
Abstract
Introduction
Although Rheumatoid Arthritis (RA) extra-articular manifestations (ExtRA) occurrence has been decreasing over time, they are still a major mortality risk factor for patients.
Objective
To determine the prevalence of ExtRA in a large cohort, and its association with demographic and clinical variables.
Method
Cross-sectional and observational study, based on a multi-centric database from a prospective cohort, in which 11 public rheumatology centres enrolled RA patients (1987 ARA or 2010 ACR-EULAR). Data collection began in 08-2015, using a single online electronic medical record. Continuous variables were compared using Mann–Whitney U-test, and Fisher’s exact test or chi-square test, as appropriate, were used for categorical variables. The level of significance was set at 5% (p < 0.05).
Results
1115 patients were included: 89% women, age [mean ± SD] 58.2 ± 11.5 years, disease duration 14.5 ± 12.2 years, positive Rheumatoid Factor (RF, n = 1108) in 77%, positive anti-cyclic citrullinated peptide (ACPA, n = 477) in 78%. Regarding ExtRA, 334 occurrences were registered in 261 patients, resulting in an overall prevalence of 23.4% in the cohort. The comparison among ExtRA and Non-ExtRA groups shows significant higher age (p < 0.001), disease duration (p < 0.001), RF high titers (p = 0.018), Clinical Disease Activity index (CDAI) (p < 0.001), Disease Activity Index 28 (DAS 28) (p < 0.001), and Health Assessment Questionnaire (HAQ) (p < 0.001) in ExtRA group. Treatment with Azathioprine (p = 0.002), Etanercept (p = 0.049) Glucocorticoids (GC) (‘p = 0.002), and non-steroidal anti-inflammatory drugs (NSAIDs) (p < 0.001) were more frequent in ExtRA group.
Conclusions
ExtRA manifestations still show an expressive occurrence that should not be underestimated. Our findings reinforce that long-term seropositive disease, associated with significant disability and persistent inflammatory activity are the key factors related to ExtRA development.
Similar content being viewed by others

Introduction
Rheumatoid arthritis (RA) is a systemic and progressive disease characterized by chronic synovitis that leads to severe functional impairment. Treatment delay often impacts health-related quality of life and morbimortality [1]. Current best practices for the treatment of RA rely on early diagnosis and initiation of a disease-modifying antirheumatic drug (DMARD) until effective suppression of inflammation is achieved [2, 3]. New diagnostic tools and therapeutic advances, aligned with a “treat-to-target” strategy, have been of utmost importance for better patient outcomes [4, 5].
Extra-articular manifestations (ExtRA) are frequent findings in RA, leading to increased morbidity and mortality [6,7,8]. Rheumatoid nodules are the most common extra-articular feature and are present in up to 30% of patients. Sicca syndrome, chronic disease anaemia and pulmonary involvement are relatively common (6 to 10%). They can be present in early stages of the disease [9, 10].
Many ExtRA likely occur due to the complex chronic inflammatory and autoimmune features of RA. Persistent systemic inflammation is a well-known risk factor for ExtRA development [11, 12]. Vasculitis, neuropathy (often vasculitis-associated), serositis, interstitial lung disease, scleritis, glomerulonephritis, and Felty syndrome are often classified as severe ExtRA. These manifestations may share immunological and inflammatory disease mechanisms, although local factors may also influence organ involvement [7, 13]. All RA patients should be screened for risk factors associated with ExtRA to prevent and manage severe complications. Additionally, appropriate treatment is crucial to limit progression towards serious events [11, 12].
The general prevalence reported for ExtRA in previous cohorts varies from 8 to 40% [7]. Most cases occur with persistently high serum titres of inflammatory activity markers [C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)] and the presence of autoantibodies [rheumatoid factor (RF) and anti-cyclic citrullinated-peptide antibodies (ACPA)]. Male sex, habitual smoking, severe joint disease, impaired functional status, and HLA-related shared epitopes have also been reported as related factors [11, 12]. So far, there is no Brazilian cohort evaluating incidence and specific ExtRA local aspects.
Most of the studies that characterise ExtRA were carried out in cohorts of patients with an RA diagnosis prior to the systematic use of the “treat to target” strategy to control the inflammatory symptoms of RA [13]. Although some subsequent studies have shown a decrease in the incidence of ExtRA over time, the real extent of its impact and incidence, particularly in the context of new treatment guidelines, is not well established. In countries where the “treat-to-target” was incorporated later, it is estimated that ExtRA occurs at a significant frequency [10, 14], representing a challenge for the proper management of the patient.
This study aims to comprehensively characterise the prevalence of ExtRA in a sample of Brazilian RA patients and assesses correlated clinical, therapeutic, and demographic characteristics.
Methods
Thirteen public healthcare centres specialising in RA management were selected to represent the five geographic regions in Brazil. Eleven centres from 4 regions enrolled in the program. The recruitment period started on August 12th, 2015, and ended on April 15th, 2016. Patients were followed for ~ 12 months, with systematic data collection at the initial visit (baseline), at the intermediate visit (6 months ± 1 month) and at the final visit (12 months ± 1 month), with additional descriptive reports of any other unscheduled visit.
The inclusion criteria were: (1) fulfilment of the 1987 American Rheumatism Association (ARA) or the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for rheumatoid arthritis [2, 15], (2) age ≥ 18 years, and (3) documented medical history of at least six months of treatment in their healthcare center prior to study enrollment. Erosive disease was defined according to EULAR 2013 recommendation [16]. Patients were excluded if they were unable to reliably report on the self-assessment sections of the data collection instrument. The REAL Study received ethical approval from the Universidade do Estado do Rio de Janeiro (the coordinating centre) Research Ethics Committee (registration number 45781015.8.1001.5259). Each participating site also obtained approval from their respective institution’s ethics committee. All patients consented to participation in the study. The complete study protocol was previously described [17].
The following comorbidities were considered extra-articular manifestations (ExtRA): sicca syndrome, interstitial lung disease, scleritis, episcleritis, pleuritis, pericarditis, glomerulonephritis, peripheral neuropathy, anaemia, cutaneous and systemic vasculitis, and subcutaneous nodules. The criteria for ExtRA definition was based on clinical judgement, similar to previous definitions [13] and are described in detail in Additional file 1: Table S1. According to the domain, they were based on clinical exam (nodules, ocular involvement, vasculitis) laboratory findings (chronic disease’s anaemia, after exclusion of other causes), imaging (pleuritis, pericarditis, interstitial lung disease, systemic vasculitis, visceral rheumatoid nodules) pathology (vasculitis, visceral rheumatoid nodules) and other specific diagnostic methods (such as electroneuromyography for peripheral neuropathy, Schimmer’s test and scintigraphy for sicca syndrome). Only ongoing manifestations were considered.
Statistical analysis
Results are presented as mean (± standard deviation) and number (%) for continuous and categorical variables, respectively. Continuous variables were compared using Mann–Whitney U-test, since most distributions failed in normality tests. For categorical variables, differences were assessed using Fisher’s exact test or chi-square test, as appropriate. A multivariate logistic regression analysis was performed using as dependent variable the presence of extra-articular manifestations, and the variables with p < 0.2 in each univariate analysis as the independent ones.
In all the statistical tests, the level of significance was set at 5% (p < 0.05). Licensed Stata/SE 14 was used as software.
Results
A total of 1115 patients were enrolled in the study. Demographic and clinical data at the time of the initial evaluation are described elsewhere [15]. Approximately 90% were female, with a mean age of 56.7 (22.1–88.8) years and median disease duration of 12.7 (0.7–56.9) years. Most subjects were white (56.8%). Almost 80% of patients belonged to low or low-middle socioeconomic classes.
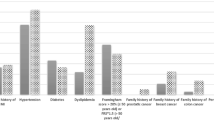
ExtRA occurred in 261 patients (23.4%). As many patients presented more than one ExtRA (Figs. 1 and 2), the total number of events was 334. The most common ExtRA was subcutaneous nodules (n = 92, 35.2% in the ExtRA group and 8% of the total 1,115 patients), followed by anaemia (n = 78, 29.8% in the ExtRA group and 7% of the entire cohort), and sicca syndrome (n = 65, 24.9% in the ExtRA group and 5.8% of the entire cohort). Interstitial lung disease occurred in 45 patients, corresponding to 17.2% of ExtRA patients and 4% of the entire cohort.

ExtRA distribution by site and/or type among 334 occurrences in 261 patients. Graphic shows the absolute number and percentage (n = 1115 patients) from each of the patient cohorts. Additionally, the number of patients presenting with the coexistence of ExtRA is shown in the connecting lines. *SC: subcutaneous, SS: sicca syndrome, ILD: interstitial lung disease

Number of cumulative ExtRA in 261 patients. As shown below, most patients (77%) presented a single ExtRA, while 33% had two or more manifestations
Demographic and clinical data from the ExtRA and non-ExtRA groups are summarized in Table 1. Comparison among the ExtRA and non-ExtRA groups showed significantly higher age (60.4 ± 10.1 vs. 57.5 ± 11.8 years, p = 0.0003), disease duration (17.5 ± 10.3 vs. 13.7 ± 9.1 years, p = 0.0001), Clinical Disease Activity Index (CDAI) (18.2 ± 16 vs. 11.5 ± 10.6, p < 0.0001), Disease Activity Score 28 (DAS 28) (4.3 ± 1.6 vs. 3.4 ± 1.4 p < 0.0001), and Health Assessment Questionnaire-Disability Index (HAQ-DI) (1.15 ± 0.8 vs. 0.87 ± 0.7, p < 0.0001) in the ExtRA group. Additionally, high titres of RF (≥ 3 × the upper limit) were significantly more prevalent in the ExtRA group (62.8% vs. 54.1%, p = 0.018).
Treatment with azathioprine (2.7% vs. 0.4%, p = 0.002), etanercept (8.4% vs. 5%, p = 0.041), glucocorticoids (GC) (52.4% vs. 43%, p = 0.0002), and nonsteroidal anti-inflammatory drugs (NSAIDs) (14.6% vs. 7.4%, p = 0004) were also more frequent in the ExtRA group (Table 2). The multivariate logistic regression showed that the independent factors associated to the presence of extra-articular RA were erosive disease (OR 1.657 [95% CI 1.154–2.380] p = 0.006), longer disease duration (OR 1.097 for each 5 years of disease [95% CI 1.002–1.200] p = 0.044), and higher CDAI (OR 1.026 [95% CI 1.010–1.042] p = 0.001).
Subgroup analyses for special interest manifestations were performed: sicca syndrome, vasculitis/neuropathy, rheumatoid nodules, and interstitial lung disease (ILD). The results were similar to the overall group (Additional file 1: Tables S2–S4), except for patients in the ILD group (Table 3) who presented differences regarding the pharmacological treatment: fewer patients in the ILD group used methotrexate (p = 0.010), whereas more ILD patients used azathioprine (p < 0.001), infliximab (p = 0.010), and GC (p < 0.001). The analysis of the non-ILD manifestations together was more similar to the overall group (Table 4), regarding the influence of age (p = 0.016), disease duration (p < 0.001), erosive disease (< 0.001) and disease activity (< 0.001), use of NSAID (p < 0.001) and glucocorticoids (p = 0.003). These patients also used more etanecerpt (p = 0.027), but not more azathioprine (p = 0.103), with a lower frequency of leflunomide (p = 0.039).
Discussion
In the present cohort, extRA manifestations had a considerable prevalence in RA patients. Persistently active and severe disease with high RF titres and established sequelae are risk factors for extRA. These findings are similar to previously reported data [6, 11,12,13]. However, unlike previous findings, we did not observe a correlation with ACPA positivity, probably due to the test’s unavailability to almost half of the patients studied. Likewise, there was no significant correlation with smoking status, except for rheumatoid nodules [13, 14]. In this specific group, smoking habit (current and ever, summed up) was more prevalent in comparison to the overall ExtRA patients (66.3 vs. 51.7%).
Although smoking is a known risk factor for extra-articular manifestations, the role of active smoking is more pronounced for this outcome than previous smoking, as demonstrated by Turesson [13], who found a relative risk of 1.52 for the development of ExtRA in active smokers at RA diagnosis. The role of ever-smoking (not at RA diagnosis) was not so well defined for ExtRA. In our cohort, the prevalence of ever-smokers was much higher than active smokers (42.1% vs. 9.6% in ExtRA patients), which can partially explain our findings. We did not specify in our questionnaire if smoking habit was present at RA diagnosis, what could be a bias. Additionally, our cohort mainly consists of older patients presenting long-term, RF-positive, erosive disease, and we believe that these other risk factors overcame smoking risk itself.
Regarding pharmacological treatment, the higher use of glucocorticoids in patients with extRA can be explained both by the greater inflammatory activity and severity of joint disease, as well as by the extRA treatment itself. Additionally, the greater use of NSAIDs is also justified by articular activity, chronic pain and damage.
Interestingly, a trend towards greater use of anti-tumour necrosis factor (TNF) drugs in the extRA group was observed, with statistical significance in favour of etanercept. One hypothesis for this finding is disease severity, which requires biological treatment for inflammatory control. In addition, when the cohort was initiated, anti-TNF drugs had a greater availability in Brazil compared to other biologics. Factors that could favour etanercept could include safety concerns, such as the lower risk for certain infections [18] (herpes zoster [19] and tuberculosis [18]) and the shorter half-life, considering the extRA patient’s profile (older, disabled, with more severe disease and more comorbidities).
When we examined the use of conventional synthetic DMARD treatment, there was a greater proportion of patients using azathioprine (AZA) in the extRA group. Presumably, this drug was chosen for extRA control, because the effectiveness of AZA for inflammatory articular activity is limited [20]. Considering the widespread AZA use for RA-ILD in Brazil, a comparison between the non-ILD ExtRA summed up, versus no-ExtRA, failed to show significant difference regarding AZA use, what may imply a preference for AZA in RA-ILD clinical management (influenced also by the drug wide availability in Brazil). On the other hand, a lower LEF use was detected in the non-ILD extRA group, probably because this csDMARD is usually avoided in the presence of neuropathy and vasculitis.
Further subgroup analysis regarding the most frequent and/or clinically significant manifestations (sicca syndrome, subcutaneous nodules, vasculitis) did not reveal differences between the extRA and control groups. However, patients with ILD presented a relevant difference that should be explored: the lower use of MTX.
ILD is a topic of growing interest because it currently represents the second leading cause of death among patients with RA and because of its novel antifibrotic therapeutic effects [21, 22]. The incidence and morbimortality of RA-ILD have grown over the years [22, 23]. Clinically significant ILD occurs in up to 10% of RA cases [23, 24]. In our cohort, ILD occurrence was lower, reported in 4% of the patients. Considering that access to diagnostic tools (such as high-resolution chest tomography) varies significantly between different regions of the country, underdiagnosis and heterogeneous data may explain this finding. Another contributing factor for this scenario is the lack of specific guidelines for ILD detection and treatment in RA patients [25].
We found that the use of MTX was less frequent in patients with ILD in Brazil. This finding is similar to a recent multicentre study [26]. Avoiding MTX in ILD has been a widespread practice for many years in rheumatology, as it is believed that MTX could exacerbate ILD. Currently, this misconception has been elucidated: MTX probably has a protective role against RA-ILD development, either by a direct immunosuppressive effect targeting the lung or by an MTX-driven decrease in systemic inflammation [26].
The REAL study [17], an observational multicentre cohort, has a limitation in its design. All enrolled sites are tertiary centres, presenting a severe disease profile predominance, and probably not fully representative of the broader management of RA across the country. Additionally, the cross-sectional nature of the study design precludes establishing causal association between variables and outcomes.
Conclusion
Our results suggest that extRA is an actual challenge in the management of RA patients in Brazil. Its high prevalence calls attention to the need for further studies, evaluating the potential effect of treatment strategies using longitudinal design. It is possible that early and rigorous medical management with effective therapies could help lower the risk and severity of ExtRA.
Availability of data and materials
All data generated or analysed during this study are included in this published article, as “supplementary materials”.
References
van der Linden MP, Knevel R, Huizinga TW, van der Helm-van Mil AH. Classification of rheumatoid arthritis: comparison of the 1987 American college of rheumatology criteria and the 2010 American college of rheumatology/European league against rheumatism criteria. Arthritis Rheum. 2011;63(1):37–42.
Singh JA, Saag KG, Bridges SL Jr, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26.
Smolen JS, Landewe RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–99.
Smolen JS, Aletaha D, Barton A, Burmester GR, Emery P, Firestein GS, et al. Rheumatoid arthritis. Nat Rev Dis Primers. 2018;4:18001.
Bonfiglioli KR, da Mota LMH, de Medeiros Ribeiro AC, Kakehasi AM, Laurindo IMM, Giorgi RDN, et al. Recommendations of the Brazilian society of rheumatology for the use of JAK inhibitors in the management of rheumatoid arthritis. Adv Rheumatol. 2021;61(1):70.
Myasoedova E, Crowson CS, Turesson C, Gabriel SE, Matteson EL. Incidence of extraarticular rheumatoid arthritis in Olmsted County, Minnesota, in 1995–2007 versus 1985–1994: a population-based study. J Rheumatol. 2011;38(6):983–9.
Turesson C, O’Fallon WM, Crowson CS, Gabriel SE, Matteson EL. Occurrence of extraarticular disease manifestations is associated with excess mortality in a community based cohort of patients with rheumatoid arthritis. J Rheumatol. 2002;29(1):62–7.
Gabriel SE, Crowson CS, Kremers HM, Doran MF, Turesson C, O’Fallon WM, et al. Survival in rheumatoid arthritis: a population-based analysis of trends over 40 years. Arthritis Rheum. 2003;48(1):54–8.
Young A, Koduri G. Extra-articular manifestations and complications of rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2007;21(5):907–27.
Louzada-Junior P. Análise descritiva das características demográficas e clínicas de pacientes com artrite reumatóide no estado de São Paulo. Brasil Revista Brasileira de Reumatologia. 2007;47(2):84–90.
Figus FA, Piga M, Azzolin I, McConnell R, Iagnocco A. Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev. 2021;20(4): 102776.
Conforti A, Di Cola I, Pavlych V, Ruscitti P, Berardicurti O, Ursini F, et al. Beyond the joints, the extra-articular manifestations in rheumatoid arthritis. Autoimmun Rev. 2021;20(2): 102735.
Turesson C, O’Fallon WM, Crowson CS, Gabriel SE, Matteson EL. Extra-articular disease manifestations in rheumatoid arthritis: incidence trends and risk factors over 46 years. Ann Rheum Dis. 2003;62(8):722–7.
Moura MC. Epidemiological profile of patients with extra-articular manifestations of rheumatoid arthritis from the city of Curitiba, South of Brazil. Rev Bras Reumatol. 2012;52(5):679–94.
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–24.
van der Heijde D, van der Helm-van Mil AH, Aletaha D, Bingham CO, Burmester GR, Dougados M, et al. EULAR definition of erosive disease in light of the 2010 ACR/EULAR rheumatoid arthritis classification criteria. Ann Rheum Dis. 2013;72(4):479–81.
da Rocha C-P, Vargas-Santos AB, de Albuquerque CP, Bertolo MB, Junior PL, Giorgi RDN, et al. The REAL study: a nationwide prospective study of rheumatoid arthritis in Brazil. Adv Rheumatol. 2018;58(1):9.
Desai RJ, Thaler KJ, Mahlknecht P, Gartlehner G, McDonagh MS, Mesgarpour B, et al. Comparative risk of harm associated with the use of targeted immunomodulators: a systematic review. Arthritis Care Res. 2016;68(8):1078–88.
Strangfeld A, Listing J, Herzer P, Liebhaber A, Rockwitz K, Richter C, et al. Risk of herpes zoster in patients with rheumatoid arthritis treated with anti-TNF-alpha agents. JAMA. 2009;301(7):737–44.
Choy EH. Two is better than one? Combination therapy in rheumatoid arthritis. Rheumatol. 2004;43(10):1205–7.
Wells AU, Flaherty KR, Brown KK, Inoue Y, Devaraj A, Richeldi L, et al. Nintedanib in patients with progressive fibrosing interstitial lung diseases-subgroup analyses by interstitial lung disease diagnosis in the INBUILD trial: a randomised, double-blind, placebo-controlled, parallel-group trial. Lancet Respir Med. 2020;8(5):453–60.
Hyldgaard C, Hilberg O, Pedersen AB, Ulrichsen SP, Lokke A, Bendstrup E, et al. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: comorbidity and mortality. Ann Rheum Dis. 2017;76(10):1700–6.
Olson AL, Swigris JJ, Sprunger DB, Fischer A, Fernandez-Perez ER, Solomon J, et al. Rheumatoid arthritis-interstitial lung disease-associated mortality. Am J Respir Crit Care Med. 2011;183(3):372–8.
Kawano-Dourado LDT, Bonfiglioli K, et al. Baseline characteristics and progression of a spectrum of interstitial lung abnormalities and disease in rheumatoid arthritis. Chest. 2020. https://doi.org/10.1016/j.chest.2020.04.061.
Kawano-Dourado L, Lee JS. Management of connective tissue disease-associated interstitial lung disease. Clin Chest Med. 2021;42(2):295–310.
Juge PA, Lee JS, Lau J, Kawano-Dourado L, Rojas Serrano J, Sebastiani M, et al. Methotrexate and rheumatoid arthritis associated interstitial lung disease. Eur Respir J. 2021;57(2).
Acknowledgements
This study was supported by the Brazilian Society of Rheumatology. The funding body had no role in study design, data collection, analysis, and interpretation or in manuscript writing.
Funding
Brazilian Society of Rheumatology. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the acquisition of data, have been involved in drafting the manuscript or revising it critically for important intellectual content, gave final approval of the version to be published and have participated sufficiently in the work to take public responsibility for appropriate portions of the content; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The REAL Study received ethical approval from the Universidade do Estado do Rio de Janeiro (the coordinating centre) Research Ethics Committee (registration number 45781015.8.1001.5259). Each participating site also obtained approval from their respective institution’s ethics committee. All patients consented to participation in the study.
Consent for publication
All authors have read and approved the final version of this manuscript.
Competing interests
ACMR: Personal fees and/or nonfinancial support from Janssen, Pfizer, and AstraZeneca. AP: Personal fees and/or nonfinancial support from Pfizer, AbbVie, UCB, BMS, Janssen, Lilly, Boehringer-Ingelheim. APC: No conflicts declared. APMG: Assistance for participation in events: Pfizer; CVB: personal or institutional support from AbbVie, Janssen and Pfizer; has delivered speeches at events related to this work and sponsored by AbbVie, Janssen, Pfizer, Bristol-Myers Squibb and UCB. DSD: Personal fees and/or non-financial support from Pfizer, UCB, AbbVie. GRCP: No conflicts declared. HCS: No conflicts declared. IAP: personal fee for lectures at AbbVie, Janssen, Pfizer and Roche; has delivered speeches at events related to this work and sponsored by AbbVie, Boehringer- Ingelheim, Janssen, Pfizer, Roche, Sandoz, Lilly and UCB. KRB: personal fees and/or nonfinancial support from Pfizer, AbbVie, Roche, Novartis, Boehringer-Ingelheim. LRP: No conflicts declared. LMHM: personal or institutional support from AbbVie, Janssen, Pfizer and Roche; has delivered speeches at events related to this work and sponsored by AbbVie, Boehringer-Ingelheim, Janssen, Pfizer, Roche, Sandoz, Lilly and UCB. MFBRG: personal fees and/or non-financial support from AbbVie, Bristol-Myers-Squibb, Janssen, Novartis, Pfizer, Roche and UCB. MFLCS: No conflicts declared. PL-J: Sponsored by Bristol-Myers Squibb, UCB, Pfizer, board Participation: Pfizer. RDNG: consulting fees, speaking fees, and support for international congresses from Roche, Pfizer, Bristol-Myers-Squibb, UCB Pharma, Eli-Lilly, AbbVie, Abbott, and EMS. SCR: Consulting fees, speaking fees, and support for clinical trials from AbbVie, Amgen, Bristol-Myers-Squibb, Lilly, Pfizer, and Roche.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Criteria for inclusion as extra-articular manifestations of RA. Table S2. Subcutaneous nodules patients: clinical data and current pharmacological treatment (compared with no-extra patients). Table S3. Secondary SS patients: clinical data and current pharmacological treatment (compared with no-extra patients). Table S4. Clinical data and current pharmacological treatment (compared with no-extra patients).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bonfiglioli, K.R., de Medeiros Ribeiro, A.C., Carnieletto, A.P. et al. Extra-articular manifestations of rheumatoid arthritis remain a major challenge: data from a large, multi-centric cohort. Adv Rheumatol 63, 34 (2023). https://doi.org/10.1186/s42358-023-00318-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42358-023-00318-y