
Abstract
Background
Cervical cancer remains a public health problem worldwide, especially in sub-Saharan Africa. There are challenges in timely screening and diagnosis for early detection and intervention. Therefore, studies on cervical cancer and cervical intraepithelial neoplasia suggest the need for new diagnostic approaches including microRNA technology. Plasma/serum levels of microRNAs are elevated or reduced compared to the normal state and their diagnostic accuracy for detection of cervical neoplasms has not been rigorously assessed more so in low-resource settings such as Uganda. The aim of this systematic review was therefore to assess the diagnostic accuracy of serum microRNAs in detecting cervical cancer.
Methods
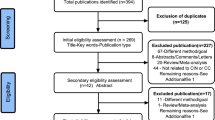
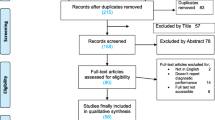
We will perform a systematic review following the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) statement. We will search for all articles in MEDLINE/PubMed, Web of Science, Embase, and CINAHL, as well as grey literature from 2012 to 2022. Our outcomes will be sensitivity, specificity, negative predictive values, positive predictive values or area under the curve (Nagamitsu et al, Mol Clin Oncol 5:189-94, 2016) for each microRNA or microRNA panel. We will use the quality assessment of diagnostic accuracy studies (Whiting et al, Ann Intern Med 155:529-36, 2011) tool to assess the risk of bias of included studies. Our results will be reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Diagnostic Test Accuracy studies (PRISMA-DTA). We will summarise studies in a flow chart and then describe them using a structured narrative synthesis. If possible, we shall use the Lehmann model bivariate approach for the meta analysis
Use of the review results
This systematic review will provide information on the relevance of microRNAs in cervical cancer. This information will help policy makers, planners and researchers in determining which particular microRNAs could be employed to screen or diagnose cancer of the cervix.
Systematic review registration
This protocol has been registered in PROSPERO under registration number CRD42022313275.
Similar content being viewed by others

Background
Worldwide, there were an estimated 770,828 incident cervical cancer cases in 2020 [1]. Cervical cancer is the second most common cancer among women aged 30 to 45 years of age worldwide [2]. It has been reported that cervical cancer accounts for more than 270 000 deaths annually, 85% of which occur in developing countries [3] especially in sub-Saharan Africa [4, 5]. Cervical Cancer stands at 43/100,000 cancer cases in East Africa [6], and in Uganda over 4,000 new cases are recorded annually and 58% of these result into death [7, 8]. A well-proven way to prevent cervical cancer is to screen and detect pre-cancers before they can turn into invasive cancer [3]. Cervical cancer is a very treatable disease when diagnosed early before advancement [6]. However, only 5% of women in low and middle-income countries undergo cervical cancer screening [8]. The current approaches to cervical cancer screening and diagnosis include visual inspection with acetic acid, Pap smear cytology, colposcopy, and histology. However, Pap smear, the most widely used screening method, is limited by its low accuracy (sensitivity and specificity), compared with newer DNA-based methods, especially in identifying cancer in dysplastic squamous and glandular cells of the cervix. New methods of cervical cancer screening that are less costly and user-friendly suit for a developing country’s contexts [8].
The research gap
There are a number of biomarkers that have been studied, many of which are associated with cervical cancer or cervical intraepithelial neoplasia, but yet to be evaluated as potential early indicators for cancer or cervical intraepithelial neoplasia. MicroRNAs are easily quantified in blood and standardised laboratory methods can easily be developed for their quantification. MicroRNAs belong to a novel category of small non-coding RNA molecules that interconnect to target mRNA to either degrade or modify it [9]. They catalyse mRNA cleavage by inhibiting its translation processes [10]. They have 22 to 24 nucleotides [11, 12]. MicroRNAs were previously thought to originate from tumour cells, but currently, it is known that they can exist in body fluids, especially blood [13, 14]. Recent evidence suggests that exosomal microRNAs in liquid biopsies like blood have the potential to improve prognostic and diagnostic workup in cancer [15].
Specifically for cervical cancer Allegra et al. [16] and Anindo and Yaqinuddin [17] revealed that microRNAs are expressed both in cancerous tissues [18] and in serum [19]. As a result, serum concentrations of microRNAs have been proposed as diagnostic and prognostic monitoring tools for cancer [20]. Evidence strongly points at microRNAs being prognostic of cervical cancer [9, 19, 21,22,23,24,25,26,27,28]. Clearly, microRNAs are the future of cervical cancer screening and diagnosis. Several studies on premalignant lesions indicate that microRNAs are involved at every stage during the development of invasive cervical cancer [29,30,31,32,33]. Multiple studies have shown that a number of microRNAs are upregulated during the progression to cervical cancer [34]. For instance, miR10a has been shown to have an increased expression during the development of cervical cancer [35,36,37] as well as miR20b [35, 37, 38], miR9 [35, 37, 38], miR16 [35, 36, 38] and miR106a [35, 36, 38]. From a systematic review by Gao et al [34], miR16, miR106a and miR21 are equally upregulated and are associated with progression from intermediate stages to cervical cancer. MiR21 has specifically been implicated by a number of studies to be upregulated during cervical carcinogenesis [35, 39,40,41,42].
Different authors however report different sensitivity and specificity values for different microRNAs in respect to cervical cancer detection. In a view of having new non-invasive, user-friendly, accurate, and standardisable tests, it is necessary to conduct a systematic review, to assess the diagnostic accuracy of different serum microRNAs in the detection of cervical neoplasms. This systematic review will therefore determine the diagnostic accuracy of individual serum or plasma microRNAs or microRNA panels in detecting cervical intraepithelial neoplasia or cervical cancer in women of reproductive age globally.
Methods
We developed a protocol a priori following the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) recommendations [43] and registered it in the PROSPERO database, number CRD42022313275. In drafting the final report, we will follow the Preferred Reporting Items for Systematic Reviews and Meta-analysis for Diagnostic Test Accuracy (PRISMADTA) [44, 45].
Review question
What is the diagnostic accuracy of individual serum/plasma microRNA or microRNA panels in detecting cervical cancer compared to histology (gold standard) among women of reproductive age worldwide?
Eligibility criteria
Study design eligibility criteria
We shall include all prospective and retrospective cohorts, cross-sectional, and case-control that report diagnostic accuracy of serum microRNAs or panels of microRNAs in the detection of cervical intraepithelial lesions or cervical cancer. Also, in the meta-analysis, we shall include those diagnostic test accuracy studies that adhered to the STARD (Standards of Reporting Diagnostic Accuracy Studies) [46]. We will exclude all studies done on nonhuman participants or those that did not report measures of diagnostic accuracy as required by STARD.
Population and condition under study
We will include all those studies that quantified serum microRNAs in symptomatic or asymptomatic women aged 18 years and above globally, as a diagnostic or screening test for cervical intraepithelial neoplasia or cervical cancer (Table 1).
Exposure/index tests
We will include those studies that quantified blood-based microRNAs from women receiving cervical cancer screening/diagnostic services (Table 1).
Comparison
The comparison gold standard or reference test will be histological results (grades) for cervical intraepithelial neoplasia or cervical cancer. No any other tests like clinical assessment will be considered (Table 1).
Outcomes
Our outcome will be measures of diagnostic accuracy (sensitivity, specificity, negative predictive values, or positive predictive values) for each reported microRNA (Table 1).
Study design
We shall include observational studies amenable to diagnostic accuracy studies, mainly cross-sectional, case-control as well as experimental designs like randomised trials, cluster randomised trials and quasi-experimental designs (Table 1).
Timeframe
We shall include primary studies carried out within a 10-year period, from 2012 to 2022 (Table 1).
Search strategy
Data sources
The data sources will include databases, institutional websites, grey literature and contacting authors. To identify all the studies, we will search MEDLINE through the PubMed platform, Web of Science, Embase through the Ovid platform, CINAHL, and Scopus. We will also search for grey literature such as conference papers, technical reports, theses, and dissertations in Google Scholar, Google, OpenGrey, ProQuest Dissertations & Theses, and British Library EThos. The authors will search each database from 2012 to 2022.
We will also screen through reference lists of included studies for additional eligible studies that may not be identified by the search. Systematic reviews will also be used to identify additional primary studies.
Electronic search
The electronic search will explore the combinations of the keywords covering the PICOS elements. The population component will include the words “Uterine cervical neoplasms*” [Mesh] OR “Cervical cancer*” [tw] OR “Human uterine cancer*” [tw] OR “SCC” [tw] OR “Cancer of the cervix*” [tw] OR “Cervical intraepithelial neoplasia*” [tw] OR “CIN” [tw].
The intervention component will include: “Circulating MicroRNA” [Mesh] OR “Circulating microRNAs*”[tw] OR “Circulating miRNAs” [tw] OR “Circulating serum microRNAs*”[tw] OR “Circulating serum miRNAs*”[tw] OR “Serum microRNAs*”[tw] OR “Serum miRNAs*”[tw] OR “Biomarkers*”[tw] OR “Blood*”[tw] OR “microRNAs*”[tw].
For the comparator, there will be no specific terms since they are already considered in the description of the population.
The outcome component will include the words “Early Detection of Cancer*” [Mesh] OR Diagnosis*[tw] OR “Diagnostic value*” [tw] OR “Diagnostic utility*” [tw] OR Sensitivity* [tw] OR Specificity*[tw] OR Specific*[tw] OR Sensitive*[tw] OR “up regulated*” [tw] OR “Down regulated*” [tw] OR “increased*” [tw] OR “Decreased*” [tw] OR “positive predictive value*” [tw]. OR “Negative predictive value*” [tw].
We will not include specific study designs in the search. We shall instead apply this in the eligibility criteria. The full search string is available in Table 2.
We will combine keywords, MESH terms and their synonyms, and these will be divided into three components. All the search components will be combined with the Boolean operators “AND” while the keywords within each component will be combined with “OR.” There will be no language restrictions for this review. We will run the searches just before the final analyses to retrieve the most recent studies eligible for inclusion.
To assess the feasibility of this review, we piloted this search in PubMed and it yielded 5,333 titles and abstracts. We sorted these by relevance and screened the first 500 for which we considered 26 (1%) as potentially eligible for data extraction (Table 2).
Selection of studies
Two reviewers (FS and RA) will perform duplicate and independent data extraction. Screening will be a two-step process with initial title/abstract screening followed by retrieval of full-texts and their screening. In any case, a discrepancy will be solved by either a third reviewer (EAO) or by consensus. We will provide a list of excluded full-text articles with reasons for exclusion as an appendix of the final report.
Data items, extraction, and management
We will develop a data extraction form, and this will be piloted initially to achieve a good level of agreement between the data extractors. Two reviewers (OM and AD) will independently extract data from all eligible articles. The following data will be extracted:
-
Study characteristics: author, year of publication, country, study design, sample size, clinical/study setting, number of dropouts with reason, and funding source.
-
Population characteristics: inclusion/exclusion criteria and patient demographics such as age as well as comorbidities.
-
Laboratory testing: index testing method, type of sample (e.g. whole blood, serum or plasma), and units of measurement. Type of microRNA(s) studied
-
Gold standard: Histological confirmation or rule out of cancer.
-
Outcomes: sensitivity, upregulated, downregulated, increased, decreased, specificity, the predictive value of positivity and negativity.
We will also extract and report the 2×2 tables (describing true and false positives and negatives) from each included study.
Risk of bias and methodological quality assessment
Two researchers will independently assess for the risk of bias using the quality assessment of diagnostic accuracy studies [47]. This widely recognised tool evaluates the risk of bias of diagnostic test accuracy research across four domains including patient selection, index test, reference standard and flow and timing. Application of this tool involves summarising the review question, tailoring the tool to the review, generating review-specific guidelines, constructing a flow diagram for each primary study and finally assessing the risk of bias and other concerns regarding applicability.
Minimising bias in selection and extraction of data from included studies
A second reviewer (AAK) will validate the electronic search by performing a second and independent search in PubMed using the same search strategy. The second reviewer will also screen all articles that will be excluded by the first pair of reviewers. We will resolve any disagreements among reviewers during screening, selection, abstraction, and risk of bias assessment through consensus or third-party reviewer (EAO) where the need arises.
Minimising publication bias
By including both published and unpublished data from multiple sources, we shall be able to minimise publication bias. However, we shall investigate for publication bias by visually inspecting a funnel plot, but only when there are more than 10 studies. We shall not search trial registries for unpublished diagnostic accuracy studies.
Statistical analyses and evidence synthesis
An overview of the available studies will be summarised in the flow chart and tabulated. We will describe data from eligible studies in a structured narrative synthesis. It is in this narrative synthesis that we will summarise the article author, year of publication, setting, study designs, sample size and population, type of laboratory index and reference tests, and diagnostic test accuracy outcomes.
Otherwise, we will use the Lehmann model bivariate approach for the meta-analysis. This will only be conducted if a given microRNA type was reported by more than two studies. We will derive summary receiver operating characteristic curves (SROC) for those specific microRNAs using the diagnostic odds ratio as the main outcome measure. We will also derive pooled sensitivity, specificity as well as areas under the curve (AUCs) for those specific microRNAs.
Heterogeneity assessment
We will inspect forest plots to initially assess heterogeneity and then check for individual study results in the ROC space. We expect potential sources of heterogeneity to include the year of publication, the country where the study was carried out, intervention types, and outcome measures. Heterogeneity will be statistically quantified using the I2 statistic and tested for significance using Cochran’s Q.
Handling of missing data
For variables that are needed but found either missing or not reported, we plan to label them as not reported, “NR”. Thereafter, we shall seek clarification from the authors on a case-by-case basis. We do not intend to apply any secondary analyses on such missing data.
Reporting the review findings
We will report the findings of this review in line with the PRISMA statement. The first table will summarise the author, publication year, study designs, participants, microRNA test details, sample types (serum or plasma) and the gold standard (reference test) used. These will be histological grades of cervical cancer or cervical intraepithelial lesions. The second table will capture the observed outcomes for each microRNA. These will include sensitivity, specificity, negative predictive value, positive predictive value, increased/upregulated, decreased/downregulated or unaffected.
Confidence in cumulative evidence
The review authors shall employ the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach to rate the certainty of evidence in primary studies. This will be done by considering the risk of bias and performing heterogeneity tests. Then we shall rate evidence as high, moderate low or very low.
Knowledge translation
To begin with, we will publish a scientific paper in an open access peer-reviewed and indexed journal relevant to the field of cervical cancer diagnostics. Also, the authors will attend and present results from this review at both local and international scientific conferences. We will engage relevant stakeholders including decision makers, patient groups, oncologists, researchers and PhD students who are currently studying microRNAs in cervical cancer, to deliberate on the policy options.
Preliminary findings
We have tabulated five example studies that potentially meet our eligibility criteria. All were identified from our PubMed search (Table 3). These studies were published between 2014 and 2021, all conducted in China. All these studies were case-control designs and addressed the diagnostic accuracy of serum microRNAs in cervical cancer or cervical intraepithelial neoplasia.
Discussion
Cervical cancer is a big health challenge all over the world, but much of it is felt in low and middle-income countries. The good news is that it can be dealt with once diagnosed at an early stage, i.e. when still at the stage of cervical intraepithelial neoplasia. This calls for accurate and user friendly tests that are easily taken up by both the patients and the health care providers. MicroRNAs are the best candidates to save the world from such a dilemma. What we do not know, however, is the diagnostic accuracy of these microRNA and which exact ones can be used by health care providers.
By answering these questions, we will have a better understanding of where these microRNAs could fit in the current screening/diagnostic strategies for cervical cancer. In particular, these microRNAs could be used as stand-alone screening tests or in conjunction with others, in a new algorithm, or together with the existing ones. This information will be of value to policy makers, planners and researchers in determining which ones and how these microRNAs could be employed to screen for cancer of the cervix.
Availability of data and materials
All the data generated from this review will be available from the corresponding author upon meaningful request.
Abbreviations
- CIN:
-
Cervical intraepithelial neoplasia
- microRNA:
-
Micro ribonucleic acid
- Pap:
-
Papanicolaou test
- PCR:
-
Polymerase chain eeaction
- VIA:
-
Visual inspection with acetic acid
- WHO:
-
World Health Organization
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Vänskä S, Luostarinen T, Lagheden C, Eklund C, Kleppe SN, Andrae B, et al. Differing age-specific cervical cancer incidence between different types of human papillomavirus: implications for predicting the impact of elimination programs. Am J Epidemiol. 2021;190(4):506–14.
WHO. Assessing national capacity for the prevention and control of noncommunicable diseases: report of the 2019 global survey. World Health Organisation. 2020.
Anorlu RI. Cervical cancer: the sub-Saharan African perspective. Reprod Health Matters. 2008;16(32):41–9.
Denny L, Quinn M, Sankaranarayanan R. Screening for cervical cancer in developing countries. Vaccine. 2006;24:S71–S7.
Sankaranarayanan R. Screening for cancer in low-and middle-income countries. Ann Glob Health. 2014;80(5):412–7.
Botha H, Cooreman B, Dreyer G, Lindeque G, Mouton A, Guidozzi F, et al. Cervical cancer and human papillomavirus: South African guidelines for screening and testing: clinical guidelines. South Afr J Gynaecol Oncol. 2010;2(1):23–6.
Sibiya N. Challenges to cervical cancer in the developing countries: South African context. Topics on Cervical Cancer with an Advocacy for Prevention. 2012.
Huang Y, Shen XJ, Zou Q, Wang SP, Tang SM, Zhang GZ. Biological functions of microRNAs: a review. J Physiol Biochem. 2011;67(1):129–39.
Farazi TA, Hoell JI, Morozov P, Tuschl T. MicroRNAs in human cancer. MicroRNA Cancer Regul. 2013;774:1–20.
Dai S, Lu Y, Long Y, Lai Y, Du P, Ding N, et al. Prognostic value of microRNAs in cervical carcinoma: a systematic review and meta-analysis. Oncotarget. 2016;7(23):35369.
Palanichamy JK, Rao DS. miRNA dysregulation in cancer: towards a mechanistic understanding. Front Genet. 2014;5:54.
Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci U S A. 2008;105(30):10513–8.
Turchinovich A, Weiz L, Langheinz A, Burwinkel B. Characterization of extracellular circulating microRNA. Nucleic Acids Res. 2011;39(16):7223–33.
Preethi KA, Selvakumar SC, Ross K, Jayaraman S, Tusubira D, Sekar D. Liquid biopsy: Exosomal microRNAs as novel diagnostic and prognostic biomarkers in cancer. Mol Cancer. 2022;21(1):1–15.
Allegra A, Alonci A, Campo S, Penna G, Petrungaro A, Gerace D, et al. Circulating microRNAs: new biomarkers in diagnosis, prognosis and treatment of cancer. Int J Oncol. 2012;41(6):1897–912.
Anindo MIK, Yaqinuddin A. Insights into the potential use of microRNAs as biomarker in cancer. Int J Surg. 2012;10(9):443–9.
Xie H, Zhao Y, Caramuta S, Larsson C, Lui W-O. miR-205 expression promotes cell proliferation and migration of human cervical cancer cells. PLoS One. 2012;7:e46990.
Ma Q, Wan G, Wang S, Yang W, Zhang J, Yao X. Serum microRNA-205 as a novel biomarker for cervical cancer patients. Cancer Cell Int. 2014;14(1):1–7.
Wittmann J, Jäck H-M. Serum microRNAs as powerful cancer biomarkers. Biochimica et Biophysica Acta (BBA)-Reviews on. Cancer. 2010;1806(2):200–7.
Luo M, Shen D, Zhou X, Chen X, Wang W. MicroRNA-497 is a potential prognostic marker in human cervical cancer and functions as a tumor suppressor by targeting the insulin-like growth factor 1 receptor. Surgery. 2013;153(6):836–47.
Wang C, Jiang T. MicroRNA-335 represents an independent prognostic marker in cervical cancer. Tumor Biol. 2015;36(8):5825–30.
He L, Wang H, Zhang L, Huang L, Li J, Xiong Y, et al. Prognostic significance of low DICER expression regulated by miR-130a in cervical cancer. Cell Death Dis. 2014;5(5):e1205.
Liang H, Li Y, Luo R-y, Shen F-j. MicroRNA-215 is a potential prognostic marker for cervical cancer. J Huazhong Univ Sci Technolog Med Sci. 2014;34(2):207–12.
Park H, Lee M-j, Jeong J-y, Choi MC, Jung SG, Joo WD, et al. Dysregulated microRNA expression in adenocarcinoma of the uterine cervix: clinical impact of miR-363-3p. Gynecol Oncol. 2014;135(3):565–72.
Wang N, Zhou Y, Zheng L, Li H. MiR-31 is an independent prognostic factor and functions as an oncomir in cervical cancer via targeting ARID1A. Gynecol Oncol. 2014;134(1):129–37.
Yang Y, Song K-l, Chang H, Chen L. Decreased expression of microRNA-126 is associated with poor prognosis in patients with cervical cancer. Diagn Pathol. 2014;9(1):1–5.
Shen S-n, Wang L-f, Jia Y-f, Hao Y-q, Zhang L, Wang H. Upregulation of microRNA-224 is associated with aggressive progression and poor prognosis in human cervical cancer. Diagn Pathol. 2013;8(1):1–7.
Rao Q, Zhou H, Peng Y, Li J, Lin Z. Aberrant microRNA expression in human cervical carcinomas. Med Oncol. 2012;29(2):1242–8.
Zheng Z-M, Wang X. Regulation of cellular miRNA expression by human papillomaviruses. Biochim Biophys Acta. 2011;1809(11-12):668–77.
Pedroza-Torres A, López-Urrutia E, García-Castillo V, Jacobo-Herrera N, Herrera LA, Peralta-Zaragoza O, et al. MicroRNAs in cervical cancer: evidences for a miRNA profile deregulated by HPV and its impact on radio-resistance. Molecules. 2014;19(5):6263–81.
Ribeiro J, Sousa H. MicroRNAs as biomarkers of cervical cancer development: a literature review on miR-125b and miR-34a. Mol Biol Rep. 2014;41(3):1525–31.
Sharma G, Dua P, Mohan AS. A comprehensive review of dysregulated miRNAs involved in cervical cancer. Curr Genomics. 2014;15(4):310–23.
Gao C, Zhou C, Zhuang J, Liu L, Liu C, Li H, et al. MicroRNA expression in cervical cancer: novel diagnostic and prognostic biomarkers. J Cell Biochem. 2018;119(8):7080–90.
Wilting S, Snijders P, Verlaat W, Jaspers AV, Van De Wiel M, Van Wieringen W, et al. Altered microRNA expression associated with chromosomal changes contributes to cervical carcinogenesis. Oncogene. 2013;32(1):106–16.
Pereira PM, Marques JP, Soares AR, Carreto L, Santos MA. MicroRNA expression variability in human cervical tissues. PLoS One. 2010;5(7):e11780.
Cheung TH, Man KN, Yu MY, Yim SF, Siu NS, Lo KW, et al. Dysregulated microRNAs in the pathogenesis and progression of cervical neoplasm. Cell Cycle. 2012;11(15):2876–84.
Li Y, Wang F, Xu J, Ye F, Shen Y, Zhou J, et al. Progressive miRNA expression profiles in cervical carcinogenesis and identification of HPV-related target genes for miR-29. J Pathol. 2011;224(4):484–95.
Zeng K, Zheng W, Mo X, Liu F, Li M, Liu Z, et al. Dysregulated microRNAs involved in the progression of cervical neoplasm. Arch Gynecol Obstet. 2015;292(4):905–13.
Xiao X, Wu Z-C, Chou K-C. A multi-label classifier for predicting the subcellular localization of gram-negative bacterial proteins with both single and multiple sites. PLoS One. 2011;6(6):e20592.
Shishodia G, Shukla S, Srivastava Y, Masaldan S, Mehta S, Bhambhani S, et al. Alterations in microRNAs miR-21 and let-7a correlate with aberrant STAT3 signaling and downstream effects during cervical carcinogenesis. Mol Cancer. 2015;14(1):1–13.
Bumrungthai S, Ekalaksananan T, Evans MF, Chopjitt P, Tangsiriwatthana T, Patarapadungkit N, et al. Up-regulation of miR-21 is associated with cervicitis and human papillomavirus infection in cervical tissues. PLoS One. 2015;10(5):e0127109.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647.
McInnes MD, Moher D, Thombs BD, McGrath TA, Bossuyt PM, Clifford T, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA. 2018;319(4):388–96.
Salameh J-P, Bossuyt PM, McGrath TA, Thombs BD, Hyde CJ, Macaskill P, et al. Preferred reporting items for systematic review and meta-analysis of diagnostic test accuracy studies (PRISMA-DTA): explanation, elaboration, and checklist. BMJ. 2020;370:m2632.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. Clin Chem. 2015;61(12):1446–52.
Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36.
Nagamitsu Y, Nishi H, Sasaki T, Takaesu Y, Terauchi F, Isaka K. Profiling analysis of circulating microRNA expression in cervical cancer. Mol Clin Oncol. 2016;5(1):189–94.
Acknowledgement
Not applicable.
Funding
This review is entirely funded by the authors. There is no external funding. We plan to use the existing library infrastructure and resources at Mbarara University of Science and technology as well as Makerere University.
Author information
Authors and Affiliations
Contributions
The corresponding author, FS, conceived the idea and developed the first draft of the protocol. Co-authors MO, DA, EN, RA, AAK, NN, JN, DT, and EAO refined the protocol, provided overall guidance in the entire write up and approved the final version prior to submission. All authors are accountable to all aspects of this protocol. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval is not required for this systematic review protocol.
Consent for publication
Not applicable.
Competing interests
We, the authors, declare that we do not have any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ssedyabane, F., Niyonzima, N., Ngonzi, J. et al. The diagnostic accuracy of serum microRNAs in detection of cervical cancer: a systematic review protocol. Diagn Progn Res 7, 4 (2023). https://doi.org/10.1186/s41512-023-00142-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41512-023-00142-4