
Abstract
Background
There are preliminary studies about the association between COVID-19 and ABO phenotypes and the results are controversial. There are only two studies which investigated the association of Rh blood groups in addition to ABO with COVID-19; however, in the statistical analysis ABO and Rh blood groups have been considered separately. Therefore, the present case-control study was performed to determine the association of COVID-19 with ABO blood groups considering the Rh blood groups simultaneously. The study was conducted in Kunduz COVID-19 treatment specific center, Spin-Zar Hospital (Kunduz Province, North East Afghanistan). A total of 301 confirmed COVID-19 cases and 1039 healthy blood donors as control group were included in the study.
Results
The Rh− phenotype strongly increased the risk of COVID-19 (OR = 2.97, 95% CI 1.86–3.89, P < 0.001). Although blood group A increased the risk of developing COVID-19, the association did not reach statistical significance. In analysis of the combination phenotypes, the A− blood group remarkably increased the risk of COVID-19 (OR = 7.24, 95% CI 3.62–14.4, P < 0.001). Multivariate analysis revealed that the interaction of Rh and ABO is significant (P < 0.013).
Conclusion
These findings indicate that susceptibility to COVID-19 is strongly associated with A− blood group.
Similar content being viewed by others


Background
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing coronavirus disease-2019 (COVID-19), is distributed to almost all countries in the world and until now (1 October 2020), more than 32,469,000 confirmed cases with 1,027,000 death have been reported from all around the world. On 24 February 2020, the first COVID-19 case was reported in Afghanistan in Herat Province and in a short time, it spread throughout the country [1]. As of 1 October 2020, there have been 39,285 COVID-19 cases with 1458 deaths in Afghanistan.
Susceptibility to COVID-19 is a multifactorial trait like other infectious disease. Several genetic elements and environmental factors are involved in its etiology. It should be noted that host and viral genetic variations might be involved in the pathogenesis of the disease [2,3,4]. There are several ecologic and case-control studies investigated the association between common genetic polymorphisms and susceptibility to COVID-19, as well as its mortality [5,6,7,8,9,10,11,12,13].
The association of genetic polymorphism in blood groups with susceptibility to some infectious diseases has been well established [14]. Very recently, it has been reported that the prevalence and mortality of COVID-19 is associated with ABO (MIM: 616093) and Rh (MIM: 111680) blood groups, based on an ecologic study. Countries with higher A phenotype and Rh negative blood group showed higher values of the prevalence and mortality rate [5]. However, studies on the association between COVID-19 and ABO phenotypes are at preliminary stage and the results are controversial [15,16,17,18,19,20,21,22,23,24,25,26,27,28].
There are three studies which investigated the association of Rh blood groups in addition to ABO with COVID-19; however, in the statistical analysis, ABO and Rh have been considered separately [15, 23, 25]. Therefore, the present case-control study was performed to determine the association of COVID-19 with ABO blood groups considering the Rh blood groups simultaneously.
Methods
Participants
This case-control study was accomplished during August and September 2020 in Kunduz COVID-19 treatment specific center, Spin-Zar Hospital supported by Ministry of Public Health of Afghanistan and JACK organization (Kunduz Province, North East Afghanistan). Afghanistan has a heterogeneous population [29,30,31,32]; therefore, we selected the participants (patients and controls) from Muslims living in Kunduz City.
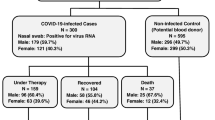
A total of 301 confirmed cases of COVID-19 patients were included in the study. From these 136, 127, and 38 individuals were Pashtuns, Tajiks, and Uzbeks, respectively. A control sample of 1039 healthy blood donors was also included in the study. From these 486, 424, and 126 individuals were Pashtuns, Tajiks, and Uzbeks, respectively. In order to increase the statistical power of the analysis, the data were pooled.
The present study was performed in accordance with the ethical codes of the Declaration of Helsinki and was approved by the ethics committee of our university. The information for case group was obtained by a questionnaire. Oral informed consent was obtained from each participant before the study.
Measurements
Infection by Covid-19 was confirmed using real-time polymerase chain reaction (RT-PCR) test in the Kunduz COVID-19 treatment specific center, Spin-Zar Hospital. The sample test procedure is as follows setups. At first, nasopharyngeal swabs were collected by Citoswab collection and transport kit (Citotest Labware Manufacturing Co., Ltd.). Total RNA was extracted from nasopharyngeal samples by QIAamp Viral RNA Mini Kit (Cat No. 52906 QIAGEN) according to the manufacturer’s instructions. RNA samples were used for RT-PCR by detection Kit DA0931, for 2019 Novel Coronavirus (2019-nCoV) RNA (PCR-Fluorescence Probing) Da An Gene Co., Ltd. of Sun Yat-sen University of China, using an Applied Biosystems 7500 Real Time PCR System. The reaction mixture was subjected to initial denaturation at 95 °C for 15 min, followed by 45 cycles of 95 °C for 15 s, 55 °C for 45 s, and 72 °C for 40 s set. The case samples compared with the positive and negative CT curve according to the manufacturer’s instructions.
Blood samples were collected without anti-coagulant by finger prick with sterile lancet and the ABO and Rh blood group were determined based on standard method of antigen-antibody agglutination test using anti-sera (anti-A, anti-B, and anti-D) kit (CinnaClone II Ltd., Iran).
Statistical analysis
For the control group, the observed frequencies of the ABO phenotypes were assessed for Hardy-Weinberg equilibrium (HWE) using the χ2 statistic [33].
Our approach for analysis of the data consisted of three steps. At first, the frequencies of blood group O (for ABO blood groups) and Rh+ (for Rh blood groups) compared separately between cases and controls, using logistic regression analysis. In the logistic model, the blood group O (for ABO blood groups) and Rh+ (for Rh blood groups) were considered as reference categories and odds ratios (ORs) and their 95% confidence intervals (95% CI) of COVID-19 risk were estimated. The genes encoding the ABO and Rh blood groups are located on human chromosomes 1 and 9, respectively [34, 35]. It means that they are independent loci. In the second step, combination phenotypes of ABO and Rh blood groups compared between cases and controls. In the analysis, O+ phenotype was used as reference group. Finally, multivariable logistic regression analysis was used to investigate the interaction of ABO and Rh phenotypes at the third step. Statistical analysis was performed using the SPSS software (SPSS Inc., Chicago, IL, USA; version 11.5). A P value less than 0.05 was considered as statistically significant.
Sample size which is required for identification a significant difference in phenotypic frequency analysis for an effect size of 0.15 (small-medium effect) with assumptions of α = 0.05, β = 0.20, Lambda = 14.88, and df = 3 were calculated using the GPOWER (www.psycho.uni-duesseldorf.de/aap/projects/gpower) software (version 3.1.3). A minimum sample of 630 would be sufficient. The present case-control study is more than sufficiently powered with an n = 1337 to detect a small-medium effect for comparing the frequency of blood groups between the two groups.
Results
There was no significant difference between COVID-19 cases and healthy controls for ethnicity of the participants (χ2 = 0.28, df = 2, P = 0.869). Therefore, the ethnic groups were pooled. Table 1 shows the frequency distribution of ABO and Rh blood groups in COVID-19 patients and control group. The allelic frequencies of A, B, and O in control group were 0.2233, 0.1707, and 0.6060, respectively. The expected values of the ABO phenotypes based on HWE showed high similarity with the observed frequencies (χ2 = 0.67, df = 1, P = 0.411). The Rh− blood group compared to the Rh+ phenotype strongly increased the risk of COVID-19 (OR = 2.97, 95% CI 1.86–3.89, P < 0.001). Although the A phenotype and the A + AB blood groups versus to the O phenotype increased the risk of COVID-19, the association did not reach statistical significance (Table 1).
In further analysis, the associations between combination of the ABO and Rh phenotypes and susceptibility to COVID-19 were investigated. The results were summarized in Table 2. The A− vs O+ blood group remarkably increased the risk of COVID-19 (OR = 7.24, 95% CI 3.62–14.4, P < 0.001). The O− vs O+ phenotype significantly associated with the risk of COVID-19, which is quite similar with the association between Rh− and susceptibility to COVID-19 (Tables 1 and 2). It seems that Rh and ABO blood groups may have interaction with each other. To investigate this point, multivariable logistic regression analysis was done, using ABO and Rh phenotypes as independent variables. Analysis revealed a significant interaction of Rh and ABO blood groups (P < 0.024). The same results were obtained after adjustment for ethnicity and gender of the participants (Tables 1 and 2).
Discussion
There are several studies reporting the relationship of ABO and Rh blood groups with susceptibility to COVID-19 or with outcome of the COVID-19 [15,16,17,18,19,20,21,22,23,24,25,26,27,28]. The results are inconsistent. However, it seems that the risk of COVID-19 is positively associated with A blood group compared with O phenotype [17, 18, 24, 26, 28]. Our present finding, confirmed the relationship of ABO genetic system with susceptibility to COVID-19. Very recently, a genome-wide scan study indicated that human chromosome segment 9q34.2 is associated with severe form of COVID-19 with respiratory failure [36]. It should be mentioned that the ABO locus is located on the 9q34.2 [34]. Taken together, these findings indicate that this locus might be involved in the etiology of the disease.
The novelty of the present study is the strong positive association between Rh− blood group and the risk of developing COVID-19. This finding is consistent with the result of a recently published ecologic study. Based on data, from 86 countries, the authors reported that frequency of the Rh− blood group is positively associated with the prevalence, mortality, and case-fatality of COVID-19. It means that prevalence of COVID-19 is higher in countries where the Rh− blood group is more frequent [5].
COVID-19 is an infectious and communicable disease. Therefore, several factors are involved in the pathogenesis of the disease. In order to confirm the role of the Rh blood groups on susceptibility to COVID-19, replication of this study in other countries is recommended with respect to these factors.
Conclusions
The present case-control study indicated that there is a strong positive association between Rh- blood group and the risk of COVID-19. Also, the present study revealed that among the combination phenotypes, the A− blood group is significantly associated with the susceptibility to COVID-19.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information file.
Abbreviations
- CI:
-
Confidence interval
- COVID-19:
-
Coronavirus disease-2019
- HWE:
-
Hardy-Weinberg equilibrium
- OR:
-
Odds ratio
- PCR:
-
Polymerase chain reaction
- SARS-CoV-2:
-
Severe Acute Respiratory Syndrome Coronavirus 2
References
Mousavi SH, Abdi M, Zahid SU, Wardak K (2020) Coronavirus disease 2019 (COVID-19) outbreak in Afghanistan: Measures and challenges. Infect Control Hosp Epidemiol. https://doi.org/10.1017/ice.2020.240
Brest P, Refae S, Mograbi B, Hofman P, Milano G (2020) Host polymorphisms may impact SARS-CoV-2 infectivity. Trends Genet 36:813–815
Di Maria E, Latini A, Borgiani P, Novelli G (2020) Genetic variants of the human host influencing the coronavirus-associated phenotypes (SARS, MERS and COVID-19): rapid systematic review and field synopsis. Hum Genomics 14:30
Saini S, Saini A, Thakur CJ, Kumar V, Gupta RD, Sharma JK (2020) Genome-wide computational prediction of miRNAs in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) revealed target genes involved in pulmonary vasculature and antiviral innate immunity. Mol Biol Res Commun 9:83–91
Ansari-Lari M, Saadat M (2020) The morbidity and mortality of COVID-19 are associated with ABO and Rh blood groups. Eur J Prev Cardiol:2047487320939216. https://doi.org/10.1177/2047487320939216
Dai X (2020) ABO blood group predisposes to COVID-19 severity and cardiovascular diseases. Eur J Prev Cardiol 27:1436–1437
Dai X (2020) C3 polymorphisms represent an important immunological confounder on the spread and outcome of COVID-19. Eur J Prev Cardiol 27:1333–1334
Delanghe JR, De Buyzere ML, Speeckaert MM (2020) C3 and ACE1 polymorphisms are more important confounders in the spread and outcome of COVID-19 in comparison with ABO polymorphism. Eur J Prev Cardiol 27:1331–1332
Delanghe JR, Speeckaert MM, De Buyzere ML (2020) COVID-19 infections are also affected by human ACE1 D/I polymorphism. Clin Chem Lab Med 58:1125–1126
Kuo CL, Pilling LC, Atkins JL, Masoli JAH, Delgado J, Kuchel GA, Melzer D (2020) APOE e4 genotype predicts severe COVID-19 in the UK Biobank community cohort. J Gerontol A Biol Sci Med Sci:glaa131. https://doi.org/10.1093/gerona/glaa131
Saadat M (2020) An evidence for correlation between the glutathione S-transferase T1 (GSTT1) polymorphism and outcome of COVID-19. Clin Chim Acta 508:213–216
Saadat M (2020) No significant correlation between ACE Ins/Del genetic polymorphism and COVID-19 infection. Clin Chem Lab Med 58:1127–1128
Saadat M (2020) The morbidity and mortality of COVID-19 are correlated with the Ile105Val glutathione S-transferase P1 polymorphism. Egypt J Med Hum Genet 21:52. https://doi.org/10.1186/s43042-020-00094-0
Cooling L (2015) Blood groups in infection and host susceptibility. Clin Microbiol Rev 28:801–870
Abdollahi A, Mahmoudi-Aliabadi M, Mehrtash V, Jafarzadeh B, Salehi M (2020) The novel Coronavirus SARS-CoV-2 vulnerability association with ABO/Rh blood types. Iran J Pathol 15:156–160
Ad’hiah AH, Allami RH, Mohsin RH, Abdollah MH, Al-Saady AJR, Alsudani MY (2020) Evaluating of the association between ABO blood groups and coronavirus disease 2019 (COVID-19) in Iraqi patients. Egyp J Med Hum Genet 21:50
Fan Q, Zhang W, Li B, Li DJ, Zhang J, Zhao F (2020) Association between ABO blood group system and COVID-19 susceptibility in Wuhan. Front Cell Infect Microbiol 10:404
Pourali F, Afshari M, Alizadeh-Navaei R, Javidnia J, Moosazadeh M, Hessami A (2020) Relationship between blood group and risk of infection and death in COVID-19: a live meta-analysis. New Microbes New Infect 37:100743
Wu Y, Feng Z, Li P, Yu Q (2020) Relationship between ABO blood group distribution and clinical characteristics in patients with COVID-19. Clin Chim Acta 509:220–223
Zalba Marcos S, Antelo ML, Galbete A, Etayo M, Ongay E, García-Erce JA (2020) Infection and thrombosis associated with COVID-19: possible role of the ABO blood group. Med Clin (Barc) 155:340–343
Zhao J, Yang Y, Huang H-P et al (2020) Relationship between the ABO blood group and the COVID-19 susceptibility. medRxiv. https://doi.org/10.1101/2020.03.11.20031096.03.11.20031096
Zietz M, Tatonetti NP (2020) Testing the association between blood type and COVID-19 infection, intubation, and death. medRxiv. https://doi.org/10.1101/2020.04.08.20058073
Taha SAH, Osman MEM, Abdoelkarim EAA, Holie MAI, Elbasheir MM, Abuzeid NMK, Al-Thobaiti SA, Fadul SB, Konozy EHE (2020) Individuals with a Rh-positive but not Rh-negative blood group are more vulnerable to SARS-CoV-2 infection: demographics and trend study on COVID-19 cases in Sudan. New Microbes New Infect 38:100763
Chegni H, Pakravan N, Saadati M, Ghaffari AD, Shirzad H, Hassan ZM (2020) Is there a link between COVID-19 mortality with genus, age, ABO blood group type, and ACE2 gene polymorphism? Iran J Public Health 49:1582–1584
Boudin L, Janvier F, Bylicki O, Dutasta F (2020) ABO blood groups are not associated with risk of acquiring the SARS-CoV-2 infection in young adults. Haematologica:haematol.2020.265066. https://doi.org/10.3324/haematol.2020.265066
Li J, Wang X, Chen J, Cai Y, Deng A, Yang M (2020) Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br J Haematol 190:24–27
Zaidi FZ, Zaidi ARZ, Abdullah SM, Zaidi SZA (2020) COVID-19 and the ABO blood group connection. Transfus Apher Sci 102838. https://doi.org/10.1016/j.transci.2020.102838
Gérard C, Maggipinto G, Minon JM (2020) COVID-19 and ABO blood group: another viewpoint. Br J Haematol 190:e93–e94
Saify K, Saadat M (2012) Consanguineous marriages in Afghanistan. J Biosoc Sci 44:73–81
Saify K, Saadat I, Saadat M (2012) Genetic polymorphisms of glutathione S-transferase T1 (GSTT1) and M1 (GSTM1) in selected populations of Afghanistan. Mol Biol Rep 39:7855–7859
Saify K, Saadat I, Saadat M (2013) First survey of the two polymorphisms (Arg194Trp and Arg399Gln) in XRCC1 gene in four Afghanistan populations and comparison with worldwide data. Mol Biol Rep 40:5281–5284
Saadat M, Tajbakhsh K (2013) Prevalence of consanguineous marriages in west and south of Afghanistan. J Biosoc Sci 45:799–805
Saadat M (2016) Estimation of allelic frequencies for ABO and Rh blood groups. Egypt J Med Hum Genet 16:205–206
Ferguson-Smith MA, Aitken DA, Turleau C, de Grouchy J (1976) Localisation of the human ABO: Np-1: AK-1 linkage group by regional assignment of AK-1 to 9q34. Hum Genet 34:35–43
Chérif-Zahar B, Mattéi MG, Le Van Kim C, Bailly P, Cartron JP, Colin Y (1991) Localization of the human Rh blood group gene structure to chromosome region 1p34.3-1p36.1 by in situ hybridization. Hum Genet 86:398–400
Ellinghaus D, Degenhardt F, Bujanda L, Buti M, Albillos A, Invernizzi P, Fernández J, Prati D, Baselli G, Asselta R et al (2020) Genomewide association study of severe Covid-19 with respiratory failure. N Engl J Med:NEJMoa2020283. https://doi.org/10.1056/NEJMoa2020283
Acknowledgements
The authors are indebted to the participants for their close cooperation. The authors would like to gratefully acknowledge the most helpful comments on this paper received from Dr. Maryam Ansari-Lari, Department of Food Hygiene and Public Health, School of Veterinary Medicine, Shiraz University, Shiraz, Iran. This study was supported by Kunduz University (Afghanistan). The authors are grateful for the good cooperation of Dr. Zabihollah Majidi Director of Kunduz COVID-19 treatment specific center, Spin-Zar Hospital and their colleagues.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KS: data collection, methodology, writing original draft of the manuscript; MSA: data collection, methodology; MS: conceptualization, methodology, data analysis, reviewing and editing of the manuscript. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The participants provided their verbal informed consent to be included in the study. The study protocol was approved by the Biology Department Ethics and Research Committee of the Kunduz University (Afghanistan) registered by the officially protocol (N4-17 2.7.99 on 16 June 2020).
Consent for publication
None
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Saify, K., Alborz, M.S. & Saadat, M. Susceptibility to the novel coronavirus disease (COVID-19) is associated with ABO and Rh blood groups: a case-control study from Afghanistan. Egypt J Med Hum Genet 22, 1 (2021). https://doi.org/10.1186/s43042-020-00124-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-020-00124-x