
Abstract
Background
The protrusion of cranial contents via a skull defect is known as an encephalocele. Unlike western countries where occipital encephalocele dominates, anterior encephaloceles are the most common types of encephalocele in Southeast Asia, parts of Russia, and Central Africa. We present the clinical presentation and surgical management of an 8-day-old infant with frontoethmoidal encephalocele.
Case presentation
An 8-day-old neonate born to a 24-year-old mother with no antenatal follow-up was referred with a compliant of frontonasal swelling which was present since birth. Physical examination of the neonate revealed a cystic lobulated swelling over the upper edge of the nasal bridge. Computed tomography imaging showed an anterior skull defect, resulting in frontonasal meningoencephalocele. The patient underwent a one-stage operation, which combined nasal-coronal approach with frontal craniotomy, to remove the dysplastic tissue and reconstruct the defect. The patient had successful recovery period with acceptable cosmesis.
Conclusion
We presented a case of frontoethmoidal encephalocele, which is rare in western countries but whose incidence is relatively higher in African countries. Perinatal care is necessary for prevention and early detection of such cases. Direct surgical repair is still the main mode of intervention.
Similar content being viewed by others


Introduction
Encephalocele is described as the displacement of cranial contents out of the skull's normal boundaries. It may include meninges alone (meningocele), meninges plus brain tissue (meningoencephalocele) or it may be linked to the ventricles (meningoencephalocystocele) [1]. Encephaloceles are divided into four groups: basal, occipital, sincipital (anterior), and convexity [2]
Researches indicate that one out of every 5000 to 10,000 newborn is born with encephalocele [3,4,5]. The occurrence of certain kinds of encephalocele is different depending on what part of the world you are in and the ethnicity of the person affected. In Central Africa, Southeast Asia, and some regions of Russia, anterior encephaloceles are the most prevalent type of encephaloceles found, occurring in up to 1 in 3500 live births. By comparison, an anterior encephalocele is a much rarer occurrence, with just 1 out of every 35,000 live births in North America, while occipital encephaloceles makes up the vast majority of cases, representing 85% of occurrences [6]. According to meta-analysis done by Paddy Ssentongo et al., the region of East Africa has one of the highest rates of neural tube defect worldwide, with Ethiopia being one of the worst affected [7].
It is believed that the development of encephalocele is due to a combination of genetic and environmental elements, such as illnesses experienced by the mother, medications taken, or a lack of vitamin B12, folic acid, or minerals in the first three months of pregnancy [8]. Folic acid supplementation and fortification are proven to decrease incidence of neural tube defects in infants [9, 10].
A CT scan is the best diagnostic tool to look for both internal and external bone abnormalities. MRI can be utilized to reveal the contents of the encephalocele and identify other irregularities in the brain [11]. Surgical repair of the encephalocele is the primary mode of treatment [12]. The objectives of the surgical procedure include: removal of non-functional herniated brain tissue, ensuring a secure closure of the dura, taking precautionary measures to prevent any tearing of the delicate sac, and averting any possible complications such as infection, bleeding, and leakage of cerebrospinal fluid, as well as reconstructing the cranium and facial features in order to achieve an aesthetically pleasing outcome [13].
The clinical presentation and management of an 8-day-old female neonate with frontonasal encephalocele are described in this case report.
Case presentation
Patient information
This is an 8-day-old Ethiopian female neonate presented with a frontonasal swelling since birth. She was born after 8 months of amenorrhea to a 24 year old Para III mother. Mother lives in the country side, where access to a healthcare facility is limited. She did not have an ANC follow-up. She did not take iron-folate supplementation, which is given to all pregnant women in Ethiopia during their antenatal follow-up. Otherwise, there is no maternal history of medical illness, drug usage, or giving birth to a child with a similar abnormality.
Clinical findings
Delivery was at local health center via spontaneous vaginal delivery to effect the delivery of 2200gm alive female neonate. The neonate cried immediately after birth. Neonate was referred to Zewditu Memorial Hospital with the compliant of swelling over the forehead since birth. There is no history of fever, abnormal body movement, or leakage from the swelling.
Upon examination, the neonate was active with stable vital signs. The occipitofrontal circumference was 35 cm. A 6 by 4 cm soft, cystic lobulated swelling between the eye globes over the upper tip of the nasal bridge was present. The neonate was awake and alert, with complete moro, sustained sucking, and strong grasp reflexes. She moved all her extremities. The pupils were mid-sized and reactive bilaterally. There was no spinal deformity.
Diagnostic assessment
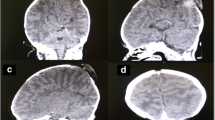
Complete blood count, serum electrolyte, liver enzymes, bilirubin level, creatinine level, coagulation profile were all within normal range. Computed tomography showed an anterior basal skull defect associated with bilateral medial frontal lobe encephalocele and associated cystic structures, suggesting large frontonasal meningoencephalocele (Fig. 1).

A Coronal and B sagittal CT scans of the brain showing an isodense lesion with defect on the anterior basal skull
Therapeutic intervention
Under general anesthesia, patient in supine position, bifrontal skin flap was raised and craniotomy was done. Extradural dissection of the encephalocele was done, and the defect was identified. Then, dura was opened and dissection was undertaken till the base of the defect is identified. The external swelling was dissected circumferentially, separating the dysplastic tissue from the skin. Dysplastic tissue was cauterized and removed. A split calvarial bone graft was used for defect construction. Then, dura was closed with water tight closure. Finally bone was replaced and fixed. Skin was closed in 2 layers after leaving epidural drain. The plastic surgery team closed the external wound of the encephalocele with primary closure (Fig. 2).

Fourth postoperative day
Follow-up and outcome
Antibiotics were given for 5 days. She had a smooth postoperative recovery period. She was discharged with follow-up to the neurosurgery clinic with acceptable cosmesis to the parents.
Discussion
An extrusion of the skull contents outside the skull through a herniated sac is known as an encephalocele [12]. Occipital, basal, convexity, and sincipital (anterior) encephaloceles are the subcategories into which encephaloceles are divided [2]. Suwanwela and Suwanwela have further divided the sincipital group into three types, which include frontoethmoidal encephaloceles, interfrontal encephaloceles, and those encephaloceles that are associated with craniofacial clefts. A protrusion of the contents of the skull through a breach at the point where the frontal and ethmoidal bones meet is referred to as a frontoethmoidal encephalocele. Frontoethmoidal encephalocele can be divided further into three distinct categories: nasofrontal, nasoethmoidal, and nasoorbital [1].
According to different studies, encephalocele occurs in 1 in 5,000 to 10,000 live births [3,4,5]. In one systematic review and meta-analysis carried out in Africa, it was shown that there was a significant variation in the prevalence of encephalocele in various African countries. High birth prevalence of encephalocele was found in Ethiopia (0.02%) among with others [14]. In Southeast Asia, some regions of Russia, and Central Africa, anterior encephaloceles are the most prevalent type of encephaloceles found, occurring in up to 1 in 3,500 live births [6].
Many theories have been postulated for the development of an anterior encephalocele [15]:
An initial bone defect results in the failure of the ethmoidal plate to enclose around the olfactory nerve eventually leading to herniation of the brain.
High pressure in the embryo's ventricles which might push the growing brain through the bone structures that are not yet fully formed.
The theory suggested by Jeffrey-Saint Hillaire (most accepted): "The skull is made up of two parts, the endochondral skull base and the intramembranous skull top." When the baby is born, the frontal and ethmoid bones are held together, but at three months of gestation, they are apart. Thus, a vulnerable area occurs between the frontal and ethmoid bones and that a congenital abnormality could cause a herniated encephalocele.
The uncommon encephaloceles which appear through the sphenoid bone may be due to a persistent craniopharyngeal canal and extrusion of brain matter or meninges through it.
The sphenoid bone's inability to form the appropriate ossification centers could also be taken into consideration as a possible origin for encephaloceles in this area.
Encephalocele development is also thought to be influenced by both genetic and environmental risk factors, including maternal illnesses, drugs consumed, or inadequate vitamin B12, folic acid, or mineral supplements during the first trimester of pregnancy [8]
In most cases, the diagnosis is clinical. The diagnosis is frequently clear, particularly when there is clinically or palpably detectable cerebral pulsation. The size and location of the cranial defect through which the herniation passes can be determined using plain radiographs of the skull and face. Encephaloceles can frequently be linked to other disorders of the central nervous system, including hydrocephalus. Although CT scans with the proper brain windows and three-dimensional reconstruction provide the greatest assessment of the diagnosis and disease anatomy, ultrasound may be useful in estimating the size of the ventricle [16].
An inter-disciplinary approach is the best way to manage these abnormalities [17]. If there is no CSF leak associated with the encephalocele, treatment can be elective. However, a crucial treatment factor to take into account is the encephalocele mass's possible impact on the growth of the craniofacial bone, which could necessitate earlier intervention. The primary mode of intervention is direct surgical repair [12].
In the past, the surgical treatment of encephalocele involved a two-step method, beginning with severance of the connection inside the cranium and followed by reshaping of the deformed face [18]. In a recently developed one-stage operation, combined nasal-coronal approach with frontal craniotomy is done. By employing this procedure, it is possible to reshape the frontal bone flap by eliminating the trigonocephalic protuberance, addressing any external skull deformities, and restoring an attractive appearance with the potential for nasal enhancement [19].
The objectives of the surgical procedure include: removal of non-functional herniated brain tissue, ensuring a secure closure of the dura, taking precautionary measures to prevent any tearing of the delicate sac, and averting any possible complications such as infection, bleeding, and leakage of cerebrospinal fluid, as well as reconstructing the cranium and facial features in order to achieve an aesthetically pleasing outcome [13]. The location, size, composition, and presence of any additional congenital anomalies all affect the prognosis. Compared to posterior encephalocele (55%), where a critical brain parenchymal structure may have herniated through the skull defect, the survival rate in anterior encephalocele is higher, approaching 100% [20].
Conclusion
A congenital or acquired condition, an encephalocele, is described as the herniation of brain matter through a hole in the skull. In Africa, the incidence of encephalocele at birth is comparably high. Ethiopia is one of the countries with a very high burden of neural tube defects. Interventions including folic acid fortification and supplementation, and preconception evaluation are needed to be implemented to tackle this high level of neural tube defect prevlance. The management of patients with encephalocele requires multidisciplinary team participation.
Availability of data and materials
Not applicable.
Abbreviations
- ANC:
-
Antenatal care
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
References
Suwanwela C, Suwanwela N. A morphological classification of sincipital encephalomeningoceles. J Neurosurg. 1972;36(2):201–11. https://doi.org/10.3171/jns.1972.36.2.0201.
Humphreys RP, et al. Encephalocele and dermal sinuses. In: Cheek WR, Marlin AE, McLone DG, et al., editors. Pediatric neurosurgery: surgery of the developing nervous system. 3rd ed. Philadelphia: WB Saunders; 1994. p. 96–103.
Dhirawani RB, Gupta R, Pathak S, Lalwani G. Frontoethmoidal encephalocele: Case report and review on management. Ann Maxillofac Surg. 2014;4(2):195–7.
Songür E, Mutluer S, Gürler T, Bilkay U, Görken C, Güner U, Celik N. Management of frontoethmoidal (sincipital) encephalocele. J Craniofac Surg. 1999;10(2):135–9.
Tanwir A, Bukhari S, Shamim MS. Frontoethmoidal encephalocele presenting in concert with schizencephaly. Surg Neurol Int. 2018;9:246. https://doi.org/10.4103/sni.sni_242_18.
Jiminez DF, Barone CM. Encephaloceles, meningoceles, and dermal sinuses. In: Albright AL, Pollack IF, Adelson PD, editors. Principles and Practice of Pediatric Neurosurgery. 2nd ed. New York, NY: Thieme; 2008. p. 233–53. https://doi.org/10.1055/b-0034-56392.
Ssentongo P, Heilbrunn ES, Ssentongo AE, Ssenyonga LVN, Lekoubou A. Birth prevalence of neural tube defects in eastern Africa: a systematic review and meta-analysis. BMC Neurol. 2022;22(1):202. https://doi.org/10.1186/s12883-022-02697-z.
Yucetas SC, Uçler N. A retrospective analysis of neonatal encephalocele predisposing factors and outcomes. Pediatr Neurosurg. 2017;52(2):73–6. https://doi.org/10.1159/000452805.
Bower C, D’Antoine H, Stanley FJ. Neural tube defects in Australia: trends in encephaloceles and other neural tube defects before and after promotion of folic acid supplementation and voluntary food fortification. Birth Defects Res A Clin Mole Teratol. 2009;85(4):269–73. https://doi.org/10.1002/bdra.20536.
Santos LM, Lecca RC, Cortez-Escalante JJ, Sanchez MN, Rodrigues HG. Prevention of neural tube defects by the fortification of flour with folic acid: a population-based retrospective study in Brazil. Bull World Health Organ. 2016;94(1):22–9. https://doi.org/10.2471/BLT.14.151365.
Naidich TP, Altman NR, Braffman BH, McLone DG, Zimmerman RA. Cephaloceles and related malformations. AJNR Am J Neuroradiol. 1992;13(2):655–90.
Gump WC. Endoscopic endonasal repair of congenital defects of the anterior skull base: developmental considerations and surgical outcomes. J Neurol Surg B Skull Base. 2015;76(4):291–5.
Koko M, Ismail N, Shehu B, Lasseini A. Surgical outcome of anterior encephalocele: report of two cases and review of literature. J Surg Rehabil. 2020. https://doi.org/10.31487/j.JSR.2019.01.08.
Oumer M, Demissie KA. Birth prevalence of encephalocele in Africa: a systematic review and meta-analysis. BMJ Paediatrics Open. 2021;5:1001117. https://doi.org/10.1136/bmjpo-2021-001117.
Bhagwati SN, Mahapatra AK. Encephalocele and anomalies of the scalp. Pediatric neurosurgery. London: Churchill Livingstone; 1999. p. 101–20.
Holmes AD, Meara JG, Kolker AR, Rosenfeld JV, Klug GL. Frontoethmoidal encephaloceles: reconstruction and refinements. J Craniofac Surg. 2001;12(1):6–18. https://doi.org/10.1097/00001665-200101000-00003.
Velho V, Naik H, Survashe P, Guthe S, Bhide A, Bhople L, et al. Management strategies of cranial encephaloceles: a neurosurgical challenge. Asian J Neurosurg. 2019;14:718–24. https://doi.org/10.4103/ajns.AJNS_139_17.
Lello GE, Sparrow OC, Gopal R. The surgical correction of fronto-ethmoidal meningo-encephaloceles. J Cranio-Maxillo-Facial Surg. 1989;17(7):293–8.
Mahatumarat C, Rojvachiranonda N, Taecholarn C. Frontoethmoidal encephalomeningocele: surgical correction by the Chula technique. Plast Reconstr Surg. 2003;111(2):556–67. https://doi.org/10.1097/01.PRS.0000040523.57406.94.
Mesterton CB. Om medfödt hjernbråck (Doctoral dissertation, Universitetet i Uppsala). 1855.
Acknowledgements
Not applicable
Funding
No funding was required for this work.
Author information
Authors and Affiliations
Contributions
Both authors participated in the writing of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Patient’s parent has provided informed written consent to publish the case report with any accompanying images.
Competing interests
The author reports no conflicts of interest in this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kibru, E.A., Mogessie, Y.G. A rare case report of frontoethmoidal encephalocele in a neonate. Egypt J Neurosurg 38, 77 (2023). https://doi.org/10.1186/s41984-023-00256-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41984-023-00256-3