
Abstract
Background
Perioperative prophylactic dexamethasone is commonly administered to reduce postoperative nausea and vomiting (PONV) and pain after surgery. In this study, we aimed to systematically review the efficacy and adverse effects of perioperative dexamethasone administration.
Methods
We conducted a systematic search until January 2023 in scientific databases, including PubMed, Scopus, Embase, Web of Science, and Google Scholar. After assessing the methodological quality of relevant studies, we synthesized those focusing on PONV, oral food intake tolerance, impaired wound healing, major postoperative complications, and postoperative infections following the perioperative administration of dexamethasone.
Results
A total of 27 studies were included in this systematic review and meta-analysis. The dexamethasone group showed decreased PONV (OR = 0.19; 95% CI 0.06–0.55), increased oral food intake tolerance (OR = 7.38; 95% CI 1.07–51.11), increased risk of impaired wound healing (OR = .48; 95% CI 0.52–4.21), decreased probability of postoperative infection (OR = 0.61; 95% CI 0.51–0.72), and increased risk of major postoperative complications (OR = 1.27; 95% CI 0.68–2.39) compared to the controls.
Conclusions
The results of our pooled data analysis showed that dexamethasone was superior to the control in terms of PONV, oral food intake tolerance, and postoperative infections.
Similar content being viewed by others

Background
Dexamethasone is often used as a premedication for anesthesia due to its anti-inflammatory properties that can help with airway manipulation, prevention of skin and drug reactions, and reduction of nausea and vomiting. Additionally, it has analgesic properties that can aid in pain management (Polderman et al. 2018). Postoperative nausea and vomiting (PONV) and pain are the side effects of this medication that can lead to patient discomfort, decreased satisfaction with surgery, and delayed functional improvement of patients undergoing surgery (Cui et al. 2015). Glucocorticoids can not only relieve pain by reducing inflammation at the wound site (Bahammam et al. 2017) but also may be used perioperatively to reduce PONV due to their antiemetic effects (Gan et al. 2007).
Meanwhile, due to induced peripheral resistance to insulin and the immunosuppressive effects of glucocorticoids, there are debates on the preoperative administration of dexamethasone (Kwon et al. 2013; Jules-Elysee et al. 2011). In this regard, Backes et al. reported side effects, such as reduced sleep quality, high risk of infection, and early postoperative hyperglycemia following the application of preoperative dexamethasone (Backes et al. 2013). It should be noted that these side effects are associated with long-term treatment using glucocorticoids (Schimmer BP, Funder JW. ACTH 2011), while it remains controversial whether a single perioperative dose of glucocorticoids is associated with an increased risk of adverse effects.
Overall, the use of dexamethasone during surgery to reduce PONV remains a topic of debate. Therefore, we aimed to conduct this systematic review and meta-analysis of the available evidence to investigate the efficacy and adverse effects of perioperative and intraoperative administration of dexamethasone in all healthy individuals undergoing different types of surgery.
Methods
In this systematic review and meta-analysis, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Search strategy
To identify relevant published studies, we conducted a systematic search until January 2023 in scientific databases, including PubMed, Scopus, Embase, Web of Science, and Google Scholar, using related keywords provided in the Additional file 1 (Supplementary file S1). A medical librarian supervised the search strategy. We also manually searched the reference lists of all eligible studies and previous reviews for additional relevant research.
Population
All healthy individuals undergoing different types of surgery were included in our study with no restrictions on age, sex, nationality, ethnicity, race, or geographic location.
Intervention
In this review, we evaluated any formulation or dose of dexamethasone, administered perioperatively or intraoperatively through various routes, alone or in combination therapy.
Comparator
Other treatment regimens or controls with either placebo or other antiemetic agents were the comparators in this study.
Outcome
The effects of dexamethasone on the prevention of PONV and oral food intake tolerance were the outcomes of this study. Also, other outcomes of interest were the adverse effects of dexamethasone, including impaired wound healing, major postoperative complications, and postoperative infections.
Inclusion and exclusion criteria
Studies based on the Population, Intervention, Comparator, Outcomes (PICO) framework were included in this systematic review. In studies where dexamethasone implant was used in ocular surgeries, the outcomes of interest were not reported, and studies with incomplete or unidentified data were excluded. Also, animal, in vitro, or in vivo studies, non-English articles, publications without accessible full-text manuscripts in English, case reports, case series, literature reviews, letters to the editor, theses, book sections, conference proceedings, and preprints were excluded.
Data extraction
After collecting records from the online databases, duplicated records were removed in Endnote Version 20, and the rest of the duplicates were deleted manually. Three authors independently extracted data, including the first author, publication date, study type, study location, total sample size, age, sex, dose, main outcomes, and adverse effects. In case of disagreement between the authors, the senior author provided guidance and advice to help resolve the issue. In studies with incomplete data, the corresponding author was contacted if possible. The extracted data were organized in Microsoft Excel 2019.
Quality assessment
Three independent investigators evaluated the quality of all studies, using the Joanna Briggs Institute (JBI) critical appraisal technique. Generally, JBI has proposed nine, 11, and 13 criteria for evaluating the quality of quasi-experimental studies, cohorts, and randomized controlled trials (RCTs), respectively.
Statistical analysis (meta-analysis)
Data are presented using descriptive statistics (mean ± SD) for continuous variables. Frequency and percentage are also measured for categorical variables. Dichotomous data are expressed as pooled odds ratio (OR) and 95% confidence intervals (95% CI). The mean difference (MD) and 95% CIs were calculated for continuous outcomes. Moreover, a random-effects meta-analysis of the available data was conducted. Heterogeneity between studies was assessed based on the I2 and P value of Cochran’s Q test; I2 > 50% and P < 0.05 were considered statistically significant. Additionally, funnel plots were used to investigate publication bias. All statistical analyses were performed in Stata Version 14.2 (StataCorp LLC, College Station, TX, USA).
Results
Search results
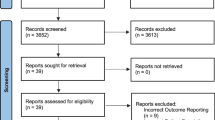
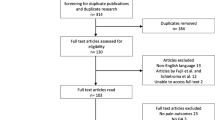
A total of 202 articles were identified in the scientific databases, 55 of which were found to be duplicates. After removing duplicates, 82 articles were excluded based on the title and abstract, and 65 articles were evaluated for the availability of their full-text manuscripts. A total of 57 full-text articles were found and screened. After screening the full-text manuscripts, 27 articles were included in the qualitative synthesis and meta-analysis, based on the inclusion criteria (Fig. 1).

Flowchart of studies included in the systematic review
The included articles were as follows: 16 RCTs, nine cohorts, one non-randomized experimental study, and one case–control study. Most studies were conducted in the USA (n = 9) and the Netherlands (n = 5), followed by China (n = 2) and then, Turkey, Scotland, Ukraine, Germany, Korea, Brazil, Russia, Pakistan, Thailand, Georgia, and Canada, each with one study.
Demographic characteristics
In the reviewed studies, a total of 31,048 cases were examined for the efficacy and adverse effects of dexamethasone administered perioperatively or intraoperatively through various routes. In studies where sex was reported, 18,872 of the subjects (61%) were male, while 11,715 (39%) were female. The sample size of the included studies ranged from 41 to 7910 participants. The mean ± SD age of the patients was 51.1 ± 9.2 years, ranging from 2 months to 88 years. In 17 studies, the administration of dexamethasone was reported to be effective. Two of the included studies (Karaman et al. 2009a; Tkachenko and Pyasetska 2019) each included two intervention groups with different characteristics; therefore, they were entered separately into Table 1 and meta-analysis. The characteristics of the reviewed studies are presented in Table 1.
PONV
The pooled data of eight eligible studies reported an OR of 0.19 in the meta-analysis (95% CI 0.06–0.55), which indicated that perioperative or intraoperative dexamethasone administration could be effective in decreasing PONV (Fig. 2).

Forest plots for comparison of dexamethasone effectiveness in decreasing postoperatively nausea and vomiting between intervention and control groups
Oral food intake tolerance
The pooled data of four eligible studies indicated an OR of 7.38 in the meta-analysis (95% CI 1.07–51.11), suggesting that perioperative or intraoperative dexamethasone increased the oral food intake tolerance (Fig. 3).

Forest plots for comparison of dexamethasone effectiveness in increasing tolerability to start taking oral foods between intervention and control groups
Impaired wound healing and postoperative infection
The meta-analysis of three eligible studies indicated that dexamethasone increased the risk of impaired wound healing (OR = 1.48; 95% CI 0.52–4.21) (Fig. 4). On the other hand, in the meta-analysis of three other eligible studies, dexamethasone decreased the probability of postoperative infection (OR = 0.61; 95% CI 0.51–0.72) (Fig. 5).

Forest plots for comparison of dexamethasone effectiveness in increasing the risk of wound healing impairment between intervention and control groups

Forest plots for comparison of dexamethasone effectiveness in decreasing the probability of postoperative infection between intervention and control groups
Major postoperative complications
The pooled OR of four eligible studies indicated that dexamethasone increased the risk of major postoperative complications, including shock, hemorrhage, deep vein thrombosis (DVT), and pulmonary embolism (PE) (OR = 1.27; 95% CI 0.68–2.39) (Fig. 6).

Forest plots for comparison of dexamethasone effectiveness in increasing the risk of major postoperative complications between intervention and control groups
Quality assessment and publication bias of studies
The JBI critical appraisal score was six for both quasi-experimental (out of 9 points) and case–control (out of 10 points) studies. It also ranged from five to eight (out of 11 points) for cohorts and from six to 10 (out of 13 points) for RCTs included in this review. The quality assessment tools varied based on the study design; consequently, the scores could not be directly compared (Supplementary file S2, Table S1–4). However, the funnel plot analysis showed a mild asymmetry due to possible publication bias or heterogeneity (Figs. 7, 8, 9, 10 and 11).

Funnel plot for publication bias of studies which reported dexamethasone effectiveness in decreasing postoperatively nausea and vomiting

Funnel plot for publication bias of studies which reported dexamethasone effectiveness in increasing tolerability to start taking oral foods

Funnel plot for publication bias of studies which reported dexamethasone effectiveness in increasing the risk of wound healing impairment

Funnel plot for publication bias of studies which reported dexamethasone effectiveness in decreasing the probability of postoperative infection

Funnel plot for publication bias of studies which reported dexamethasone effectiveness in increasing the risk of major postoperative complications
Discussion
In this PRISMA-compliant systematic review and meta-analysis, we aimed to investigate the efficacy and adverse effects of perioperative or intraoperative administration of dexamethasone in all healthy individuals undergoing any type of surgery. Dexamethasone, due to its antiemetic and analgesic effects, is the first intervention to reduce PONV associated with general anesthesia and relieve pain following various surgeries. However, the efficacy of this medication in preventing PONV is still controversial (Fan et al. 2018). Feelings of discomfort, shame, dissatisfaction with the surgery outcome, as well as fear of a new surgery, are some psychiatric problems following PONV (Jolley 2013). In this regard, Apfel et al. showed that the patients' fear of PONV was more significant than their fear of postoperative pain (Apfel et al. 2004). Therefore, evidence-based studies are necessary to help anesthesiologists make accurate clinical decisions.
The present review indicated that perioperative or intraoperative dexamethasone administration could effectively decrease PONV. Three recent systematic reviews reported that prophylactic dexamethasone decreased the incidence of PONV after mastectomy (Xu et al. 2020), total hip arthroplasty (Fan et al. 2018), and thyroidectomy (Chen et al. 2012) relative to the placebo. Evidence suggests that the central antiemetic effects of dexamethasone reduced the incidence of PONV (Lunn and Kehlet 2013). On the other hand, in three RCTs conducted by Corcoran et al. (Corcoran et al. 2017), Ituk et al. (Ituk and Thenuwara 2018), and Kleif et al. (Kleif et al. 2017), it was found that dexamethasone did not effectively relieve PONV after different types of surgery.
This systematic review revealed that prophylactic dexamethasone increased the oral food intake tolerance of the patients in the dexamethasone group compared to the placebo group. Consistent with our results, Pappas et al. showed that administration of prophylactic dexamethasone in children undergoing tonsillectomy improved their postoperative oral intake (Pappas et al. 1998). The beneficial anti-nausea and vomiting effects of dexamethasone persisted until about three days after surgery and facilitated early oral intake (PO) (Karaman et al. 2009b).
The possible adverse effects of dexamethasone are impaired wound healing, hyperglycemia, and increased major/infectious complications (Kwon et al. 2013; Bartlett and Hartle 2013). Adverse effects, such as impaired wound healing and increased anastomotic drainage, often occur following chronic dexamethasone administration (Bartlett and Hartle 2013; Eriksen et al. 2014). Our meta-analysis showed that dexamethasone increased the risk of impaired wound healing. Blume et al. also observed a significantly higher rate of wound infection following the administration of high-dose (0.4–0.8 mg/kg/day) prophylactic dexamethasone in cervical spondylotic myelopathy surgery (Blume et al. 2018a). In another study on mandibular surgeries, no significant difference was observed in the incidence of impaired wound healing between the dexamethasone and control groups (Snäll et al. 2013).
In the present study, dexamethasone decreased the risk of postoperative infection. According to a study by Sandini et al., a single intraoperative dose of dexamethasone was associated with a lower probability of post-pancreaticoduodenectomy sepsis (Sandini et al. 2018a). A meta-analysis by Dan et al. demonstrated that intraoperative dexamethasone did not significantly increase the risk of infection (Dan et al. 2010). Nevertheless, it is worth mentioning that the prescription of dexamethasone could increase blood sugar by increasing peripheral insulin resistance. Meanwhile, the risk of developing infections after surgery increased in patients with uncontrolled blood sugar (Kwon et al. 2013), and dexamethasone exerted well-known immunosuppressive effects, which might increase the risk of infectious complications.
The pooled data of our meta-analysis indicated that dexamethasone increased the risk of major postoperative complications. There are conflicting reports regarding the effect of intraoperative glucocorticoids on postoperative complications. Diabetic burn patients receiving intraoperative steroids showed increased rates of major complications, especially partial graft loss compared to the control group (Egan et al. 2019a). However, another study reported that prophylactic dexamethasone was not associated with any differences in postoperative major/infectious complications compared to the control group (Newhook et al. 2021a). In some evaluated studies, the score of the verbal analogue scale for pain was significantly lower in patients who received perioperative prophylactic dexamethasone compared to the control group (Lim et al. 2011; Hatfield 2017; Samona et al. 2017; Khan and Iqbal 2012; Thongrong et al. 2018). Nonetheless, due to a lack of sufficient data, we were unable to conduct a meta-analysis on this subject.
The major limitation of the present study was the lack of a subgroup analysis based on different types of surgery, anesthesia techniques, and characteristics of patients, such as sex or age. Also, we did not compare the efficacy of dexamethasone with that of other antiemetics. Despite these limitations, our study is the most recent meta-analysis evaluating the efficiency and safety of prophylactic administration of dexamethasone.
Conclusions
The results of this meta-analysis suggested that prophylactic administration of dexamethasone not only decreased the incidence of PONV and the probability of postoperative infection in all healthy individuals undergoing surgery but also increased their tolerance to start oral food intake. However, dexamethasone administration increased the risk of impaired wound healing and major postoperative complications. Since the advantages of dexamethasone outweigh its disadvantages, the perioperative administration of prophylactic dexamethasone can benefit the patients.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PONV:
-
Postoperative nausea and vomiting
- OR:
-
Odds ratio
- MD:
-
Mean difference
- CI:
-
Confidence interval
- SD:
-
Standard deviation
- DVT:
-
Deep vein thrombosis
- RCT:
-
Randomized controlled trials
- PO :
-
Per Os
- PE:
-
Pulmonary embolism
References
Apfel C, Kranke P, Eberhart L (2004) Comparison of surgical site and patient’s history with a simplified risk score for the prediction of postoperative nausea and vomiting. Anaesthesia 59(11):1078–1082
Backes JR, Bentley JC, Politi JR, Chambers BT (2013) Dexamethasone reduces length of hospitalization and improves postoperative pain and nausea after total joint arthroplasty: a prospective, randomized controlled trial. J Arthroplasty 28(8):11–17
Bahammam MA, Kayal RA, Alasmari DS, Attia MS, Bahammam LA, Hassan MH et al (2017) Comparison between dexamethasone and ibuprofen for postoperative pain prevention and control after surgical implant placement: a double-masked, parallel-group, placebo-controlled randomized clinical trial. J Periodontol 88(1):69–77
Bartlett R, Hartle AJ (2013) Routine use of dexamethasone for postoperative nausea and vomiting: the case against. Anaesthesia. 68(9):892–6
Bateman MC, Conejero JA, Mooney EK, Rothkopf DM (2006) Short-stay cleft palate surgery with intraoperative dexamethasone and marcaine. Ann Plast Surg. 57(3):245–7
Blume C, Wiederhold H, Geiger M, Clusmann H, Müller CA (2018a) Lacking benefit of intraoperative high-dose dexamethasone in instrumented surgery for cervical Spondylotic myelopathy. J Neurol Surg A Central Eur Neurosurg 79(02):116–122
Blume C, Wiederhold H, Geiger M, Clusmann H, Müller CA (2018b) Lacking Benefit of Intraoperative High-Dose Dexamethasone in Instrumented Surgery for Cervical Spondylotic Myelopathy. J Neurol Surg A Cent Eur Neurosurg 79(02):116–122
Chen CC, Siddiqui FJ, Chen TL, Chan ESY, Tam KW (2012) Dexamethasone for prevention of postoperative nausea and vomiting in patients undergoing thyroidectomy: meta-analysis of randomized controlled trials. World J Surg. 36(1):61–8
Corcoran T, Kasza J, Short T, O’loughlin E, Chan M, Leslie K et al (2017) Intraoperative dexamethasone does not increase the risk of postoperative wound infection: a propensity score-matched post hoc analysis of the ENIGMA-II trial (EnDEX). Br J Anaesthesia. 118(2):190–9
Corcoran T, Kasza J, Short T, Oloughlin E, Chan M, Leslie K et al (2017) Intraoperative dexamethasone does not increase the risk of postoperative wound infection: a propensity score-matched post hoc analysis of the ENIGMA-II trial (EnDEX). Br J Anaesth. 118(2):190–9
Cui Z, Liu X, Teng Y, Jiang J, Wang J, Xia Y (2015) The efficacy of steroid injection in total knee or hip arthroplasty. Knee Surg Sports Traumatol Arthrosc 23(8):2306–2314
Dan AE, Thygesen TH, Pinholt EM (2010) Corticosteroid administration in oral and orthognathic surgery: a systematic review of the literature and meta-analysis. J Oral Maxillofac Surg 68(9):2207–2220
Dieleman JM, Nierich AP, Rosseel PM, van der Maaten JM, Hofland J, Diephuis JC et al (2012) Intraoperative High-Dose Dexamethasone for Cardiac Surgery: a Randomized Controlled Trial. JAMA 308(17):1761–1767
Egan KG, Allen A, Hendren G, Mellott AJ, Bhavsar D (2019a) Effects of intraoperative dexamethasone administration in adult diabetic burn patients. J Burn Care Res 40(5):627–632
Egan KG, Allen A, Hendren G, Mellott AJ, Bhavsar D (2019b) Effects of intraoperative dexamethasone administration in adult diabetic burn patients. J Burn Care Res 40(5):627–632
Eriksen T, Lassen C, Gögenur I (2014) Treatment with corticosteroids and the risk of anastomotic leakage following lower gastrointestinal surgery: a literature survey. Colorectal Dis 16(5):O154–O160
Fan Z-r, Ma J, Ma X-l, Wang Y, Sun L, Wang Y, et al (2018) The efficacy of dexamethasone on pain and recovery after total hip arthroplasty: A systematic review and meta-analysis of randomized controlled trials. Medicine. 97(13):e0100
Foulkes G, Robinson Jr JJ (1990) Intraoperative Dexamethasone Irrigation in Lumbar Microdiskectomy. Clin Orthop Relat Res 261:224–228
Gan TJ, Meyer TA, Apfel CC, Chung F, Davis PJ, Habib AS et al (2007) Society for Ambulatory Anesthesia guidelines for the management of postoperative nausea and vomiting. Anesth Analg 105(6):1615–1628
Hatfield S (2017) The association between intraoperative single-dose dexamethasone and postoperative pain in patients undergoing laparoscopic cholecystectomy
Ituk U, Thenuwara K (2018) The effect of a single intraoperative dose of intravenous dexamethasone 8 mg on post-cesarean delivery analgesia: a randomized controlled trial. Int J Obstet Anesth 35:57–63
Jacob KA, Leaf DE, Dieleman JM, Van Dijk D, Nierich AP, Rosseel PM et al (2015a) Intraoperative High-Dose Dexamethasone and Severe AKI after Cardiac Surgery. J Am Soc Nephrol 26(12):2947–2951
Jacob KA, Dieleman JM, Nathoe HM, van Osch D, de Waal EE, Cramer MJ et al (2015b) The Effects of Intraoperative Dexamethasone on Left Atrial Function and Postoperative Atrial Fibrillation in Cardiac Surgical Patients. Neth Heart J 23(3):168–173
Jolley S (2001) Managing post-operative nausea and vomiting. Nursing Standard (through 2013). 15(40):47
Jules-Elysee KM, Lipnitsky JY, Patel N, Anastasian G, Wilfred SE, Urban MK et al (2011) Use of low-dose steroids in decreasing cytokine release during bilateral total knee replacement. Regional Anesthesia Pain Med. 36(1):36–40
Karaman M, İlhan AE, Dereci G, Arman T (2009a) Determination of optimum dosage of intraoperative single dose dexamethasone in pediatric tonsillectomy and adenotonsillectomy. Int J Pediatr Otorhinolaryngol 73(11):1513–1515
Karaman M, İlhan AE, Dereci G, Tek A (2009b) Determination of optimum dosage of intraoperative single dose dexamethasone in pediatric tonsillectomy and adenotonsillectomy. Int J Pediatr Otorhinolaryngol 73(11):1513–1515
Khan MI, Iqbal MK (2012) Post Tonsillectomy pain: Role of single intraoperative dose of Dexamethasone. Pakistan J Med Health Scie Online http://pjmhsonline.com/July-Sept
Kleif J, Kirkegaard A, Vilandt J, Gögenur I (2017) Randomized clinical trial of preoperative dexamethasone on postoperative nausea and vomiting after laparoscopy for suspected appendicitis. J Br Surg 104(4):384–392
Klement MR, Wilkens HS, Fillingham YA, Manrique J, Austin MS, Parvizi J (2018) Intraoperative dexamethasone reduces readmission rates without affecting risk of thromboembolic events or infection after total joint arthroplasty. J Arthroplasty. 33(10):3252–6
Kwon S, Thompson R, Dellinger P, Yanez D, Farrohki E, Flum D (2013) Importance of perioperative glycemic control in general surgery: a report from the Surgical Care and Outcomes Assessment Program. Ann Surg 257(1):8
Lim SH, Jang EH, Kim M-H, Cho K, Lee JH, Lee KM et al (2011) Analgesic Effect of Preoperative versus Intraoperative Dexamethasone after Laparoscopic Cholecystectomy with Multimodal Analgesia. Korean J Anesthesiol 61(4):315
Lomivorotov V, Kornilov I, Boboshko V, Shmyrev V, Bondarenko I, Soynov I et al (2020) Effect of intraoperative dexamethasone on major complications and mortality among infants undergoing cardiac surgery: the DECISION randomized clinical trial. JAMA. 323(24):2485–92
Lunn T, Kehlet H (2013) Perioperative glucocorticoids in hip and knee surgery–benefit vs. harm? A review of randomized clinical trials. Acta Anaesthesiologica Scandinavica. 57(7):823–34
Newhook TE, Soliz JM, Prakash LR, Hancher-Hodges S, Speer BB, Wilks JA et al (2021a) Impact of intraoperative dexamethasone on surgical and oncologic outcomes for patients with resected pancreatic ductal adenocarcinoma. Ann Surg Oncol 28(3):1563–1569
Newhook TE, Soliz JM, Prakash LR, Hancher-Hodges S, Speer BB, Wilks JA et al (2021b) Impact of Intraoperative Dexamethasone on Surgical and Oncologic Outcomes for Patients with Resected Pancreatic Ductal Adenocarcinoma. Ann Surg Oncol 28(3):1563–1569
Pappas A, Sukhani R, Hotaling A, Mikat-Stevens M, Donzelli J, Shenoy K (1998) The effect of intraoperative dexamethasone on the immediate and delayed postoperative morbidity in children undergoing ambulatory adenotonsillectomy. Anesth Analg 86(2S):14S
Pappas A, Sukhani R, Hotaling A, Mikat-Stevens M, Donzelli J, Shenoy K (1998) The effect of intraoperative dexamethasone on the immediate and delayed postoperative morbidity in children undergoing ambulatory adenotonsillectomy. Anesth Analg 86(2S):14S
Polderman JA, Farhang-Razi V, Van Dieren S, Kranke P, DeVries JH, Hollmann MW et al (2018) Adverse side effects of dexamethasone in surgical patients. Cochrane Database Syst Rev. 8(8):CD01940-CD
Samona J, Cook C, Krupa K, Swatsell K, Jackson A, Dukes C et al (2017) Effect of Intraoperative Dexamethasone on Pain Scores and Narcotic Consumption in Patients Undergoing Total Knee Arthroplasty. Orthop Surg 9(1):110–114
Sandini M, Ruscic KJ, Ferrone CR, Warshaw AL, Qadan M, Eikermann M et al (2018a) Intraoperative dexamethasone decreases infectious complications after pancreaticoduodenectomy and is associated with long-term survival in pancreatic cancer. Ann Surg Oncol 25(13):4020–4026
Sandini M, Ruscic KJ, Ferrone CR, Warshaw AL, Qadan M, Eikermann M et al (2018b) Intraoperative Dexamethasone Decreases Infectious Complications after Pancreaticoduodenectomy and is Associated with Long-Term Survival in Pancreatic Cancer. Ann Surg Oncol 25(13):4020–4026
Sauër AMC, Slooter AJ, Veldhuijzen DS, van Eijk MM, Devlin JW, van Dijk DJA et al (2014) Intraoperative dexamethasone and delirium after cardiac surgery: a randomized clinical trial. Anesth Analg. 119(5):1046–52
Schimmer BP, Funder JW (2011) ACTH, adrenal steroids, and pharmacology of the adrenal cortex. Goodman and Gilman’s the pharmacological basis of therapeutics. pp 1209–36
Shakeel M, Trinidade A, Al-Adhami A, Karamchandani D, Engelhardt T, Ah-See KW et al (2010) Intraoperative Dexamethasone and the Risk of Secondary Posttonsillectomy Hemorrhage. J Otolaryngol Head Neck Surg 39(6):732–736
Snäll J, Kormi E, Lindqvist C, Suominen AL, Mesimäki K, Törnwall J et al (2013) Impairment of wound healing after operative treatment of mandibular fractures, and the influence of dexamethasone. Br J Oral Maxillofac Surg 51(8):808–812
Splinter WM, Roberts DJ (1996) Dexamethasone decreases vomiting by children after tonsillectomy. Anesth Analg 83(5):913–916
Thongrong C, Chullabodhi P, Kasemsiri P, Kitkhuandee A, Plailaharn N, Sabangban L, et al (2018) Effects of intraoperative dexamethasone and ondansetron on postoperative nausea and vomiting in microvascular decompression surgery: a randomized controlled study. 2018
Tkachenko R, Pyasetska N (2019) The efficiency of intrathecal dexamethasone for spinal anaesthesia in elective caesarean section. Regional Anesthesia Pain Med. 44(10):A192-A
Van Osch D, Dieleman JM, Nathoe HM, Boasson MP, Kluin J, Bunge JJ et al (2015) Intraoperative High-Dose Dexamethasone in Cardiac Surgery and the Risk of Rethoracotomy. Ann Thorac Surg 100(6):2237–2242
Xu L, Xie X, Gu X (2020) Dexamethasone for preventing postoperative nausea and vomiting after mastectomy. Medicine 99(30):e21417
Zhang H, Lu J, Wu Q, Wu B, Xu C, Fan Y et al (2019) A perioperative small dose of dexamethasone enhances postoperative recovery by reducing volume and inflammatory contents in wound drainage after thyroid surgery: a double-blinded, randomized, prospective study. World J Surg 43(7):1721–1727
Acknowledgements
We appreciate the Kerman University of Medical Sciences.
Funding
Nil.
Author information
Authors and Affiliations
Contributions
NN and PN designed the study, MJN, MOS and, MS collected data, MJN wrote the first draft of the paper, MH contributed to the writing and revision of the manuscript. NN designed the Meta-analysis. All authors contributed to finalizing the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary file S1. Relevant published studies
Additional file 2:
Supplementary file S2. Table 1. Quality Assessment of Cohort Studies. Table 2. Quality Assessment of Randomized Controlled Trial Studies. Table 3. Quality Assessment of Non-Randomized Experimental Studies. Table 4. Quality Assessment of Case Control Studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Najafzadeh, M.J., Shafiei, M., Sharifi, M. et al. The efficacy and safety of perioperative administration of dexamethasone: a systematic review and meta-analysis. Ain-Shams J Anesthesiol 15, 79 (2023). https://doi.org/10.1186/s42077-023-00376-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42077-023-00376-w