
Abstract
Background
Studying breast carcinoma is of great importance as it is the commonest female malignancy. Accurate preoperative assessment of disease characteristics and prognosis would be of great help in the diagnosis and treatment planning of breast cancer. The aim of this study was to evaluate the role of the apparent diffusion coefficient (ADC) value in detecting the grading of invasive breast carcinoma prior to management.
Results
There was a significant difference between the mean ADC value of tumors of grade I and III (p = 0.001) and between grade I and II (p = 0.002). However, there was no significant difference between grade II and III (p = 0.979). High ADC values were associated with low-grade tumors. The mean ADC value of 0.93 × 10–3 mm2/s showed sensitivity 98%, specificity 100%, PPV 100%, NPV 83.3%, accuracy 98.2%, AUC = 0.994, and 95% confidence interval of 0.978 to 1.000.
Conclusion
DWI is a contrast-free modality that allows for both morphological and quantitative analysis. ADC value may not be the proper modality to determine the prognosis of breast cancer due to overlap values, yet it could be a good discriminator between low- and high-grade tumors and hence predictor of breast cancer cells that would respond to chemotherapy.
Similar content being viewed by others


Background
Breast cancer is considered the second leading cause of cancer-related death and the highest number of newly recognized cases of cancer in women. Precise preoperative evaluation of disease characteristics and prognosis would be of enormous help in the management of breast cancer. Noninvasive diagnosis by means of in vivo imaging is turning to be of more significance for the diagnosis and treatment of breast cancer [1].
Dynamic contrast-enhanced breast MR imaging is now considered as the most precise imaging procedure for diagnosis of breast cancer; nevertheless, it gives no definitive information about tumor cellularity, which is well-known to be a vital indicator of tumor grade. Therefore, there has been a growing interest in the use of diffusion-weighted breast imaging for its potential to advance the diagnosis of breast lesions at the expense of a little increase in the examination time and with no need for intravenous contrast material injection [2].
Diffusion-weighted MRI detects the biologic characteristics of tissue and gives unique data regarding the cellularity and the status of molecular content of water. Moreover, it has a privilege of short exam duration with no need to use contrast medium [3].
The ADC is a q value that can be quantified measuring signal attenuation being influenced by microscopic motion, including molecular diffusion of water as well as blood microcirculation [4].
In the current study, we evaluated the impact of interpreting apparent diffusion coefficient (ADC) value as a prognostic factor that can predict the grading of invasive breast carcinoma before deciding the options of management.
Methods
This study was a prospective analysis, approved by the ethics committee at our institute during the period from December 2015 to December 2018. Tumor grading was established by mean of open surgical or a core needle biopsy (considered as the standard reference).
Patients
It included 156 patients that were referred from general surgery department and they were subjected to primary sonomammogram evaluation and MRI scanning including pre-contrast, dynamic post-contrast as well as diffusion-weighted sequences prior to biopsy.
Inclusion criteria
Patients proved to have invasive breast carcinoma that requires further advanced pathological analysis for grading.
Exclusion criteria
-
Cases that received neoadjuvant chemotherapy.
-
Cases that lacked pathological confirmation.
-
Cases proved to be benign.
-
Solid masses less than 1 cm or complex masses that presented with small solid component (The ADC value could not be evaluated).
MR imaging
MRI was performed for the breasts using 1.5 Tesla magnet scanners by two devices (Intera and Achieva, Philips medical system). All patients were examined in the prone position using a dedicated phased array breast coil with eight channels. Total study time ranged from 30 to 45 min. No sedation was used.
MRI imaging protocol
-
A-
Cases were examined first by pre-contrast sequences:
Axial T1 weighted images (TR/TE = 500/5.3 ms), sagittal and axial T2 weighted images (TR/TE = 120/4.9 ms), axial short time inversion recovery (STIR) (TR/TE = 80/6.5 ms). and a pre-contrast fat-saturated T2-weighted pulse sequence. Pre-contrast images are obtained over a 512 × 192 matrix in the axial plane with a slice thickness of 4 mm without gap, flip angle = 90° and FOV = 34–37 cm.
- B-
Diffusion-weighted images:
They were performed before the dynamic contrast-enhanced (DCE-MRI) acquisition using a “Echo-Planar Imaging” (EPI) sequence with following parameters: TR/TE = 5000/77 ms; slice thickness = 5 mm and 1 mm interslice gap; matrix = 124 × 100, b values (0, 850, 1000, 1500 s/mm2); and the diffusion image was supplied from “Spectral Adiabatic Inversion Recovery” (SPAIR) MR sequence. Respiratory triggering was used for better resolution.
- C-
Dynamic contrast-enhanced series:
A bolus of contrast (Magnevist (gadopentetate dimeglumine) 0.1 mmol/kg) was injected manually intravenous.
Post-processing and image analysis
Magnetic resonance images were reviewed by two radiologists (the first with 10 years of experience and the second with 6 years of experience) in the same setting and the final diagnosis was reached by their agreement (in consensus).
Post-processing image subtraction was obtained using the software subtraction function available on the work station.
Qualitative and quantitative analysis of the examined masses were done as follows:
- I-
Qualitative analysis:
Restricted diffusion was determined by visualization of abnormal bright signal intensity that became enhanced with increasing b values (0 → 850 → 1000 → 1500) at “diffusion-weighted” (DW) images. The ADC map presented intermediate/low signal intensity (SI) that corresponded to the abnormality (Figs. 1 and 2).
- II-
Quantitative analysis:

DWIs analysis. a DWI at b 1500 and b ADC map c ADC value: 0.82 × 10− 3 mm2/s. The right breast lower inner mass showed restricted diffusion of persistent bright SI on DWI and intermediate SI on ADC map with an estimated ADC value of 0.82 × 10− 3 mm2/s. Pathology and immunohistopathology revealed invasive duct carcinoma, grade II, positive for ER, PR and HER2 receptors

DWIs analysis. a DWI at b 1500, b ADC map, c ADC value of 0.99 × 10− 3 mm2/s. The left breast deep central mass showed restricted diffusion of persistent bright SI on DWI and intermediate SI on ADC map with an estimated ADC value of 0.99 × 10− 3 mm2/s. Pathology and immunohistopathology revealed invasive duct carcinoma, grade I, negative for ER, PR and HER2 receptors (TNBC)
The ADC values were measured manually by applying ROI at areas of bright SI on DW images and intermediate/low SI on ADC maps, aiming to cover as much as possible of the lesion, avoiding cystic/necrotic areas (Figs. 3 and 4).

DWIs analysis. a DWI at b 1500, b ADC map, c ADC value of 0.74 × 10–3 mm2/s. Right breast upper outer solid mass showed restricted diffusion of persistent bright SI on DWI and low SI on ADC map with an estimated ADC value of 0.74 × 10–3 mm2/s. Pathology and immunohistopathology revealed invasive duct carcinoma, grade III, positive for ER, PR and HER2 receptors

DWIs analysis. a DWI at b 1500, b ADC map, c ADC value of 0.65 × 10–3 mm2/s. Left breast axillary tail mass showed restricted diffusion of persistent bright SI on DWI and low SI on ADC map with an estimated ADC value of 0.65 × 10–3 mm2/s. Pathology and immunohistopathology revealed invasive duct carcinoma, grade III, negative for ER and HER2 and positive for PR receptors
Histological analysis
Nottingham combined histologic grade was used for assessment of histological grades of invasive ductal carcinoma, NOS using a numerical scoring system for tubule formation, pleomorphism and mitotic count. The total score could range from 3 to 9, with a total score of 3–5 representatives of grade 1, a total score of 6 or 7 representatives of grade 2, and a total score of 8 or 9 representatives of grade 3 (Table 1) [5].
Statistical analysis
Data were coded and entered using the statistical package SPSS (Statistical Package for the Social Sciences) version 23. Data were summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Kruskal-Wallis and Mann-Whitney tests [6]. ROC curve was constructed with area under curve analysis performed to detect the best cutoff value of ADC for the detection of high-grade tumors. P values less than 0.05 were considered statistically significant.
Results
One hundred fifty-six patients were included in this study, their age ranged from 26 to 67 years (mean age 47.62 ± 10.36).
All included carcinomas were invasive ductal carcinomas and their grading was 14 lesions (9%) were grade I, 108 lesions (69.2%) were grade II, and 34 (21.8%) lesions were grade III.
Analysis of the diffusion-weighted images and comparison of the mean ADC value with the pathological grade of the tumor was done.
All the included carcinomas (100%) showed persistent high signal on DWI with low to intermediate signal on ADC map (i.e., restricted diffusion).
ADC values ranged from 0.50 to 1.10 × 10− 3 mm2/s (mean 0.75 ± 0.14 × 10− 3 mm2/s).
The mean ADC value of grade I, grade II, and grade III were 1.01 ± 0.06 × 10− 3 mm2/s, 0.74 ± 0.12 × 10− 3 mm2/s, and 0.70 ± 0.09 × 10− 3 mm2/s, respectively.
There was a significant difference between the mean ADC value of tumors of grade I and III (p = 0.001) and between grade I and II (p = 0.002). However, there was no significant difference between grade II and III (p = 0.979).
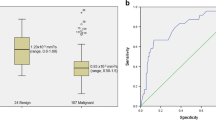
Moreover, ROC curve analysis of the data revealed that using the ADC value of 0.79 × 10–3 mm2/s as a cutoff value to differentiate between grade III from grades I and II yielded a sensitivity, specificity, PPV, NPV, and accuracy of 83.3%, 52.3%, 32.3%, 91.0%, and 58.9%, respectively, AUC = 0.647, and 95% confidence interval of 0.498 to 0.795. The use of mean ADC value of 0.93 × 10–3 mm2/s as a cutoff value to differentiate between grades II and III from grade I showed better statistical indices (sensitivity 98%, specificity 100%, PPV 100%, NPV 83.3%, and accuracy 98.2% AUC = 0.994, and 95% confidence interval of 0.978 to 1.000) and enhanced the performance of the ADC value in the assessment of the tumor cellularity of the induced breast carcinoma (Tables 2 and 3—Figs. 5 and 6).

ROC curve analysis to explore the discriminant ability of mean ADC value to differentiate (grade III) from (grades I and II) tumors

ROC curve analysis to explore the discriminant ability of mean ADC value to differentiate (grade II and III) from (grades I) tumors
Discussion
Breast carcinoma shows various molecular characteristics and differences in biological behavior, clinical progress, and prognosis [7].
Precise assessment of disease characteristics and prognosis preoperatively would be of extreme importance in the diagnosis and treatment planning of breast cancer [8].
The role of breast MRI has been greatly increasing and it is becoming rather mandatory for preoperative assessment of patients because of its accurate valuable information regarding the characteristics, extent, and number of breast lesions.
The rapid growth of cancer is coupled with a change of both anabolism and catabolism affecting its growth and changing the intracellular and extracellular environment. Functional MR imaging techniques—such as diffusion-weighted imaging (DWI) and the measured apparent diffusion coefficient (ADC)—are helpful to detect such changes coupled with tumor proliferation [9].
In this study, we found that the mean ADC value of the studied breast malignant masses was 0.75 ± 0.14 × 10− 3 mm2/s.
This was comparable to the mean ADC values reported by previous studies; Kato et al. [10] reported that the mean ADC value of 0.894 ± 0.204 × 10− 3 mm2/s, it was 0.85 ± 0.12 × 10− 3 mm2/s in Gouhar et al. [11] study, 0.91 ± 0.20 × 10− 3 mm2/s in Park et al. [12] study, 0.93 ± 0.27 × 10− 3 mm2/s in Ulghaffara et al. [13] study, and 0.91 ± 0.151× 10− 3 mm2/s in Matsubayashi et al. [14] study.
However, Belli et al. [7] and Costantini et al. [4] reported a slightly higher mean ADC value measuring 1.02 × 10− 3 mm2/s and 1.03 × 10− 3 mm2/s, respectively.
This is probably because both Belli et al. [7] and Costantini et al. [4] studies included ductal carcinoma in situ among their investigated cases, while our study specifically included only invasive carcinomas which were more likely to have lower ADC values than the non-invasive forms.
ADC values ranged from 0.50 to 1.10 × 10− 3 mm2/s in our study and so, it did not exceed the cutoff value between benign and malignant breast lesions set by previous studies, such as Sharma et al. [9] who estimated a cutoff ADC value of 1.23 × 10–3 mm2/s, and Tan et al. [15] who found that the cutoff ADC values for benign and malignant lesions were 1.21 × 10–3 mm2/s for b = 500 s/mm2 and 1.22 × 10–3 mm2/s for b = 1000 s/mm2, respectively.
The relation between the mean ADC value and the histological grade of the detected breast carcinoma was studied in the current work. We found that there was a significant inverse relation between them, meaning that tumors with higher grade showed lower ADC values when compared with those of lower grade (p = 0.001).
This was consistent with the previous researches done by of Belli et al. [7], Abdel Razek et al. [16], Costantini et al. [4], and Gouhar et al. [11] who had reached the same conclusion.
Our results agreed also with Sharma et al. [9], Guo et al. [17], Hatakenaka et al. [18], and Matsubayashi et al. [14] who reported a significant correlation between the ADC value and the tumor cellularity.
On the other side, Park et al. [12] and Tan et al. [15] stated that no significant correlation was found between ADC values and tumor grades.
Also, Yoshikawa et al. [19] research which included 27 breast cancer patients, 24 of which were invasive ductal carcinoma, found that the mean ADC of breast cancer did not significantly correlate with cancer cellularity.
In our study, the mean ADC value of grade I tumors was 1.01 ± 0.06 × 10− 3 mm2/s, of grade II was 0.74 ± 0.12 × 10− 3 mm2/s, and of grade III was 0.70 ± 0.09 × 10− 3 mm2/s.
This is comparable to the results obtained by Gouhar et al. [11] who reported that the mean ADC values of grade I, II, and III were 0.96 ± 0.12 × 10− 3 mm2/s, 0.87 ± 0.07 × 10− 3 mm2/s, and 0.75 ± 0.12 × 10− 3 mm2/s, respectively.
However, it differs from the results obtained by Costantini et al. [4] who reported that the mean ADC values for grade I, II, and III tumors were 1.25 × 10− 3 mm2/s, 1.02 × 10− 3 mm2/s, and 0.92 × 10− 3 mm2/s, respectively.
This variation may be attributed to the discrepancy in the sample size and the MRI technique specially the use of different b values.
We found a significant difference between the mean ADC value of tumors of grade I and III (p = 0.001) and between grade I and II (p = 0.002). However, there was no significant difference between grades II and III (p = 0.979).
This was different from the results of Gouhar et al. [11], who reported that there was a significant difference in the mean ADC value of tumors of grade II and III (p = 0.003), and no significant difference between grade I and II (p = 0.054), we think the difference was due to the difference in the b values used as Gouhar et al. used only two b values (0 and 1000).
Analysis of our data revealed that using the ADC value 0.79 × 10− 3 mm2/s as a cutoff value between grade III and grades I and II has a sensitivity, specificity, PPV, NPV, and accuracy of 83.3%, 52.3%, 32.3%, 91.0%, and 58.9%, respectively. On the other hand, using the ADC value of 0.93 × 10− 3 mm2/s as a cutoff value between grade I and grades II and III has a sensitivity, specificity, PPV, NPV, and accuracy of 98%, 100%, 100%, 83.3%, and 98.2%, respectively.
Yet, we have to admit that our study was limited by the uneven distribution of the different histological grades which is due to the limited number of grade I and grade III tumors included.
Conclusion
ADC value could be a good discriminator between low- and high-grade tumors and hence predictor of breast cancer cells that would respond to chemotherapy.
Availability of data and materials
All the datasets used and analyzed during this study are available with the corresponding author on reasonable request.
Abbreviations
- ADC:
-
Apparent diffusion coefficient
- AUC:
-
Area under curve
- DWI:
-
Diffusion-weighted images
- MRI:
-
Magnetic resonance imaging
- NOS:
-
Invasive duct carcinoma not otherwise specified
- NPV:
-
Negative predictive value
- PPV:
-
Positive predictive value
References
Almubarak M, Osman S, Marano G, Abraham J (2009) Role of positron-emission tomography scan in the diagnosis and management of breast cancer. Oncology 23:255–261
Woodhams R, Ramadan S, Stanwell P, Sakamoto S, Hata H, Ozaki M et al (2011) Diffusion-weighted imaging of the breast: principles and clinical applications. Radiographics 31(4):1059–1084
Baltzer PA, Benndorf M, Dietzel M, Gajda M, Camara O, Kaiser WA (2010) Sensitivity and specificity of unenhanced MR mammography (DWI combined with T2-weighted TSE imaging, ueMRM) for the differentiation of mass lesions. Eur Radiol 20(5):1101–1110
Costantini M, Belli P, Rinaldi P, Bufi E, Giardina G, Franceschini G et al (2010) Diffusion-weighted imaging in breast cancer: relationship between apparent diffusion coefficient and tumour aggressiveness. Clin Radiol 65(12):1005–1012
Zbytek B, Cohen C, Wang J, Page A, Williams DJ, Adams AL (2013) Nottingham-defined mitotic score: comparison with visual and image cytometric phosphohistone H3 labeling indices and correlation with Oncotype dx recurrence score. Appl Immunohistochem Mol Morphol 21:48–53
Chan YH (2003) Biostatistics102: quantitative data—parametric & non-parametric tests. Singap Med J 44(8):391–396
Belli P, Costantini M, Bufi E, Giardina GG, Rinaldi P, Franceschini G et al (2015) Diffusion magnetic resonance imaging in breast cancer characterisation: correlations between the apparent diffusion coefficient and major prognostic factors. La Radiologia Medica 120(3):268–276
Baba S, Isoda T, Maruoka Y, Kitamura Y, Sasaki M, Yoshida T et al (2014) Diagnostic and prognostic value of pretreatment SUV in 18F-FDG/PET in breast cancer: comparison with apparent diffusion coefficient from diffusion-weighted MR imaging. J Nucl Med 55(5):736–742
Sharma U, Sah RG, Agarwal K, et al (2016) Potential of Diffusion-Weighted Imaging in the Characterization of Malignant, Benign, and Healthy Breast Tissues and Molecular Subtypes of Breast Cancer. Front Oncol 6:126. https://doi.org/10.3389/fonc.2016.00126
Kato F, Kudo K, Yamashita H, Wang J, Hosoda M, Hatanaka KC et al (2016) Differences in morphological features and minimum apparent diffusion coefficient values among breast cancer subtypes using 3-tesla MRI. Eur J Radiol 85(1):96–102
Gouhar GK, El-Hariri MA, Lotfy WE (2011) Malignant breast tumours: correlation of apparent diffusion coefficient values using diffusion-weighted images and dynamic contrast enhancement ratio with histologic grading. Egypt J Radiol Nucl Med 42:451–460
Park EK, Cho KR, Seo BK, Woo OH, Cho SB, Bae JW (2016) Additional Value of Diffusion-Weighted Imaging to Evaluate Prognostic Factors of Breast Cancer: Correlation with the Apparent Diffusion Coefficient. Iran J Radiol 13(1):e33133. https://doi.org/10.5812/iranjradiol.33133.
Ulghaffara WA, Magdy M (2013) Role of diffusion-weighted imaging in assessment of breast lesions.Med. J. Cairo Univ 81(2):87–93.
Matsubayashi RN, Fujii T, Yasumori K, Muranaka T, Momosaki S (2010) Apparent diffusion coefficient in invasive ductal breast carcinoma: correlation with detailed histologic features and the enhancement ratio on dynamic contrast-enhanced MR images. J Oncol. 2010;ID821048:6.
Tan SL, Rahmat K, Rozalli FI, Mohd-Shah MN, Aziz YF, Yip CH et al (2014) Differentiation between benign and malignant breast lesions using quanti-tative diffusion-weighted sequence on 3 T MRI. Clin Radiol 69:63–71. https://doi.org/10.1016/j.crad.2013.08.007
Abdel Razek AA, Gaballa G, Denewer A, Nada A (2010) Invasive ductal carcinoma: correlation of apparent diffusion coefficient value with pathological prognostic factors. NMR Biomed 23:619–623
Guo Y, Cai YQ, Gao YG, An NY, Ma L, Gao JH et al (2002) Differentiation of clinically benign and malignant breast lesions using diffusion weighted imaging. J Magn Reson Imaging 16:172–178
Hatakenaka M, Soeda H, Yabuuchi H, Matsuo Y, Kamitani T, Oda Y et al (2008) Apparent diffusion coefficients of breast tumors: clinical application. Magn Reson Med Sci 7(1):23–29
Yoshikawa MI, Ohsumi S, Sugata S, Kataoka M, Takashima S, Mochizuki T et al (2008) Relation between cancer cellularity and apparent diffusion coefficient values using diffusion-weighted magnetic resonance imaging in breast cancer. Radiat Med 26:222–226
Acknowledgements
Not applicable.
Funding
Not applicable (no funding received for this study).
Author information
Authors and Affiliations
Contributions
All authors have read and approved the manuscript. HA, SM, NS, and HE contributed equally to this work. HA and SM designed research. HA and NS performed research. HE and SM analyzed data. HA and HE wrote the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the research ethics committee of the Radiology Department of the Faculty of Medicine Cairo University on 3/5/2015, Reference number of approval: 580–2015.
All patients included in this study gave a written informed consent to participate in the research. If the patient was less than 16 years old, or unconscious at the time of the study, written informed consent was given by their parent or legal guardian.
Consent for publication
All patients included in this study gave a written informed consent to publish the data contained in this study. If the patient was less than 16 years old, or unconscious at the time of the study, written informed consent was given by their parent or legal guardian.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Azzam, H., Mansour, S., Salem, N. et al. Correlative study between ADC value and grading of invasive breast cancer. Egypt J Radiol Nucl Med 51, 12 (2020). https://doi.org/10.1186/s43055-019-0124-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-019-0124-6