus decreasing unnecessary biopsies and increasing cancer detection rate.
Those patients presented with either breast lump/s (n=45/86, 52.3%), inflammatory manifestations (red hot tender swollen breast) (n=6/86, 7%), or screening and post-mastectomy follow-up (n=35/86, 40.7%).
Patients included in our study were those with at least one of the following: (1) high-risk patients, (2) patients above the age of 40 with newly developed lesion, (3) patients with rapidly growing lesions, or (4) equivocal sonomammographic findings.
We excluded patients who have a contraindication to MRI (cardiac pacemaker, aneurismal clips, bone growth stimulators) and/or intravenous contrast (renal impairment, allergic patients, or those known to have a history of anaphylactic reaction from contrast media).
Magnetic resonance imaging acquisition
All patients were subjected to DCE-MRI and DW-MRI examination using Philips Achieva 1.5 T machine. They were imaged in prone position using a dedicated double breast coil.
DCE-MRI
Dynamic post-contrast acquisition was performed using six series of 3D THRIVE (T1 High Resolution Isotropic Volume Examination sequence) acquisition—1 before and 5 after power injection of 0.1 mmol/kg body weight of contrast (Gd-DTPA) with the parameters (TR/TE 2.8/9 ms) and slice thickness = 1.5 mm. Kinetic curves were done by placing a region of interest (ROI) at the area of maximum enhancement to measure the amount of contrast uptake, and dynamic curve patterns were prepared.
DW-MRI protocol
DW-MRI was done using single-shot echo-planar imaging, fat suppression, with repetition time/echo time of 5000 ms /77ms, 5-mm section thickness, 30× 30 cm field of view, 256× 256 matrix, 3-mm section gap, and 7:14 s acquisition time. b values were obtained at 0, 500, and 850 s/mm2. A ROI was drawn on the ADC map to calculate the ADC value (in case there was no signal change seen on ADC map, the ROI was placed over the area of concern on diffusion). Mean ADC for each lesion was calculated by averaging the ADC values from all the voxels enclosed by the ROI.
Image analysis
Image analysis and interpretation were done by two breast imaging consultants with 10 years or more of field experience who were blind to each other’s analysis, sonomammorgaphy findings, and final pathologic diagnosis. In case of disagreement, re-evaluation was done, and agreement was achieved in consensus.
DCE-MRI
We started assessing the images by looking for the presence or absence of any mass or non-mass enhancement. Then, the margins (in case of mass) or distribution (in case of non-mass), the intensity of enhancement, and internal enhancement pattern were noted. Classification of each lesion to benign or suspicious was then done based on the morphology and enhancement pattern.
Assessment of the kinetic curve was done; as when no enhancement or rising curve was noted, we considered the lesion benign while when there was a plateau or wash out curve the lesion was considered suspicious.
Finally, we determined the MRI BIRADS classification of each lesion based on the combination of both morphologic and kinetic criteria in reference to MRI BIRADS atlas 2013 [10].
DW-MRI
Qualitative (i.e., the signal pattern on high b value in DWI and ADC map) and quantitative (i.e., ADC value on the ADC map) assessment of diffusion-weighted MRI were done. In this study, the ADC cutoff value that was used to differentiate benign from malignant breast lesions was 1.3 × 10−3mm2/s as recommended by the European Society of Breast Imaging (EUSOBI) [11]. Lesions were considered restricted if they showed high signal intensity on high b value images with ADC value equal to or below 1.3 × 10−3mm2/s.
Each lesion was given a final classification of either benign or suspicious based on the worst or highest finding on DCE-MRI (morphology, kinetic curve, and combined) and DW-MRI individually. This classification was then compared to the pathology results (used as the gold standard) in 70 out of the 90 lesions (77.8%), and to ultrasound and routine follow-up in the remaining 20 typically benign lesions (22.2%) (adenosis, hamartoma, complicated cyst, and fibroadenomas). Histopathological analysis of the breast lesions was obtained either by core biopsy or surgery.
Correlation of ADC values with final pathology was assessed with the aim of getting a new cutoff value that may improve the sensitivity and specificity of DW-MRI. Then re-evaluation of the diagnostic indices of DW-MRI was done and recorded based on the new cutoff value proposed by our study.
Statistical analysis
Data were coded and entered using the statistical package SPSS (Statistical Package for the Social Sciences) version 26 (IBM Corp., Armonk, NY, USA). Data was summarized using mean, standard deviation, median, minimum, and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Mann-Whitney test [12]. For comparing categorical data, Chi-squared (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5 [13]. Standard diagnostic indices including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic efficacy were calculated as described by Galen [14]. ROC curve was constructed with area under curve analysis performed to detect best cutoff value of ADC for detection of malignancy. P value less than 0.05 was considered as statistically significant.
Results
The present prospective study included 86 patients with 90 detected probably benign or probably malignant (BIRADS 3 or 4) breast lesions on sonomammography or sonography only (according to the age) and underwent dynamic MRI with DWIs. Their age ranged between 25 and 70 years (mean age 42± 12.9). In relation to the final pathology, the age of patients with benign lesions was younger than that of those with malignant lesions, with mean age 39.57 ± 9.55 for benign and 48.56 ± 9.96 for malignant lesions (statistically significant p< 0.001).
Among our study population, 82/86 (95.3 %) had single lesions and 4/86 (4.7 %) had 2 lesions in the same or contralateral breast (multiple fibroadenomas and multiple invasive duct carcinoma (IDC)).
Among the studied cases and according to the histopathological results (n=70/90) or ultrasound findings and routine follow-up (n=20/90), 49/90 lesions were found to be benign while 41/90 lesions were found to be malignant. The different pathologies encountered in our study are illustrated in Table 1.
Mammographic and ultrasound findings
All patients (n=86/86) had previously reported either sonomammography (n=77/86, findings of both modalities were combined with the classification of each lesion according to the highest BI-RADS assignment) or sonography alone (n=9/86, young patients).
Out of all cases, 38/86 (44.2%) had non-dense breasts (ACR A and B on mammography and/or non-prominent parenchyma on US) while 48/56 (55.8%) had dense breasts (ACR C and D on mammography and/or prominent parenchyma on US).
In our study, we had 50/90 lesions (55.6%) BIRADS 3 and 40/90 (44.4 %) BIRADS 4; their relation to the final pathology is illustrated in Table 2.
All the false-negative lesions (11 cases) presented with dense breasts (either ACR C or D). The false-positive lesions included fat necrosis, granulomatous mastitis, and fibroadenomas with atypical features.
Contrast-enhanced MRI (CE-MRI) findings
Two out of the 90 lesions did not show enhancement: one fibroadenoma and one ductal carcinoma in situ (DCIS) but the remaining 88 lesions showed corresponding enhancement. The 90 lesions were given a classification of benign or suspicious based on combination of both morphologic criteria, and enhancement pattern and correlation with final pathology was done.
Five (false positive) cases were seen as suspicious non-mass enhancement yet the pathology yielded 2 adenosis, 1 fat necrosis, 1 atypical ductal hyperplasia, and 1 sclerosing adenosis (fibrocystic changes spectrum).
Three (false negative) cases were diagnosed as normal or benign; however, the pathology yielded malignancy: 1 DCIS (indeterminate calcifications on mammography with no lesions or enhancement on MRI), 1 mucinous neoplasm (well defined with homogeneous enhancement), and 1 intrapapillary neoplasm (well defined and homogeneous enhancement).
Kinetic curve findings
The kinetic curve analysis (dynamic behavior) of the detected breast lesions was done. A statistically significant correlation (p-value < 0.001) was found between the malignant curves (plateau and wash out types) and pathologically proven malignant lesions, and between the benign curves (rising curve) or no enhancement and benign lesions.
We had 4 false-negative lesions; 3 lesions showed rising curve (1 DCIS and 2 IDC), and 1 lesion showed no enhancement (DCIS).
Out of the false-positive cases, we had 2 lesions with wash out curves, and the pathology yielded benign nature (granulomatous mastitis and papilloma).
Combined DCE-MRI findings
Combined analysis of morphologic and kinetic findings was performed, and final BIRADS classification was given according to the most suspicious finding. The detailed relation of DCE-MRI (morphology, kinetic, and combined) to the pathology was shown in Table 3.
Accordingly, we had 11 false-positive cases; 9 lesions displayed borderline or malignant curve (plateau and wash out types) while the other 2 lesions (proved to be sclerosing adenosis and atypical ductal hyperplasia) were suspicious morphologically yet showing rising curve.
Thirty-nine cases were diagnosed as malignant (true positive); one of them showed benign morphology (diagnosed as mucinous neoplasm) yet with suspicious kinematic finding (wash out curve) (Fig. 1).

A 38-year-old female patient with positive family history presented with left breast lump. Mammography (A) showed left breast deeply seated dense mass lesion and ultrasound (B) showed left UIQ well-circumscribed hypoechoic complicated cystic lesion with posterior enhancement. Sonomammography revealed BIRADS 3. Dynamic MRI axial images showing upper inner quadrant rounded well-defined mass lesion displaying low T1 (C) and intermediate T2 signal intensity (D). MRI axial dynamic THRIVE sequence and subtraction image (E) showed left UIQ homogenously enhanced well-defined mass. Time/signal intensity analysis (F) of ROI showed wash out curve pattern (type III) with SI% of 103%. Diffusion sequence b 850 (G) and post-processing ADC map (H) showed restricted diffusion. ADC value for ROI was 0.9 × 10−3mm2/s. Both the DCE-MRI and DWI-MRI revealed BIRADS 4 and suspicious findings. Pathology revealed mucinous adenocarcinoma
DW-MRI findings
The detected 90 breast lesions were classified according to their criteria on DWI and the automatically generated ADC map to restricted and non-restricted. For proper interpretation, both qualitative and quantitative analyses were done. ADC values for the 90 breast lesions ranged from 0.3 to 2.2 ×10−3mm2/s (mean 1.3± 0.52). A statistically significant correlation was found between the malignant lesions and restricted pattern with p-value< 0.001. Correlation with the pathology is done and illustrated in Table 4.
In our study, we had 11 false-negative lesions (among which were cases with DCIS, IDC with central break down) and 8 false-positive lesions (all of them were fibroadenoma except 3: hematoma, abscess, and papilloma).
By applying a ROC curve of ADC value for the true-positive rate (sensitivity) plotted against false-positive rate (specificity) analysis with area under the curve=0.917, it was found that the best cutoff point is 1.365×10−3mm2/s to differentiate benign from malignant lesions according to the ADC value with a sensitivity of 90% and specificity of 75.5% (Fig. 2).

ROC curve of ADC value for the true-positive rate (sensitivity) was plotted against false-positive rate (specificity) analysis
The accuracy measures and diagnostic indices of sonomammography, DCE-MRI, and DW-MRI were calculated individually and showed that the sensitivity and accuracy of DCE-MRI were still found to be the highest among the imaging techniques to differentiate benign from malignant lesions. All the accuracy measure details are illustrated in Table 5.
Discussion
The BIRADS 3 and 4 categories are the gray zone of lesion characterization. The former can cause confusion to the interpreter as well as patient anxiety [15]. The current BIRADS lexicon offers significant statistical difference regarding the classification of BIRADS 4 lesion that ranges from greater than 2% to less than 95% malignant [16]. In practical terms, this means that there is a high percent chance that a biopsy can yield a benign result and in retrospect be deemed unnecessary [17].
Our study encompassed lesions that were classified into the BIRADS 3 and BIRADS 4 lesions and aimed to highlight the role of further MRI with emphasis on DW-MRI.
It was noted that most benign lesions we encountered tended to occur in the younger age group while the incidence of malignancy increased with age which is in accordance with what Alawi et al. stated [18]. We both also concluded that they comprise a wide range of pathology.
A respective sonomammographic sensitivity and specificity of 73% and 80% were achieved in our study which is much higher than the overall reported sensitivity of 30–60 and 40–80 stated by Mehnati et al. [5]. However, it is comparative with Eisa et al. who reported a sensitivity of 68 and specificity of 74% [19].
Mammography remains the mainstay for diagnosis of breast cancer; however, its sensitivity decreases with increasing breast density owing to the superimposition of glandular tissue [20]. This was the case in our study as the false negatives deduced in our study were seen in dense breasts categorized as ACR C and D. Complementary ultrasound can increase the mammographic sensitivity and thus the number of detected cancers [21].
Based on its ability to assess both morphological and enhancement patterns, MRI has been known to act as a problem solver [22]. We found that the morphological characteristic of a lesion is an important discriminator (sensitivity 92.7% and specificity 89.8%), and this was comparable to the results of Seifeldein et al. who achieved a sensitivity of 97.5% and a specificity of 85% [23]. According to and in agreement with Ebrahim et al., the spiculated margin seen in malignant lesions is a cornerstone when trying to evaluate a pathology [24]. In our study, we were faced with an incidentally discovered lesion in an older patient during her first screening sonomammogram that appeared rather well defined with the exception of mild lobulation to one of its borders. On MRI, the combined analysis of its margins and the lack of any enhancement allowed us to overcome the need of further biopsy. Further follow-up confirmed the stable benign nature of the lesion.
The low specificity was highlighted in our study when benign pathologies such as adenosis and fat necrosis demonstrated confusing non-mass enhancement. On the other hand, one of the malignant entities (DCIS) failed to enhance in our study.
Another fundament in the assessment of a lesion detected on MRI that is an important part of the multiparametric MRI approach is the dynamic contrast enhancement. In the current study, we were able to achieve a sensitivity of 90.2% and a specificity of 81.6%. Aribal et al. [25] reported a higher sensitivity of 97%, and Ebrahim et al. [24] were able to achieve a sensitivity of 100%. Our low specificity was in agreement with the above studies which showed a specificity of 88.9% and 76%, respectively. In our study, we allotted no enhancement or type one curve to benign lesions and jointly allotted both type two and three curves to malignant lesions.
Failure to correctly classify a lesion as benign was seen in two cases, papilloma and granulomatous mastitis with both lesions demonstrating a washout curve rather than more benign rising one. Several papers have similarly described papillomas as falsely malignant acquiring this benign characteristic with a range of 55–72.7% [26].
We also had three false-negative results that yielded benign rising curves rather than malignant washout curves when in fact their pathology was IDC (Fig. 3) and DCIS.

A 54-year-old female came for follow-up after mastectomy. Mammography (A) showed left breast cluster of microcalcification, and ultrasound (B) showed left 12 o’clock hypoechoic lesion with irregular outline. Sonomammography revealed BIRADS 4. MRI axial images showed left upper central ill-defined area with intermediate signal on T1 (C) and T2 (D). MRI axial dynamic THRIVE sequence and subtraction image (E) showed left upper central heterogeneously enhanced mass. Time/signal intensity analysis of ROI (F) showed rising curve pattern (type I) with SI% of 137%. Diffusion sequence b 850 (G) and post-processing ADC map (H) showed restricted diffusion. ADC value for ROI was 0.8 × 10−3 mm2/s. DCE-MRI revealed suspicious morphology and benign curve BIRADS 4 and DWI-MRI revealed suspicious findings BIRADS 4. Pathology revealed invasive duct carcinoma
By analyzing the morphological and kinetic features of lesions, together we attained a higher sensitivity and lower specificity of 95.1 and 77.6%. This increase in sensitivity when both parameters were combined was also reached by Ebrahim et al. who reported sensitivity of 100% [24].
More false-positive cases (11 cases) were noted on the final MRI assessment (combined) as we considered the most suspicious finding. Two cases (proved to be sclerosing adenosis and atypical ductal hyperplasia) with suspicious non-mass enhancement showed type 1 rising curve. On the other hand, two cases showed benign morphology yet washout curves, and for the remaining seven cases, plateau curves were attained with either benign or suspicious morphology. In those cases, a final BIRADS categorization of 4 was given necessitating the need for further biopsy.
On the other hand, the false-negative cases were just two where the morphology and kinetic analysis revealed benign features (DCIS, IDC triple negative).
The currently employed sequences in breast MRI including the pre- and post-contrast series when read in conjunction with the ACR MRI BIRADS lexicon allows for the high sensitivity but low specificity of breast MRI [27].
The addition of DWI to the protocol can add more information about the lesion enabling its better characterization as they both provide different data about the lesion with the former concerned with the lesion vascularity and the latter with water diffusivity. An added advantage of DWI is that we can overcome the worry of gadolinium-based contrast agent safety [28].
Reading DWI-MRI combines both qualitative approach as well as the quantitative interpretation that is based on the ADC values. The background signal suppression in high b value DWI allowed better lesion detection in one of our cases where a small satellite was better detected on DW-MRI compared to the DCE-MRI (Fig. 4).

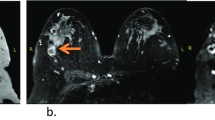
A 49-year-old female patient presented with left breast lump. Mammography (A) showed left upper central focal asymmetry with mild architectural distortion and linear clustered calcification. Ultrasound (B) showed left 12 o’clock irregular hypoechoic lesion. Sonomammography revealed BIRADS 4. MRI axial images showed left upper central microlobulated lesion of intermediate T1 (C) and T2 signal intensity (D). MRI axial dynamic THRIVE sequence and subtraction image (E) showed left upper central microlobulated heterogeneously enhancing mass with a small nearby (anterior) suspected ring enhancing nodule. Time/signal intensity analysis of ROI (F) showed plateau curve pattern (type II) with SI % of 270%. Diffusion sequence b 850 (G) and post-processing ADC map (H) showed restricted diffusion with more evident anterior restricted nodule. ADC value for ROI was 0.9 × 10−3mm2/s. DCE-MRI and DWI-MRI revealed BIRADS 5 and suspicious findings. Pathology revealed invasive ductal carcinoma
When categorizing our results into benign and malignant lesions, we relied on the EUSOBI recommendations which specified a cutoff value of 1.3 × 10−3mm2/s. Accordingly, we were able to achieve a sensitivity of 73%, and specificity of 83.7%. We understand that this specificity was lower when compared to El Bakry et al. [29] and Yadav et al. [30] who reached a respective specificity of 92.1% and 91.6%.
We can attribute this result to the fact that we had a significant number of false-positive benign lesions especially fibroadenomas which appeared restricted owing to their high cellularity (Fig. 5). These false-positive results have been acknowledged by Brandão et al. [31].

A 31-year-old female presented with right breast lump and pain. Mammography (A) showed two large retroareolar well-defined lesions of mixed densities predominantly hyperdense, and ultrasound (B) showed right retroareolar large well-defined mass of mixed echogenicity predominantly hypoechoic with posterior acoustic shadowing. Sonomammography revealed BIRADS 3. MRI axial images showed right large well-defined retroareolar mass showing heterogeneous signal on T1 (C) with elements of hyperintensity and intermediate signal on T2 WIs (D). MRI axial dynamic THRIVE sequence and subtraction image (E) showed right retroareolar well-defined mass with marginal contrast uptake. Time/signal intensity analysis (F) of ROI showed continuous rising curve pattern (type I) with SI % of 35%. Diffusion sequence b 850 (G) and post-processing ADC map (H) showed mixed signal intensity with foci of restricted diffusion in the right retroareolar mass. ADC value for ROI was 0.9 × 10−3mm2/s. DCE-MRI revealed BIRADS 2, but DWI-MRI gave suspicious findings BIRADS 4. Pathology revealed fibroadenoma
We also encountered false-negative results which were evident in DCIS, invasive ductal carcinomas associated with areas of breaking down, and as well as in small lesions. Durur-Subasi states that these scenarios can result in malignant lesions appearing facilitated rather than restricted [32]. Pinker et al. suggested that lesion less than 10–12mm was missed on blind reading [33].
On further retrospective analysis of our results, we found that using ADC value of 1.435 as a cutoff value gave a sensitivity of 100% (no cancers missed) yet a specificity of 75.5%. However, we believed that the ADC value of 1.365×10−3mm was considered the best cutoff point to differentiate benign from malignant lesions with resultant sensitivity (90.2%) and specificity (81.6%). Unfortunately, the different protocols among institutions and the variations in reported ADC values mean that there is no established cutoff value [32]. However, our results were close to the cutoff value suggested by the European Society of Breast Imaging [11].
A significant drawback to DW-MRI which we encountered is its inability to adequately assess the margins of a lesion. This is in accordance with what Chen et al. stated [34] in their study regarding the inferior spatial resolution and partial volume effect attributed to DW images.
A note of interest we came across in our study is a case of a mucinous carcinoma in a high-risk patient. It appeared well defined and acquired homogenous contrast on DCE-MRI. However, it demonstrated a wash out type 3 curve. On DWI-MRI it appeared to be restricted with a corresponding low ADC value. This contraindicates to Amornsiripanitch et al. who wrote that lesions with high water content including mucinous carcinoma display high ADC values [35]. Baltzer et al. [36] and Pinker et al. [33] also report that in up to 67% of the time they were not visible on DWI.
According to our results, the diagnostic performance of DCE-MRI was higher than DW-MRI and that means that it serves as a better option when trying to solve problematic lesions. In contrary, Daimiel et al. concluded that DWI was more specific (86.3% vs 65.7%, p < 0.001) but less sensitive (62.8% vs 90%, p < 0.001) and accurate (71% vs 80.7%, p = 0.003) compared to DCE-MRI for breast cancer detection [37].
One of our limitations was the sample size, which was considered small to calculate a standardized ADC cutoff value. Moreover, although we encountered a wide diversity of pathologies in our study, yet 34.4% of lesions were fibroadenomas which might have affected our final results.
The relatively high sensitivity but low specificity in our study has led us to believe that DW-MRI is a beneficial tool with limitations. Its role can be especially highlighted when there is concern regarding contrast safety or when cost and availability limit the use of enhanced MRI. There still remains work to be done regarding standardizing both a protocol and an ADC value.
Conclusion
Breast MRI has been highlighted as a problem-solving tool in lesions that prove to be a dilemma in other imaging modalities. When comparing the ability of DCE-MRI and DW-MRI in assessing BIRADS 3 and BIRADS 4 lesions with the ultimate aim of reducing unnecessary biopsies, we reached the conclusion that DW-MRI is best delegated to cases where indeed contrast administration is contraindicated. However, DCE-MRI is still the cornerstone of a breast MRI with multiparametric MRI combining both sequences being the ultimate technique.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- DCE-MRI:
-
Dynamic contrast-enhanced magnetic resonance imaging
- DWI:
-
Diffusion-weighted imaging
- ADC:
-
Apparent diffusion coefficient
- DW-MRI:
-
Diffusion-weighted magnetic resonance imaging
- BIRADS:
-
Breast Imaging Reporting and Data System
- US:
-
Ultrasound
- ROI:
-
Region of interest
- EUSOBI:
-
European Society of Breast Imaging
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- IDC:
-
Invasive ductal carcinoma
- TN:
-
True negative
- FN:
-
False negative
- TP:
-
True positive
- FP:
-
False positive
- CE-MRI:
-
Contrast-enhanced magnetic resonance imaging
- DCIS:
-
Ductal carcinoma in situ
References
Bertos NR, Park M (2011) Breast cancer—one term, many entities? J Clin Invest 121(10):3789–3796. https://doi.org/10.1172/JCI57100
Martelotto LG, Ng CK, Piscuoglio S et al (2014) Breast cancer intra-tumor heterogeneity. Breast Cancer Res 16(3):210. https://doi.org/10.1186/bcr3658
Kuhl C (2007) The current status of breast MR imaging. Part I. choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology. 244(2):356–378. https://doi.org/10.1148/radiol.2442051620
Kuhl CK (2009) Why do purely intraductal cancers enhance on breast MR images? Radiology. 253(2):281–283. https://doi.org/10.1148/radiol.2532091401
Mehnati P, Tirtash MJ (2015) Comparative efficacy of four imaging instruments for breast cancer screening. Asian Pac J Cancer Prev 16(15):6177–6186. https://doi.org/10.7314/APJCP.2015.16.15.6177
Quinn EM, Coveney AP, Redmond HP (2012) Use of magnetic resonance imaging in detection of breast cancer recurrence: a systematic review. Ann Surg Oncol 19(9):3035–3041. https://doi.org/10.1245/s10434-012-2341-3
et al (2011) Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumors. AJR Am J Roentgenol 196(1):210–217. https://doi.org/10.2214/AJR.10.4258Kul S, Cansu A, Alhan Eet al Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumors. AJR Am J Roentgenol 2011; 196:210-217, 1, DOI: https://doi.org/10.2214/AJR.10.4258.
Partridge SC, Richardson PW and Lorenzo JM. Discrimination of benign and malignant breast lesions by diffusion tensor MRI. American Society of clinical oncology, Breast Cancer Symposium Meeting. 2007; Session A, Abstract 72.
Rahim R, Michell MJ, Londero V et al (2017) Innovation in breast cancer radiology. In: Veronesi U, Goldhirsch A, Veronesi P et al (eds) Breast cancer, vol 18. Springer, Cham, pp 205–246. https://doi.org/10.1007/978-3-319-48848-6_18
Morris EA, Comstock CE, Lee CH, et al. ACR BI-RADS® magnetic resonance imaging. In: ACR BI-RADS® atlas, breast imaging reporting and data system. Reston, VA. American College of Radiology; 2013.
Baltzer P, Mann RM, Iima M et al (2020) Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI international breast diffusion-weighted imaging working group. Eur Radiol 30(3):1436–1450. https://doi.org/10.1007/s00330-019-06510-3
Chan YH (2003a) Biostatistics102: quantitative data – parametric & non-parametric tests. Singap Med J 44(8):391–396
Chan YH (2003b) Biostatistics 103: qualitative data –tests of independence. Singap Med J 44(10):498–503
Galen RS (1980) Predictive values and efficiency of laboratory testing. Pediat J Clin North Am 27(4):861–869. https://doi.org/10.1016/S0031-3955(16)33930-X
Lee K, Talati N, Oudsema R (2018) BI-RADS 3: current and future use of probably benign. Curr Radiol Rep 6(2):5. https://doi.org/10.1007/s40134-018-0266-8
D’Orsi CJ, Sickles EA, Mendelson EB, et al. ACR BI-RADS atlas, breast imaging reporting and data system. Reston, Va: American College of Radiology, 2013.
Liu G, Zhang MK, He Y, Liu Y, Li XR, Wang ZL (2019) BI-RADS 4 breast lesions: could multi-mode ultrasound be helpful for their diagnosis? Gland Surg 8(3):258–270. https://doi.org/10.21037/gs.2019.05.01
Alawi A, Hasan M, Harraz MM, Kamr WH, Alsolami S, Mowalwei H, Salem A, Qronfla H Breast lesions in women under 25 years: radiologic-pathologic correlation. Egypt J Radiol Nucl Med 2020; 51,96. https://doi.org/https://doi.org/10.1186/s43055-020-00209-y
Eisa HM, EAS G, Ibrahim AM et al (2018) Sonomammography versus MRI in evaluation of BI-RADS III breast lesion. Egypt J Hospital Med 72(2):3861–3866. https://doi.org/10.21608/EJHM.2018.9061
Wadhwa A, Sullivan JR, Gonyo MB (2016) Missed breast cancer: what can we learn? Curr Probl Diagn Radiol 45(6):402–419. https://doi.org/10.1067/j.cpradiol.2016.03.001
Okello J, Kisembo H, Bugeza S, Galukande M (2014) Breast cancer detection using sonography in women with mammographically dense breasts. BMC Med Imaging 14(1):41. https://doi.org/10.1186/s12880-014-0041-0
Pereira FP, Martins G, Figueiredo E (2009) Assessment of breast lesions with diffusion-weighted MRI: comparing the use of different b values. AJR Am J Roentgenol 193(4):1030–1035. https://doi.org/10.2214/AJR.09.2522
Seifeldein S, Elsaba T, Gabr A et al (2020) The diagnostic efficacy of tailored multiparametric breast MRI in indeterminate mammographic lesions: a single tertiary oncology center. Int J Cancer Biomed Res 4(3):217–228
Ebrahim YGS, Louis MR, Ali EA (2018) Multi-parametric dynamic contrast enhanced MRI, diffusion-weighted MRI and proton-MRS in differentiation of benign and malignant breast lesions: imaging interpretation and radiology-pathology correlation. Egypt J Radiol Nucl Med 49(4):1175–1181. https://doi.org/10.1016/j.ejrnm.2018.07.018
Aribal E, Asadov R, Ramazan A, Ugurlu MÜ, Kaya H (2016) Multiparametric breast MRI with 3T: effectivity of combination of contrast enhanced MRI, DWI and 1H single voxel spectroscopy in differentiation of breast tumors. Eur J Radiol 85(5):979–986. https://doi.org/10.1016/j.ejrad.2016.02.022
Kurz KD, Roy S, Saleh A, Diallo-Danebrock R, Skaane P (2011) MRI features of intraductal papilloma of the breast: sheep in wolf’s clothing? Acta Radiol 52(3):264–272. https://doi.org/10.1258/ar.2011.100434
Partridge SC, Amornsiripanitch N (2017) DWI in the assessment of breast lesions. Top MagnReson Imaging 26(5):201–209. https://doi.org/10.1097/RMR.0000000000000137
Dekkers IA, Roos R, Van der Molen AJ (2018) Gadolinium retention after administration of contrast agents based on linear chelators and the recommendations of the European medicines agency. Eur Radiol 28(4):1579–1584. https://doi.org/10.1007/s00330-017-5065-8
El Bakry MAH, Sultan AA, El-Tokhy NAE et al (2015) Role of diffusion weighted imaging and dynamic contrast enhanced magnetic resonance imaging in breast tumors. Egypt J Radiol Nucl Med 46(3):791–804. https://doi.org/10.1016/j.ejrnm.2015.04.008
Yadav P, Chauhan S (2018) Effectivity of combined diffusion-weighted imaging and contrast-enhanced MRI in malignant and benign breast lesions. Pol J Radiol 83:e82–e93. https://doi.org/10.5114/pjr.2018.74363
Brandão AC, Lehman CD, Partridge SC (2013) Breast magnetic resonance imaging: diffusion-weighted imaging. MagnReson Imaging Clin N Am 21(2):321–336. https://doi.org/10.1016/j.mric.2013.01.002
Durur-Subasi I (2019) DW-MRI of the breast: a pictorial review. Insights Imaging 10(1):61. https://doi.org/10.1186/s13244-019-0745-3
Pinker K, Moy L, Sutton EJ, Mann RM, Weber M, Thakur SB, Jochelson MS, Bago-Horvath Z, Morris EA, Baltzer PAT, Helbich TH (2018) Diffusion-weighted imaging with apparent diffusion coefficient mapping for breast cancer detection as a stand-alone parameter: comparison with dynamic contrast-enhanced and multiparametric magnetic resonance imaging. Investig Radiol 53(10):587–595. https://doi.org/10.1097/RLI.0000000000000465
Chen X, He XJ, Jin R, Guo YM, Zhao X, Kang HF, Mo LP, Wu Q (2012) Conspicuity of breast lesions at different b values on diffusion-weighted imaging. BMC Cancer 12(1):334. https://doi.org/10.1186/1471-2407-12-334
Amornsiripanitch N, Bickelhaupt S, Shin HJ et al (2019) Diffusion-weighted MRI for unenhanced breast cancer screening. Radiology 293(3):504–520. https://doi.org/10.1148/radiol.2019182789
Baltzer PAT, Bickel H, Spick C, Wengert G, Woitek R, Kapetas P, Clauser P, Helbich TH, Pinker K (2018) Potential of noncontrast magnetic resonance imaging with diffusion-weighted imaging in characterization of breast lesions: intraindividual comparison with dynamic contrast-enhanced magnetic resonance imaging. Investig Radiol 53(4):229–235. https://doi.org/10.1097/RLI.0000000000000433
Daimiel Naranjo I, Lo Gullo R, Saccarelli C, Thakur SB, Bitencourt A, Morris EA, Jochelson MS, Sevilimedu V, Martinez DF, Pinker-Domenig K (2021) Diagnostic value of diffusion-weighted imaging with synthetic b-values in breast tumors: comparison with dynamic contrast-enhanced and multiparametric MRI. Eur Radiol 31(1):356–367. https://doi.org/10.1007/s00330-020-07094-z
Acknowledgements
No acknowledgements.
Funding
No funding sources.
Author information
Authors and Affiliations
Contributions
AH wrote the manuscript. YT collected patient data. YT worked on image processing and collection of patient’s images. LH participated in the design of the study and performed the statistical analysis. SG and LH conceived the study and participated in its design and coordination and helped to draft the manuscript. YT and SF were responsible for revision of the draft from clinical point of view. AH collected the clinical and pathological data and statistics analysis. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of the “Faculty of medicine, Cairo University” with ethical committee approval number and date not available. An informed written consent was taken from all subjects.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hashem, L.M.B., Gareer, S.W.Y., Hashem, A.M.B. et al. Can DWI-MRI be an alternative to DCE-MRI in the diagnosis of troublesome breast lesions?. Egypt J Radiol Nucl Med 52, 138 (2021). https://doi.org/10.1186/s43055-021-00514-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00514-0