
Abstract
Background
Lesser wing of sphenoid joins the body of sphenoid by two roots which are separated by the optic canal. Optic canal is a communicating channel between orbit and middle cranial fossa, forming a passage for the ophthalmic artery and optic nerve. Considering the delicate neurovascular structure that traverses the narrow confines of the optic canal, knowledge of the morphometry, anatomical variations of this canal and their relations becomes an important part of diagnostic medicine and surgical management.
Objective
The aim of the study was to conduct morphometric analysis and document variations of optic canal in north Indian population and study its sexual dimorphism.
Material and Method
Type of Study Cross-sectional study. Sample size 200 Computerized tomography head axial section scans from picture archiving and communication system. The computer-assisted measurements of optic canal parameters were obtained on both right and left sides. Statistical analysis Unpaired t-test, paired t-test and ANOVA were applied.
Result
Optic canal of 110 males, 90 females were examined. The overall cranial opening diameter, orbital opening diameter and length of optic canal in males were 4.34 ± 0.74, 3.17 ± 0.58 and 9.81 ± 1.62 and in females they were 3.99 ± 0.71, 2.97 ± 0.59 and 9.38 ± 2.02 respectively.
Conclusion
Significant gender difference is seen in cranial and orbital opening diameter, and distance from midsagittal plane. No statistical significant difference is observed in right and left side parameters. A thorough knowledge of the normal dimensions of optic canal is important for evaluation and management of cases of optic nerve decompression.
Similar content being viewed by others


Introduction
Optic canal (OC) lies between the two roots of lesser wing of sphenoid which are attached to the body of sphenoid by a thin, flat anterior root and thick triangular posterior root. It form a communicating channel between the orbit and middle cranial fossa and transmits the optic nerve, ophthalmic artery, meningeal sheaths and sympathetic nerve fibres [1].
Studies have been done in the past regarding dimensions of OC like its length, diameter of cranial and orbital openings of the canal, area of the canal, height and other parameters [2,3,4,5,6]. Our study focuses on describing variables in different sex and age groups.
The comprehension of the typical variants will be useful in surgical field to correct optic nerve decompressions (trans-cranial and trans-sphenoidal routes), lesions/tumors of the orbit, schwannoma of optic nerve, neoplasms, osseous lesions and ophthalmic artery aneurysms and provide a better and safe route to access this region [7,8,9,10,11].
When one considers the delicate neurovascular structures that traverse their narrow confines, knowledge of the anatomical variations of these canal and their relations become an important part of diagnostic medicine and surgical management. The aim of the study was to conduct morphometric analysis and document variations of optic canal in north Indian population and study its sexual dimorphism.
Materials and methods
This is a cross sectional study in which 200 Computerized tomography (CT) head in axial sections were examined. Institutional Ethics Committee clearance has been taken. These scans were collected from picture archiving and communication system of a tertiary care hospital catering to a large North Indian population. We studied high-resolution images from a Philips Brilliance 64 channel multi-detector CT scanner where we visualized spiral head CT scans in axial plane between 0.9 and 2.00 mm thickness (range of detector: 0.55–7.5 mm).
Sample size calculation
Sample size was calculated estimating for two sample comparison of means [3].
Test Ho: m1 = m2, where mi is the mean in population 1, and m2 is the mean in population 2.
Assumption
Estimated required sample size: n1 = 94, n2 = 94. So minimum 94 scans of each male and female subjects was required.
Subject selection
Inclusion: We had selected every 10th scan from last 5 year PACS system of our Institute. CT head of 110 males and 90 females, with age ranging from 1 to 80 years without any anomaly which can change anatomy of foramen were included. The foraminal parameters were obtained on both right and left sides using computer-assisted measurements.
Exclusion: Technically suboptimal scans, skull base fractures, disease or tumour involving skull base, any congenital anomaly involving skull base, and scans of subjects less than 1 year of age were excluded.
Variables measured
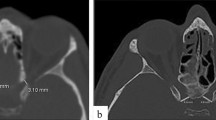
Width of cranial opening, orbital opening and width at the centre of OC- a line was drawn between inside surface of medial and lateral wall such that, the points selected were analogous to the data under consideration. For example: for calculation of mid-width: mid points of medial and lateral walls were marked, and a line was drawn between them to measure length (Figs. 1 and 2).

CT head axial plane showing optic canal


CT head axial section showing measured variables of the optic canal: a width at orbital opening, b width at the centre of optic canal, c width at cranial opening, d optic canal length at the middle, e distance from mid-sagittal plane
Length of the OC—centre of the orbital and cranial openings of OC were marked and a line was drawn in between (Fig. 2). Length of intracanalicular portion of optic nerve was taken as the length of optic canal measured from centre of orbital opening to the centre of cranial opening as previously documented by Slavian et al. [6].
Distance from Mid-Sagittal Plane—the mid-point of the inner surface of medial wall was marked, and a perpendicular was drawn to the MSP (Fig. 2).
Statistical analysis
Descriptive statistics were used to analyse the results. Discrete (categorical) data were summarized in proportions and percentages (%), while continuous as mean and SD. Arithmetic mean, standard deviation, Unpaired and Paired t-test, One way ANOVA were calculated in the present study. In our study, we have taken 95% confidence interval and P value < 0.05–Significant, < 0.01—Highly Significant.
Results
A total of 400 optic canals were analysed (220 males and 180 females), with age ranging from 1 to 80 years. Observing CT scan in axial plane, lateral wall of OC was seen formed laterally by the anterior clinoid process and medially by the sphenoethmoidal cell of the posterior ethmoid sinus and the sphenoid sinus. We observed sphenoethmoidal air cell also known as onodi air cell in 4% cases unilaterally and 1% cases bilaterally. The overall cranial opening diameter, orbital opening diameter and length of OC in males was 4.34 ± 0.74, 3.17 ± 0.58 and 9.81 ± 1.62 and in females was 3.99 ± 0.71, 2.97 ± 0.59 and 9.38 ± 2.02, respectively (in mm). The mean ± SD of all the variables measured are shown in Table 1.
Statistically significant difference was seen among males, between left and right side for width at mid length (p value = 0.039). In females, no significant difference was seen between left and right side parameters of OC.
Statistically significant difference was seen between males and females in width of cranial side (p value = 0.001), and of orbital side (p value = 0.013) and in the distance from MSP (p value < 0.001).
Comparative age-related morphometry in males and females is shown in Table 2.
Discussion
Optic canal is the narrowest part at the apex of orbit that allows for the passage of optic nerve from orbit to the middle cranial fossa. Accurate knowledge of its dimensions in males, females on the right and left side and in different populations is imperative for evaluation and management of different optic neuropathies. Radiographic description of OC was first described by Winckler in 1901, and its oblique position was observed by Rhese [12]. Recent advances in endoscopic endonasal Optic nerve decompression and other surgical approaches to optic nerve as in transfrontal craniotomy, orbitotomy and trans-ethmoidal and spheno-ethmoidal surgeries have emphasized the need for precise information about the morphological and metrical details of the optic canal, specific to each population [11,12,13,14]. This is especially in light of the fact that no age-specific studies have been found in literature to the best of our knowledge.
Shape of optic canal OC shape has been quoted in previous studies as hour-glass, cone or cylindrical shaped [15, 16]. In the present study, optic canal was observed to be cylindrical in shape with width slightly broader towards its cranial end in all the cases. Width at the centre of the optic canal was more on the right side than the left in males and the difference was statistically significant.
Orbital and cranial openings of optic canal Statistically significant difference was seen in width on cranial side between males and females (p value = 0.001), width on orbital side (p value = 0.013) and in the distance from MSP (p value < 0.001). These dimensions were smaller in females than in males and orbital opening was seen as the narrowest point of OC. Previous studies have documented similar difference in the volume and area of OC between females and males [17,18,19]. The smaller orbital opening diameter in females could predispose to partial or complete obstruction of subarachnoid space as seen in patients with papilledema, normal tension glaucoma and thus rapid progression of disease seen more commonly in females [17, 19,20,21,22]. These measurements are extremely important in light of the fact that OC connects the intracranial cerebrospinal fluid space with the subarachnoid space of the intraorbital part of optic nerve with the OC subarachnoid space size being the narrowest [23]. Recent observations suggest that circulatory dysfunction of cerebrospinal fluid may be a factor responsible for normal tension glaucoma and papilledema [24,25,26]. Pircher et al. described narrower OC area in Caucasian normal tension glaucoma patients compared with subjects without optic nerve disease. The importance of documenting OC dimensions in these patients is more as with a narrow optic canal there may be a discontinuity of the cerebrospinal fluid flow between the intracranial and orbital subarachnoid space in these patients [17].
OC Length In patients with traumatic neuropathy the prior knowledge of length of OC is important to decide what length of OC must be opened [27,28,29]. Length of OC as seen in previous studies varies from 5 to 15 mm [26, 29] (Table 3), comparable to the present study.
Similar to Berlis et al., [4] in present study, we measured the distance from mid-point of medial wall of optic canal to mid-sagittal plane and it was 10.91 ± 1.55 in males and 9.70 ± 1.99 in females.
General morphometrical parameters of OC Comparing the morphometric results of our study with previous studies, values of all parameters in the present study were slightly lower than the studies done in the past. The only comparable study was a CT-based study done on Indian population by Kalthur et al. [3]. The lower values of parameters in the present study may be because of racial differences and that most of the previous studies have been done on dried skull (Table 4).
Right–left asymmetry Zhang et al. commented that optic canal asymmetry is not uncommon and documented larger dimensions of right optic canal as compared to the left. Asymmetry of OC may affect risk factors of papilledema severity and explain cases of unilateral or asymmetric papilledema and possibly asymmetric glaucoma [28]. Contrarily, in the present study, no statistically significant differences were seen on right and left side. Sinanoglu et al. [6] in their study also observed no asymmetry in laterality in the same sex.
Anatomical variations Studies in the past have documented a variation called as keyhole anomaly which is seen as a result of the absence of the floor at cranial opening (3.3% cases). Another variant documented is figure-of-eight OC, with a bony spicule creating a separate canal for the ophthalmic artery [4]. The only variant observed in our study is the Onodi air cell, an anatomical variant of the paranasal sinuses, important due to its close proximity to the optic nerve, observed in 5% of scans in our study.
Morphometric data obtained from out study shows that despite variability there are approximate anatomic standards derived from our population that can be used in neurosurgical practice. Since injury to any part of the optic pathway result in visual defects, knowledge of the gross features of the OC and related structures is very important for surgeons. Also required is the accurate knowledge of both openings of optic canal its, length and shape before performing any surgical procedure on the canal for decompression, removal of tumour or approaches to sella.
Limitations In the present study, neuro-arterial relations of OC have not been assessed. Also distance of OC from landmarks like nasal bone tip, middle point of tuberculum sellae and root of columella nasi which are useful for endoscopic surgeries have not been documented.
Strength The present study provides a comprehensive morphometry of OC in our population, particularly in relation to different age groups, which has not been reported in any previous studies to the best of our knowledge.
Conclusions
In males, values of all measured parameters of OC were higher in comparison with female and the differences were statistically significant. No statistical significant difference is observed in right and left side parameters. A thorough knowledge of the normal dimensions of OC is important for evaluation and management of disease involving the canal. This study provides a clear understanding of OC and its morphometric variations in the North Indian population.
Availability of data and materials
The data analysed during the current study available in the institutional PACS system.
Abbreviations
- OC:
-
Optic canal
- CT:
-
Computerized tomography
References
Standring SM. Gray’s anatomy. 39th New York: Elsevier Churchill Livingstone; 2005. p. 462–6.
Radunovic M, Vukcevic B, Radojevic N, Vukcevic N, Popovic N, Vuksanovic-Bozaric A. Morphometric characteristics of the optic canal and the optic nerve. Folia Morphol. 2019;78(1):39–46.
Kalthur S, Periyasamy R, Kumar S, Gupta C, D’souza AS. A morphometric evaluation of the optic canal: comparative study between CT study and direct anatomic study. Saudi J Med Med Sci. 2015;3:204–8.
Berlis A, Putz R, Schumacher M. Measurements and variations in the region of the optic canal CT and anatomy. Radiology. 1992;32(9):436–40.
Ugradar S, Goldberg R, Rootman D. Anatomic variation of the entrance of the optic canal into the orbit. Orbit. 2019;38(4):305–7.
Slavin KV, Dujovny M, Soeira G, et al. Optic canal: microanatomic study. Skull Base. 1994;4:136–44.
Liu X, Zhou C, Zhang G, Lin Y, Li S. CT anatomic measurement of the optic canal and its clinical significance. Zhonghua Er Bi Yan Hou Ke Za Zhi. 2000;35(4):275–7.
Hart CK, Theodosopoulos PV, Zimmer LA. Anatomy of the optic canal: a computed tomography study of endoscopic nerve decompression. Ann Otol Rhinol Laryngol. 2009;118:839–44.
Govsa F, Erturk M, Kayalioglu G, Pinar Y, Ozer MA, Ozgur T. Neuro-arterial relations in the region of the optic canal. Surg Radiol Anat. 1999;21:329–35.
Housepian EM. Microsurgical anatomy of the orbital apex and principles of transcranial orbital exploration. Clin Neurosurg. 1978;25:556–73.
Di Somma A, Cavallo LM, de Notaris M, Solari D, Topczewski TE, Bernal-Sprekelsen M, Enseñat J, Prats-Galino A, Cappabianca P. Endoscopic endonasal medial-to-lateral and transorbital lateral-to-medial optic nerve decompression: an anatomical study with surgical implications. J Neurosurg. 2017;127(1):199–208.
Hammerschlag SB, O’Reilly GVA, Mohammad HN. Computed tomography of optic canal. AJNR. 1981;2:593–4.
Jiang P-F, Dai X-Y, Lv Y, Liu S, Xiao-Yan M. Imaging study on the optic canal using sixty four-slice spiral computed tomography. Int J Clin Exp Med. 2015;8(11):21247–51.
Abdulmannan DM. Successful surgical management of a patient with traumatic optic neuropathy: a case report. Cureus. 2022;14(1):e21685. https://doi.org/10.7759/cureus.21685.
Guseva YA, Denisov SD. Structure of the optic canal in human ontogenesis. Ann Anat. 2006;188(2):103–16.
Sinanoglu A, Orhan K, Kursun S, Inceoglu B, Oztas B. Evaluation of optic canal and surrounding structures using cone beam computed tomography: considerations for maxillofacial surgery. J Craniofac Surg. 2016;27(5):1327–30.
Pircher A, Montali M, Berberat J, Remonda L, Killer HE. The optic canal: a bottleneck for cerebrospinal fluid dynamics in normal-tension glaucoma? Front Neurol. 2017;8:47.
Friedrich RE, Bruhn M, Lohse C. Cone-beam computed tomography of the orbit and optic canal volumes. J Craniomaxillofac Surg. 2016;44(9):1342–9.
da Silva FV, Ferreira-Pileggi BC, Rossi AC, Prado FB, Alexandre R. Freire Morphometric analysis of the optic canal and the superior orbital fissure in a Brazilian sample – study in CT scans. Eur J Anat. 2023;27(2):165–70.
Bidot S, Clough L, Saindane AM, Newman NJ, Biousse V, Bruce BB. The optic canal size is associated with the severity of papilledema and poor visual function in idiopathic intracranial hypertension. J Neuroophthalmol. 2016;36(2):120–5.
Killer HE, Jaggi GP, Miller NR, Huber AR, Landolt H, Mironov A, et al. Cerebrospinal fluid dynamics between the basal cisterns and the subarachnoid space of the optic nerve in patients with papilloedema. Br J Ophthalmol. 2011;95(6):822–7.
Killer HE, Miller NR, Flammer J, Meyer P, Weinreb RN, Remonda L, et al. Cerebrospinal fluid exchange in the optic nerve in normal-tension glaucoma. Br J Ophthalmol. 2012;96(4):544–8.
Drance S, Anderson DR, Schulzer M; Collaborative Normal-Tension Glaucoma Study Group. Risk factors for progression of visual field abnormalities in normal-tension glaucoma. Am J Ophthalmol 2001; 131(6): 699–708.
Killer HE, Laeng HR, Flammer J, Groscurth P. Architecture of arachnoid trabeculae, pillars, and septa in the subarachnoid space of the human optic nerve: anatomy and clinical considerations. Br J Ophthalmol. 2003;87(6):777–81.
Wostyn P, De Groot V, Van Dam D, Audenaert K, Killer HE, De Deyn PP. Glaucoma and the role of cerebrospinal fluid dynamics. Invest Ophthalmol Vis Sci. 2015;56(11):6630–1.
Hayreh SS. Pathogenesis of oedema of the optic disc (papilloedema). Br J Ophthalmol. 1964;48:522–43.
Li J, Ran QS, Hao B, Xu X, Yuan HF. Transsphenoidal optic canal decompression for traumatic optic neuropathy assisted by a computed tomography image postprocessing technique, Hindawi. J Ophthalmol. 2020. https://doi.org/10.1155/2020/1870745.
Zhang X, Lee Y, Olson D, et al. Evaluation of optic canal anatomy and symmetry using CT. BMJ Open Ophthalmol. 2019;4:e000302.
Akdemir G, Tekdemir I, Altın L. Transethmoidal approach to the optic canal: surgical and radiological microanatomy. Surg Neurol. 2004;62:268–74.
Manisalco JE, Habal MB. Microanatomy of the optic canal. J Neurosurg. 1978;48:402–6.
Peyman G, Sanders D, Goldberg M. Principles and practice of ophthalmology. Philadelphia: W.B. Saunders Co; 1980. p. 3–87.
Lang J, Gehmann G. Form development of optic canal, measurements and position with respect to cranial bones. Verh Anat Ges. 1976;70:567–74.
Orhan Mağden A, Kaynak S. Bilateral duplication of the optic canals. Ann Anat. 1996;178:61–4.
Acknowledgements
Not applicable
Funding
The research did not receive any specific grant from funding agencies in the public, commercial, or not for-profit sectors.
Author information
Authors and Affiliations
Contributions
Plagiarism checked by authors. ES was responsible for conceptualization, methodology, investigation and writing of Initial Draft. NP was responsible for validation of the study, visualization and writing—review and editing of the final draft. SN was instrumental in investigation and provision of study materials. AG did the formal analysis and helped with data curation. RB was responsible for overall supervision and project administration. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript. Separate document is attached.
Corresponding author
Ethics declarations
Ethics approval and consent of participate
Institutional Ethics Committee (IEC) clearance has been taken (letter number 563/RMLIMS/2019 dated 3/5/2019).
Consent for publication
Manuscript and its images does reveal any individuals name of any other details.
Competing interests
All authors declared that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sthapak, E., Pasricha, N., Narayan, S. et al. Optic canal: a CT-based morphometric study in north Indian population. Egypt J Neurosurg 38, 46 (2023). https://doi.org/10.1186/s41984-023-00220-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41984-023-00220-1