
Abstract
Background
Ependymomas are neuroectodermal tumors that grow from the ependymal cells of the ventricles or the central canal of the spinal cord. When the ependymoma is anaplastic, extramedullary, intradural and multifocal, it is a very rare anatomical entity, same as case described by us.
Case presentation
A 44-year-old man had been admitted to our hospital for progressive paralysis of both legs over the past 5 weeks. Contrast-enhanced MRI showed intradural extramedullary tumor at T11 with cord compression and an other more little tumor at T6 level, also intradural and extramedullary. The largest lesion was completely removed by laminectomy. Histology documented an anaplastic ependymoma. Contrast-enhanced brain and spinal MRI showed the results of the previous surgery.
Conclusion
Multifocal intradural extramedullary anaplastic ependymomas are very rare entity. Surgery is the main treatment that can improve prognosis, while radiotherapy is useful, after surgery, in the treatment of residues, recurrences, anaplastic transformations, metastases and multifocal lesions.
Similar content being viewed by others


Background
Ependymomas are neuroectodermal tumors arising from the ependymal cell of the ventricles and the central canal of the spinal cord and account about 4–6% of all tumors of the central nervous system. They are the most common tumors of the spinal cord, accounting for about 60%, and because they originate from ependymal cells, their usual localization is intramedullary [1, 10]. Their most common spinal location is at the level of the conus medullaris, cauda equina and terminal filum; less commonly it is dorsal and cervical; less commonly malignant; rarely it is intradural extramedullary; and rarely multifocal in spine. At the level of the spinal cord, ependymomas are often benign and, rarely, multifocal in spine [1,2,3, 8, 11]. We describe very rare case report of multifocal intradural extramedullary anaplastic ependymoma with a great T11 lesion and a little T6 lesion, also extramedullary and intradural and review the literature.
Case presentation
A 44-year-old man was admitted to our division of Neurosurgery in November 2020.
His medical history has been characterized by worsening weakness in both legs (score: 2/5) over the past 5 weeks and urinary incontinence over the past 5 days. Sensory examination revealed a reduction in sensation along both legs. Thoracic contrast-enhancement MRI revealed a well-circumscribed intradural and extramedullary mass of T11 with a dural attachment on the dorsal side of the spinal canal (Fig. 1), moreover, revealed the presence of another millimeter lesion at T6 level, also intradural and extramedullary (Fig. 2). The T11 tumor occupied the canal for 80% of the space and compressed the spinal cord towards the left anterior part of the spinal canal. In MRI, both lesions were hyso-hypointense on T1-weighted images, hyperintense on T2-weighted images and reinforced after gadolinium administration. The patient underwent a T10–T12 laminectomy for resection of T11 tumor. At the opening of the dura, there was the presence of an intradural extramedullary mass that had adhered to the sheet of the spinal pia mater. A total resection without damage to the spinal cord was performed, with central emptying of the lesion using an ultrasound surgical aspirator and the operating microscope.

Sagittal T2-weighted without gadolinium (A), sagittal T1-weighted (B) and axial T2-weighted gadolinium-enhanced (C) views of preoperative magnetic resonance imaging (1.5T) displaying the intradural extramedullary D11 ependymoma with spinal cord compression displaced ventrally

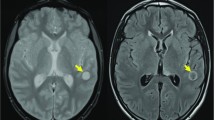
Sagittal T2-weighted (A) and axial T2-weighted (B) views of preoperative magnetic resonance imaging without gadolinium enhanced displaying other little localization in T6 of ependymoma
Pathological study revealed fragments of highly cellular glial neoplasm consisting of ependymal elements, sometimes with a solid pattern, with evidence of perivascular rosettes, presence of vascular proliferation and areas of necrosis (Fig. 3). The phenotype of neoplastic cells was: GFAP+, Olig2−, EMA focal+, protein S100+, CD99 *, SOX10−, synaptophysin−, absence of overexpression of the p53 protein. The final conclusion was anaplastic ependymoma (grade III, WHO). After the surgery, the patient showed a marked improvement in legs (score: 4/5) and normalization of urinary function. After 6 weeks, the patient received radiotherapy between T6 and cauda equina with a total dose of 5000 cGy. After 3 months of follow-up, the patient presented himself intact neurologically and contrast-enhancement spinal MRI showed absence of recurrence and stability of T6 lesion (Fig. 4).

Histology of our anaplastic ependymoma. A Increased mitotic activity and cellular anaplasia are readily evident in this image. B Microvascular proliferation. The proliferating endothelial cells practically occlude the lumen. C The tumor cells are arranged around a blood vessel creating a perivascular pseudorosette

Sagittal T1-weighted (A) and axial T2-weighted (B) views of post-operative magnetic resonance imaging with gadolinium enhanced displaying T11 completely excised
Discussion
Multifocal intradural and extramedullary anaplastic ependymoma of the spinal cord is a very rare anatomo-pathological entity.
From the literature, we find only 28 cases of intradural extramedullary ependymomas described, excluding ours. They were 21 females and 7 males; age was between 11 and 87 (average: 45.32; median: 46). The localization was in 15 cases thoracic, 3 cervical, 3 lumbar and 1 cervical–thoracic, in 6 cases were multifocal. Our case was very rare pathological entity, because it had various rare findings together, in fact ours ependymoma was: intradural, extramedullary, anaplastic and multifocal. Only 3 cases were described same as ours (Table 1). The etiopathogenesis was much discussed among the authors. Some, such as Duffau et al. in 2000, leaned towards a hormonal theory following the predominance of female sex in the patient population [5]. Other authors, the majority, did not accept the hormonal theory due to the presence of males among the patients and supported the theory of an origin from ependymal ectopic cells that remained trapped in the dural layers during the closure of the neural tube. This theory was supported by the fact that this type of tumor presented sometimes an attachment to the pial layer similar to an implant base from which tumor growth started [9, 10, 12]. The symptomatology of the lesion depended on its location and the degree of compression on the spinal cord or nerve roots.
In all cases, MRI showed a well delineated intradural and extramedullary mass, hyperintense on T2-weighted images and hypo-hysointense on T1-weighted images and reinforced after gadolinium administration, except in the case of Graca et al. where the lesion was not reinforced after gadolinium administration, such that it looked like an arachnoid cyst [6, 14]. However, for their radiological characteristics, in most cases, as in our case, these malignant tumors were confused with spinal meningiomas or neurinomas, especially when they had an extradural component, as in the case of De Bonis et al. [4, 14].
Intraoperatively, these tumors were encapsulated with mild adhesions to the pial layer, except in 6 cases where adhesions were important. Indeed, Robles et al. and Guppy et al. described a vascular lesion with pial infiltration (similar to our case) [7]; Graves et al. and Iunes et al. described a tumor infiltrating the arachnoid membrane that required a fine dissection between the tumor and the spinal cord [8]; Li et al. and Krisman et al. on the other hand, described a tumor with tenacious adhesions with medulla that required a small amputation [10]. From the pathological point of view, we have found 7 cases of primary anaplastic Ependymoma, as in our case. The treatment considered by the various authors for the 28 cases found was very variable. All cases of benign ependymoma underwent complete surgical resection without additional treatment as recommended by et al.; while the 7 cases of primary malignant tumors, they were managed by the authors in various ways. Katoh et al. and Olive et al. after surgery, did not perform radiotherapy obtaining a favorable prognosis even though the follow-up period described was only a few months [9]. The group of Shurmans, Kinsman, Guppy and Chakravorty performed a complete resection and post-operative radiotherapy at the surgical site, as in our case [7, 10, 12]; Case et al., after complete resection of the anaplastic tumor, intended to perform radiotherapy but the patient refused the treatment, but after a year he had recurrence of the disease which was removed surgically followed radiotherapy to the whole central nervous system, with death after a month [3, 4, 12]. Regarding the formation of metastases in other levels of the spinal cord, we have found 2 cases. Some authors, such as Shurmans et al. hypothesized a migration of neoplastic cells from the primary tumor following the direction of the CSF circulation. In this way, they could explain why recurrences or metastases, in all cases reported in Table 1, occurred in a higher level of the spinal cord than in the primary intradural extramedullary ependymoma [8, 12, 13]. Regarding recurrences, they occurred in 7 cases: 5 cases were recurrences from grade II (WHO) ependymoma, while 2 were from grade III (WHO) ependymoma. All recurrences had anaplastic histology (grade III, WHO). Some authors have hypothesized that the recurrence was due to residual neoplastic cells that have undergone anaplastic transformation over time, without however explaining a precise mechanism. In our opinion, about this question, in literature there are very little information.
Conclusion
Multifocal intradural extramedullary anaplastic ependymomas are very rare entities. They should be considered in the differential diagnosis of extramedullary intradural spinal lesions. The main treatment is complete surgical resection which clearly improves the prognosis. Radiotherapy plays an important role after surgery for the treatment of residues, recurrences, anaplastic transformation, metastases and multifocal lesions.
Availability of data and materials
The data and material of this manuscript are available and are in the archive of the Department of Neurosurgery of the “Casa Sollievo della Sofferenza” Hospital, San Giovanni Rotondo, Italy.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- GFAP:
-
Gliofibrillar acid protein
- WHO:
-
World Health Organization
- cGy:
-
Centi-gray
References
Brotchi J, Fischer G. Spinal cord ependymomas. Neurosurg Focus. 1998;4: e2.
Cerase A, Venturi C, Oliveri G, De Falco D, Miracco C. Intradural extramedullary spinal anaplastic ependymoma. Case Illus J Neurosurg Spine. 2006;5:476.
Chakravorty A, Frydenberg E, Shein T, Ly J, Earls P, Steel T. Multifocal intradural extramedullary anaplastic ependymoma of the spine. J Spine Surg. 2017;3(4):727–31.
De Bonis P, Montano N, Cioni B, Colosimo C, Lauriola L, Papacci F, et al. Primary extramedullary extradural ependymoma of the thoracic spine mimicking a schwannoma. J Neurol Neurosurg Psychiatry. 2009;80(5):579–81.
Duffau H, Gazzaz M, Kuhas M, et al. Primary intradural extramedullary ependymoma: case report and review of the literature. Spine. 2000;25(15):1993–5.
Graca J, Gultasli N, d’Haene N, Brotchi J, Salmon I, Baleriaux D. Cystic extramedullary ependymoma. AJNR Am J Neuroradiol. 2006;27(4):818–21.
Guppy KH, Hou L, Moes GS, Sahrakar K. Spinal intradural, extramedullary anaplastic ependymoma with an extradural component: case report and review of the literature. Surg Neurol Int. 2011;2:119.
Iunes EA, Stavale JN, de Cassia Caldas Pessoa R, Ansai R, Onishi FJ, de Paiva Neto MA, et al. Multifocal intradural extramedullary ependymoma Case report. J Neurosurg Spine. 2011;14(1):65–70.
Katoh S, Ikata T, Inoue A, Takahashi M. Intradural extramedullary ependymoma. Spine. 1995;20(18):2036–8.
Kinsman M, Callahan J, Hattab EM, Coehn-Gadol AA. Extramedullary spinal ependymomas: a diagnostic challenge and review of the literature. Clin Neurol Neurosurg. 2011;113(8):661–4.
Robles SG, Saldana C, Boto GR, Martinez A, Zamarron AP, Jorquera M, et al. Intradural extramedullary spinal ependymoma: a benign pathology? Spine. 2005;30(9):E251–4.
Schuurmans M, Vanneste JA, Verstegen M, van Furth WR. Spinal extramedullary anaplastic ependymoma with spinal and intracranial metastases. J Neurooncol. 2006;79(1):57–9.
Takashi M, Koichi I, Yu-ichiro O, Masao U, Masahiro I, Toshiki Y. Intradural extramedullary spinal ependymoma: a case report of malignant transformation occurring. Asian Spine J. 2013;7(2):139–42.
Koeller K, Shih Y. Intradural extramedullary spinal neoplasm: radiologic-pathologic correlation. Radiographics. 2019;39:468–90.
Acknowledgements
The authors thank the patient, who gave consent for the publication, the hospital that made the data and materials available.
Funding
There is no funding for this manuscript.
Author information
Authors and Affiliations
Contributions
All authors of this manuscript participated. CDB: creator and writer of study and final check; RG: acquisition of consents, data and materials; LG: second final check.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In this manuscript, there are ethical approval e patient’s consent to participate. The name of the “Ethics Committe” is “Casa Sollievo della Sofferenza Ethics Committe”. It met and approved the study on 11 January 2021 (progressive number: 2/2021). They can be found in the archive of Department of Neurosurgery in Hospital “Casa Sollievo della Sofferenza”, San Giovanni Rotondo, Italy.
Consent for publication
Authors and patient give their consent for publication for this manuscript; it can be found in the archive of Department of Neurosurgery in Hospital “Casa Sollievo della Sofferenza”, San Giovanni Rotondo, Italy.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
De Bonis, C., Gazzeri, R. & Gorgoglione, L. Multifocal thoracic intradural extramedullary anaplastic ependymoma: case report and review of the literature. Egypt J Neurol Psychiatry Neurosurg 59, 157 (2023). https://doi.org/10.1186/s41983-023-00757-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00757-w