
Abstract
Background
The aim of this review is to (a) characterize social cognition impairments in the domains of emotion recognition (ER) and theory of mind (ToM) in patients with epilepsy and (b) to review assessment tools with a focus on their validity and usability in clinical practice.
Methods
An electronic search for clinical studies investigating social cognition in epilepsy populations vs healthy control subjects (HC) yielded 53 studies for the meta-analysis and descriptive review.
Results
Results suggest that (1) social cognition is significantly impaired in patients with temporal lobe epilepsy (TLE), frontal lobe epilepsy (FLE) and patients with epilepsy not originating within the temporal or frontal lobes including idiopathic generalized epilepsies (eTLE/eFLE); (2) there is no significant difference between eTLE/eFLE and TLE regarding ER, while TLE and FLE patients perform worse than those with eTLE/eFLE, without significant differences between FLE and TLE regarding ToM ability. A descriptive analysis of the most commonly used assessment tools and stimulus material in this field revealed a lack of ecological validity, usability, and economic viability for everyday clinical practice.
Conclusions
Our meta-analysis shows that patients with epilepsy are at a significantly increased risk of deficits in social cognition. However, the underlying multifactorial mechanisms remain unclear. Future research should therefore specifically address the impairment of processing and methodological problems of testing.
Similar content being viewed by others


Background
Social behaviour and social cognition shape the nature of human behaviour [1] and remain essential throughout the entire lifespan [2]. A majority of daily activities are guided by socio-emotional motivations and needs. Consequently, impairment in socio-cognitive abilities is associated with reduced psychosocial well-beings in clinical populations [3, 4]. Furthermore, socio-cognitive impairment seems to be a serious phenotype in many psychiatric, developmental, and neurological disorders, including epilepsy [5]. It is a great step forward that the most recent version of the Diagnostic and Statistical Manual for Mental Disorders (DSM-5) from the American Psychiatric Association [6] highlights the clinical importance of social cognition by recognizing it as a core neurocognitive domain.
Social cognition can be defined as the ability to construe representations about the intentions and motives of others, their mental states, the relationships between oneself and others, as well as the ability to apply those representations to govern social behaviors [7, 8]. In clinical research, social cognition is often divided into the domains of empathy, theory of mind (ToM), and emotion recognition (ER). Most often, it is assessed through neuropsychological performance tests for ER and ToM. The former is usually assessed through the inference of basic emotions based on socio-emotionally salient, context-free, non-verbal sensory input, such as facial expressions, prosody and gait, while the latter implies the inference of more complex mental states, such as motivations, intentions, thoughts, desires, plans, beliefs, and complex emotions (e.g. [7, 9,10,11,12,13,14,15,16,17]). Social cognition enables us to be engaged in social activities and relationships to satisfy our social needs [18], and accumulate individual social capital (i.e., social integration, social support, social network size, etc.), which constitutes a key factor in subjective well-being and health [19,20,21,22,23]. Epidemiological studies have revealed that the major social determinants of quality of life (QoL) are at a considerable risk of impairment in patients with epilepsy [24, 25].
Correct interpretation of social signals and behaviour is a prerequisite for successful interpersonal interaction [26,27,28]. Difficulties in social competence in patients with epilepsy may arise from a number of interrelated factors. From the perspective of social, clinical and developmental psychology, interacting disease-related social and intrapsychic factors can impact on social skills and engagement [29]. From the traditional neuropsychological perspective of the twentieth century, social difficulties may result from cognitive impairment, such as impaired speed and capacity of information processing, attention deficits and memory impairments, which are common in this population [29]. The psychiatric perspective concerns higher prevalence of affective disorders in patients with epilepsy than in the general population [30] and higher rate of fatigue and attention deficit hyperactivity disorder [31]. These alterations may have an impact on social engagement and functioning and result in an impaired coping ability and a poor perceived QoL [24]. A complementary perspective comes from neuroscience and the relatively new area of social cognition. In this discipline, social cognition is defined as a form of information processing that contributes to the correct perception of dispositions and intentions of others [32] and encompasses a wide range of sub-processes. Effective social cognition relies on the exchange of signals, which can be processed at an automatic and controlled level and influenced by motivational aspects [33]. These processes act rapidly in different sensory modalities in parallel, provide social information from others and draw on implicit as well as explicit memories [33, 34]. Imaging and lesion studies have revealed that the cerebral networks employed in social cognition [11, 35,36,37,38,39] are those frequently affected in patients with temporal lobe epilepsy (TLE) and frontal lobe epilepsy (FLE) [27, 40,41,42,43,44,45,46,47].
To date, five meta-analytic reviews have been published since 2015 regarding social cognition in patients with epilepsy [48,49,50,51,52]. The findings of Stewart et al. [48] revealed ToM deficits in adults with TLE and FLE, but not in adults with focal seizures outside temporal and frontal structures (extra-temporal, extra-frontal lobe epilepsy; eTLE/eFLE), while ToM deficits were also observed in children with generalised seizures (caveat: only two studies with adult patients with seizures outside temporal and frontal structures and two studies with children with generalised seizures were included). Edwards et al. [49] found large deficits regarding ER in patients with epilepsy, with TLE patients being significantly impaired on all emotion types except surprise, and patients with genetic generalised epilepsy being significantly impaired in anger, disgust and fear recognition. They also found that in patients with TLE, younger age was associated with lower accuracy. Monti and Meletti [50] reported that ER deficits are consistently observed across studies in patients with TLE, with impaired visual and fear recognition being the most consistently reported deficit, followed by deficits in sadness and disgust recognition, and conflicting evidence regarding the severity of ER deficits in right and left TLE. Furthermore, Bora and Meletti [51] found significant deficits in ToM and facial ER in patients with TLE. They found no significant difference in social cognition between TLE patients with and without medial temporal lobectomy, while earlier onset of seizures was associated with ToM impairment and right-sided TLE was associated with more severe deficits in recognition of fear, sadness and disgust. The most recent meta-analysis [52] reported that FLE and TLE patients have difficulties in all aspects of social cognition relative to the non-clinical controls, while the effect sizes were larger for ToM relative to ER, and the right TLE patients performed significantly worse than the left TLE patients, specifically in the ToM domain.
As Henry et al. [1] pointed out, although the DSM-5 [6] formally recognizes social cognition as a core neurocognitive domain, it does not name or recommend any specific tests for clinical practice. Despite the growing amount of research on social cognition in epilepsy patients and other clinical populations, there is still a paucity of viable and standardized assessment tools for neuropsychological clinical practice with valid norms, satisfactory psychometric properties [1] and usability, especially for non-English speaking populations, although some attempts have been made in recent years [53, 54]. Two main critiques of existing assessment tools are their low ecological validity / artificiality [50, 54, 55] and their narrow scope regarding specific subfunctions [53]. The latter also affects the usability and economic viability of these tests, since global testing via the use of multiple tests for narrowly defined subfunctions in order to broadly assess social cognition becomes too time-consuming for standard clinical practice [53]. For an overview regarding the most commonly used assessment tools for social cognition in epilepsy research, see Ziaei et al. [52].
In this meta-analytic review, we set out to explore the social functioning of patients with FLE, TLE and eTLE/eFLE and to analyse the predominant assessment tools for social cognition in patients with epilepsy, in particular with regard to their viability for everyday clinical practice and ecological validity.
Methods
This meta-analytic review follows the PRISMA recommendations as closely as feasible [56, 57].
Search strategy
An electronic search strategy was used to identify published studies investigating the relationship between social cognition and epilepsy. Original research articles were identified and retrieved via EBSCO (APA PsycInfo and APA PsycArticles) and Embase (Medline and Embase). No date limits were placed on any of the database searches. The following search string was used (title search):
(((affect* OR emot* OR expression* OR social*) AND (perce* OR identif* OR recog* OR process*)) AND (epilepsy OR epilep* OR seizure* OR ictal* OR convulsion*) NOT (mice OR mouse OR rat* OR rodent*)) OR ((tom OR ttom OR (theory AND of AND mind) OR mentalizing OR mentalising OR empath* OR mindreading OR (mind AND reading) OR (social AND inference) OR (pragmatic AND ability) OR pragmati* OR (social AND predictive AND coding) OR (interpersonal AND predictive AND coding) OR (social AND perception)) AND (epilepsy OR epilep* OR seizure* OR ictal* OR convulsion*) NOT (mice OR mouse OR rat* OR rodent*)) OR ((social AND cognition) AND (epilepsy OR epilep* OR seizure* OR ictal* OR convulsion*) NOT (mice OR mouse OR rat* OR rodent*)).
Relevant reviews were consulted to refine the literature search by combining and slightly adjusting their search strings (title and abstract search) to detect subsequent articles [48,49,50,51,52]:
((face OR facial) AND (affect* OR emotion* OR expression*) AND (perce* OR identif* OR recogni* OR process*)) AND ((epilepsy OR epilep* OR seizure* OR (epileptic AND seizure) OR convulsion)) OR ((TLE AND emotion recognition) or (Temporal lobe epilepsy AND emotion recognition) OR (Amygdala AND emotion recognition) NOT (mouse OR rat OR mice)) OR (((Theory of Mind) OR (Theory AND of AND mind) OR (social cognition) OR (social AND cognition) OR (social perception) OR (social AND perception) OR (social behaviour) OR (social AND behaviour) OR (perspective taking) OR (perspective AND taking) OR (mentalising) OR (mentalizing) OR (mind reading) OR (mind AND reading) OR (empathy)) AND ((epileps*) OR (seizure*))).
Backward searching (screening the reference lists of retrieved articles and reviews) and forward searching (subsequent articles citing the retrieved relevant articles) were performed in relevant articles (primary studies and reviews).
The search for relevant articles was finished on June 20th 2021.
Study selection
The titles and abstracts of articles retrieved in the identification process were screened to exclude irrelevant articles. For the included records after the initial screening process, the full articles were inspected to determine the eligibility. The identified studies were included for further statistical and descriptive analysis if they met the following criteria: the diagnosis of an epileptic disorder, the patients were aged 18 and above (mean rounded up, or range 18 and above on the lower end); and behavioral data relating to a social cognitive task in one or more of the following domains were reported; emotion recognition and/or theory of mind. Furthermore, studies needed a control group with no neurological or psychiatric disorders; every study required at least ten participants in the control group and epilepsy group each. If sufficient data were available, pooled effect sizes were calculated and information on sample characteristics and paradigms was extracted from each study. If the data were insufficient for effect size calculation, the authors were contacted. If the authors did not respond after 8 weeks, effect sizes were extracted from previously published meta-analyses [48,49,50,51,52], if available.
Literature search results
After the process of identification, screening and eligibility assessment, the literature search yielded a total of 53 studies that were ultimately included in the meta-analysis and descriptive review (for details, see the PRISMA flowchart in Fig. 1).

Regarding ER, 31 studies [41, 54, 58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86] were included in the TLE subgroup for inferential statistical analysis with a total of 1235 TLE patients and 908 healthy control subjects (HCs), while only 4 studies [18, 87,88,89] were included in the eTLE/eFLE subgroup with a total of 85 eTLE/eFLE patients and 122 HCs. Only one study [90] reported a comparison between FLE patients and HCs, which was therefore not included in the subgroup analysis.
Regarding ToM, 15 studies [54, 58, 60, 63, 74, 91,92,93,94,95,96,97,98,99,100] were included in the TLE subgroup with a total of 617 TLE patients and 449 HCs. The FLE subgroup consisted of 5 studies [42, 90, 101,102,103] with a total of 145 FLE patients and 182 HCs, the eTLE/eFLE subgroup of 6 studies [18, 43, 87, 88, 104, 105] with a total of 157 eTLE/eFLE patients and 212 HCs.
For further details regarding sample characteristics, see Table 1 for TLE, Table 2 for FLE, and Table 3 for eTLE/eFLE.
Analysis
Effect sizes were calculated for results of tests of ER and ToM separately. If more than one effect size was extracted per study and function (ER/ToM), the mean effect size was calculated for further inferential statistical analysis, including subgroup analyses between TLE, FLE and eTLE/eFLE. If two or more of those subgroups were reported in a single study, the study was assigned to the subgroup with the smaller overall number of studies included only to avoid partial statistical dependency/redundancy due to overlapping control groups across studies. In these cases, we summarized those studies with between-group comparisons of different types of epilepsy patients separately. We used Meta-Essentials [106, 107] (a set of Excel workbooks) for the meta-analyses including the subgroup-analyses.
For a descriptive review regarding ER and ToM paradigms, pooled effect sizes (hedges’ g = d), the numbers of studies and subjects for each paradigm were calculated individually.
Results
Emotion recognition
ER was significantly impaired across subgroups compared to HCs (d = 0.80, 95% CI 0.66-0.93, Z = 11.79, p < 0.001). Heterogeneity was significant (I2 = 52.4%, Q = 71.42, p < 0.001). TLE (d = 0.81, Z = 11.01, p < 0.001) as well as eTLE/eFLE (d = 0.67, Z = 4.43, p < 0.001) patients were significantly impaired compared to HCs. Although the TLE subgroup shows a numerically larger effect size than the eTLE/eFLE subgroup, the subgroup-analysis comparing TLE to eTLE/eFLE did not reveal a statistically significant difference (χ2df=1 = 1.10, p = 0.294). The heterogeneity within the subgroups was significant for TLE (I2 = 55.33, Q = 67.16, p < 0.001) but not for eTLE/eFLE (I2 = 5.11%, Q = 3.16, p = 0.367). For an overview see Fig. 2 (forest plot). Due to the low number of studies in the eTLE/eFLE subgroup, these results should be interpreted with caution. The single study comparing FLE patients with HC yielded an effect size of d = 1.70 (95% CI 0.83-2.57), with FLE patients performing significantly worse than HCs [90].

Forest plot of individual and mean weighted effect sizes (Hedge’s g = d) for ER in patients with TLE and eTLE/eFLE in comparison to HC. Abbreviations: CI low, lower limit of the 95% confidence interval; CI up, upper limit of the 95% confidence interval
Visual inspection of the Funnel Plot, Galbraith Plot, Normal Quantile Plot and the Standardized Residual Histogram does not clearly indicate the presence of publication bias in the TLE subgroup. The Egger Regression t-test (t = -0.96, p = 0.346) indicated the absence of severe publication bias [108]. The Failsafe-N as supposed by Rosenthal [109] also did not indicate the presence of publication bias (Failsafe-N = 3127) in the TLE subgroup. Due to the small number of studies, no conclusions can be drawn regarding the presence of publication bias in the eTLE/eFLE subgroup.
Five studies included in the meta-analysis reported statistical comparisons of different types of epilepsy groups regarding ER. A descriptive inspection of effect sizes and p-values revealed a tendency of TLE patients performing worse in ER tasks than eTLE/eTLE patients [18, 88, 89]. No studies reported comparisons between FLE and eTLE/eFLE patients or between TLE and eTLE/eFLE patients. For further details, see Table 4.
Theory of mind
ToM was significantly impaired across subgroups compared to HCs (d = 0.87, 95% CI 0.71-1.03, Z = 11.00, p < 0.001). Heterogeneity was significant (I2= 53.18%, Q = 53.40, p = 0.001). ToM was significantly impaired in TLE (d = 0.92, Z = 8.64, p < 0.001) as well as FLE (d = 1.16, Z = 24.43, p < 0.001) and eTLE/eFLE (d = 0.55, Z = 3.49, p < 0.001) patients compared to HCs. The between-group heterogeneity across all subgroups was significant (Qbet = 14.94, p < 0.001). Post-hoc comparisons revealed that TLE and FLE patients had significantly more impaired ToM than eTLE/eFLE patients (TLE vs eTLE/eFLE: χ2df=1 = 8.7, p = 0.003; FLE vs eTLE/eFLE: χ2df=1 = 13.77, p < 0.001). No statistically significant difference was found between TLE and FLE patients (χ2df=1 = 2.76, p = 0.097). There was no evidence for significant heterogeneity within groups for eTLE/eFLE (I2 = 40.50%, Q = 8.40, p = 0.135) and FLE (I2 = 0.00%, Q = 0.57, p = 0.966), except for the TLE group (I2 = 52.52%, Q = 29.49, p = 0.009). Again, the results should be interpreted with caution due to the small sample sizes in the eTLE/eFLE and FLE subgroups. For an overview see Fig. 3 (forest plot).

Forest plot of individual and mean weighted effect sizes (Hedge’s g = d) for ToM in patients with TLE, FLE and eTLE/eFLE in comparison to HC. Abbreviations: CI low, lower limit of the 95% confidence interval; CI up, upper limit of the 95% confidence interval
Visual inspection of the Funnel Plot, Galbraith Plot, Normal Quantile Plot, the Standardized Residual Histogram, and the Failsafe-N (Failsafe-N = 984) proposed by Rosenthal [109] did not indicate the presence of publication bias in the TLE subgroup. Due to the small number of studies, no conclusion can be drawn regarding the presence of publication bias in the eTLE/eFLE and the FLE subgroups.
Five studies included in the meta-analysis reported statistical comparisons of ToM between different types of epilepsy. A descriptive inspection of effect sizes and p-values revealed that TLE patients tend to perform worse in ToM tasks than eTLE/eTLE patients [18, 43, 88]. No clear trend was found from the comparison between FLE and TLE patients [42, 101], while no study reported a comparison between FLE and eTLE/eFLE patients. For further details, see Table 4.
The assessment of emotion recognition in epilepsy
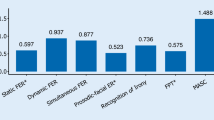
The paradigms used for the assessment of emotion recognition in epilepsy research can be roughly categorized into three types with regards to the modality. The vast majority of studies used facial emotion recognition paradigms [110,111,112,113,114,115,116] predominantly by using stimulus material from the Ekman & Friesen series of static pictures [110]. Only a small number of studies utilized task paradigms with prosodic emotion recognition [117,118,119,120] and tasks for affect recognition in emotionally expressive gaits and postures [121] to assess emotion recognition. Regarding the presentation of the stimuli, there are a broad variety of presentation methods and assessment designs, most specifically designed for individual studies. These included, for example, morphed pictures of the Ekman & Friesen series [66] and selective presentation of a subset of basic emotions [58, 86]. Only a small number of studies used more comprehensive batteries [54, 122,123,124]. For more detailed information see Table 5.
The assessment of theory of mind in epilepsy
The most commonly used task in the assessment of ToM in epilepsy is the Faux Pas Test, a text-based task in which participants are required to make ToM inferences in stories about social faux pas [125]. Other commonly used tasks include the Reading the Mind in the Eyes test [126], in which participants are required to infer mental states based on photographs of the eye region of faces, and the Frith-Happé Animations [127, 128], in which participants are required to attribute mental states to moving geometric shapes. Other paradigms are rarely used, including the inference of mental states based on cartoons [129, 130], short stories [131], movies [132], the recognition/comprehension of irony [54], sarcasm [100], metaphor and hinting [105]. Again, the use of comprehensive test batteries is rare [54, 124]. For an overview see Table 6.
Discussion
Social cognition in epilepsy
In this meta-analytic review, we demonstrated that ER is impaired in TLE and eTLE/eFLE patients and ToM is impaired in TLE, FLE and eTLE/eFLE patients. There are no significant differences in ER performance between TLE and eTLE/eFLE patients, although a declarative review of reported within-study comparisons revealed a trend of TLE patients performing worse than eTLE/eFLE patients in ER; and there is also no significant difference in ToM between FLE and TLE patients. There are significant differences in ToM ability between eTLE/eFLE and FLE as well as between eTLE/eFLE and TLE patients, with less pronounced deficits in eTLE/eFLE. Due to the small number of studies comparing eTLE/eFLE and FLE, the results should be interpreted with caution. While there is a growing number of studies on social cognition in TLE, there is still a paucity of studies on FLE and eTLE/eFLE patients, especially regarding ER. More studies are needed, particularly to identify specific eTLE/eFLE pathologies and disorders with higher risks of socio-cognitive impairment.
Although cognitive domains including attention, memory, and executive functioning have been found to be impaired in epilepsy, few studies have addressed the impairment in the context of social cognition [133]. It has been argued by several authors that the neurocognitive deficits may contribute to impairment of social cognition in epilepsy patients, for example, deficits in executive functions in patients with idiopathic generalized epilepsies [134]. To date, there is a paucity of research on this subject. Current research presents conflicting evidence on a relationship between general intelligence and emotion recognition in TLE [50]. It is argued that deficits in social cognition are independent of intellectual disability in epilepsy [135], and that there is no formal correlation between ToM and general intelligence in epilepsy patients [48]. Others have pointed out conflicting evidence for a correlation between IQ and ToM, while there is no evidence for a significant correlation between verbal IQ and ToM in epilepsy patients [48]. Furthermore, it has been pointed out that although there is evidence for impaired executive functioning in epilepsy subgroups such as TLE, most studies have failed to identify correlations between executive functions and social cognition in patients with idiopathic generalized epilepsy[48, 134]. Due to the paucity of research and conflicting evidence regarding the relationship between neurocognitive functions, general cognitive ability and social cognition, cognitive deficits may nevertheless play a role in the associated impairments of social cognition and may have confounded the current as well as previous meta-analytic reviews in this field. The discrepancies of the results among studies, as well as the high level of heterogeneity in social cognition within subgroups in this meta-analysis, may be due to the variety of tests used to measure social cognition, as well as the variety of patients included in the primary studies (for example, heterogeneity regarding disease- and patient-related variables, selective samples of subgroups such as TLE patients after amygdalo-hippocampectomy, or patients with idiopathic generalized epilepsies in the eTLE/eFLE subgroup). This prevents accurate comparison between results and limits the reproducibility.
A limitation of this meta-analysis is the lack of inclusion of potentially relevant covariates such as the subtype and etiology of the epileptic syndrome – especially with regard to the very broadly defined and etiologically diverse subgroup of eTLE/eFLE patients – age at seizure onset, seizure laterality, history of febrile seizures, seizure frequency, history of brain surgery, duration of epilepsy, and pharmacological therapy. These variables tend to be underreported in primary studies. In particular, early seizure onset seems to be associated with more severe impairment in ToM and ER in epilepsy patients [49, 51, 135], as well as longer duration of disease [50, 135]. Furthermore, there is a tendency for more severe ER and ToM deficits in right-sided TLE compared to left-sided TLE [51, 52]. Systematic reviews suggest no relevant differences between TLE patients with or without as well as pre- and post-temporal lobectomy surgery regarding social cognition [50, 51]. There is still a paucity of research and conflicting evidence regarding the effects of pharmacological therapy on social cognition in epilepsy patients [50, 136].
Assessment tools in clinical practice and research
Ecological validity
The most common approach to testing ER in epilepsy research is to label photographs of static facial expressions of basic emotions [54] in a variety of ways (matching tasks, labeling tasks, etc.). Such tasks do not correspond with the dynamic visuo-spatial and temporal information in faces processed in everyday social interactions [55] and do not reflect the multimodality of everyday emotion recognition [1, 54], including body movement, prosody, verbal information and context. Regarding ToM, the most commonly used assessment tools in epilepsy research are too artificial in nature (short stories, cartoons, static pictures of eyes, moving triangles) and/or assess narrowly defined sub-processes (e.g. faux-pas detection), which limit their ecological validity [54].
Economic viability / usability in clinical practice
Many of the assessment tools that lack ecological validity are often well suited for clinical practice with regard to the complexity and duration of application. However, due to their lack of ecological validity and narrow scope regarding socio-cognitive subprocesses, it is necessary to use multiple tools to achieve a more comprehensive assessment. Accordingly, attempts to construct ecologically valid assessment tools, such as the Movie for the Assessment of Social Cognition (MASC) [132] and more comprehensive batteries, such as the NEmo battery (Networks of Emotion Processing) [54], CATS (comprehensive affect testing system) [122], and TASIT (The Awareness of Social Inference Test) [124], result in longer administration times, which are often too long for everyday clinical neuropsychological practice.
Attempts to provide new and apply existing more ecologically valid and/or economically viable assessment tools for social cognition are scarce in clinical epilepsy research (e.g. [1, 53, 140]) as well as in other clinical populations [138].
Future directions
We recommend an increased effort in the development and use of multimodal, comprehensive, ecologically valid, economically viable assessment tools for social cognition in epilepsy research and clinical practice as well as in other clinical populations at risk of socio-cognitive impairment. We suggest two approaches for the development of new research tools: (a) short tests with high ecological validity and a broad integration of socio-cognitive subprocesses, (b) short screening tools for social cognition via the integration of parts of multiple established assessment tools in the manner of, for example, the Montreal Cognitive Assessment [137] for general cognitive function or Frontal Assessment Battery [139] for executive function.
Future studies that test multiple subfunctions in ER, ToM, general cognition, speed, attention, memory, and executive functions in the same population would be informative. Furthermore, larger longitudinal studies with a broad variety of relevant covariates would help advance our understanding of the effects of epilepsy duration, seizure frequency, age of epilepsy onset, effect of seizure freedom, and antiepileptic drugs on social cognition. The standardization of terminology and testing in the field of applied social cognition would enhance the reproducibility and comparability of results.
The difficulties with social interaction and functioning observed in some epilepsy patients may, at least in part, be due to an altered ability to interpret emotions or mental states. It appears that epilepsy patients may struggle more with subtle or nuanced expressions of emotion. Currently, it is unknown how the socio-cognitive deficits seen in some patients significantly affect diverse areas of life including employment, romantic and family relationships, and friendships. It is therefore important to quantify the functional burden of impaired social cognition in epilepsy to determine its specific clinical relevance in future studies.
Conclusions
Considering the importance of social skills in personal and economic success and QoL, the exclusion of social cognition from the canon of relevant functions investigated in epilepsy as well as the many other conditions affecting social cognition [5] can no longer be justified. A richer understanding of the nature of social cognition in epilepsy may help further characterize certain epilepsy syndromes, and facilitate development of therapeutic interventions to improve social abilities in these patients. Further studies on social cognition in epilepsy, especially in FLE and eTLE/eFLE, with the use of ecologically valid and diverse, multimodal assessment tools, are recommended. Further, there is a need for standardized, psychometrically sound, ecologically valid and economically viable assessment tools for social cognition in daily clinical practice with (but not limited to) epilepsy patients [140].
Availability of data and materials
The datasets used during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- eFLE/eTLE:
-
Extra-temporal/extra-frontal epilepsy
- ER:
-
Emotion recognition
- FLE:
-
Frontal lobe epilepsy
- QoL:
-
Quality of life
- TLE:
-
Temporal lobe epilepsy
- ToM:
-
Theory of mind
References
Henry JD, Von Hippel W, Molenberghs P, Lee T, Sachdev PS. Clinical assessment of social cognitive function in neurological disorders. Nat Rev Neurol. 2016;12(1):28–39.
Ronay R, von Hippel W. Sensitivity to changing contingencies predicts social success. Soc Psychol Personal Sci. 2015;6(1):23–30.
Brüne M, Abdel-Hamid M, Lehmkämper C, Sonntag C. Mental state attribution, neurocognitive functioning, and psychopathology: what predicts poor social competence in schizophrenia best? Schizophr Res. 2007;92(1–3):151–9.
Phillips LH, Scott C, Henry JD, Mowat D, Bell JS. Emotion perception in Alzheimer’s disease and mood disorder in old age. Psychol Aging. 2010;25(1):38–47.
Cotter J, Granger K, Backx R, Hobbs M, Looi CY, Barnett JH. Social cognitive dysfunction as a clinical marker: a systematic review of meta-analyses across 30 clinical conditions. Neurosci Biobehav Rev. 2017;2018(84):92–9.
APA. Diagnostic an statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
Broicher S, Jokeit H. Emotional agnosis and theory of mind. In: Trimble MR, Schmitz B, editors. The neuropsychiatry of epilepsy. 2nd ed. New York, New York, USA: Cambridge University Press; 2011. p. 109–23.
Beer JS, Ochsner KN. Social cognition: a multi level analysis. Brain Res. 2006;1079(1):98–105.
Adolphs R. Recognizing emotion from facial expressions: psychological and neurological mechanisms. Behav Cogn Neurosci Rev. 2002;1(1):21–62.
Ekman P. Are there basic emotions? Psychol Rev. 1992;99(3):550–3.
Dricu M, Frühholz S. Perceiving emotional expressions in others: activation likelihood estimation meta-analyses of explicit evaluation, passive perception and incidental perception of emotions. Neurosci Biobehav Rev. 2016;71:810–28.
Mitchell RLC, Phillips LH. The overlapping relationship between emotion perception and theory of mind. Neuropsychologia. 2015;70:1–10.
Phillips ML. Understanding the neurobiology of emotion perception: Implications for psychiatry. Br J Psychiatry. 2003;182(MAR.):190–2.
Premack D, Woodruff G. Does the chimpanzee have a theory of mind? Behav Brain Sci. 1978;4:515–26.
Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21(1):37–46.
Byom LJ, Mutlu B. Theory of mind: mechanisms, methods, and new directions. Front Hum Neurosci. 2013;7(JUL):1–12.
Frith CD, Frith U. Mechanisms of social cognition. Annu Rev Psychol. 2012;63:287–313.
Broicher SD, Kuchukhidze G, Grunwald T, Krämer G, Kurthen M, Jokeit H. “Tell me how do I feel” - Emotion recognition and theory of mind in symptomatic mesial temporal lobe epilepsy. Neuropsychologia. 2012;50(1):118–28.
Helliwell JF, Putnam RD. The social context of well-being. Philos Trans R Soc B Biol Sci. 2004;359(1449):1435–46.
Helliwell JF, Aknin LB, Shiplett H, Huang H, Wang S. Social Capital and Prosocial Behaviour as Sources of Well-Being. In: Diener E, Oishi S, Tay L, editors. Handbook of well-being. Salt Lake City, UT: DEF Publishers; 2018. https://www.nobascholar.com/.
Thoits PA. Stress, coping, and social support processes: where are we? What next? J Health Soc Behav. 1995;1(Extra Issue):53–79.
Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav. 2011;52(2):145–61.
Umberson D, Karas MJ. Social Relationships and health: a flashpoint for health policy. J Health Soc Behav. 2010;51:S54-66.
Sherman EMS. Maximizing quality of life in people living with epilepsy. Can J Neurol Sci. 2009;36(SUPPL. 2):S17–24.
Beghi E. Social functions and socioeconomic vulnerability in epilepsy. Epilepsy Behav. 2019;100:1–14.
Steiger BK, Jokeit H. Why epilepsy challenges social life. Seizure. 2017;44:194–8.
Broicher S, Jokeit H. On clinical diagnostics of social cognition in patients with epilepsies. Epileptologie. 2011;28:215–28.
Szemere E, Jokeit H. Quality of life is social - towards an improvement of social abilities in patients with epilepsy. Seizure. 2015;26:12–21.
McCagh J, Fisk JE, Baker GA. Epilepsy, psychosocial and cognitive functioning. Epilepsy Res. 2009;86(1):1–14.
Gaitatzis A, Trimble MR, Sander JW. The psychiatric comorbidity of epilepsy. Acta Neurol Scand. 2004;110(4):207–20.
Dunn DW, Austin JK, Harezlak J, Ambrosius WT. ADHD and epilepsy in childhood. Dev Med Child Neurol. 2003;45(1):50–4.
Brothers L. The neural basis of primate social the neural basis of primate communication. Motiv Emot. 1990;14(2):81–91.
Lieberman MD. Social cognitive neuroscience: a review of core processes. Annu Rev Psychol. 2007;58(1):259–89.
Haxby JV, Hoffman EA, Gobbini MI. Human neural systems for face recognition and social communication. Biol Psychiatry. 2002;51(1):59–67.
Pannese A, Grandjean D, Frühholz S. Amygdala and auditory cortex exhibit distinct sensitivity to relevant acoustic features of auditory emotions. Cortex. 2016;85:116–25.
Abu-Akel A, Shamay-Tsoory S. Neuroanatomical and neurochemical bases of theory of mind. Neuropsychologia. 2011;49(11):2971–84.
Fusar-Poli P, Placentino A, Carletti F, Landi P, Allen P, Surguladze S, et al. Functional atlas of emotional faces processing: a voxel-based meta-analysis of 105 functional magnetic resonance imaging studies. J Psychiatry Neurosci. 2009;34(6):418–32.
Schurz M, Radua J, Aichhorn M, Richlan F, Perner J. Fractionating theory of mind: a meta-analysis of functional brain imaging studies. Neurosci Biobehav Rev. 2014;42:9–34.
Wang Y, Metoki A, Alm KH, Olson IR. White matter pathways and social cognition. Neurosci Biobehav Rev. 2018;90:350–70.
Kirsch HE. Social cognition and epilepsy surgery. Epilepsy Behav. 2006;8(1):71–80.
Meletti S, Benuzzi F, Rubboli G, Cantalupo G, Stanzani Maserati M, Nichelli P, et al. Impaired facial emotion recognition in early-onset right mesial temporal lobe epilepsy. Neurology. 2003;60(3):426–31.
Giovagnoli AR, Parente A, Villani F, Franceschetti S, Spreafico R. Theory of mind and epilepsy: what clinical implications? Epilepsia. 2013;54(9):1639–46.
Schacher M, Winkler R, Grunwald T, Kraemer G, Kurthen M, Reed V, et al. Mesial temporal lobe epilepsy impairs advanced social cognition. Epilepsia. 2006;47(12):2141–6.
Toller G, Adhimoolam B, Grunwald T, Huppertz HJ, Kurthen M, Rankin KP, et al. Right mesial temporal lobe epilepsy impairs empathy-related brain responses to dynamic fearful faces. J Neurol. 2015;262(3):729–41.
Steiger BK, Muller AM, Spirig E, Toller G, Jokeit H. Mesial temporal lobe epilepsy diminishes functional connectivity during emotion perception. Epilepsy Res. 2017;134(April):33–40.
Ives-Deliperi V, Butler JT. Mechanisms of cognitive impairment in temporal lobe epilepsy: a systematic review of resting-state functional connectivity studies. Epilepsy Behav. 2021;115:107686.
Ives-Deliperi VL, Jokeit H. Impaired social cognition in epilepsy: a review of what we have learnt from neuroimaging studies. Front Neurol. 2019;10(September):940.
Stewart E, Catroppa C, Lah S. Theory of mind in patients with epilepsy: a systematic review and meta-analysis. Neuropsychol Rev. 2016;26(1):3–24.
Edwards M, Stewart E, Palermo R, Lah S. Facial emotion perception in patients with epilepsy: a systematic review with meta-analysis. Neurosci Biobehav Rev. 2017;83:212–25.
Monti G, Meletti S. Emotion recognition in temporal lobe epilepsy: a systematic review. Neurosci Biobehav Rev. 2015;55:280–93.
Bora E, Meletti S. Social cognition in temporal lobe epilepsy: A systematic review and meta-analysis. Epilepsy Behav. 2016;60:50–7.
Ziaei, M., Arnold, C., Thompson, K., & Reutens D. Social cognition in frontal and temporal lobe epilepsy : systematic review and meta-analysis. MedRxiv [Preprint]. 2021 [cited April 30, 2021]. Available from: https://doi.org/10.1101/2021.04.28.21255765.
Martory MD, Pegna AJ, Sheybani L, Métral M, Bernasconi Pertusio F, Annoni JM. Assessment of social cognition and theory of mind: Initial validation of the geneva social cognition scale. Eur Neurol. 2015;74(5–6):288–95.
Bauer J, Kegel LC, Steiger BK, Jokeit H. Assessment tools for social cognition in epilepsy. Zeitschrift fur Epileptol. 2019;32(3):183–6.
Arsalidou M, Morris D, Taylor MJ. Converging evidence for the advantage of dynamic facial expressions. Brain Topogr. 2011;24(2):149–63.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62:1–34.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, PRISMA, et al. explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2020;2021:372.
Amlerova J, Cavanna AE, Bradac O, Javurkova A, Raudenska J, Marusic P. Emotion recognition and social cognition in temporal lobe epilepsy and the effect of epilepsy surgery. Epilepsy Behav. 2014;36:86–9.
Bonora A, Benuzzi F, Monti G, Mirandola L, Pugnaghi M, Nichelli P, et al. Recognition of emotions from faces and voices in medial temporal lobe epilepsy. Epilepsy Behav. 2011;20(4):648–54.
Boucher O, Rouleau I, Lassonde M, Lepore F, Bouthillier A, Nguyen DK. Social information processing following resection of the insular cortex. Neuropsychologia. 2015;71:1–10.
Brierley B, Medford N, Shaw P, David AS. Emotional memory and perception in temporal lobectomy patients with amygdala damage. J Neurol Neurosurg Psychiatry. 2004;75(4):593–9.
Carvajal F, Rubio S, Martín P, Serrano JM, García-Sola R. Perception and recall of faces and facial expressions following temporal lobectomy. Epilepsy Behav. 2009;14(1):60–5.
Cohn M, St-Laurent M, Barnett A, McAndrews MP. Social inference deficits in temporal lobe epilepsy and lobectomy: risk factors and neural substrates. Soc Cogn Affect Neurosci. 2015;10(5):636–44.
Glogau S, Ellgring H, Elger CE, Helmstaedter C. Face and facial expression memory in temporal lobe epilepsy patients: preleminary results. Epilepsy Behav. 2004;5(1):106–12.
Gomez-Ibañez A, Urrestarazu E, Viteri C. Recognition of facial emotions and identity in patients with mesial temporal lobe and idiopathic generalized epilepsy: an eye-tracking study. Seizure. 2014;23(10):892–8.
Gosselin N, Peretz I, Hasboun D, Baulac M, Samson S. Impaired recognition of musical emotions and facial expressions following anteromedial temporal lobe excision. Cortex. 2011;47(9):1116–25.
Hennion S, Szurhaj W, Duhamel A, Lopes R, Tyvaert L, Derambure P, et al. Characterization and prediction of the recognition of emotional faces and emotional bursts in temporal lobe epilepsy. J Clin Exp Neuropsychol. 2015;37(9):931–45.
Hlobil U, Rathore C, Alexander A, Sarma S, Radhakrishnan K. Impaired facial emotion recognition in patients with mesial temporal lobe epilepsy associated with hippocampal sclerosis (MTLE-HS): Side and age at onset matters. Epilepsy Res. 2008;80(2–3):150–7.
Huang YA, Dupont P, Van de Vliet L, Jastorff J, Peeters R, Theys T, et al. Network level characteristics in the emotion recognition network after unilateral temporal lobe surgery. Eur J Neurosci. 2020;52(5):3470–84.
Meletti S, Benuzzi F, Cantalupo G, Rubboli G, Tassinari CA, Nichelli P. Facial emotion recognition impairment in chronic temporal lobe epilepsy. Epilepsia. 2009;50(6):1547–59.
Meletti S, Picardi A, De Risi M, Monti G, Esposito V, Grammaldo LG, et al. The affective value of faces in patients achieving long-term seizure freedom after temporal lobectomy. Epilepsy Behav. 2014;36:97–101.
Palermo R, Schmalzl L, Mohamed A, Bleasel A, Miller L. The effect of unilateral amygdala removals on detecting fear from briefly presented backward-masked faces. J Clin Exp Neuropsychol. 2010;32(2):123–31.
Sedda A, Rivolta D, Scarpa P, Burt M, Frigerio E, Zanardi G, et al. Ambiguous emotion recognition in temporal lobe epilepsy: the role of expression intensity. Cogn Affect Behav Neurosci. 2013;13(3):452–63.
Shaw P, Lawrence E, Bramham J, Brierley B, Radbourne C, David AS. A prospective study of the effects of anterior temporal lobectomy on emotion recognition and theory of mind. Neuropsychologia. 2007;45(12):2783–90.
McClelland S, Garcia RE, Peraza DM, Shih TT, Hirsch LJ, Hirsch J, et al. Facial emotion recognition after curative nondominant temporal lobectomy in patients with mesial temporal sclerosis. Epilepsia. 2006;47(8):1337–42.
Rotshtein P, Richardson MP, Winston JS, Kiebel SJ, Vuilleumier P, Eimer M, et al. Amygdala damage affects event-related potentials for fearful faces at specific time windows. Hum Brain Mapp. 2010;31(7):1089–105.
Szaflarski JP, Allendorfer JB, Heyse H, Mendoza L, Szaflarski BA, Cohen N. Functional MRI of facial emotion processing in left temporal lobe epilepsy. Epilepsy Behav. 2014;32:92–9.
Szaflarski JP, Allendorfer JB, Nenert R, LaFrance WC, Barkan HI, DeWolfe J, et al. Facial emotion processing in patients with seizure disorders. Epilepsy Behav. 2018;79:193–204.
Tanaka A, Akamatsu N, Yamano M, Nakagawa M, Kawamura M, Tsuji S. A more realistic approach, using dynamic stimuli, to test facial emotion recognition impairment in temporal lobe epilepsy. Epilepsy Behav. 2013;28(1):12–6.
Walpole P, Isaac CL, Reynders HJ. A comparison of emotional and cognitive intelligences in people with and without temporal lobe epilepsy. Epilepsia. 2008;49(8):1470–4.
Wendling AS, Steinhoff BJ, Bodin F, Staack AM, Zentner J, Scholly J, et al. Selective amygdalohippocampectomy versus standard temporal lobectomy in patients with mesiotemporal lobe epilepsy and unilateral hippocampal sclerosis: post-operative facial emotion recognition abilities. Epilepsy Res. 2015;111:26–32.
Åhs F, Engman J, Persson J, Larsson EM, Wikström J, Kumlien E, et al. Medial temporal lobe resection attenuates superior temporal sulcus response to faces. Neuropsychologia. 2014;61(1):291–8.
Anderson AK, Spencer DD, Fulbright RK, Phelps EA. Contribution of the anteromedial temporal lobes to the evaluation of facial emotion. Neuropsychology. 2000;14(4):526–36.
Arani AM. A comparison of facial emotion recognition in patients with temporal lobe epilepsy and non-epileptics. Adv Nurs Midwifery. 2020;29(2):12–8.
Batut AC, Gounot D, Namer IJ, Hirsch E, Kehrli P, Metz-Lutz MN. Neural responses associated with positive and negative emotion processing in patients with left versus right temporal lobe epilepsy. Epilepsy Behav. 2006;9(3):415–23.
Benuzzi F, Meletti S, Zamboni G, Calandra-Buonaura G, Serafini M, Lui F, et al. Impaired fear processing in right mesial temporal sclerosis: A fMRI study. Brain Res Bull. 2004;63(4):269–81.
Hu Y, Jiang Y, Hu P, Ma H, Wang K. Impaired social cognition in patients with interictal epileptiform discharges in the frontal lobe. Epilepsy Behav. 2016;57:46–54.
Realmuto S, Zummo L, Cerami C, Agrò L, Dodich A, Canessa N, et al. Social cognition dysfunctions in patients with epilepsy: evidence from patients with temporal lobe and idiopathic generalized epilepsies. Epilepsy Behav. 2015;47:98–103.
Reynders HJ, Broks P, Dickson JM, Lee CE, Turpin G. Investigation of social and emotion information processing in temporal lobe epilepsy with ictal fear. Epilepsy Behav. 2005;7(3):419–29.
Farrant A, Morris RG, Russell T, Elwes R, Akanuma N, Alarcón G, et al. Social cognition in frontal lobe epilepsy. Epilepsy Behav. 2005;7(3):506–16.
Bala A, Okruszek Ł, Piejka A, Głębicka A, Szewczyk E, Bosak K, et al. Social perception in mesial temporal lobe epilepsy: Interpreting social information from moving shapes and biological motion. J Neuropsychiatry Clin Neurosci. 2018;30(3):228–35.
Giovagnoli AR, Canafoglia L, Reati F, Raviglione F, Franceschetti S. The neuropsychological pattern of Unverricht-Lundborg disease. Epilepsy Res. 2009;84(2–3):217–23.
Hennion S, Delbeuck X, Koelkebeck K, Brion M, Tyvaert L, Plomhause L, et al. A functional magnetic resonance imaging investigation of theory of mind impairments in patients with temporal lobe epilepsy. Neuropsychologia. 2016;93:271–9.
Li Y-H, Chiu M-J, Yeh Z-T, Liou H-H, Cheng T-W, Hua M-S. Theory of mind in patients with temporal lobe epilepsy. J Int Neuropsychol Soc. 2013;19(5):594–600.
Okruszek Ł, Bala A, Wordecha M, Jarkiewicz M, Wysokiński A, Szczepocka E, et al. Social cognition in neuropsychiatric populations: a comparison of theory of mind in schizophrenia and mesial temporal lobe epilepsy. Nat Sci Reports. 2017;7(484):1–9.
Wang W-H, Yu H-Y, Hua M-S. Theory of mind and its brain distribution in patients with temporal lobe epilepsy. Int J Med Heal Sci. 2015;9(5):408–11.
Broicher SD, Frings L, Huppertz HJ, Grunwald T, Kurthen M, Krämer G, et al. Alterations in functional connectivity of the amygdala in unilateral mesial temporal lobe epilepsy. J Neurol. 2012;259(12):2546–54.
Giovagnoli AR, Parente A, Didato G, Deleo F, Villani F. Expanding the spectrum of cognitive outcomes after temporal lobe epilepsy surgery: a prospective study of theory of mind. Epilepsia. 2016;57(6):920–30.
Giovagnoli AR, Parente A, Ciuffini R, Tallarita GM, Turner K, Maialetti A, et al. Diversified social cognition in temporal lobe epilepsy. Acta Neurol Scand. 2021;143(4):396–406.
Hennion S, Delbeuck X, Duhamel A, Lopes R, Semah F, Tyvaert L, et al. Characterization and prediction of theory of mind disorders in temporal lobe epilepsy. Neuropsychology. 2015;29(3):485–92.
Giovagnoli AR, Franceschetti S, Reati F, Parente A, MacCagnano C, Villani F, et al. Theory of mind in frontal and temporal lobe epilepsy: cognitive and neural aspects. Epilepsia. 2011;52(11):1995–2002.
Giovagnoli AR, Tallarita GM, Parente A, Pastori C, de Curtis M. The understanding of mental states and the cognitive phenotype of frontal lobe epilepsy. Epilepsia. 2020;61(4):747–57.
Javor A, Ciumas C, Ibarrola D, Ryvlin P, Rheims S. Social cognition, behaviour and therapy adherence in frontal lobe epilepsy: A study combining neuroeconomic and neuropsychological methods. R Soc Open Sci. 2019;6(8):1–14.
Giorgi FS, Guida M, Caciagli L, Pagni C, Pizzanelli C, Bonanni E, et al. Social cognition in Juvenile myoclonic epilepsy. Epilepsy Res. 2016;128:61–7.
Morou N, Papaliagkas V, Markouli E, Karagianni M, Nazlidou E, Spilioti M, et al. Theory of mind impairment in focal versus generalized epilepsy. Epilepsy Behav. 2018;88:244–50.
Suurmond R, van Rhee H, Hak T. Introduction, comparison, and validation of meta-essentials: a free and simple tool for meta-analysis. Res Synth Methods. 2017;8(4):537–53.
van Rhee H, Suurmond R, Hak T. User manual for Meta-Essentials: Workbooks for meta-analysis (Version 1.4) Rotterdam, The Netherlands: Erasmus Research Institute of Management. Retrieved from www.erim.eur.nl/research-support/meta-essentials.
Card NA. Applied Meta-Analysis for Social Science Research. Kenny DA, Little TD, editors. New York, New York, USA: The Guilford Press; 2012.
Rosenthal R. The file drawer problem and tolerance for null results. Psychol Bull. 1979;86(3):638–41.
Friesen WV, Ekman P. Pictures of facial affect. Palo Alto: Consult Psychol Press. 1976.
Tottenham T, Tanaka JW, Leon AC, McCarry T, Nurse M, Hare T, Marcus DJ, et al. The NimStim set of facial expressions: judgments from untrained research participants. Psychiatry Res. 2009;168(3):242–9.
Goeleven E, De Raedt R, Leyman L, Verschuere B. The Karolinska directed emotional faces: a validation study. Cogn Emot. 2008;22(6):1094–118.
Langner O, Dotsch R, Bijlstra G, Wigboldus DHJ, Hawk ST, van Knippenberg A. Presentation and validation of the radboud faces database. Cogn Emot. 2010;24(8):1377–88.
Roy S, Roy C, Ethier-Majcher C, Fortin I, Belin P, Gosselin F. STOIC: a database of dynamic and static faces expressing highly recognizable emotions. J Vis. 2007;7(514):944.
Gur RC, Sara R, Hagendoorn M, Marom O, Hughett P, Macy L, et al. A method for obtaining 3-dimensional facial expressions and its standardization for use in neurocognitive studies. J Neurosci Methods. 2002;115(2):137–43.
Kan Y, Kawamura M, Hasegawa Y, Mochizuki S, Nakamura K. Recognition of emotion from facial, prosodic and written verbal stimuli in Parkinson’s disease. Cortex. 2002;38(4):623–30.
Ariatti A, Benuzzi F, Nichelli P. Recognition of emotions from visual and prosodic cues in Parkinson’s disease. Neurol Sci. 2008;29(4):219–27.
Burkhardt F, Paeschke A, Rolfes M, Sendlmeier W, Weiss B. A database of German emotional speech. 9th Eur Conf Speech Commun Technol. 2005;5:1517–20.
Scott SK, Young AW, Calder AJ, Hellawell DJ, Aggleton JP, Johnson M. Impaired auditory recognition of fear and anger fellowing bilateral amygdala lesions. Nature. 1997;385:254–7.
Belin P, Fillion-Bilodeau S, Gosselin F. The montreal affective voices: a validated set of nonverbal affect bursts for research on auditory affective processing. Behav Res Methods. 2008;40(2):531–9.
Jastorff J, Huang YA, Giese MA, Vandenbulcke M. Common neural correlates of emotion perception in humans. Hum Brain Mapp. 2015;36(10):4184–201.
Froming KB, Levy CM, Schaffer SG, Ekman P. Comprehensive affect testing system(CATS).© 2000–2006.
Bowers D, Ph D, Blonder LX, Heilman KM. Florida affect battery. Center for Neuropsychological Studies Cognitive Neuroscience Laboratory University of Florida; 1999.
McDonald S, Flanagan S, Rollins J, Kinch J. A new clinical tool for assessing social perception after traumatic brain injury. J Head Trauma Rehabil. 2003;18(3):219–38.
Baron-Cohen S, O’Riordan M, Stone V, Jones R, Plaisted K. A new test of social sensivity: recognition of faux pas in normally developing children and children with Asperger syndrome. J Autism Dev Disord. 1999;29(5):407–18.
Baron-Cohen S, Jolliffe T, Mortimore C, Robertson M. Another advanced test of theory of mind: evidence from very high functioning adults with autism or asperger syndrome. J Child Psychol Psychiatry Allied Discip. 1997;38(7):813–22.
Abell F, Happé F, Frith U. Do triangles play tricks? Attribution of mental states to animated shapes in normal and abnormal development. Cogn Dev. 2000;15(1):1–16.
White SJ, Coniston D, Rogers R, Frith U. Developing the Frith-Happé animations: a quick and objective test of theory of mind for adults with autism. Autism Res. 2011;4(2):149–54.
Gallagher HL, Happé F, Brunswick N, Fletcher PC, Frith U, Frith CD. Reading the mind in cartoons and stories: an fMRI study of “theory of mind” in verbal and nonverbal tasks. Neuropsychologia. 2000;38(1):11–21.
Dodich A, Cerami C, Canessa N, Crespi C, Iannaccone S, Marcone A, et al. A novel task assessing intention and emotion attribution: Italian standardization and normative data of the story-based empathy task. Neurol Sci. 2015;36(10):1907–12.
Happé F. An advanced test of theory of mind: understanding of story characters’ thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. J Autism Dev Disord. 1994;24(2):129–54.
Dziobek I, Fleck S, Kalbe E, Rogers K, Hassenstab J, Brand M, et al. Introducing MASC: a movie for the assessment of social cognition. J Autism Dev Disord. 2006;36(5):623–36.
Weightman MJ, Air TM, Baune BT. A review of the role of social cognition in major depressive disorder. Front Psychiatry. 2014;5(NOV):1–13.
Guida M, Caciagli L, Cosottini M, Bonuccelli U, Fornai F, Giorgi FS. Social cognition in idiopathic generalized epilepsies and potential neuroanatomical correlates. Epilepsy Behav. 2019;100:106118.
Richard AE, Scheffer IE, Wilson SJ. Features of the broader autism phenotype in people with epilepsy support shared mechanisms between epilepsy and autism spectrum disorder. Neurosci Biobehav Rev. 2017;75:203–33.
Mirabel H, Guinet V, Voltzenlogel V, Pradier S, Hennion S. Social cognition in epilepsy: state of the art and perspectives. Rev Neurol. 2020;176(6):468–79.
Nasreddine ZS, Phillipe NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for cognitive assessment. J Am Geriatr Soc. 2005;53(4):695–9.
Karmakar A, Dogra AK. Assessment of theory of mind in adults: beyond false belief tasks. Act Nerv Super (Praha). 2019;61(3):142–6.
Slachevsky A, Villalpando JM, Sarazin M, Hahn-Barma V, Pillon B, Dubois B. Frontal assessment battery and differential diagnosis of frontotemporal dementia and Alzheimer disease. Arch Neurol. 2004;61(7):1104–7.
Bujarski KA, Flashman L, Li Z, Tosteson TD, Jobst BC, Thadani VM, et al. Investigating social cognition in epilepsy using a naturalistic task. Epilepsia. 2016;57(9):1515–20.
Acknowledgements
We thank Victoria Reed and Victoria Lyn Ives-Deliperi for their assistance with the current and previous versions of the manuscript. The project was supported by the Swiss Epilepsy Foundation.
Funding
Not applicable (no funding was received).
Author information
Authors and Affiliations
Contributions
ME: conception, design, systematic literature search, study extraction, screening for study eligibility, data extraction, data analysis, data interpretation, drafting; HJ: conception, designing, data interpretation, revision, approval. The author(s) read and approved the final manuscript.
Authors’ information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
HJ is a member of the Editorial Board of Acta Epileptologica. HJ was not involved in the journal’s review of, or decision related to this manuscript. The authors declare that they have no further competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eicher, M., Jokeit, H. Toward social neuropsychology of epilepsy: a meta-analysis on social cognition in epilepsy phenotypes and a critical narrative review on assessment methods. Acta Epileptologica 4, 24 (2022). https://doi.org/10.1186/s42494-022-00093-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42494-022-00093-1