
Abstract
Background
There is a lack of comprehensive national data on prevalence, geographical distribution of different species, and temporal trends in soil-helminthiasis (STHs). Therefore, this study aimed to provide a summary and location of the available data on STHs infection among preschool and school-age children in Ethiopia.
Methods
The search was carried out in Medline via PubMed, Scopus, Science Direct, Web of Science, and Google Scholar on data published between 1997 to February 2020 for studies describing the rate of STHs infection among preschool and school-age in Ethiopian. We followed the Patient, Intervention, Comparison, and Outcome (PICO) approach to identify the studies. Meta-regression was performed to understand the trends and to summarize the prevalence using the “metaprop” command using STATA software version 14.0
Results
A total of 29,311 of the 61,690 children examined during the period under review were infected with one or more species of intestinal parasites yielding an overall prevalence of 48% (95% CI: 43–53%). The overall pooled estimate of STHs was 33% (95% CI: 28–38%). The prevalence was 44% (95% CI: 31–58%) in SNNPR, 34% (95% CI: 28–41%) in Amhara region, 31% (95% CI: 19–43%) in Oromia region and 10% (95% CI: 7–12%) in Tigray region. Soil-transmitted helminths infection rate has been decreasing from 44% (95% CI: 30–57%) pre-Mass Drug Administration (MDA) era (1997–2012) to 30% (95% CI: 25–34%) post-MDA (2013–2020), although statistically not significant (p = 0.45). A lumbricoides was the predominant species with a prevalence of 17%.
Conclusion
Southern Nations Nationalities and Peoples Region, Amhara, and Oromia regions carry the highest-burden and are categorized to Moderate Risk Zones (MRZ) and therefore, requiring MDA once annually with Albendazole or Mebendazole. The prevalence of STHs decreased after MDA compared to before MDA, but the decline was not statistically significant. A. lumbricoides was the predominant species of STHs among preschool and school-age children in Ethiopia. The high prevalence of STHs observed in this review, underscores the need for better control and prevention strategies in Ethiopia.
Similar content being viewed by others


Background
Soil-transmitted helminths (STHs) infections are one of the most common infections in countries with limited resources. Globally, more than 4.5 billion people are at risk of infection and nearly 2 billion are infected with STHs [1, 2]. In contrast to other infectious diseases, infection due to STHs such as Ascaris lumbricoides, hookworm species, and Trichuris trichiura do not usually cause significant mortality rates; instead adapted to chronic illness and extended morbidity affecting poor people [3,4,5,6].
Transmissions of the STHs are mainly by eggs or larvae that are passed with feces of an infected person or hatched in the soil after defecation. Adult worms residing in the gut of an infected person produce thousands of eggs every day, which may contaminate environments or foods that lack adequate sanitation [7]. Additionally, climatic conditions of tropical and sub-tropical countries are suitable for the survival of STH eggs and larvae hatching and embryonated in warm temperature and adequate moisture soil [8]. Consequently, the complication of STH may cause gut blood losses, malabsorption of nutrients, loss of appetites, and anemia due to loss of iron and other important protein [9]. For instance, the outcome of the infection on the children results in serious problems such as anemia, growth retardation, impaired cognitive developments, school absenteeism, and disability-adjusted life-years lost [10, 11].
World Health Organization (WHO) has published comprehensive road map data in 2012 to combat Neglected tropical diseases (NTDs) by 2020. Mass Drug Administration (MDA) approach was also designed to undertake 75% coverage in all of the known endemic countries for STHs. The ideas of WHO was strengthened by the London declaration to control or eliminate other ten [10) NTDs in addition to the STHs [12, 13]. Recently, following WHO strategic plan, Ethiopia has launched a nationwide MDA to control STHs, which targets 17 million children within the age range of 5–14 years old. The Ethiopian Ministry of Health and WHO started deworming in 2013, of which approximately 6.8 million and 7.8 million pre-school children (PSAC) and school-age children (SAC) were treated, respectively. Even before the deworming program, the ministry of health has undertaken some other measures to control poverty-related diseases including STHs among the population at risk, particularly SAC. For instance, the implementation of a health extension program focusing on creating awareness on latrine construction and utilization and keeping personal and environmental hygiene among the community is one priority program since 2003/2004. However, current individual reports indicated that the prevalence of STHs in Ethiopia is not declining. A large-scale study conducted in Amhara regional state showed that the prevalence of STHs was 36.4% [14]. Another study in Jimma town showed that the prevalence of STHs among SAC was 49.0% [15]. A similar study also reported that the prevalence of STHs was 47% in the rural community of Ethiopia [16]. Nevertheless, numerous fragmented studies have been carried out on assessing the prevalence of STHs among preschool children (PSAC) and SAC in Ethiopia, but comprehensive nationwide data on the prevalence, geographic distribution of different species, and time trends of STHs are lacking. Therefore, this study aimed to provide a summary of prevalence, geographical location, and time trends of STHs among preschool and SAC to measure the impact of the ongoing control and preventive measures in the country. In addition, such an effort might help the government and other concerned bodies to focus on specific areas of high prevalence for further preventive measures such as chemotherapy and improved sanitation practices.
Methods
We used and were guided by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [17] guideline and checklist to carry out the current Systematic Reviews and Meta-analyses. The outcome of interest was the prevalence of STHs among PSAC and SAC in Ethiopia.
Search strategy
The search was carried out in Medline via PubMed, Scopus, Science Direct, Web of Science, and Google Scholar using searching terms such as “intestinal helminths’’, ‘’intestinal parasites’’, "soil-transmitted helminths”, ‘’STHs’’, ‘’ Strongyloides stercoralis '', ‘’Ascaris lumbricoides’’, ‘’ Trichuris trichiura'', '' Hookworms’’, ‘’preschool-age’’, ‘’school-age’’, “Ethiopia”. These key terms were combined using "AND" and "OR" Boolean operators. Medical Subject Headings (MeSH terms) were used to search relevant original articles in PubMed. Searching was carried out on articles published between 1997 to February 2020 and limited to English language and human studies. A manual search for additional relevant studies using references from retrieved articles and related systematic reviews was also performed to identify original articles we might have missed.
Endnote citation manager software version X9 for Windows was utilized to collect and organize search outcomes (into relevant and irrelevant studies) and for the removal of duplicate articles. We followed the PICO approach to identify the relevant articles:
-
Population (P): School-age children
-
Exposure (E): Presence of soil-transmitted helminths
-
Comparison (C): Preschool-age children
-
Outcome (O): Prevalence of soil-transmitted helminths.
Prevalence was calculated as the number of subjects positive for STHs in the study divided by the total number of participants in a study multiplied by 100.
Inclusion and exclusion criteria
We included observational studies conducted between 1997 to February 2020 which documented the baseline prevalence or incidence of STHs and studies published in the English language targeting both PSAC (< 5 years) and SAC (≥ 5 years). We excluded case reports, case series, studies that compared the sensitivity and specificity of different methods for diagnosis of STHs, and studies not reported either prevalence or incidence as an outcome of interest. This is due to those articles and/or reports will not adequately address the review objective. The current review didn’t include unpublished studies or grey literature.
Data abstraction and quality assessment
Following preliminary assessment and downloading of the abstracts by two authors, they were assessed for agreement with the inclusion criteria. Irrelevant articles (articles that were out of the scope of the study) were excluded after assessment of the abstracts unless it was unclear to classify articles into irrelevant based on abstracts, where we downloaded the full text for further clarity. Once articles were deemed to be relevant, the full text of the articles was downloaded for further detailed review. We extracted information on the name of the first author and year of publication, study design, gender, region of study, laboratory method identification of the parasites, total sample size, the number of positives for intestinal parasites in general, number of positive for STHs in particular, and quality score for quality assessment. The Grading of Recommendation Assessment, development, and Evaluation (GRADE) approach was used to assess the overall quality of evidence [18]. Studies were given one point each if they had probability sampling, larger sample sizes of more than 200, and repeated detection, and up to four points could be assigned to each study. We regarded publications with a total score of 3–4 points to be of high quality, whereas 2 points represented moderate quality and scores of 0–1 represented low quality.
Statistical analysis
We used forest plots to estimate pooled effect size and effect of each study with their confidence interval (CI) to provide a visual summary of the data. A random-effects model was used in this meta-analysis because of anticipated heterogeneity. Statistical heterogeneity among studies was expressed as the Cochrane’s Q test and I2, where a p < 0.05 and I2 values of 0, 25, 50, and 75% were considered as no, low, moderate, and high heterogeneities, respectively. Because we expected geographical variation and socio-economic contexts might differ radically across these studies, subgroup analysis based on the geography of the region, age children included, and year of publication. In addition to visual inspection for symmetry of the plot, we also used Begg's Funnel plot and Egger's regression test for quantitative evaluation of the possibility of publication bias. Meta-regression analysis was employed to identify the source of heterogeneity using regional states, age of children, publication years, and study design as covariates. All reported p values were 2-sided and were statistically significant if p < 0.05.
Results
Literature searches and selection
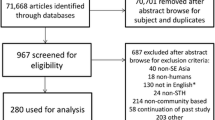
Our initial search of electronic databases such as Medline via PubMed, Scopus, Science Direct, Web of Sciences, and Google scholar yielded 953 articles and 3 articles manually from which 213 records remained after removing duplications. Upon screening the articles, 123 articles were further excluded; 112 were irrelevant because they were not specifically about PSACor SAC, 6 studies were about sensitivity and specificity of diagnosis of STHs, and 5 articles were not about humans. Upon further assessment for eligibility, 2 studies were excluded being review articles. Finally, 88 [6, 14, 16, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110] published studies between 1997 and February 2020 fulfilling the inclusion criteria were included in the final analyses (Fig. 1). The sample size of the included studies ranged from 100 [20] to 15,455 [14]. A total of 61,690 children with age of < 5 years (n = 5577) and ≥ 5 years (n = 55,731) or mix of both (n = 382) were recruited in the studies. Fifty-two percent (52%) of the study participants were male. The majority (83) of the studies were cross-sectional. Seventy-three studies were about STHs in SAC, thirteen were about preschool-age and the rest were studies that involved both PSAC and SAC. Thirty-five and twenty-four studies used Kato-Katz or in combination with other tools and formalin-ether concentration plus direct microscopic method for screening stools, respectively. Formalin-ether concentration techniques in 19 studies, direct wet mount method in 5 studies, McMaster in 4 studies, and Harada Mori (Test tube culture) technique in one study utilized as screening of stools. According to our quality assessment criteria, 43 publications were of high quality with a score of 3; 11 had a score of 2 indicating moderate quality; and the remaining 34 were of low quality with a score of zero or one (Table 1).

Flow diagram showing the selection process
The pooled prevalence estimate of intestinal parasites and heterogeneity
Eighty studies (88) studies consisting of 61,690 PSAC and SAC reported the proportion of intestinal parasitic infections. Out of these, 29,311 children were infected with one or more species of intestinal parasites giving the pooled prevalence estimate of 48% (95% CI: 43–53%) with considerable heterogeneity (χ2 = 17,303.64, p < 0.001; I2 = 99.50%). The prevalence of intestinal parasitic infection was 53% (95% CI: 38–67%), 50% (95% CI: 44–57%), 45% (95% CI: 35–54%) and 43% (95% CI: 29–58%) in Southern Nations Nationalities and Peoples Region (SNNPR), Amhara, Oromia, and Tigray regions, respectively (Fig. 2). We also did a subgroup analysis to see the influence of study design on prevalence. Interestingly enough, the prevalence was 48% (95% CI: 43–53%) for cross-sectional study design and therefore, the inclusion of other study designs does not influence the overall rate of infection (not shown).

Forest plot showing pooled prevalence of intestinal parasites among children according to regional states in Ethiopia
The overall prevalence estimate of soil-transmitted helminths (STHs) and heterogeneity
Soil-transmitted helminths detected in the studies were Ascaris lumbricoides, Hookworms, Trichuris trichiura, and Strongyloides stercoralis. A total of 19, 678 of the 61,690 children examined during the period under review were infected with one or more species of STHs yielding an overall prevalence of 33% (95% CI: 28–38%) with substantial heterogeneity (χ2 = 30,360.02, p < 0.001; I2 = 99.71%) (Fig. 3). The asymmetry of funnel plot visual inspection (Fig. 4) showed that the presence of publication bias which was statistically confirmed by Egger’s test (β = 16.7, [95% CI: 10.7–22.5]), p < 0.001 and Begg’s test p < 0.001.

Forest plot showing pooled prevalence of STHs

Publication bias assessment plot: Egger’s regression test (p < 0.0001) and Begg’s rank correlation (p < 0.001)
We did meta-regression analyses to search for the sources of heterogeneity. A univariate meta-regression between the prevalence of STHs and the age of children showed a statistically significant correlation (p = 0.003, Fig. 5). However, year of publications, (p = 0.076), regional states (p = 0.70) and study design (p = 0.23) did not show a statistically significant correlation as shown in Table 2.

Meta-regression of prevalence of STHs (log event rate) by Age
Sub-group analysis based on geographical region and age of children
Subgroup analysis showed that the prevalence of STHs was 44% (95% CI: 31–58%) in SNNPR, 34%(95% CI: 28–41%) in Amhara region, 31% (95% CI: 19–43%) in Oromia region and 10% (95% CI: 7–12%) in Tigray region as shown in Fig. 6. The age-related prevalence was 51% (95% CI: 45–56%) in SAC and 32% (95% CI: 20–44%) in PSAC (p = 0.003) as shown in Fig. 7. Subgroup analysis by publication year showed that the pooled prevalence of STHs between 1995 and 2012 years was 44% (95% CI: 30–57%) while, it was 30% (95% CI: 25–34%) for studies conducted between 2013 and 2020 years (Fig. 8). In summary, STHs were more common in SNNPR among SAC in studies published between 1990 and 2012 as shown in Table 3. We performed subgroup analysis based on study design and the result showed that the prevalence of STHs was 34% (95% CI: 29–39%) for cross-sectional study, 25% (95% CI: 23–28%), 4% (95% CI: 3–5%) for prospective study and 20% (95% CI: 15–26%) for case–control study (not shown). This indicates that the overall prevalence is almost the same as the prevalence of studies with cross-sectional study design and was not affected by other study designs.

Forest plot showing prevalence of STHs by region

Forest plot showing prevalence of STHs by age

Forest plot showing prevalence of STHs by year of publication
Prevalence of STHs by species
Ascaris lumbricoides
Eighty five studies consisting of 58, 234 children have reported that the pooled prevalence of A. lumbricoides was 17% (95% CI: 15–19%) with substantial heterogeneity (χ2 = 8961.94, p < 0.001; I2 = 99.06%). The prevalence was 27% (95% CI: 21–34%) in SNNPR, 14% (95% CI: 11–17%) in Amhara region, 15% (95% CI: 11–19%) in Oromia region and 6% (95% CI: 3–8%) in Tigray region (Additional file 1: Fig. S1). The age related prevalence of A. lumbricoides was 18% (95% CI: 15–20%) in SAC and 12% (95% CI: 8–17%) in PSAC (p = 0.06). The pooled prevalence of A. lumbricoides was 25% (95% CI: 19–31%) in studies published between 1997 and 2012 years and 14% (95% CI: 12–16%) between 2013 and 2020 years. A univariate meta-regression between prevalence and year of publications showed statistically significant correlation [β = −0.49 (95% CI: −1.1 to −0.07, p = 0.035)] (Additional file 1: Fig. S2). However, regional states [β: 0.046, (95% CI: −0.12 to 0. 0.22, p = 0.58)] and age of children [β: 0.52, (95% CI: −0.02 to 1.1, p = 0.06)] did not show a statistically significant relationship. Therefore, Ascaris lumbricoides was the most predominant species of STHs among Ethiopian children and significant decline in prevalence was observed over two decades (from late 1990s to 2020) (Table 4).
Trichuris trichiura
Seventy six studies included of 54,854 children have reported that the pooled prevalence of Trichuris trichiura was 6% (95% CI: 6–7%) with considerable heterogeneity (χ2 = 3766.86, p < 0.001; I2 = 98.01%). The pooled prevalence was 11% (95% CI: 11–13%) in SNNPR, 10% (95% CI: 8–13%) in Oromia region, 4% (95% CI: 3–4%) in Amhara region and 1% (95% CI: 0–2%) in Tigray region and 1 (Additional file 1: Fig. S3). The age related prevalence was also 7% (95% CI: 6–8%,) among SAC and 4% (95% CI: 2–6%) among PSAC (p = 0.24). The pooled prevalence of T. trichura was 14% (95% CI: 12–17%) in studies conducted between 1997 and 2013 years and 4% (95% CI: 4–24%) between 2013 and 2020 years. A univariate meta-regression between prevalence and year of publications showed statistically significant correlation [Β = − 0.78, (95% CI: − 1.5 to − 0.069, p = 0.03)] (Additional file 1: Fig. S4). However, regional states [β: 0.003, (95% CI: − 0.22 to 0. 0.23, p = 0.97)] and age of children [β: 0.46 (95% CI: − 0.29 to 1.2, p = 0.23)] did not show a statistically significant relationship. The bottom line is that the rate of infection of Trichuris trichiura among Ethiopian children decreased significantly after starting of MDA as detailed in Fig. 5. In addition, infection from Trichuris trichiura was more prevalent among children in SNNP region and Oromia region compared to other regions and also significant decline in prevalence was observed over two decades (Table 5).
Hookworms
Seventy six studies consisting of 54,854 children have also reported the pooled prevalence of Hookworms. Hence, the pooled prevalence on analysis was 12% (95% CI: 10–13%) with substantial heterogeneity (χ2 = 7920.16, p < 0.001; I2 = 99.05%). The pooled prevalence of hookworms was 12% (95% CI: 9–15%) in SNNPR, 16% (95% CI: 13–19%) in Amhara region, 6% (95% CI: 5–8%) in Oromia region, and 3% (95% CI: 2–4%) in Tigray region as shown in Additional file 1: Fig. S5. The age related prevalence of hookworms was 13% (95% CI: 11–15%) among SAC and 2% (95% CI: 1–3%) among PSAC (p = 0.01). The pooled prevalence of hookworms was 13% (95% CI: 9–15%) in studied conducted between 1997 and 2012 years and 11% (95% CI: 9–13%) in studies between 2013 and 2020 years.
A univariate meta-regression between prevalence and age of children showed statistically significant correlation [Β = 1.03, (95% CI: 0.27–1.8, p = 0.01)], (Additional file 1: Fig. S6A). Additionally, meta-regression of the prevalence and regional states [β: − 0.20, (95% CI: − 0.40 to − 0. 0.005, p = 0.045)], (Additional file 1: Fig. S6B) revealed a significant correlation. However, year of publication [β: − 0.09, (95% CI: − 0.79–0.61, p = 0.81)] did not show a statistically significant relationship. In summary, infection from hookworms was more prevalent among children in Amhara region compared to other regions and among SAC compared to PSAC (Table 6).
Strongyloides stercoralis
Twenty six studies consisting of 11,748 children have reported that the pooled prevalence of Strongyloides stercoralis was 1% (95% CI: 1–2%). The pooled prevalence of Strongyloides stercoralis was 3% (95% CI: 1–4%) in Amhara region, 1% (95% CI: 1–2%) in SNNPR, 1% (95% CI: 0–1%) in Oromia region and 0% (95% CI: 0–1%) in Tigray region as shown in Additional file 1: Fig. S7. The prevalence was 1% (95% CI: 1–2%) in SAC. The pooled prevalence of Strongyloides stercoralis was 1% (95% CI: 1–2%) in studies done between 1997 and 2012 years and 2% (95% CI: 1–2%) between 2013 and 2020.
A univariate meta-regression between prevalence and regional states showed statistically significant correlation [Β = − 0.30, (95% CI: − 0.56 to − 0.03, p = 0.03)] (Additional file 1: Fig. S8). However, year of publication [β: − 0.17, (95% CI: − 0.70 to 1.0, p = 0.70)] and age of children [β: − 0.02, (95% CI: − 0.96 to 0.92, p = 0.97)] did not show a statistically significant relationship. Therefore, Strongyloides stercoralis is more common among children in the Amhara region compared to other regions (Table 7). For further details, the summary of species-specific STHs presented in Table 8.
The intensity of STHs infection
Only 13 out of 88 studies included 5, 676 children reported about intensity of infection of STHs. Low intensity of infection of A. lumbricoides was observed in 16% (95% CI: 10–21%), (Additional file 1: Fig. S9) children. Moderate and high intensity of infections of A. lumbricoides were observed in 13% (95% CI: 7–19%), (Additional file 1: Fig. S10) and 6% (95% CI: 2–11%), (Additional file 1: Fig. S11) of children, respectively. Low, moderate and high intensity of infections of T. trichura were observed in 16% (95% CI: 12–20%), (Additional file 1: fig. S12), 3% (95% CI: 2–4%), (Additional file 1: Fig. S13), 1% (95% CI: 1–2%, (Additional file 1: Fig. S14) children, respectively. This review also showed that low, moderate and high intensity of infections of Hookworms were recorded in 20% (95% CI: 10–29%), (Additional file 1: Fig. S15), 4% (95% CI: 2–6%), (Additional file 1: Fig. S16) and 5% (95% CI: 0–11%), (Additional file 1: Fig. S17) children, respectively.
Regional distribution of eligible studies and risk zones (RZs) for STHs infections
The highest numbers of studies were reported from Amhara 36 (40.90%) and SNNPR 22(25%). These were followed by the Oromia region 20 (22.7%), Tigray 8 (9.1%), Benishangul-Gumuz region, and Addis Ababa city each with one (1.1%) study. None of the regions is classified as High-Risk Zone (HRZ) according to the world health organization (WHO) risks classification. SNNPR, Amhara, and Oromia regions recorded STH prevalence of 44%, 34%, 31%, respectively and are classified as moderate-risk zones (MRZs) while, the rest of the regions and cities recorded prevalence estimates ranging between 1 and 10% and are classified as Low-Risk Zones (LRZs).
Discussion
The purpose of the current systematic review and meta-analysis of STHs infections data analysis among Ethiopian children was to measure the impact of the ongoing control and preventive measures in the country and support the efforts undertaken to control and eliminate neglected tropical diseases (NTDs) by nurturing or supplementing useful national epidemiological data. Such studies have the potential to guide concerned bodies to focus their efforts in highly endemic areas. Although several studies have been published from different regions of Ethiopia on STHs with the earliest scientific literature dating back 1990s, the data on STHs infections remains unorganized and scattered. Therefore, organizing and locating information has the potential to inform and develop a comprehensive approach to control STH infections and target highly endemic areas with greater urgency.
The overall pooled estimate of STHs (33%) observed in the present review is in line with the study from south America 27.1% [118], but higher than the study done in Iran (9.48%) [119] and Côte d'Ivoire (19.1%) [120]. The prevalence is lower than studies from Nigeria (54.8%) and reports from other Sub-Sharan African countries (52.4 and 65.8%) [121]. The variation between the findings might be attributed to differences in sensitivity and specificity of diagnostic methodology, environmental factors such as soil moisture, humidity, temperature, and level of participants’ hygiene and sanitation. In addition, our review included more recent surveys that the ongoing MDA and Sustainable water, sanitation, and hygiene (WASH) programs decreased the prevalence of STHs in Ethiopian children unlike the systematic review from Nigeria which included old studies from the year 1985 [121].
Subgroup analysis of the current review also showed that STHs are more common in SNNPR, Amhara, and Oromia regions, although variation among the regional states was not statistically significant (p = 0.70). The majority of these infections are related to the low standard of living, poor socioeconomic status, poor personal hygiene, and poor environmental sanitation. The higher prevalence of STHs infection among children in SNNPR, Amhara and Oromia regions might be also related to the high rainfall, forest, and low temperature which favors the survival and transmission of the helminths in these regions. The lowest prevalence in Addis Ababa, the capital city of Ethiopia, might be due to an advanced lifestyle, good personal hygiene, and good quality of life.
Our review suggests that the risk of STH infections has decreased from 44 to 30% in studies conducted between 1997–2012 and 2013–2020 respectively, although the decline is not statistically significant (p = 0.45). Prevalence might have declined in some parts due to improvement in living conditions globally and expansion of major deworming efforts, including in Ethiopia. Nevertheless, the increase in population growth in Ethiopia is tremendous and therefore, might have increased the numbers infected and resulted in a slight decline in rate. It is also suggested that the widespread use of monotherapy of antihelminthic for deworming purposes might have facilitated the development of drug resistance and hence, decreased the rate of decline STHs in general and hookworms in particular [122, 123].
If environmental and behavioral conditions are not changed at the same time that the chemotherapy program is being implemented, the prevalence will tend to return to original pretreatment levels through reinfection and therefore, need a holistic approach [3, 123,124,125,126,127,128]. According to WHO risk categorization, our finding (33%) indicates that MRZ of STHs requires MDA once annually, specifically in SNNPR, Amhara, and Oromia regions.
Concerning the species of STH, A. lumbricoides was the predominant species with a prevalence of 17% indicating that about one in six of Ethiopian children is living with Ascariasis. The current prevalence of the parasite is higher than the findings from other countries such as Iran (0.75%) and Srilanka (2.8%) which indicated that indoor and outdoor biotic contamination of the living environment arising partly from improper disposal of human waste, and partly from the integration of the lives of humans and animals of Ethiopian community might account for the still-high rate of the infection in the country. The finding of the current review (17%) is in line with findings from South America (15.6%), studies conducted in the Amhara region, Ethiopia (16.8%), and the overall burden in Sub-Saharan African countries (15%) [129]. However, it was lower than the results from Nigeria (44.6%), Rwanda (38.6%), Uganda (43.5%) [130], Kenya (24.3%) [131], and previous estimates in Ethiopia (37%). The observed differences might be due to variation in some factors putting the population at risk of acquiring STHs such as geographical variations, the lifestyle of the community, soil humidity, and exposure to contaminated environments.
In the current review, the prevalence of A. lumbricoides significantly decreased from 25% in 1997–2012 to 14% in 2013–2020 (p = 0.006). There was a 49% decline in the prevalence of A. lumbricoides observed before the implementation of the MDA program in school children compared to post-MDA. This risk reduction might be related to improved sanitation, access to better water supply, improved personnel hygiene, or the higher efficacy of the available treatments against A lumbricoides [122]. In support of this, a local study conducted on the efficacy of albendazole and Mebendazole indicated that the drugs have 95% efficacy in decreasing the burden of the parasite in Ethiopia [132].
The pooled prevalence of 6% observed for T. trichiura was higher than the 1.9% and 3.4% reported from Uganda [119] and Rwanda [121], respectively. The present finding is, however, lower than the reports of the disease burden of Sub-Saharan Africa (13%) [106], Nigeria (18.2%) [110], and Cameroon (15.6%) [118]. This might be due to the geographical variations, the lifestyle of the community, soil humidity, and exposure to contaminated environments. Meta-regression analysis by year of publication revealed that the prevalence of T. trichiura decreased from 14% in 1997–2012 to 4% in 2013–2020 (p = 0.03). The reason behind the substantial decrease in the prevalence of T. trichiura in the country during the study period might be due to the synergistic effect of overall improvements in sanitation, personnel hygiene, and deworming programs.
The finding of the current review showed that the prevalence of hookworms was 12% indicating that the current finding is lower than other studies conducted in Nigeria (32.7%) [121] and Uganda (18.5%) [130]. However, it was higher than studies conducted in Kenya (0.4%) [131], Rwanda (1.8%) [133] and Cameroon (3.9%) [134]. In general, increments of prevalence in our data might be attributed to the re-infection rate, low coverage or unequal distribution of MDA in all regions of the country, level of poverty (walking bare of the foot), and lack of good quality of life. For instance, most Ethiopians are living in the rural area and engaged in agriculture. Engagement in agricultural pursuits remains a common denominator for adult human hookworm infection, which might serve as a reservoir for reinfection of children [128]. Hookworm did not show a significant trend of decrement in prevalence between 1997 and 2012 (13%) as compared to the years between 2013 and 2020. This is, in contrast, to a study conducted in Nepal where the prevalence of Hookworms significantly decreased between the 1990s and 2015[135].
Eliminating STHs as a public health has to go beyond preventive chemotherapy for SAC, as other groups at risk also serve as a reservoir of infection (preschool children and pregnant women, and even adults), which might have resulted in a slight decline again. It is also suggested that the widespread monotherapy of antihelminthic for deworming purposes might have facilitated the development of drug resistance and hence, decreased the rate of decline STHs in general and Hookworms in particular [122, 123].
The strengths of our review include a rigorous search of several databases and other sources to identify eligible studies on the large pediatric population infected by STHs and generate data for policymakers to strengthen or modify the already ongoing control and prevent measures on the place. We also estimated the geographical distribution and identified risk areas that should be prioritized for MDA and other control interventions, which complement global efforts towards the elimination of STHs and other parasitic infections by 2020. In addition, this work also highlighted the need for surveys in areas where data are not available such as the Somalia region, Afar region, Harari, Dire Dawa city, and Gambela regions or scanty (Addis Ababa city and Benishangul-Gumuz region). There are a few limitations of the present meta-analysis. First, It is prudent to interpret the results of this study as 34(38.6%) of the included studies were low quality based on our quality assessment criteria. Second, in almost all of the studies included in this review, single stool sample examinations were used despite multiple stool samples recommendation for standard diagnosis, and therefore, there is a possibility for underestimation of the prevalence. Almost all studies included the current analyses examined the stool specimens for many parasites at a time and the diagnostic performance of such an approach is not known compared to studies that examine solely for STHs, such a diagnostic approach might affect the detection rate and prevalence estimates of STHs infections. Third WHO has recommended the Kato-Katz method as the best and most reliable diagnostic tool with better efficacy, accuracy, and predictive value than other techniques in resource-poor settings [136]. However, only 39.8% of the studies reported the use of the Kato-Katz method or in combination with other methods. Morbidity due to STH infections is a result of worm burden (number of eggs per gram of feces), otherwise called infection intensity. The disease prevalence is commonly combined with the intensity of infection to assess the epidemiological situation for STH infections and to classify communities into transmission categories, which enables the determination of the appropriate strategies for treatment and control [137]. However, only a few studies (13 out of 88) reported the intensity of infection of species-specific STHs, and thus, difficult to reach on definitive conclusion about the intensity of infection of STH in Ethiopia children. Therefore, there is an urgent need for a large-scale study to assess the intensity of infection of STH in children using the sensitive diagnostic tool on a repeated stool sample. Finally, the review protocol has not registered ahead of actual meta-analysis, which could be a source of bias.
Conclusions
Despite efforts made to reduce, STHs infection is still highly prevalent across the Ethiopian region with some degree of variation. Southern, Amhara, and Oromia regional states carry the highest burden. We observed a decreased prevalence of STHs among Ethiopian children post-MDA compared to preMDA, but the decrease is not statistically significant. A. lumbricoides had the highest prevalence among STHs. A. lumbricoides and T. trichiura were the most prevalent species in the Southern region while hookworms recorded the highest prevalence in the Amhara region. With effort made by the country in eradicating STHs infections, none of the regions in the country is classified as HRZ according to WHO risk classification. Southern, Amhara, and Oromia regions carried the moderate burden and are classified as MRZs, and therefore annual MDA is recommended while, the rest of the regions and city are classified as low-risk zones LRZs. We hope that the results of this study will provide valuable information to policymakers, the National Health Bureau, and other interested bodies, in particular on the endemicity, national and regional distribution, and the prevalence of STHs species in Ethiopia. The high prevalence of STHs observed in this review, underscores the need for better control and prevention strategies in Ethiopia.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- STH:
-
Soil-transmitted Helminth
- MRZ:
-
Moderate risk zone
- HRZ:
-
High-risk zone
- LRZ:
-
Low-risk zone
- MDA:
-
Mass Drug Administration
- GRADE:
-
Grading of recommendations assessment, development, and evaluation
- CI:
-
Confidence interval
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- WHO:
-
World Health Organization
- NTDs:
-
Neglected tropical diseases
- SAC:
-
School age children
- PSAC:
-
Pre-school age children
- MeSH:
-
Medical subject headings
- WASH:
-
Water, sanitation and hygiene
- SNNPR:
-
Southern Nations, Nationalities, and Peoples' Region
References
Savioli L, Stansfield S, Bundy DA, Mitchell A, Bathia R, Engels D, et al. Schistosomiasis and soil-transmitted helminth infections: forging control efforts. Trans R Soc Trop Med Hyg. 2002;96(6):577.
Helminthiases WS-t. Eliminating soil-transmitted helminthiases as a public health problem in children: progress report 2001–2010 and strategic plan 2011–2020. France: World Health Organization. 2012:19–29.
Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A, Diemert D, et al. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. The Lancet. 2006;367(9521):1521–32.
Gyorkos TW, Gilbert NL, Larocque R, Casapía M. Trichuris and hookworm infections associated with anaemia during pregnancy. Trop Med Int Health. 2011;16(4):531–7.
Hotez PJ, Brindley PJ, Bethony JM, King CH, Pearce EJ, Jacobson J. Helminth infections: the great neglected tropical diseases. J Clin Investig. 2008;118(4):1311–21.
Mekonnen Z, Meka S, Ayana M, Bogers J, Vercruysse J, Levecke B. Comparison of individual and pooled stool samples for the assessment of soil-transmitted helminth infection intensity and drug efficacy. PLoS Negl Trop Dis. 2013;7(5):e2189.
Tefera T, Biruksew A, Mekonnen Z, Eshetu T. Parasitic contamination of fruits and vegetables collected from selected local markets of Jimma Town, Southwest Ethiopia. Int Schol Res Not. 2014. https://doi.org/10.1155/2014/382715.
World Health Organization. Prevention and control of schistosomiasis and soil-transmitted helminthiasis: report of a WHO expert committee. 2002; https://apps.who.int/iris/handle/10665/42588
Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7(1):37.
Östan İ, Kilimcioğlu AA, Girginkardeşler N, Özyurt BC, Limoncu ME, Ok ÜZ. Health inequities: lower socio-economic conditions and higher incidences of intestinal parasites. BMC Public Health. 2007;7(1):342.
De Silva NR, Brooker S, Hotez PJ, Montresor A, Engels D, Savioli L. Soil-transmitted helminth infections: updating the global picture. Trends Parasitol. 2003;19(12):547–51.
World Health Organization; Accelerating work to overcome the global impact of neglected tropical diseases: a roadmap for implementation: executive summary. World Health Organization; 2012. https://apps.who.int/iris/handle/10665/70809.
Silver ZA, Kaliappan SP, Samuel P, Venugopal S, Kang G, Sarkar R, et al. Geographical distribution of soil transmitted helminths and the effects of community type in South Asia and South East Asia—a systematic review. PLoS Negl Trop Dis. 2018;12(1):e0006153.
Nute AW, Endeshaw T, Stewart AE, Sata E, Bayissasse B, Zerihun M, et al. Prevalence of soil-transmitted helminths and Schistosoma mansoni among a population-based sample of school-age children in Amhara region, Ethiopia. Parasit Vectors. 2018;11(1):431.
Mekonnen Z, Getachew M, Bogers J, Vercruysse J, Levecke B. Assessment of seasonality in soil-transmitted helminth infections across 14 schools in Jimma Town, Ethiopia. Pan Afr Med J. 2019;32:6. https://doi.org/10.11604/pamj.2019.32.6.16085.
Gadisa E, Jote K. Prevalence and factors associated with intestinal parasitic infection among under-five children in and around Haro Dumal Town, Bale Zone, Ethiopia. BMC Pediatr. 2019;19(1):385.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Atkins D, Eccles M, Flottorp S, Guyatt GH, Henry D, Hill S, et al. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv Res. 2004;4(1):38.
Alamir M, Awoke W, Feleke A. Intestinal parasites infection and associated factors among school children in Dagi primary school, Amhara National Regional State, Ethiopia. Health. 2013;5(10):1697.
Fekadu D, Petros B, Kebede A. Hookworm species distribution among school children in Asendabo town, Jimma Zone, South West Ethiopia. Ethiop J Health Sci. 2008;18(2):53–6.
Desalegn A, Mossie A, Gedefaw L. Nutritional iron deficiency anemia: magnitude and its predictors among school age children, southwest Ethiopia: a community based cross-sectional study. PLoS ONE. 2014;9(12):e114059.
Fentie T, Erqou S, Gedefaw M, Desta A. Epidemiology of human fascioliasis and intestinal parasitosis among schoolchildren in Lake Tana Basin, northwest Ethiopia. Trans R Soc Trop Med Hyg. 2013;107(8):480–6.
Haileamlak A. Intestinal parasites in asymptotic children in Southwest Ethiopia. Ethiop J Health Sci. 2005;15(2):107–18.
Mulatu G, Zeynudin A, Zemene E, Debalke S, Beyene G. Intestinal parasitic infections among children under five years of age presenting with diarrhoeal diseases to two public health facilities in Hawassa, South Ethiopia. Infect Dis Poverty. 2015;4(1):49.
Alemu A, Atnafu A, Addis Z, Shiferaw Y, Teklu T, Mathewos B, et al. Soil transmitted helminths and Schistosoma mansoni infections among school children in Zarima town, northwest Ethiopia. BMC Infect Dis. 2011;11(1):189.
Amare B, Ali J, Moges B, Yismaw G, Belyhun Y, Gebretsadik S, et al. Nutritional status, intestinal parasite infection and allergy among school children in Northwest Ethiopia. BMC Pediatr. 2013;13(1):7.
Ayalew A, Debebe T, Worku A. Prevalence and risk factors of intestinal parasites among Delgi school children, North Gondar, Ethiopia. J Parasitol Vector Biol. 2011;3(5):75–81.
Beyene G, Tasew H. Prevalence of intestinal parasite, Shigella and Salmonella species among diarrheal children in Jimma health center, Jimma southwest Ethiopia: a cross sectional study. Ann Clin Microbiol Antimicrob. 2014;13(1):10.
Legesse M, Erko B. Prevalence of intestinal parasites among schoolchildren in a rural area close to the southeast of Lake Langano. Ethiop Ethiop J Health Dev. 2004;18(116):120.
Merid Y, Hegazy M, Mekete G, Teklemariam S. Intestinal helminthic infection among children at Lade Awassa Area, South Ethiopia. Ethiop J Health Dev. 2001;15(1):31–8.
Nguyen NL, Gelaye B, Aboset N, Kumie A, Williams MA, Berhane Y. Intestinal parasitic infection and nutritional status among school children in Angolela, Ethiopia. J Prev Med Hyg. 2012;53(3):157.
Nyantekyi LA, Legesse M, Belay M, Tadesse K, Manaye K, Macias C, et al. Intestinal parasitic infections among under-five children and maternal awareness about the infections in Shesha Kekele, Wondo Genet. Southern Ethiopia. Ethiop J Health Dev. 2010;24(3):185–90.
Tadesse G. The prevalence of intestinal helminthic infections and associated risk factors among school children in Babile town, eastern Ethiopia. Ethiop J Health Dev. 2005;19(2):140–7.
Degarege A, Erko B. Association between intestinal helminth infections and underweight among school children in Tikur Wuha Elementary School, Northwestern Ethiopia. J Infect Public Health. 2013;6(2):125–33.
Jemaneh L. Schistosomiasis mansoni and geo-Helminthiasis in school children in the Dembia Plains, Northwest Ethiopia. Ethiop J Health Dev. 1998;12(3):237–44.
Jejaw A, Zemene E, Alemu Y, Mengistie Z. High prevalence of Schistosoma mansoni and other intestinal parasites among elementary school children in Southwest Ethiopia: a cross-sectional study. BMC Public Health. 2015;15(1):600.
King JD, Endeshaw T, Escher E, Alemtaye G, Melaku S, Gelaye W, et al. Intestinal parasite prevalence in an area of Ethiopia after implementing the SAFE strategy, enhanced outreach services, and health extension program. PLoS Negl Trop Dis. 2013;7(6):e2223.
Tulu B, Taye S, Amsalu E. Prevalence and its associated risk factors of intestinal parasitic infections among Yadot primary school children of South Eastern Ethiopia: a cross-sectional study. BMC Res Notes. 2014;7(1):848.
Workneh T, Esmael A, Ayichiluhm M. Prevalence of intestinal parasitic infections and associated factors among Debre Elias primary schools children, East Gojjam Zone, Amhara Region, North West Ethiopia. J Bacteriol Parasitol. 2014;15(1):1–5.
Erosie L, Merid Y, Ashiko A, Ayine M, Balihu A, Muzeyin S, et al. Prevalence of Hookworm infection and haemoglobin status among rural elementary school children in Southern Ethiopia. Ethiop J Health Dev. 2002;16(1):113–5.
Gelaw A, Anagaw B, Nigussie B, Silesh B, Yirga A, Alem M, et al. Prevalence of intestinal parasitic infections and risk factors among schoolchildren at the University of Gondar Community School, Northwest Ethiopia: a cross-sectional study. BMC Public Health. 2013;13(1):304.
Jemaneh L. Soil-transmitted helminth infections and Schistosomiasis mansoni in school children from Chilga District, Northwest Ethiopia. Ethiop J Health Sci. 2001;11(2):79–87.
Mahmud MA, Spigt M, Mulugeta Bezabih A, Lopez Pavon I, Dinant G-J, Blanco VR. Risk factors for intestinal parasitosis, anaemia, and malnutrition among school children in Ethiopia. Pathog Global Health. 2013;107(2):58–65.
Mahmud MA, Spigt M, Bezabih AM, Pavon IL, Dinant G-J, Velasco RB. Efficacy of handwashing with soap and nail clipping on intestinal parasitic infections in school-aged children: a factorial cluster randomized controlled trial. PLoS Med. 2015;12(6):e1001837.
Reji P, Belay G, Erko B, Legesse M, Belay M. Intestinal parasitic infections and malnutrition amongst first-cycle primary schoolchildren in Adama, Ethiopia. Afr J Primary Health Care Fam Med. 2011;3(1):192–8.
Roma B, Worku S. Magnitude of Schistosoma mansoni and intestinal helminthic infections among school children in Wondo-Genet Zuria, southern Ethiopa. Ethiop J Health Dev. 1997;11:125–30.
Wegayehu T, Adamu H, Petros B. Prevalence of Giardia duodenalis and Cryptosporidium species infections among children and cattle in North Shewa Zone, Ethiopia. BMC Infect Dis. 2013;13(1):419.
Adamu H, Endeshaw T, Teka T, Kifle A, Petros B. The prevalence of intestinal parasites in paediatric diarrhoeal and non-diarrhoeal patients in Addis Ababa hospitals, with special emphasis on opportunistic parasitic infections and with insight into the demographic and socio-economic factors. Ethiop J Health Dev. 2006;20(1):39–46.
Belyhun Y, Medhin G, Amberbir A, Erko B, Hanlon C, Alem A, et al. Prevalence and risk factors for soil-transmitted helminth infection in mothers and their infants in Butajira, Ethiopia: a population based study. BMC Public Health. 2010;10(1):21.
Dejenie T, Asmelash T, Teferi M. Intestinal helminthes infections and re-infections with special emphasis on schistosomiasis mansoni in Waja, North Ethiopia. Momona Ethiop J Sci. 2009;1(2):4–16.
Kidane E, Menkir S, Kebede A, Desta M. Prevalence of intestinal parasitic infections and their associations with anthropometric measurements of school children in selected primary schools, Wukro town, eastern Tigray. Ethiop Sci J Zool. 2013;229(1319):1–16.
Legesse L, Erko B, Hailu A. Current status of intestinal Schistosomiasis and soiltransmitted helminthiasis among primary school children in Adwa Town. Northern Ethiopia. Ethiop J Health Dev. 2010;24(3):191–7.
Mathewos B, Alemu A, Woldeyohannes D, Alemu A, Addis Z, Tiruneh M, et al. Current status of soil transmitted helminths and Schistosoma mansoni infection among children in two primary schools in North Gondar, Northwest Ethiopia: a cross sectional study. BMC Res Notes. 2014;7(1):88.
Alemayehu B, Tomass Z, Wadilo F, Leja D, Liang S, Erko B. Epidemiology of intestinal helminthiasis among school children with emphasis on Schistosoma mansoni infection in Wolaita zone, Southern Ethiopia. BMC Public Health. 2017;17(1):587.
Assefa A, Dejenie T, Tomass Z. Infection prevalence of Schistosoma mansoni and associated risk factors among schoolchildren in suburbs of Mekelle city, Tigray, Northern Ethiopia. Momona Ethiop J Sci. 2013;5(1):174–88.
Dejenie T, Petros B. Irrigation practices and intestinal Helminth infections in southern and central zones of Tigray. Ethiop J Health Dev. 2009;23(1):48–56.
Gashaw F, Aemero M, Legesse M, Petros B, Teklehaimanot T, Medhin G, et al. Prevalence of intestinal helminth infection among school children in Maksegnit and Enfranz Towns, northwestern Ethiopia, with emphasis on Schistosoma mansoni infection. Parasit Vectors. 2015;8(1):567.
Jemaneh L. Intestinal helminth infections in school children in Adarkay District, Northwest Ethiopia, with special reference to schistosoma mansoni. Ethiop J Health Dev. 1997;11(3):289–94.
Mengist HM, Taye B, Tsegaye A. Intestinal parasitosis in relation to CD4+ T cells levels and anemia among HAART initiated and HAART naive pediatric HIV patients in a model ART center in Addis Ababa, Ethiopia. PLoS ONE. 2015;10(2):e0117715.
Tekeste Z, Belyhun Y, Gebrehiwot A, Moges B, Workineh M, Ayalew G, et al. Epidemiology of intestinal schistosomiasis and soil transmitted helminthiasis among primary school children in Gorgora, Northwest Ethiopia. Asian Pac J Trop Dis. 2013;3(1):61–4.
Terefe A, Shimelis T, Mengistu M, Hailu A, Erko B. Schistosomiasis mansoni and soil-transmitted helminthiasis in Bushulo village, southern Ethiopia. Ethiop J Health Dev. 2011;25(1):46–50.
Wale M, Wale M, Fekensa T. The prevalence of intestinal helminthic infections and associated risk factors among school children in Lumame town, Northwest, Ethiopia. J Parasitol Vector Biol. 2014;6(10):156–65.
Aiemjoy K, Gebresillasie S, Stoller NE, Shiferaw A, Tadesse Z, Chanyalew M, et al. Epidemiology of soil-transmitted helminth and intestinal protozoan infections in preschool-aged children in the Amhara region of Ethiopia. Am J Trop Med Hyg. 2017;96(4):866–72.
Alemu M, Hailu A, Bugssa G. Prevalence of intestinal schistosomiasis and soil-transmitted helminthiasis among primary schoolchildren in Umolante district South Ethiopia. Clin Med Res. 2014;3(6):174–80.
Tullu B, Solomon T, Yohannes ZENEBE EA. Intestinal parasitic infections and nutritional status among primary school children in Delo-mena district, South Eastern Ethiopia. Iran J Parasitol. 2016;11(4):549.
Dejenie T, Asmelash T. Schistosomiasis mansoni among school children of different water source users in Tigray, Northern Ethiopia. Momona Ethiop J Sci. 2010;2(1):49–60.
Teklemariam A, Dejenie T, Tomass Z. Infection prevalence of intestinal helminths and associated risk factors among schoolchildren in selected kebeles of Enderta district, Tigray, Northern Ethiopia. J Parasitol Vector Biol. 2014;6(11):166–73.
Zemene T, Shiferaw MB. Prevalence of intestinal parasitic infections in children under the age of 5 years attending the Debre Birhan referral hospital, North Shoa, Ethiopia. BMC Res Notes. 2018;11(1):58.
Firdu T, Abunna F, Girma M. Intestinal protozoal parasites in diarrheal children and associated risk factors at Yirgalem Hospital, Ethiopia: a case-control study. Int Sch Res Not. 2014;2014:1–8. https://doi.org/10.1155/2014/357126.
Tefera E, Belay T, Mekonnen SK, Zeynudin A, Belachew T. Prevalence and intensity of soil transmitted helminths among school children of Mendera Elementary School, Jimma, Southwest Ethiopia. Pan Afr Med J. 2017;27:1–12.
Unasho A. An investigation of intestinal parasitic infections among the asymptomatic children in, Southern Ethiopia. Int J Child Health Nutr. 2013;2(3):212–22.
Yimam Y, Degarege A, Erko B. Effect of anthelminthic treatment on Helminth infection and related anaemia among school-age children in northwestern Ethiopia. BMC Infect Dis. 2016;16(1):613.
Abdi M, Nibret E, Munshea A. Prevalence of intestinal helminthic infections and malnutrition among schoolchildren of the Zegie Peninsula, northwestern Ethiopia. J Infect Public Health. 2017;10(1):84–92.
Abera A, Nibret E. Prevalence of gastrointestinal helminthic infections and associated risk factors among schoolchildren in Tilili town, northwest Ethiopia. Asian Pac J Trop Med. 2014;7(7):525–30.
Wegayehu T, Karim MR, Li J, Adamu H, Erko B, Zhang L, et al. Multilocus genotyping of Giardia duodenalis isolates from children in Oromia Special Zone, central Ethiopia. BMC Microbiol. 2016;16(1):89.
Abossie A, Seid M. Assessment of the prevalence of intestinal parasitosis and associated risk factors among primary school children in Chencha town, Southern Ethiopia. BMC Public Health. 2014;14(1):166.
Hailegebriel T. Prevalence of intestinal parasitic infections and associated risk factors among students at Dona Berber primary school, Bahir Dar, Ethiopia. BMC Infect Dis. 2017;17(1):362.
Alemu G, Aschalew Z, Zerihun E. Burden of intestinal helminths and associated factors three years after initiation of mass drug administration in Arbaminch Zuria district, southern Ethiopia. BMC Infect Dis. 2018;18(1):435.
Alemu A, Tegegne Y, Damte D, Melku M. Schistosoma mansoni and soil-transmitted helminths among preschool-aged children in Chuahit, Dembia district, Northwest Ethiopia: prevalence, intensity of infection and associated risk factors. BMC Public Health. 2016;16(1):422.
Alemu G, Abossie A, Yohannes Z. Current status of intestinal parasitic infections and associated factors among primary school children in Birbir town, Southern Ethiopia. BMC Infect Dis. 2019;19(1):270.
Bajiro M, Dana D, Ayana M, Emana D, Mekonnen Z, Zawdie B, et al. Prevalence of Schistosoma mansoni infection and the therapeutic efficacy of praziquantel among school children in Manna District, Jimma Zone, southwest Ethiopia. Parasit Vectors. 2016;9(1):560.
Amor A, Rodriguez E, Saugar JM, Arroyo A, López-Quintana B, Abera B, et al. High prevalence of Strongyloides stercoralis in school-aged children in a rural highland of north-western Ethiopia: the role of intensive diagnostic work-up. Parasit Vectors. 2016;9(1):617.
Gebretsadik D, Metaferia Y, Seid A, Fenta GM, Gedefie A. Prevalence of intestinal parasitic infection among children under 5 years of age at Dessie Referral Hospital: cross sectional study. BMC Res Notes. 2018;11(1):771.
Bekana T, Hu W, Liang S, Erko B. Transmission of Schistosoma mansoni in Yachi areas, southwestern Ethiopia: new foci. Infect Dis Poverty. 2019;8(1):1–8.
Diro E, Lynen L, Gebregziabiher B, Assefa A, Lakew W, Belew Z, et al. Clinical aspects of paediatric visceral leishmaniasis in N orth-west E thiopia. Trop Med Int Health. 2015;20(1):8–16.
Birhanu M, Gedefaw L, Asres Y. Anemia among School-Age Children: Magnitude, Severity and Associated Factors in Pawe Town, Benishangul-Gumuz Region, Northwest Ethiopia. Ethiop J Health Sci. 2018;28(3):259–66.
Leta GT, French M, Dorny P, Vercruysse J, Levecke B. Comparison of individual and pooled diagnostic examination strategies during the national mapping of soil-transmitted helminths and Schistosoma mansoni in Ethiopia. PLoS Negl Trop Dis. 2018;12(9):e0006723.
Tefera E, Mohammed J, Mitiku H. Intestinal helminthic infections among elementary students of Babile town, Eastern Ethiopia. Pan Afr Med J. 2015;20(1):1–10.
Hailu T, Alemu M, Abera B, Mulu W, Yizengaw E, Genanew A, et al. Multivariate analysis of factors associated with Schistosoma mansoni and hookworm infection among primary school children in rural Bahir Dar, Northwest Ethiopia. Trop Dis Travel Med Vaccines. 2018;4(1):4.
Alemayehu B, Tomass Z. Schistosoma mansoni infection prevalence and associated risk factors among schoolchildren in Demba Girara, Damot Woide District of Wolaita Zone, Southern Ethiopia. Asian Pac J Trop Med. 2015;8(6):457–63.
Ali I, Mekete G, Wodajo N. Intestinal parasitism and related risk factors among students of Asendabo Elementary and Junior Secondary School South western Ethiopia. Ethiop J Health Dev. 1999;13(2):157–62.
Jemaneh L. Intestinal helminth infections in schoolchildren in Gonder town and surrounding areas Northwest Ethiopia. SINET Ethiop J Sci. 1999;22(2):209–20.
Debalke S, Worku A, Jahur N, Mekonnen Z. Soil transmitted helminths and associated factors among schoolchildren in government and private primary school in Jimma Town, Southwest Ethiopia. Ethiop J Health Sci. 2013;23(3):237–44.
Dejene T. Impact of irrigation on the prevalence of intestinal parasite infections with emphasis on schistosomiasis in Hintallo-Wejerat, North Ethiopia. Ethiop J Health Sci. 2008;18(2):33–8.
Abera B, Alem G, Yimer M, Herrador Z. Epidemiology of soil-transmitted helminths, Schistosoma mansoni, and haematocrit values among schoolchildren in Ethiopia. J Infect Dev Ctries. 2013;7(03):253–60.
Kabeta A, Assefa S, Hailu D, Berhanu G. Intestinal parasitic infections and nutritional status of pre-school children in Hawassa Zuria District, South Ethiopia. Afr J Microbiol Res. 2017;11(31):1243–51.
Shumbej T, Belay T, Mekonnen Z, Tefera T, Zemene E. Soil-transmitted helminths and associated factors among pre-school children in Butajira town, south-Central Ethiopia: a community-based cross-sectional study. PLoS ONE. 2015;10(8):e0136342.
Tadege B, Shimelis T. Infections with Schistosoma mansoni and geohelminths among school children dwelling along the shore of the Lake Hawassa, southern Ethiopia. PLoS ONE. 2017;12(7):e0181547.
Andualem MA. Parasitic infection and associated factors among the primary school children in Motta town, western Amhara, Ethiopia. Am J Public Health Res. 2014;2(6):248-54.
Teshale T, Belay S, Tadesse D, Awala A, Teklay G. Prevalence of intestinal helminths and associated factors among school children of Medebay Zana wereda; North Western Tigray, Ethiopia 2017. BMC Res Notes. 2018;11(1):444.
Elfu BF. Epidemiology of Hookworm Infection in the School-age Children: A Comparative Cross-sectional Study. Iran J Parasitol. 2018;13(4):560.
Eyamo T, Girma M, Alemayehu T, Bedewi Z. Soil-transmitted helminths and other intestinal parasites among schoolchildren In Southern Ethiopia. Res Rep Trop Med. 2019;10:137.
Mekonnen Z, Suleman S, Biruksew A, Tefera T, Chelkeba L. Intestinal polyparasitism with special emphasis to soil-transmitted helminths among residents around Gilgel Gibe Dam, Southwest Ethiopia: a community based survey. BMC Public Health. 2016;16(1):1185.
Molla E, Mamo H. Soil-transmitted helminth infections, anemia and undernutrition among schoolchildren in Yirgacheffee, South Ethiopia. BMC Res Notes. 2018;11(1):585.
Sitotaw B, Mekuriaw H, Damtie D. Prevalence of intestinal parasitic infections and associated risk factors among Jawi primary school children, Jawi town, north-west Ethiopia. BMC Infect Dis. 2019;19(1):341.
Tadesse M, Dobo B, Birmeka M. Prevalence and associated risk factors of intestinal parasitic infections among school children in Bamo no 2 primary school, Adele town, East Arsi, Ethiopia. Sub-Saharan Afr J Med. 2019;6(2):77.
Weldesenbet H, Worku A, Shumbej T. Prevalence, infection intensity and associated factors of soil transmitted helminths among primary school children in Gurage zone, South Central Ethiopia: a cross-sectional study design. BMC Res Notes. 2019;12(1):231.
Workineh L, Kiros T, Damtie S, Andualem T, Dessie B. Prevalence of Soil-Transmitted Helminth and Schistosoma mansoni Infection and Their Associated Factors among Hiruy Abaregawi Primary School Children, Rural Debre Tabor, North West Ethiopia: A Cross-Sectional Study. J Parasitol Res. 2020; 1-6.
Shumbej T, Girum T. Helminth infections in light of an ongoing intervention in endemic areas of Guragae zone, Southern Ethiopia: an implication for neglected tropical diseases elimination in Ethiopia by 2020. Trop Dis Travel Med Vaccines. 2019;5(1):8.
Zenu S, Alemayehu E, Woldemichael K. Prevalence of intestinal parasitic infections and associated factors among street children in Jimma Town; South West Ethiopia in 2019: a Cross Sectional Study. BMC Public Health. 2019;19:1731.
Gizaw Z, Adane T, Azanaw J, Addisu A, Haile D. Childhood intestinal parasitic infection and sanitation predictors in rural Dembiya, northwest Ethiopia. Environ Health Prevent Med. 2018;23(1):26.
Mekonnen HS, Ekubagewargies DT. Prevalence and factors associated with intestinal parasites among under-five children attending Woreta Health Center, Northwest Ethiopia. BMC Infect Dis. 2019;19(1):256.
Gebrehiowot Y, Degarege A, Erko B. Prevalence of intestinal parasitic infections among children under five years of age with emphasis on Schistosoma mansoni in Wonji Shoa Sugar Estate, Ethiopia. PLoS ONE. 2014;9(10):e109793.
Hailu T, Alemu M, Abera B, Mulu W, Yizengaw E, Genanew A, et al. Multivariate analysis of factors associated with Schistosoma mansoni and hookworm infection among primary school children in rural Bahir Dar, Northwest Ethiopia. Trop Dis Travel Med Vaccines. 2018;4:4.
Assefa T, Woldemichael T, Dejene A. Intestinal parasitism among students in three localities in south Wello, Ethiopia. Ethiop J Health Dev. 1998;12(3):231.
Kidane E, Menkir S. Prevalence of intestinal parasitic infections and their associations with anthropometric measurements of school children in selected primary schools, Wukro Town, Eastern Tigray, Ethiopia: Haramaya University. Int J Curr Microbiol Appl Sci. 2014;3(3):11–29.
Samuel F. Status of soil-transmitted helminths infection in Ethiopia. Am J Health Res. 2015;3(3):170–6.
Chammartin F, Scholte RG, Guimarães LH, Tanner M, Utzinger J, Vounatsou P. Soil-transmitted helminth infection in South America: a systematic review and geostatistical meta-analysis. Lancet Infect Dis. 2013;13(6):507–18.
Daryani A, Hosseini-Teshnizi S, Hosseini S-A, Ahmadpour E, Sarvi S, Amouei A, et al. Intestinal parasitic infections in Iranian preschool and school children: a systematic review and meta-analysis. Acta Trop. 2017;169:69–83.
Yapi RB, Chammartin F, Hürlimann E, Houngbedji CA, Prisca B, Silué KD, et al. Bayesian risk profiling of soil-transmitted helminth infections and estimates of preventive chemotherapy for school-aged children in Côte d’Ivoire. Parasit Vectors. 2016;9(1):162.
Karshima SN. Prevalence and distribution of soil-transmitted helminth infections in Nigerian children: a systematic review and meta-analysis. Infect Dis Poverty. 2018;7(1):69.
Keiser J, Utzinger J. Efficacy of current drugs against soil-transmitted helminth infections: systematic review and meta-analysis. JAMA. 2008;299(16):1937–48.
Levecke B, Montresor A, Albonico M, Ame SM, Behnke JM, Bethony JM, et al. Assessment of anthelmintic efficacy of mebendazole in school children in six countries where soil-transmitted helminths are endemic. PLoS Negl Trop Dis. 2014;8(10):e3204. https://doi.org/10.1371/journal.pntd.0003204.
Asaolu S, Ofoezie I. The role of health education and sanitation in the control of helminth infections. Acta Trop. 2003;86(2–3):283–94.
Barker WH. Perspectives on acute enteric disease epidemiology and control. Bull Pan Am Health Org(PAHO); 1975;9(2).
Okun DA. The value of water supply and sanitation in development: an assessment. Am J Public Health. 1988;78(11):1463–7.
Prichard RK, Basáñez M-G, Boatin BA, McCarthy JS, García HH, Yang G-J, et al. A research agenda for helminth diseases of humans: intervention for control and elimination. PLoS Negl Trop Dis. 2012;6(4):e1582. https://doi.org/10.1371/journal.pntd.0001582.
Hotez PJ, Pritchard DI. Hookworm infection. Sci Am. 1995;272(6):68–74.
Hotez PJ, Kamath A. Neglected tropical diseases in sub-Saharan Africa: review of their prevalence, distribution, and disease burden. PLoS Negl Trop Dis. 2009;3(8):412. https://doi.org/10.1371/journal.pntd.0000412.
Ojja S, Kisaka S, Ediau M, Tuhebwe D, Kisakye AN, Halage AA, et al. Prevalence, intensity and factors associated with soil-transmitted helminths infections among preschool-age children in Hoima district, rural western Uganda. BMC Infect Dis. 2018;18(1):408.
Ngonjo T, Okoyo C, Andove J, Simiyu E, Lelo AE, Kabiru E, et al. Current status of soil-transmitted helminths among school children in kakamega county, western kenya. J Parasitol Res. 2016. https://doi.org/10.1155/2016/7680124
Tefera E, Belay T, Mekonnen SK, Zeynudin A, Belachew T. Therapeutic efficacy of different brands of albendazole against soil transmitted helminths among students of Mendera Elementary School, Jimma, Southwest Ethiopia. Pan Afr Med J. 2015;22(1):252. https://doi.org/10.11604/pamj.2015.22.252.6501.
Staudacher O, Heimer J, Steiner F, Kayonga Y, Havugimana JM, Ignatius R, et al. Soil-transmitted helminths in southern highland R wanda: associated factors and effectiveness of school-based preventive chemotherapy. Trop Med Int Health. 2014;19(7):812–24.
Tchuenté L-AT, Ngassam RIK, Sumo L, Ngassam P, Noumedem CD, Nzu DDL, et al. Mapping of schistosomiasis and soil-transmitted helminthiasis in the regions of centre, east and west Cameroon. PLoS Negl Trop Dis. 2012;6(3):1553.
Kunwar R, Acharya L, Karki S. Trends in prevalence of soil-transmitted helminth and major intestinal protozoan infections among school-aged children in Nepal. Trop Med Int Health. 2016;21(6):703–19.
Nikolay B, Brooker SJ, Pullan RL. Sensitivity of diagnostic tests for human soil-transmitted helminth infections: a meta-analysis in the absence of a true gold standard. Int J Parasitol. 2014;44(11):765–74.
World Health Organization; Preventive chemotherapy in human helminthiasis. Coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers, 2006; https://apps.who.int/iris/handle/10665/43545.
Acknowledgements
None.
Funding
We did not receive any funding support for this work.
Author information
Authors and Affiliations
Contributions
LCH and TSM conceived the study. LCH, ZM, and TSM extracted the data, and independently decided for inclusion or exclusion, and in events of disagreement, WJ helped to resolve. LCH, TSM, and DE performed all the statistical analyses. LCH, ZM, and WJ prepared the manuscript with help from DE. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
None applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Supplementary Information
Additional file 1:
Forest plot and meta-regression result of the prevalence of soil-transmitted helminths infections by region and species.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chelkeba, L., Mekonnen, Z., Emana, D. et al. Prevalence of soil-transmitted helminths infections among preschool and school-age children in Ethiopia: a systematic review and meta-analysis. glob health res policy 7, 9 (2022). https://doi.org/10.1186/s41256-022-00239-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41256-022-00239-1