
Abstract
Background
Sjögren Syndrome (SS) is a systemic autoimmune disease with a wide spectrum of manifestations that can lead to misdiagnosis. This study describes and compares demographic, clinical, serological, and histopathological data from subjects with SS and non-Sjögren Syndrome (NSS). It also details specific features within the primary SS (pSS) and secondary SS (sSS) groups identifying sub-groups.
Methods
The sample included individuals referred to an academic medical center in Brazil for investigation of SS from 2012 to 2020. Patients were retrospectively classified as primary SS (pSS), secondary SS (sSS), or NSS, based on the American-European Consensus Group criteria (AECG-2002), after multi-professional clinical and laboratory evaluation.
Results
A total of 676 individuals were screened and 510 (75.4%) completed the assessments; 198 patients were classified as pSS, 149 as sSS, and 163 as NSS. Symptoms and glandular dysfunction tests were similar in the groups. Concerning pSS, extraglandular manifestations were present in 59% of patients; the elderly had more dry symptoms and peripheral neurological disorders; and 2.5% developed non-Hodgkin lymphoma. In sSS, each overlap promoted distinct clinical and laboratory variants. Several alternative diagnoses were identified as a cause of sicca complex in NSS group.
Conclusions
The diagnosis of SS remains a challenge behind dryness. Up to 31% of the suspected cases had other conditions associated to the symptoms. Histopathological analysis of LSG and SSa determined the diagnostic. Aging in pSS and overlap disease in sSS were responsible for distinct phenotypes and characteristic sub-groups in SS.
Similar content being viewed by others


Introduction
Sjögren syndrome (SS) is an autoimmune lymphocytic disease characterized by inflammation and hypofunction of exocrine glands that causes dryness of the mouth and eyes, and multi-organ manifestations [1,2,3,4]. There is a broad range of clinical presentations, from mild glandular involvement to severe systemic conditions, hence the challenges of establishing the diagnosis [4,5,6]. Discernment of numerous other causes of xerostomia and xerophthalmia, and identification of complex systemic diseases require careful multidisciplinary assessment and patient follow-up. The syndrome has a low rate of diagnosis since dry complaints are not systematically evaluated [5]. It is also misdiagnosed, even in experienced rheumatology departments, as patients may carry clinical and serological abnormalities that overlap with other diseases [5]. Almost a century after its description, the physiopathology and outcomes of SS are still unclear and issues such as the role of estrogen exposure, microchimerism, and interferon signature are yet to be clarified [7,8,9]. Genetic and environmental factors have been proposed in the etiology of SS and some biomarkers and features have been associated with the prognosis [10,11,12,13,14].
The use of different criteria, the lack of a multidisciplinary team, and the limited access to laboratory tests can reduce the validity of SS diagnosis and explain the variable prevalence of the disease worldwide. In addition to not differentiating data between primary (pSS) and secondary (sSS) forms of SS, in some cases. A previous Brazilian study revealed a prevalence of 0.17% [15], comparable to other series of pSS around the world [3, 16,17,18,19]. The 2002 American European Consensus Group (AECG) criteria, the 2016 American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) classification criteria have been useful in clinical practice and research, allowing comparisons between studies [20,21,22].
To measure symptoms intensity and systemic activity in pSS patients, the EULAR developed tools that are suitable for grading disease severity and treatment response [23]. The EULAR SS Patient-Reported Index (ESSPRI) assesses the level of dryness, pain and fatigue complaints, and the EULAR SS Disease Activity Index (ESSDAI) assesses activity across multiples clinical and biological domains [24,25,26,27,28,29,30,31]. Multicenter registries have reported an association between higher ESSDAI scores and poorer outcomes [26, 32]. Not least, ESSDAI should be used for the diagnosis of pSS through the active involvement of specific organ systems predicted therein, and even in the absence of dry symptoms, based on the 2016 criteria [22].
Secondary SS has been less researched and is often excluded from clinical trials. The associated rheumatic diseases (e.g., systemic lupus erythematosus—SLE; rheumatoid arthritis—RA; and systemic sclerosis—SSc) essentially affect clinical presentation, autoantibody profile, salivary gland (SG) histology, and therapeutic approaches in sSS [18, 33, 34]. The co-occurrence of SS, in turn, alters the severity and the prognosis of the central disease [18, 33, 35,36,37].
Of note, sicca symptoms are frequently reported in the general population and may be caused by several factors, including medications (antihistamines, antidepressants, diuretics, and anticholinergic drugs), environmental conditions (pollution, smoke, dry air), ocular trauma (nerve damage, contact lens, laser eye surgery), chronic topical exposure to irritants such as benzalkonium chloride or systemic, menopause and aging [14, 15, 20, 21, 38,39,40,41,42]. Patients with sicca symptoms that do not meet minimum criteria for SS, as well as those with sicca complex under exclusion criteria (sarcoidosis, amyloidosis, graft versus host disease—GVHD, acquired immunodeficiency syndrome—AIDS, IgG4 related disease, and Hepatitis C), establish a large and heterogeneous group of non-Sjögren Syndrome (NSS).
Considering this context, the present study proposes a comparative description of patients underwent to a comprehensive clinical and laboratory examination for SS, and subsequent classification as pSS, sSS, or NSS groups. In parallel, it intends to detail specific characteristics within SS; to evaluate the most relevant elements to achieve the final diagnosis; and to describe conditions or diseases composing the group of alternative diagnosis (NSS).
Materials and methods
Study design and patients
This was a descriptive study of patients referred for diagnostic evaluation and treatment of SS to Ribeirão Preto Clinics Hospital, Brazil, consecutively selected from January 2012 to November 2020. The inclusion criteria were adult patients (≥ 18 years old) presenting with complaints of sicca complex, and/or any other symptom and sign suggestive of SS. Patients were excluded if they did not complete the minimal investigation requirements to distinguish the pSS, sSS, and NSS groups. The study was approved by the institutional review board (CAAE #: 37688914.2.0000.5440), and all patients provided written informed consent. An electronic database was created for the registration of clinical and laboratory data by members of the study group, housed in the institutional account of the Research Electronic Data Capture (RED Cap).
Clinical and laboratory variables
Recorded data included medical history, demographics, ocular examination, and measurement of unstimulated whole salivary flow rate (UWSF, collected for 15 min and expressed as mL/min). The ocular evaluation consisted of the Ocular Surface Disease Index questionnaire (OSDI), corneal fluorescein staining score (CFS), tear film break-up time (TFBUT) measured in seconds, and the Schirmer’s test (ST). The worst values comparing the right and left sides for eye tests were used for analysis between the groups. Laboratory tests included detection of the antinuclear antibody (ANA), rheumatoid factor (RF), anti-Ro (SSa) and anti-La (SSb), cryoglobulinemia, serum levels of complement factors (C3 and C4), lactate-dehydrogenase (LDH), β2-microglobulin (B2M), gammaglobulin level (γ fraction), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and virus serology (HIV, and hepatitis B and C). A labial salivary gland (LSG) biopsy was obtained for the histological analysis and focus score, as previously described [43]. Disease activity was defined as “moderate” if ESSDAI ≥ 5 or “severe” if ESSDAI > 15 [23].
Study groups
Patients were classified as pSS according to the AECG criteria or as sSS if there was any other concomitant inflammatory rheumatic disease [20]. The NSS diagnosis was assigned to patients who did not meet the minimum diagnostic criteria for SS or those who had any of the conditions listed as exclusion criteria. Dry eye and dry mouth symptoms were defined based on positive answers to the first two items of the AECG criteria, respectively [20]. Dry eye disease (DED) was defined as a positive dry eye symptom or an OSDI score > 12, and one positive test (ST ≤ 5 mm, RB or CFS score > 3). Dry mouth disease (DMD) was defined as the presence of dry mouth symptoms and a UWSFR ≤ 0.1 mL/min. The presence of coexisting illnesses and habits, and exposure to therapeutic regimens, were also investigated.
Statistical analysis
Demographic and clinical data were evaluated using descriptive statistics. Data were checked for normality using the Kolmogorov–Smirnov test. Categorical variables were expressed as frequencies and percentages, and continuous variables as means and standard deviation or median and interquartile ranges, as appropriate. The comparison of continuous data between the pSS, sSS, and NSS groups was performed using the Kruskal–Wallis test or ANOVA for non-parametric and parametric data, respectively. Whenever differences were observed Dunn’s and Bonferroni’s post-hoc tests were applied, respectively. Correlations between demographic, clinical, and laboratory data were determined using the Spearman test. The comparisons of categorical variables among the three groups (pSS, sSS and NSS) and between the SSa-positive versus SSa-negative pSS groups were performed with the chi-square test, relative risk (RR) and confidence interval 95% (CI 95%) were also calculated. False Discovery Rate method was proposed to adjust the p-values and balance multiple comparisons. Statistical significance was set at p-value < 0.05. The analysis was performed using GraphPad Prism 5.0 software (San Diego, CA).
Results
Patients
A total of 676 patients were included and 510 (75.4%) completed the study; 347 (68.2%) were diagnosed with SS, of which 198 (57%) with pSS and 149 patients (43%) with sSS. One hundred sixty-three (31.8% of the 510 patients) did not match the AECG criteria for SS; therefore, these patients were classified as NSS. In the whole study population (n = 510), 92.3% were women, and the mean age was 53.9 ± 14.3 years (Table 1). The most common comorbidities were systemic arterial hypertension, obesity, dyslipidemia, diffuse pain associated with fibromyalgia or psychiatric disorders, type 2 diabetes mellitus and hypothyroidism with no differences between the groups. The smoking (current or past) rate was 24.7% in SS patients versus 40.5% in NSS patients. Two-thirds of all patients were sedentary or insufficiently active.
Primary SS
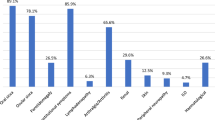
In the pSS group (n = 198), 95.9% were women, 35% retired worker or pensioner, 28.5% employed or self-employed, 28.5% homemaker and 6.5% unemployed. The mean age was 44.3 ± 14.8 years at the onset of the disease and 54.2 ± 14.3 years at the time of enrollment in the study. The interval between the initial symptoms and diagnosis was 4.6 ± 4.4 years. Thirty percent of patients had extra glandular manifestations (EGM) at the initial stage of the disease, either preceding or concomitant with sicca symptoms, and 117 patients (59%) presented some EGM throughout the disease. Swelling of the parotid, salivary and/or lacrimal glands was identified in 28.8% of the 198 pSS patients, arthritis in 23.2%, Raynaud´s phenomenon in 18.1%, fever and/or involuntary weight loss were present in 18%, cytopenia in 14.1%, cutaneous vasculitis in 12.6%, lymphadenopathy in 11.6%, peripheral neuropathy in 11.6%, interstitial lung disease in 10.1%, central nervous system disorders in 5% and renal involvement in 4%. The ESSDAI score at the onset of the disease was 7 (IQR = 3–14), indicating moderately active disease. The initial ESSPRI was 6 (IQR = 4–8).
After the diagnosis, 2.5% (5/198) of pSS patients developed non-Hodgkin lymphoma (NHL): four cases of B-cell extranodal marginal zone of mucosa-associated lymphoid tissue (MALT lymphoma of the parotid, submandibular salivary gland, and lachrymal gland) and one case of diffuse large B-cell lymphoma (cervical lymph nodes). One case (0.5%) developed multiple myeloma (MM). All patients were female, mean age of 69.4 ± 18.4 years, and median disease duration of 5 (IQR 4–7) years. Only 20% were positive anti-SSa cases. Treatment regimens with rituximab combined or not with corticosteroids, alkylating agents, or CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) to NHL were proposed.
A high rate of positive SSa (79%), SSb (43.5%), ANA (68.4%), and RF (41.7%), and a high percentage of patients with abnormal microscopic features of LSG tissue (91.4%) were revealed (Table 2). Further irregular immunological markers were detected, such as antiphospholipid antibodies (APL) (14%), anti-citrullinated protein antibodies (7.5%), anti-neutrophil cytoplasmic antibodies (pANCA) (5.3%), anti-ribonucleoprotein (anti-RNP) (5.1%), anticentromere antibodies (2.7%), anti-DNA (1.2%) and anti-Sm (1.2%), in the absence of another autoimmune disease. Of note, there were among these pSS patients, 18 cases of Hashimoto´s thyroiditis, 8 cases of neuromyelitis optica spectrum disorder, 6 cases of chronic liver disease (3 patients with biliary cholangitis and 3 patients with autoimmune hepatitis), 3 cases of atrophic gastritis, and 1 case of positive anti-acetylcholine receptor antibody myasthenia gravis. Five of the 198 (2.7%) pSS patients were current smokers.
Correlation among clinical and laboratory data in the pSS group
Some weak correlations, mostly concerning the effects of age on dryness and B cell activation parameters, were established (Table 3). Age was positively correlated with keratitis (CFS) and inversely correlated with blood levels of SSa and SSb, and the degree of CFS was inversely correlated with ST and TFBUT. B2M was correlated with higher disease activity index (ESSDAI), keratitis and other inflammatory markers (Table 3). Cryoglobulinemia was investigated in 162 of 198 pSS patients (81.8%) and detected in 6 (3.7%) of them. These 6 patients had major EGM as arthritis, cutaneous vasculitis, optic neuritis, mononeuritis multiplex, and two developed lymphoma.
Effect of aging on clinical and laboratory parameters in the pSS group
The pSS group showed differences in some clinical and laboratory parameters based on the cut-off points of 65 years (older patients), 35–64 years, and younger than 35 years. Dry eye symptom based on OSDI score > 12 was more frequently observed in the pSS subgroup ≥ 65 years (p = 0.014). Schirmer’s test values (mm) were higher in patients under 35 years (p = 0.035). Dry mouth symptom was correspondingly less frequent in this group < 35 years (p = 0.008). However, the frequencies of altered TFBUT, ST, CFS and UWSF tests were not able to distinguish the subgroups (Table 4).
Subjects in the three age groups were similar in terms of proportion of men, obesity rates, degree of disease activity (ESSDAI), and clinical presentation considering the ESSDAI domains. Exception for a higher occurrence of peripheral nervous system diseases (21%, 11%, 10%, p = 0.039, RR = 2.03, 95% CI = 1.09–3.80) in patients ≥ 65 years and a higher occurrence of glandular enlargement and lymphadenopathy (35%, 29%, 63%, p = 0.001, RR = 3.35, 95% CI 1.38–8.09 and 14%, 8%, 35%, p = 0.002, RR = 3.86, 95% CI 1.72–8.67) in those under 35 years.
Positive SSa and SSb were more frequent among the younger patients (67%, 81%, 90% and 31%, 44%, 67%, p = 0.031 and p = 0.014, respectively). FS, ANA and RF levels were not statistically different between the age groups in pSS, nor was any other laboratory parameter, such as ESR, reactive-C protein, B2M, lactate dehydrogenase, and gammaglobulin levels, cryoglobulinemia, hypocomplementemia, or cytopenia as well (Table 4).
Association of SSa positivity with other laboratory parameters
The analysis of SSa-positive and SSa-negative patients in the pSS group showed younger age and higher disease activity index in SSa-positive patients (p = 0.012 and p = 0.020, respectively). SSa-positive pSS patients had higher positivity for ANA (p < 0.0001, RR = 2.1, 95% CI 1.4–3.2), for RF (p < 0.0001, RR = 3.7, 95% CI 1.6–8.5), and hypergammaglobulinemia (p < 0.0001, RR = 3.72, 95% CI 1.62–8.57). The other parameters studied were not statistically different between the two subgroups (Table 5).
Almost all patients tested for SSa have also been tested for SSb. The percentages of positive SSb tests were lower in all groups, as compared with SSa (Table 1); 34% of pSS patients and 32% of the sSS patients were positive only for SSa but not for SSb, and no patient reacted to SSb alone.
Focus score in the pSS group
A high number of pSS patients (176/198; 89%) underwent LSG biopsies, and 91.4% (161/176) of them presented lymphocytic sialadenitis. Comparing the distribution of patients according to the intensity of LSG inflammation, based on the foci counts, a FS of 4 was more frequently observed in pSS than sSS or NSS patients (Table 2). There was no significant association between the degree of inflammation (FS) and salivary gland dysfunction (UWSF).
Secondary SS
Among the 149 patients identified with sSS, 73 (49%) had systemic lupus erythematosus, 36 (24%) had rheumatoid arthritis, 21 (14%) had systemic sclerosis and 19 (13%) had other overlapping conditions. Every association in sSS exposed distinct clinical variants. Patients with sSS constituted a heterogeneous group, although indistinguishable from pSS in terms of dry complaints and functional tests (Table 1). The analysis in clusters, however, emphasized differences in focus score and serological features between SS secondary to SLE (sSS-SLE), RA (sSS-RA), SSc (sSS-SSc), and other overlaps (Table 2 and Additional file 1: Table S1). Based on focus score > 1, the highest rates of inflammation were in the sSS-SSc group and the lowest in the sSS- SLE group. The SLE-sSS patients were younger and had higher positivity for SSb. The sSS-RA group had lower positivity for SSa and ANA, and higher positivity for RF.
NSS group
Diagnosis of NSS (n = 163) was attributed to 139 patients who did not meet the minimum diagnostic criteria (NSS-NM) and 24 patients with any of the conditions listed as exclusion criteria for pSS (NSS-EC). Among the NSS-EC patients, there were cases of viral infections (HIV, HTLV-I and HCV), IgG4-related disease (n = 7), hematological neoplasia (n = 5), GVHD (n = 2), and sarcoidosis (n = 2). Symptoms in NSS-NM subgroup were attributed to several ocular, oral, or salivary gland conditions, systemic or psychiatric disorders, climacteric syndrome, and exposure to medications or environmental conditions, which composed an extensive list of differential diagnoses (Additional file 1). Comparing the two subgroups, we realized some differences. Patients with any of the exclusion conditions (NSS-EC) were older, and had a higher frequency of focus score ≥ 1 (43.7 versus 13.5%), SSa (27.3 versus 7%) and cryoglobulinemia (33 versus 2.1%) than NSS-NM, as a result of the underlying disease producing tissue damage and immunological deviations. The statistical analysis showed differences in NSS patients compared to pSS for the intensity of LSG inflammation, based specifically on the foci counts (Table 2).
Comparative description of pSS, sSS and NSS patients
Mean age and sex were not statistically different between pSS, sSS and NSS patients. The presence of dry eye and dry mouth symptoms, based on positive answers to the AECG criteria or OSDI questionnaire score, was similar among them, as well (Table 1).
The percentage of patients with CFS ≥ 3 and a ST ≤ 5 mm was lower in the NSS group, while the mean values of the ST and the TFBUT were comparable among the three groups. Although no difference was noted in the percentage of patients with reduced UWSF, its values were lower in the pSS and sSS groups than in the NSS group (Table 1). In summary, oral and ocular symptoms and the functional tests had a low ability to distinguish between SS and NSS patients and slightly affected classification performance.
By contrast, SSa and FS ≥ 1 were determinants for the diagnosis of SS. The logistic adjustment confirms the strength of these variables and reinforces the usefulness of autoantibodies and biopsy (FS, SSa, SSb, and ANA) in distinguishing SS and NSS. The percentages of patients with positive SSa, SSb, RF and ANA were higher in SS subjects (p < 0.0001) (Table 1). Higher levels of SSa, SSb, B2M and gammaglobulin were observed in the pSS and sSS groups than in the NSS group (p < 0.0001, p < 0.0001, p < 0.001 and p < 0.001, respectively). We detected a higher percentage of focus score ≥ 1 in SS patients (91.4% and 71.8%, for pSS and sSS, respectively) than in NSS patients. However, 17.5% of NSS patients who underwent a LSG biopsy also had a FS ≥ 1 (Table 2).
Discussion
This study summarizes the clinical and laboratory profile of a well-characterized sample of SS patients and evaluates the most relevant elements to achieve the diagnosis, emphasizing that a comprehensive investigation and follow-up of suspected subjects may reveal several clusters. Age and sex distributions were similar to those described in studies performed in other countries, and some differences may be explained by geographic, environmental and ethnic heterogeneity of the Brazilian population [17, 44,45,46]. Our findings confirm the predominance of white female patients in the mid-forties in pSS [27]. The multidisciplinary analysis and long follow-up allowed the classification of SS patients into subgroups (pSS and sSS) and the identification of several differential conditions that occasionally lead to misdiagnosis (NSS).
The signs and symptoms of the ocular and oral disease were similar among patients who completed the assessments. Considering the AECG criteria, only half of the patients in the SS group presented abnormal ocular tests (i.e.; ST and CFS). No single functional examination of DED or UWSF rate was able to distinguish SS from NSS and revealed a low positive predictive value to discriminate them, emphasizing that a combination of tests is appropriate for the diagnosis [47]. The difficulty of carrying them out and the small achievement rate reported in several studies reinforce the need for a multidisciplinary approach. In addition, the slight discriminative power of the clinical parameters supports that testing for SSa and the LSG biopsy for focus score are key elements in the SS diagnostic criteria [20, 22].
Recent studies have confirmed our finding that SSa is more relevant than SSb as a diagnostic marker for SS, and that SSb positivity does not affect its classification performance [48, 49]. Nevertheless, SSb is associated with particular manifestations and appears to be a sign of increased risk of B-cell expansion, and, like SSa, SSb is associated with younger age and hypocomplementemia [48, 49]. Other relevant laboratory exams observed were focus score, B2M, hypocomplementemia, and hypergammaglobulinemia. Although not specific, changes in biomarkers' levels throughout the treatment may be used to evaluate the progression of the disease, survival rates, and EGM and lymphoma development as previously demonstrated in the literature [50,51,52].
The occurrence of some clinical manifestations (such as fever, arthritis, skin lesions, neuropathy and Raynaud's phenomenon) as well as some autoantibodies (such as ANA, RF and APL) were frequent in pSS and can lead to a prior incorrect diagnosis. Thus, it becomes relatively common for pSS patients to receive suspicion and previous treatment for RA, SLE, and even SSc [6, 53, 54]. This supports de usefulness of ESSDAI as a diagnostic tool in addition to measuring disease index. ANA was also positive in some patients in the NSS group, endorsing its restricted specificity [46, 49]. Likewise, ANA positivity agreed with SSa but not with DES, DMS, ST, or sialography, suggesting it is an early, although weak, predictive marker of pSS [55, 56].
In young patients, features of pSS are usually different from those in old patients [57, 58]. Dry symptoms and exocrine gland dysfunction were more frequent in the older pSS group, and lymphadenopathy, glandular enlargement and positive laboratory findings were more frequent in the younger group. An exocrine and hormonal deterioration and an age-associated low-grade inflammation in the elderly may explain these aspects [59,60,61]. Moreover, the rate of EGM (59%) in our pSS subjects, which sometimes preceded the dry symptoms (30%), was remarkable, a fact that may delay the diagnosis. The median ESSDAI score in our study indicates moderately active disease, but with a poor association between complaints (ESSPRI) and biochemical data (LDH, ESR, CRP). It suggests that the diagnosis of pSS in patients with systemic manifestations should be considered even with disconnected dryness, and points to the heterogeneity of SS phenotypes [62, 63].
Like other systemic autoimmune diseases, SS exhibits a diverse spectrum of clinical and molecular phenotypes to be explored. Type-I- and type-II-interferon signaling [9, 64] lymphoid and myeloid lineage transcripts, the kynurenine metabolic pathway [61], and cytokines from the acute-phase response of inflammation seem to be implicated [65]. The combined use of epigenetics and genomics to the classical serological and clinical parameters would allow better grouping of patients according to the expression of cytokines, biomarkers, and different patterns of immune dysregulation, and could help in the differentiation from other diseases [34, 66].
Regardless of the university hospital selection bias, the NSS group was large and showed a low degree of glandular inflammation and reactive autoantibodies. The causes of sicca included a range of medications and clinical, psychiatric, oral and ophthalmologic disorders. NSS individuals with underlying diseases that met exclusion criteria revealed an inflammatory profile similar to SS and diagnostic confounder [67]. Neither symptoms nor functional parameters were capable of distinguishing SS from NSS patients, which was achieved by a combination of tests that included LSG histopathology, SSa and laboratory. Hypergammaglobulinemia, ANA, and hypocomplementemia are feasible prognostic factors for the progression of NSS to SS [67], and atypical autoantibodies in pSS can be useful markers to recognize patients at risk for developing severe extra glandular manifestations, polyautoimmunity and overlapping diseases [51, 64].
A notable strength of this study was the high rate of diagnostic completion with comprehensive interdisciplinary and laboratory assessments that minimized misclassification [44, 45]. One possible criticism was the use of the AECG criteria for SS since the study started in 2012. However, the agreement between the 2002 AECG and the 2016 ACR-EULAR criteria is high [68].
Conclusion
Diagnosis of SS remains a challenge, as many suspected cases have other diseases or conditions simulating signs and symptoms of SS. This study describes SS and NSS and indicates the importance of laboratory diagnosis, especially SSa and LSG biopsy. Aging and markers of B cells activation identified phenotypic sub-groups among pSS patients; the overlap disease (including SLE, RA, and SSc) led to distinct features in sSS. Among the NSS, when the diagnosis was determined by the exclusion criteria versus lack of the minimal criteria for SS distinct sub-groups were also identified. Follow-up improves the identification of phenotypic subgroups, prognostic markers, and the development of malignancy or associated rheumatic disease.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its Additional file 1].
References
Kassan SS, Moutsopoulos HM. Clinical manifestations and early diagnosis of Sjogren syndrome. Arch Intern Med. 2004;164(12):1275–84.
Daniels TE, Whitcher JP. Association of patterns of labial salivary gland inflammation with keratoconjunctivitis sicca. Analysis of 618 patients with suspected Sjogren’s syndrome. Arthritis Rheum. 1994;37(6):869–77.
Birlik M, Akar S, Gurler O, Sari I, Birlik B, Sarioglu S, et al. Prevalence of primary Sjogren’s syndrome in Turkey: a population-based epidemiological study. Int J Clin Pract. 2009;63(6):954–61.
Qin B, Wang J, Yang Z, Yang M, Ma N, Huang F, et al. Epidemiology of primary Sjogren’s syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(11):1983–9.
Ramos-Casals M, Brito-Zeron P, Siso-Almirall A, Bosch X. Primary Sjogren syndrome. BMJ. 2012;344:e3821.
Rasmussen A, Radfar L, Lewis D, Grundahl K, Stone DU, Kaufman CE, et al. Previous diagnosis of Sjogren’s syndrome as rheumatoid arthritis or systemic lupus erythematosus. Rheumatology. 2016;55(7):1195–201 (Oxford).
McCoy SS, Sampene E, Baer AN. Association of Sjogren’s syndrome with reduced lifetime sex hormone exposure: a case-control study. Arthritis Care Res. 2020;72(9):1315–22 (Hoboken).
Kuroki M, Okayama A, Nakamura S, Sasaki T, Murai K, Shiba R, et al. Detection of maternal-fetal microchimerism in the inflammatory lesions of patients with Sjogren’s syndrome. Ann Rheum Dis. 2002;61(12):1041–6.
Bodewes ILA, Al-Ali S, van Helden-Meeuwsen CG, Maria NI, Tarn J, Lendrem DW, et al. Systemic interferon type I and type II signatures in primary Sjogren’s syndrome reveal differences in biological disease activity. Rheumatology. 2018;57(5):921–30 (Oxford).
Murube J. Primary and secondary Sjogren-Jones syndromes-historical evolution. Ocul Surf. 2011;9(1):13–6.
Konsta OD, Thabet Y, Le Dantec C, Brooks WH, Tzioufas AG, Pers JO, et al. The contribution of epigenetics in Sjogren’s Syndrome. Front Genet. 2014;5:71.
Chao WC, Lin CH, Liao TL, Chen YM, Chen DY, Chen HH. Association between a history of mycobacterial infection and the risk of newly diagnosed Sjogren’s syndrome: a nationwide, population-based case-control study. PLoS ONE. 2017;12(5):e0176549.
Weller ML, Gardener MR, Bogus ZC, Smith MA, Astorri E, Michael DG, et al. Hepatitis delta virus detected in salivary glands of Sjogren’s syndrome patients and recapitulates a Sjogren’s syndrome-like phenotype in vivo. Pathog Immun. 2016;1(1):12–40.
Venables PJ. Sjögren’s syndrome. Best Pract Res Clin Rheumatol. 2004;18(3):313–29.
Valim V, Zandonade E, Pereira AM, de Brito Filho OH, Serrano EV, Musso C, et al. Primary Sjogren’s syndrome prevalence in a major metropolitan area in Brazil. Rev Bras Reumatol. 2013;53(1):24–34.
Kim HJ, Kim KH, Hann HJ, Han S, Kim Y, Lee SH, et al. Incidence, mortality, and causes of death in physician-diagnosed primary Sjogren’s syndrome in Korea: a nationwide, population-based study. Semin Arthritis Rheum. 2017;47(2):222–7.
Alamanos Y, Tsifetaki N, Voulgari PV, Venetsanopoulou AI, Siozos C, Drosos AA. Epidemiology of primary Sjogren’s syndrome in north-west Greece, 1982–2003. Rheumatology. 2006;45(2):187–91 (Oxford).
Patel R, Shahane A. The epidemiology of Sjogren’s syndrome. Clin Epidemiol. 2014;6:247–55.
Maciel G, Crowson CS, Matteson EL, Cornec D. Prevalence of primary Sjogren’s syndrome in a population-based cohort in the United States. Arthritis Care Res. 2016;69(10):1612–6 (Hoboken).
Vitali C, Bombardieri S, Jonsson R, Moutsopoulos H, Alexander E, Carsons S, et al. Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European consensus group. Ann Rheum Dis. 2002;61(6):554–8.
Brito-Zeron P, Theander E, Baldini C, Seror R, Retamozo S, Quartuccio L, et al. Early diagnosis of primary Sjogren’s syndrome: EULAR-SS task force clinical recommendations. Expert Rev Clin Immunol. 2016;12(2):137–56.
Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American college of rheumatology/European league against rheumatism classification criteria for primary Sjogren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis. 2017;76(1):9–16.
Seror R, Bootsma H, Saraux A, Bowman SJ, Theander E, Brun JG, et al. Defining disease activity states and clinically meaningful improvement in primary Sjogren’s syndrome with EULAR primary Sjogren’s syndrome disease activity (ESSDAI) and patient-reported indexes (ESSPRI). Ann Rheum Dis. 2016;75(2):382–9.
Seror R, Gottenberg JE, Devauchelle-Pensec V, Dubost JJ, Le Guern V, Hayem G, et al. European league against rheumatism Sjogren’s syndrome disease activity index and European league against rheumatism Sjogren’s syndrome patient-reported index: a complete picture of primary Sjogren’s syndrome patients. Arthritis Care Res. 2013;65(8):1358–64 (Hoboken).
Seror R, Ravaud P, Bowman SJ, Baron G, Tzioufas A, Theander E, et al. EULAR Sjogren’s syndrome disease activity index: development of a consensus systemic disease activity index for primary Sjogren’s syndrome. Ann Rheum Dis. 2010;69(6):1103–9.
Brito-Zeron P, Kostov B, Solans R, Fraile G, Suarez-Cuervo C, Casanovas A, et al. Systemic activity and mortality in primary Sjogren syndrome: predicting survival using the EULAR-SS disease activity index (ESSDAI) in 1045 patients. Ann Rheum Dis. 2016;75(2):348–55.
Baldini C, Pepe P, Quartuccio L, Priori R, Bartoloni E, Alunno A, et al. Primary Sjogren’s syndrome as a multi-organ disease: impact of the serological profile on the clinical presentation of the disease in a large cohort of Italian patients. Rheumatology. 2014;53(5):839–44 (Oxford).
Gottenberg JE, Seror R, Miceli-Richard C, Benessiano J, Devauchelle-Pensec V, Dieude P, et al. Serum levels of beta2-microglobulin and free light chains of immunoglobulins are associated with systemic disease activity in primary Sjogren’s syndrome. Data at enrollment in the prospective ASSESS cohort. PLoS ONE. 2013;8(5):e59868.
Dumusc A, Ng WF, James K, Griffiths B, Price E, Pease C, et al. Comparison of ESSDAI and ClinESSDAI in potential optimisation of trial outcomes in primary Sjogren’s syndrome: examination of data from the UK primary Sjogren’s syndrome registry. Swiss Med Wkly. 2018;148:w14588.
Seror R, Mariette X, Bowman S, Baron G, Gottenberg JE, Bootsma H, et al. Accurate detection of changes in disease activity in primary Sjogren’s syndrome by the European league against rheumatism Sjogren’s syndrome disease activity index. Arthritis Care Res. 2010;62(4):551–8 (Hoboken).
Seror R, Ravaud P, Mariette X, Bootsma H, Theander E, Hansen A, et al. EULAR Sjogren’s syndrome patient reported index (ESSPRI): development of a consensus patient index for primary Sjogren’s syndrome. Ann Rheum Dis. 2011;70(6):968–72.
Qian J, He C, Li Y, Peng L, Yang Y, Xu D, et al. Ten-year survival analysis of patients with primary Sjogren’s syndrome in China: a national prospective cohort study. Ther Adv Musculoskelet Dis. 2021;13:1759720X211020179.
Gilboe IM, Kvien TK, Uhlig T, Husby G. Sicca symptoms and secondary Sjogren’s syndrome in systemic lupus erythematosus: comparison with rheumatoid arthritis and correlation with disease variables. Ann Rheum Dis. 2001;60(12):1103–9.
Garcia DM, de Reis OF, Modulo CM, Faustino J, Barbosa AP, Alves M, et al. Is Sjogren’s syndrome dry eye similar to dry eye caused by other etiologies. Discriminating different diseases by dry eye tests. PLoS ONE. 2018;13(12):e0208420.
Alani H, Henty JR, Thompson NL, Jury E, Ciurtin C. Systematic review and meta-analysis of the epidemiology of polyautoimmunity in Sjogren’s syndrome (secondary Sjogren’s syndrome) focusing on autoimmune rheumatic diseases. Scand J Rheumatol. 2018;47(2):141–54.
Haga HJ, Naderi Y, Moreno AM, Peen E. A study of the prevalence of sicca symptoms and secondary Sjogren’s syndrome in patients with rheumatoid arthritis, and its association to disease activity and treatment profile. Int J Rheum Dis. 2012;15(3):284–8.
Pasoto SG, de Adriano Oliveira Martins V, Bonfa E. Sjogren’s syndrome and systemic lupus erythematosus: links and risks. Open Access Rheumatol. 2019;11:33–45.
Dogru M, Katakami C, Inoue M. Tear function and ocular surface changes in noninsulin-dependent diabetes mellitus. Ophthalmology. 2001;108(3):586–92.
Eckstein AK, Finkenrath A, Heiligenhaus A, Renzing-Kohler K, Esser J, Kruger C, et al. Dry eye syndrome in thyroid-associated ophthalmopathy: lacrimal expression of TSH receptor suggests involvement of TSHR-specific autoantibodies. Acta Ophthalmol Scand. 2004;82(3 Pt 1):291–7.
Baffa Ldo P, Ricardo JR, Dias AC, Modulo CM, Braz AM, Paula JS, et al. Tear film and ocular surface alterations in chronic users of antiglaucoma medications. Arq Bras Oftalmol. 2008;71(1):18–21.
Rocha EM, Mantelli F, Nominato LF, Bonini S. Hormones and dry eye syndrome: an update on what we do and don’t know. Curr Opin Ophthalmol. 2013;24(4):348–55.
Akpek EK, Mathews P, Hahn S, Hessen M, Kim J, Grader-Beck T, et al. Ocular and systemic morbidity in a longitudinal cohort of Sjogren’s syndrome. Ophthalmology. 2015;122(1):56–61.
Chisholm DM, Mason DK. Labial salivary gland biopsy in Sjogren’s disease. J Clin Pathol. 1968;21(5):656–60.
Kvarnstrom M, Ottosson V, Nordmark B, Wahren-Herlenius M. Incident cases of primary Sjogren’s syndrome during a 5-year period in Stockholm County: a descriptive study of the patients and their characteristics. Scand J Rheumatol. 2015;44(2):135–42.
Plesivcnik Novljan M, Rozman B, Hocevar A, Grmek M, Kveder T, Tomsic M. Incidence of primary Sjogren’s syndrome in Slovenia. Ann Rheum Dis. 2004;63(7):874–6.
Restrepo-Jimenez P, Molano-Gonzalez N, Anaya JM. Geoepidemiology of Sjogren’s syndrome in Latin America. Joint Bone Spine. 2019;86(5):620–6.
Alves M, Reinach PS, Paula JS, Vellasco e Cruz AA, Bachette L, Faustino J, et al. Comparison of diagnostic tests in distinct well-defined conditions related to dry eye disease. PLoS ONE. 2014;9(5):e97921.
Baer AN, McAdams DeMarco M, Shiboski SC, Lam MY, Challacombe S, Daniels TE, et al. The SSB-positive/SSA-negative antibody profile is not associated with key phenotypic features of Sjogren’s syndrome. Ann Rheum Dis. 2015;74(8):1557–61.
Maslinska M, Manczak M, Wojciechowska B, Kwiatkowska B. The prevalence of ANA antibodies, anticentromere antibodies, and anti-cyclic citrullinated peptide antibodies in patients with primary Sjogren’s syndrome compared to patients with dryness symptoms without primary Sjogren’s syndrome confirmation. Reumatologia. 2017;55(3):113–9.
Rozzatti MS, Fontaneto E, Pedano V, Racca A, Pelosso M, Gobbi C, et al. Clinical usefulness of Beta2microglobulin in patients with primary Sjogren syndrome. Rev Fac Cien Med Univ Nac Cordoba. 2015;72(1):7–15.
Pertovaara M, Korpela M. Serum beta2 microglobulin correlates with the new ESSDAI in patients with Sjogren’s syndrome. Ann Rheum Dis. 2011;70(12):2236–7.
Asashima H, Inokuma S, Onoda M, Oritsu M. Cut-off levels of salivary beta2-microglobulin and sodium differentiating patients with Sjogren’s syndrome from those without it and healthy controls. Clin Exp Rheumatol. 2013;31(5):699–703.
He J, Ding Y, Feng M, Guo J, Sun X, Zhao J, et al. Characteristics of Sjögren’s syndrome in rheumatoid arthritis. Rheumatology. 2013;52(6):1084–9 (Oxford).
Kollert F, Fisher BA. Equal rights in autoimmunity: is Sjogren’s syndrome ever “secondary”? Rheumatology. 2020;59(6):1218–25 (Oxford).
Huo AP, Lin KC, Chou CT. Predictive and prognostic value of antinuclear antibodies and rheumatoid factor in primary Sjogren’s syndrome. Int J Rheum Dis. 2010;13(1):39–47.
Theander E, Jonsson R, Sjostrom B, Brokstad K, Olsson P, Henriksson G. Prediction of Sjogren’s syndrome years before diagnosis and identification of patients with early onset and severe disease course by autoantibody profiling. Arthritis Rheumatol. 2015;67(9):2427–36.
Tishler M, Yaron I, Shirazi I, Yaron M. Clinical and immunological characteristics of elderly onset Sjogren’s syndrome: a comparison with younger onset disease. J Rheumatol. 2001;28(4):795–7.
Yayla ME, Karaman Z, Torgutalp M, Kelesoglu Dincer AB, Aydemir Guloksuz EG, Sezer S, et al. Early onset primary Sjogren syndrome, clinical and laboratory characteristics. Clin Rheumatol. 2020;39(9):2689–96.
Ng KP, Isenberg DA. Sjogren’s syndrome: diagnosis and therapeutic challenges in the elderly. Drugs Aging. 2008;25(1):19–33.
Soret P, Le Dantec C, Desvaux E, Foulquier N, Chassagnol B, Hubert S, et al. A new molecular classification to drive precision treatment strategies in primary Sjogren’s syndrome. Nat Commun. 2021;12(1):3523.
de Oliveira FR, Fantucci MZ, Adriano L, Valim V, Cunha TM, Louzada-Junior P, et al. Neurological and inflammatory manifestations in Sjogren’s syndrome: the role of the kynurenine metabolic pathway. Int J Mol Sci. 2018;19(12):3953.
Bunya VY, Bhosai SJ, Heidenreich AM, Kitagawa K, Larkin GB, Lietman TM, et al. Association of dry eye tests with extraocular signs among 3514 participants in the Sjogren’s syndrome international registry. Am J Ophthalmol. 2016;172:87–93.
Haldorsen K, Moen K, Jacobsen H, Jonsson R, Brun JG. Exocrine function in primary Sjogren syndrome: natural course and prognostic factors. Ann Rheum Dis. 2008;67(7):949–54.
Li H, Ice JA, Lessard CJ, Sivils KL. Interferons in Sjogren’s syndrome: genes, mechanisms, and effects. Front Immunol. 2013;4:290.
Roescher N, Tak PP, Illei GG. Cytokines in Sjogren’s syndrome: potential therapeutic targets. Ann Rheum Dis. 2010;69(6):945–8.
Nezos A, Gravani F, Tassidou A, Kapsogeorgou EK, Voulgarelis M, Koutsilieris M, et al. Type I and II interferon signatures in Sjogren’s syndrome pathogenesis: contributions in distinct clinical phenotypes and Sjogren’s related lymphomagenesis. J Autoimmun. 2015;63:47–58.
Shiboski CH, Baer AN, Shiboski SC, Lam M, Challacombe S, Lanfranchi HE, et al. Natural history and predictors of progression to Sjogren’s syndrome among participants of the Sjogren’s international collaborative clinical alliance registry. Arthritis Care Res. 2018;70(2):284–94 (Hoboken).
Billings M, Amin Hadavand M, Alevizos I. Comparative analysis of the 2016 ACR-EULAR and the 2002 AECG classification criteria for Sjogren’s syndrome: findings from the NIH cohort. Oral Dis. 2018;24(1–2):184–90.
Acknowledgements
We would like to thank Dr. Rodrigo de Oliveira, Dr. Rodrigo Luppino Assad, and Dr. Flavio Calil Petean for the medical care to outpatients. We also thank Dra. Graziela Cavalcanti for performing the labial salivary gland biopsies and Prof. Dr. Alfredo Ribeiro-Silva (in memorian) for the histopathological analysis.
Funding
This study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (Grants: 2015/20580-7, 2014/22451-7, and 2015/07249-0) (São Paulo, SP, Brazil); Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (Grant: 474450/2012-0) (Brasilia, DF, Brazil); CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) (Finance Code 001) (Brasilia, DF, Brazil); Fundação de Apoio ao Ensino, Pesquisa e Assistência do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FAEPA) (Grant: 669/2018) (Ribeirão Preto, SP. Brazil); and Research Core of Ocular Physiopathology and Therapeutics at the University of São Paulo (NAP-FTO) (Grant: 12.1.25431.01.7) (Ribeirão Preto, SP. Brazil). This study was also supported by an NIDCR, NIH intramural research grant to JAC (1ZIADE000695).
Author information
Authors and Affiliations
Contributions
FRO, PLJ and EMR, conceptualization; FRO, CFM, CMM and DMG, methodology; FRO and EMR, validation and formal analysis; PLJ and EMR, resources; FRO, ACFM, JAC and EMR, writing-original draft preparation; FRO, ACFM, JAC and EMR, writing-review and editing. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional review board (CAAE #: 37688914.2.0000.5440), and all patients provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors have no commercial or proprietary interest in any concept or product described in this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
Table S1: Demographic and laboratorial profile of secondary SS (sSS) patients according to other rheumatic diseases, such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SSc) and other overlaps (n=149). Table S2: Etiological diagnosis, clinical and laboratory features of patients with sicca non-Sjogren’s Syndrome (NSS, n=163).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Oliveira, F.R., Motta, A.C.F., Módulo, C.M. et al. Clinical and laboratory evaluation of sicca complaints: distinctive aspects of primary, secondary and non-Sjogren syndrome. Adv Rheumatol 62, 23 (2022). https://doi.org/10.1186/s42358-022-00255-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42358-022-00255-2