
Abstract
Background
Cardiovascular diseases are the main cause of mortality in the world. This study aimed to estimate the incidence and identify the risk factors of these diseases.
Methods
This prospective cohort study was performed on 9442 individuals aged 40–70 years in Kharameh, a city in the South of Iran, in 2015–2022. The subjects were followed up for 4 years. The demographic information, behavioral habits, biological parameters, and history of some diseases were examined. The density incidence of cardiovascular disease was calculated. The log-rank test was calculated to assess the cardiovascular incidence difference between men and women. Simple and multiple Cox regression with Firth's bias reduction method were used to identify the predictors of cardiovascular disease.
Results
The mean ± SD age of the participants was 51.4 ± 8.04 years, and the density incidence was estimated at 1.9 cases per 100,000 person-day. The log-rank test showed that men had a higher risk of cardiovascular disease than women. The Fisher's exact test showed a statistically significant difference between the incidence of cardiovascular diseases in different age groups, education levels, diabetes, and hypertension in men and women. The results of multiple Cox regression revealed that with increasing age, the risk of developing CVDs increased. In addition, the risk of cardiovascular disease is higher in people with kidney disease (HRadj = 3.4, 95% CI 1.3 to 8.7), men (HRadj = 2.3, 95% CI 1.7 to 3.2), individuals with hypertension (HRadj = 1.6, 95% CI 1.3 to 2.1), diabetics (HRadj = 2.3, 95%c CI 1.8 to 2.9), and alcohol consumption (HRadj = 1.5, 95% CI 1.09 to 2.2).
Conclusions
In the present study, diabetes, hypertension, age, male gender, and alcohol consumption were identified as the risk factors for cardiovascular diseases; three variables of diabetes, hypertension and alcohol consumption were among the modifiable risk factors, so if they were removed, the incidence of cardiovascular disease could greatly reduce. Therefore, it is necessary to develop strategies for appropriate interventions to remove these risk factors.
Similar content being viewed by others

Background
Cardiovascular diseases (CVDs) are among the most common non-communicable diseases [1]. They are the leading cause of death worldwide, and it is estimated that out of 55 million deaths in 2017, 17.7 million were related to CVDs [2, 3]. In addition, it is predicted that this figure will reach 23.6 million in 2030 [4, 5]. According to the Global Burden of Diseases (GBD) report in 2019, total cases of CVDs doubled from 1990 to 2019 and increased from 271 to 532 million. In addition, Disability Adjusted Life Years (DALYs) increased from 17.7 million to 34.4 million [6]. The report on the burden of diseases in 2015 introduced Iran as one of the countries with the highest rates of CVDs in the world due to having more than 9000 cases of CVDs per 100,000 population. In addition, it has been stated that the mortality rate due to these diseases has increased in Iran. Moreover, CVDs have important clinical consequences, cause premature death, and reduce the quality of life [5, 7].
There are several risk factors for CVDs that are generally divided into two categories: non-modifiable (age, sex, race, and family history) and modifiable (diabetes, lipid profile, hypertension, alcohol consumption, smoking, inadequate physical activity, inappropriate diet, and obesity) [8, 9]. Behavioral, environmental, and social factors are the other risk factors for CVDs [6]. Global evidence shows that by controlling and managing the modifiable risk factors, up to 90% of cases of CVDs can be reduced [5]. Therefore, appropriate identification of individuals with these risk factors and those susceptible to CVDs is an important step in controlling these diseases [10].
Epidemiological studies have played an important role in understanding the risk factors of CVDs [6]. Nevertheless, health service planning units in Iran do not yet have accurate estimates of the current status of CVDs regionally [11]. At the same time, we need to accurately estimate the incidence rate and risk factors of CVDs in each region to determine appropriate strategies for preventing and controlling these diseases [5]. In addition, most studies in this field have been performed on a specific group of patients, and information on the general population has not been extensively reviewed. Therefore, this study was conducted to investigate the incidence rate and identify the risk factors affecting the incidence of CVDs in the population aged 40–70 years in Kharameh in the South of Iran to help health policymakers to develop preventive guidelines.
Methods
Kharameh cohort study design
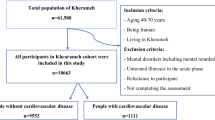
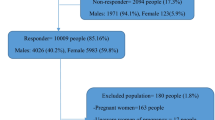
The present prospective cohort study was conducted based on the data of the Kharameh cohort study, which is part of a large Prospective Epidemiological Studies in Iran (PERSIAN) launched in 2014. Other details are explained in the Persian cohort study [12]. The target population of the Kharameh cohort study includes all individuals aged 40–70 years. At first, all these individuals were invited to participate in the study. Finally, 10,663 subjects (97.3% participation rate) participated in the study after they signed the informed consent forms.
The inclusion criteria for the Kharameh cohort study were age 40–70 years and at least 9 months of residence in Kharameh to allow time to adapt to the environment and culture [13]. Exclusion criterion was the individuals with mental retardation or mental disorders who could not participate in the study. In addition, the exclusion criteria of this study were having a history of CVDs, heart attacks, and stroke. At first, there were 1221 people; after some of them were excluded, 9442 subjects were followed up in the present study (Fig. 1).

Flow chart of the study population
The baseline data of the Kharameh cohort study were collected from March 2015 to March 2017, and the information about the incidence of CVDs in individuals was collected during four stages of the follow-up in 2018, 2019, 2020, and 2021. Trained experts collected the participants' demographic information and behavioral habits through face-to-face interviews; physicians of the Kharameh cohort team recorded their clinical information. Questionnaires related to the PERSIAN cohort study, which had previously been validated, were used to collect the data. The history of chronic diseases in individuals was recorded by their self-declaration and review of medical records by physicians.
Demographic and clinical data of the study patients
In this study, data related to the demographic characteristics of individuals and some of their behavioral habits were used. This information included age, sex, marital status, education, place of residence, having a job, Body Mass Index (BMI), waist circumference, hip circumference, alcohol consumption, smoking, and socioeconomic status (SES). In this study, having a job was defined as working at least 8 h per week at the time of enrollment visit. In addition, alcohol consumption and smoking were considered as drinking approximately 200 ml of beer or 45 ml of liquor, once per week for at least 6 months, and smoking at least 100 cigarettes during lifetime, respectively.
The history of diseases such as diabetes, hypertension, fatty liver disease, and chronic kidney disease was also examined. In addition, fasting blood sugar (FBS), low-density lipoprotein (LDL), triglyceride (TG), and high-density lipoprotein (HDL) were assessed. To assess the SES of the individuals, we completed the PERSIAN cohort questionnaires related to the socioeconomic information of individuals, and the collected variables related to SES were analyzed using Principal Component Analysis (PCA) to identify the components for grouping related individuals into different SES categories. Accordingly, the participants were divided into four classes: low, moderate, high, and very high [14].
Weight was measured without shoes and with light clothing using a SECA scale (made in Germany), and height was measured using a standard measuring tape. BMI was calculated by dividing the body weight (kilogram) by height squared (meter). Accordingly, the participants were divided into four groups: underweight (less than 18.5 kg/m2), normal (18.5 to 24.9 kg/m2), overweight (25 to 29.9 kg/m2), and obese (over 30 kg/m2) [15]. For the laboratory experiments, the individuals were requested to fast for 12 defined as a history of diabetes, treatment of diabetes, or fasting blood sugar above 126 mg/dL. Blood pressure was measured from the participants' left arms using a standard calibrated sphygmomanometer (Reister Model, Germany) after a 5-min rest in a sitting position. It was measured twice with an interval of 10 min, and the mean was recorded.
Cardiovascular disease
In this study, individuals were followed for 4 years from 2018 to 2021, and in each follow-up period, we initially recorded the incidence of CVDs according to their self-declaration. Then, their medical records were reviewed by physicians, and if confirmed, they were registered as a new case of CVDs. CVDs in this study included coronary heart disease, cerebrovascular disease, rheumatoid arthritis, myocardial infarction, stroke, and heart valve disease.
Statistical analysis
In the present study, the dependent variable was the time to event of CVDs, from the time of enrollment until the event of CVDs. In addition, individuals were considered right censors if they did not have the event of CVDs until the end of the study. Quantitative and qualitative variables were described with the mean (standard deviation) and number (percentage). The Kolmogorov–Smirnov test determined the normality of quantitative variables. The difference between the mean of quantitative variables and the levels of qualitative variables between the two groups with and without CVDs was assessed using an independent t test, Mann–Whitney, and Fisher's exact test. The density incidence rate was calculated in terms of person-day unit, which is the actual number of days that individuals are at risk of CVDs. We summed the days of observation which started from the participant's enrollment to the date of the event of CVDs or the end of the study. For survival analysis, the Kaplan–Meier curve for CVDs was plotted, and the log-rank test was calculated to compare the risk of CVDs curve between men and women. Finally, simple Cox regression with Firth's bias reduction method was used to identify the risk factors of CVDs. To control the confounders, we entered all variables with a p value less than 0.2 into multiple Cox regression. The association was also reported with Hazard Ratio (HR) with a 95% confidence interval (CI). Firth's method was used in the Cox proportional hazards framework to develop and validate a prediction model for rare event survival data (heavily censored). All analyses were carried out using software R version 4.1.2, the "Coxphf" package, and STATA software version 12.
Results
In the present study, 9442 individuals aged 40–70 with a mean age of 51.47 ± 8.04 were followed up for 19,744,954 person-days. During this period, 386 new cases of CVDs were observed. The density incidence was 1.9 cases per 100,000 persons-days. Women and the illiterate accounted for 55.6% and 50.7% of the participants, respectively. Most participants were married (89.7%), and 59% were overweight and obese (Table 1).
Based on the results presented in Table 1, the incidence of CVDs was higher in the older age groups for both sexes (p < 0.01). The incidence of CVDs was associated with marital status of women (p < 0.01) and with the SES level of men (p = 0.04). In addition, the incidence of CVDs was associated with education level, status of diabetes, and high blood pressure in both men and women. (p < 0.01).
There was a statistically significant difference between the FBS, LDL, TG, and waist and hip circumference in the two groups of women with and without CVDs. In addition, there was a significant difference between the mean of LDL in men with and without CVDs (Table 2).
Figure 2A shows the Kaplan–Meier survival curve for all individuals, and Fig. 2B displays the Kaplan–Meier survival curve by gender. It was observed that the risk of developing CVDs was higher in men than in women. The log-rank test (p < 0.01) also revealed that the difference between women and men was statistically significant.

Kaplan–Meier curve of the time to first diagnosis of cardiovascular diseases in a population of 40–70 years in the Kharameh cohort study (A), and by gender (B)
In addition, we performed simple Cox regression to identify the predictors of CVDs. The results of simple Cox regression showed a statistically significant relationship between the variables of sex, age, marital status, having job, alcohol consumption, smoking, history of diabetes, chronic kidney disease, hypertension, education, location, hip circumference, waist circumference, TG, LDL, and FBS with the risk of developing CVDs. Then, we examined the correlation between smoking and alcohol variables, LDL and TG, LDL and HDL, as well as waist circumference and hip circumference. A high correlation was observed only between waist circumference and hip circumference (ρ = 0.8. p < 0.0001). For this reason, we did not enter the waist circumference variable into the First Cox multiple regression model. Finally, after performing multiple Cox regression to control the confounders, we found that with increasing age, the risk of developing CVDs increased, so that the risk of developing CVDs in individuals was 2.4 times higher in the age group of 50–60 years and 3.7 times higher in individuals aged 60–70 years than the 40–50-year-old subjects. The risk of developing CVDs in men was 2.3 times higher than in women (HRadj: 2.3, 95% CI 1.7–3.2); in individuals with chronic kidney disease, it was almost 3.4 times higher than in participants without chronic kidney disease. (HRadj: 3.4, 95% CI 1.3–8.7). People with diabetes were 2.3 times more likely to develop CVDs than non-diabetics. The risk of CVDs in the subjects with hypertension was 68% higher than those without hypertension; also, in subjects who consumed alcohol, it was 58% higher. There was also a small but statistically significant positive relationship between LDL and the risk of CVDs (Table 3).
Discussion
This study estimated the incidence and risk factors of CVDs in adults 40–70 years in Kharameh. In this study, 9442 subjects were followed for 4 years. The density incidence in the present study was estimated to be 6.9 cases per 1000 person-year. In the study of Framingham that conducted by Donald et al., the incidence of CVDs was estimated at 15.7 cases per 1000 person-year [16]. The reason for the difference in incidence density between our study and the study by Donald et al. is probably due to the age difference of the cohort under study; Donald's study included people 50 years and above, and our study was done on 40 to 70-year-old subjects.
In this study, after the age of 60–70 years, chronic kidney disease was identified as the strongest risk factor for CVDs. In another study, in line with the results of the present study, it was stated that kidney dysfunction could double the risk of developing CVDs [17]. Chen et al. also, in their study on people aged 35–65 years who had kidney disease, stated that the risk of developing CVDs in patients with chronic kidney disease was 3.8 times higher than those without it [18]. However, there are several specific factors in chronic kidney patients that may increase the risk of developing CVDs, for example, anemia due to kidney disease, albuminuria, hyperparathyroidism, and oxidative stress [19]. Anemia due to impaired renal function causes left ventricular dysfunction and left ventricular hypertrophy, leading to CVDs and increasing mortality risk fourfold. Other studies have shown that albuminuria plays an important role in the pathogenesis of CVDs and increases the risk of these diseases by 2 to 4 times [19]. Although the rate of CVD is high in those with kidney disease in our study, there were only 31 subjects (0.33% in Table 1), with a total of 4 subjects who eventually developed CVD. However, health policy makers should recognize this to identify and implement appropriate interventions.
Diabetes was also introduced as another risk factor in this study. Dinesh Shah et al. in their cohort study in England on diabetic people over 30 years reported a positive and significant relationship between diabetes and the risk of developing CVDs [20]. Donald and colleagues in the Framingham Cohort Study of people over 50 years of age also identified diabetes as the strongest risk factor for CVDs [16]. In addition, Lee et al. in a cohort study of 2879 men in Singapore reported that the risk of developing CVDs in diabetics was 1.77 times higher than non-diabetics [21]. In Iran, the attributed risk of diabetes for CVDs is reported to be 7.3% [22]. However, many risk factors for diabetes and CVDs are common, such as the role of obesity, age over 45, unhealthy diet, hypertension, stress, and smoking, the role of which cannot be ignored [22]. Furthermore, an unhealthy lifestyle is very common in diabetics, especially the non-elderly and those with academic education [23]. Due to the impact of lifestyle on the incidence of diabetes as a modifiable risk factor for CVDs, health policymakers should develop more up-to-date guidelines to prevent CVDs in individuals with diabetes by modifying their lifestyle [23]. On the other hand, screening for type-2 diabetes is an important strategy to reduce the incidence of CVDs. A study in Denmark showed that screening middle-aged people significantly reduced the risk of all types of CVDs in individuals with diabetes [24].
In the present study, the risk of CVDs in subjects with hypertension was 64% higher than those without it. Donald et al. also in the Framingham Cohort Study of people over 50 years stated that hypertension was significantly associated with the risk of CVDs [16]. A cohort study conducted in Singapore also reported hypertension as the strongest risk factor for CVDs [21]. In another study in Iran, the risk of CVD attributed to hypertension was reported to be 36% [5]. We must remember that hypertension is an important, independent, and modifiable risk factor for CVDs and causes 50% of heart attacks [20]. In Iran, the prevalence of hypertension in individuals aged 40–75 years is estimated at 26.9%. This increase in the prevalence of hypertension is related to changes in individuals' lifestyles, increasing urbanization, and increasing life expectancy [5]. It is, therefore, recommended that the lifestyle should be modified [22].
In this study, the CVDs incidence rate was twice higher in men than in women. In line with the results of our study, another study in south India reported the prevalence of CVDs in men more than women [25]. The prevalence of CVDs in the two sexes is generally different due to several factors, including biological factors and sex hormones, especially estrogens and androgens [26]. The prevalence of CVDs before 50 is higher in men than women and increases in women due to menopause and hormonal changes. In addition, pregnancy-related factors such as diabetes and blood pressure, preeclampsia, and hormonal changes are among the factors that can play a protective role for women [20].
The present study showed that alcohol consumption increased the CVDs incidence rate by 58%. Lee and colleagues in their cohort study in Singapore reported that alcohol played a protective role against CVDs, and stated that the lack of alcohol consumption increased the risk of CVDs 1.8 times [21]. The results of this study were not in the same line with those of the present study. Rehm et al. in their modeling study using WHO data also stated that moderate or low alcohol consumption had no beneficial effect on the risk of CVDs [27]. Another study found that consuming every 30 g of alcohol increased the HDL by 3.66 Mg/dl and Apo Lipoprotein by 8.76 Mg/dl. These factors have a protective role against CVDs [27]. However, we should note that for some reason, including cultural and religious issues in Iran, individuals may not report their alcohol consumption, and there is a probability of underestimation.
In the present study, a significant relationship was seen between the LDL level and risk of developing CVDs. The results of a cohort study in Iran on 8698 people aged 35 to 65 showed that the risk of developing CVDs was 1.54 times higher with increasing levels of LDL [28]. Wilson in a cohort study in Europe and Wallece et al. in their cohort study on 30–74-year-old subjects also reported a direct and significant relationship between LDL levels and the risk of developing CVDs [29, 30]. Two clinical trial studies have shown that the risk of developing CVDs in patients with dyslipidemia is reduced by treating these individuals with a statin drug that reduces dyslipidemia [31, 32].
This study showed a statistically significant relationship between aging and the risk of developing CVDs. In line with the results of our study, Ravi and colleagues stated that the risk of CVD increased with age. They have found that although increasing age has an independent role in the occurrence of CVD, it can be a reflection of the intensity and duration of exposure to other risk factors of CVD [33].
The present study found no statistically significant relationship between BMI and CVDs. However, contrary to the results of our study, overweight and obesity have been suggested as the risk factors for CVDs in many studies [34,35,36,37]. On the other hand, in some studies, the obesity paradox is mentioned as an important factor in the relationship between obesity and CVDs [38, 39]. It has also been stated that although obesity increases the risk factors of CVDs and has adverse effects on the structure and function of the heart vessels, obese individuals usually have a better prognosis and less mortality due to CVDs. Lavie and his colleagues have stated several factors for the paradox between obesity and CVDs, such as the presence of protective cytokines in obese individuals, poor response to the renin–angiotensin–aldosterone system, and hypertension in these individuals, which leads to the use of cardiac drugs. In addition, other factors are an increase in body muscle mass and muscle strength, presence of genetic factors, and presence of more metabolic reserves [38].
This study is conducted as the continuation of the cross-sectional study by Baaradeh and his colleagues which investigated the prevalence and risk factors of CVD using the baseline data of the Kharamah cohort [34]. We must state that cross-sectional studies are unable to correctly estimate the causal relationships due to the lack of time sequence. For this reason, there is a need to conduct this cohort study to carefully examine the risk factors. In addition, for accurate intervention planning, in addition to knowing the prevalence rate, we also need the incidence rate. In the present study and a cross-sectional study by Baradeh et al., CVDs were associated with old age, diabetes and hypertension. This is despite the fact that in our study CVDs were associated with alcohol consumption and male sex, but in Baeradeh’s study this relationship was not seen. In addition, in Baeradeh’s study, CVDs were associated with high TGs and smoking, but it was not observed in our study.
Strengths and limitations
Compared to many other studies, the cohort design and the coverage of a wide range of risk factors are two important strengths of our study. In addition, our study had a large sample size, which increased its generalizability. However, the main limitation of our study was the average duration of the follow-up period (4 years). In addition, we did not have data on the specific types of cardiovascular diseases for each subject. For this reason, we could not calculate the incidence of these diseases separately.
Conclusion
The present study showed that aging was a risk factor for developing CVDs. In addition, except for age, other identified risk factors are modifiable, such as diabetes, hypertension, and alcohol consumption; however, a large share of cardiovascular events can be reduced by modifying these factors. Therefore, determining interventional strategies and planning to implement appropriate interventions to control and eliminate the risk factors affecting the incidence of CVDs are essential in preventing the occurrence of CVDs. In addition, early disease detection in individuals with risk factors and their control can reduce the risk of CVDs and their burden on the society and individuals.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CVDs:
-
Cardiovascular diseases
- DALYs:
-
Disability adjusted life years
- BMI:
-
Body mass index
- FBS:
-
Fasting blood sugar
- LDL:
-
Low-density lipoprotein
- TG:
-
Triglyceride
- HDL:
-
High-density lipoprotein
- PCA:
-
Principal component analysis
References
Kaptoge S, Pennells L, De Bacquer D, Cooney MT, Kavousi M, Stevens G, Riley LM, Savin S, Khan T, Altay S. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332–45.
Mamani-Ortiz Y, San Sebastián M, Armaza AX, Luizaga JM, Illanes DE, Ferrel M, Mosquera PA. Prevalence and determinants of cardiovascular disease risk factors using the WHO STEPS approach in Cochabamba, Bolivia. BMC Public Health. 2019;19(1):1–13.
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, Brauer M, Kutty VR, Gupta R, Wielgosz A. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–808.
Celermajer DS, Chow CK, Marijon E, Anstey NM, Woo KS. Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detection. J Am Coll Cardiol. 2012;60(14):1207–16.
Sarrafzadegan N, Mohammadifard N. Cardiovascular disease in Iran in the last 40 years: prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. 2019.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Mensah GA, Roth GA, Fuster V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. American College of Cardiology Foundation Washington, DC; 2019. p. 2529–32.
Rezaei Hachesu V, Naderyan Feli S, Zare Sakhvidi MJ. Prevalence of cardiovascular risk factors among taxi drivers in Yazd, Iran, 2016. J Community Health Res. 2017;6(4):200–6.
Rezaei F, Seif M, Fattahi MR, Gandomkar A, Hasanzadeh J. Estimation of 10-year risk of cardiovascular diseases using WHO risk prediction charts: a population-based study in southern Iran. Iran J Public Health. 2022;51(7):1667–76.
Najafipour H, Afshari M, Rostamzadeh F. Prevalence of multiple coronary artery disease risk factors in Kerman: a population-based study in Southeast Iran. Iran J Med Sci. 2018;43(2):140.
Rosengren A, Smyth A, Rangarajan S, Ramasundarahettige C, Bangdiwala SI, AlHabib KF, Avezum A, Boström KB, Chifamba J, Gulec S. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Glob Health. 2019;7(6):e748–60.
Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar AA, Hekmatdoost A, Mohammadi Z, Mahmoudi Z, Shayanrad A, Roozafzai F, Sheikh M, Jalaeikhoo A, Somi MH, Mansour-Ghanaei F, Najafi F, Bahramali E, Mehrparvar A, Ansari-Moghaddam A, Enayati AA, Esmaeili Nadimi A, Rezaianzadeh A, Saki N, Alipour F, Kelishadi R, Rahimi-Movaghar A, Aminisani N, Boffetta P, Malekzadeh R. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. 2018;187(4):647–55. https://doi.org/10.1093/aje/kwx314.
Moftakhar L, Jafari F, Ghoddusi Johari M, Rezaeianzadeh R, Hosseini SV, Rezaianzadeh A. Prevalence and risk factors of kidney stone disease in population aged 40–70 years old in Kharameh cohort study: a cross-sectional population-based study in southern Iran. BMC Urol. 2022;22(1):1–9.
Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan. 2006;21(6):459–68. https://doi.org/10.1093/heapol/czl029.
Organization. OWOpamtgeRoaWHOCGWH. WHO Obesity Technical Report Series 2000:284:56
Lloyd-Jones DM, Leip EP, Larson MG, d’Agostino RB, Beiser A, Wilson PW, Wolf PA, Levy D. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation. 2006;113(6):791–8.
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJL, Mann JF, Matsushita K, Wen CP. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339–52.
Chen S, Hsu W-Y, Lin Y-N, Wang C-Y, Wu C-H, Chang K-H. Incidence and risk of major adverse cardiovascular events in middle-aged patients with chronic kidney disease: a population-based cohort study. Int Urol Nephrol. 2019;51(7):1219–27.
Subbiah AK, Chhabra YK, Mahajan S. Cardiovascular disease in patients with chronic kidney disease: a neglected subgroup. Heart Asia. 2016;8(2):56–61.
Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1· 9 million people. Lancet Diabetes Endocrinol. 2015;3(2):105–13.
Lee J, Heng D, Chia KS, Chew SK, Tan BY, Hughes K. Risk factors and incident coronary heart disease in Chinese, Malay and Asian Indian males: the Singapore Cardiovascular Cohort Study. Int J Epidemiol. 2001;30(5):983–8.
Pirani N, Khiavi FF. Population attributable fraction for cardiovascular diseases risk factors in selected countries: a comparative study. Mater Sociomed. 2017;29(1):35.
Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):1–19.
Simmons RK, Griffin SJ, Lauritzen T, Sandbæk A. Effect of screening for type 2 diabetes on risk of cardiovascular disease and mortality: a controlled trial among 139,075 individuals diagnosed with diabetes in Denmark between 2001 and 2009. Diabetologia. 2017;60(11):2192–9.
Krishnan M, Zachariah G, Venugopal K, Mohanan P, Harikrishnan S, Sanjay G, Jeyaseelan L, Thankappan K. Prevalence of coronary artery disease and its risk factors in Kerala, South India: a community-based cross-sectional study. BMC Cardiovasc Disord. 2016;16(1):1–12.
Arnold AP, Cassis LA, Eghbali M, Reue K, Sandberg K. Sex hormones and sex chromosomes cause sex differences in the development of cardiovascular diseases. Arterioscler Thromb Vasc Biol. 2017;37(5):746–56.
Rehm J, Shield KD, Roerecke M, Gmel G. Modelling the impact of alcohol consumption on cardiovascular disease mortality for comparative risk assessments: an overview. BMC Public Health. 2016;16(1):1–9.
Hedayatnia M, Asadi Z, Zare-Feyzabadi R, Yaghooti-Khorasani M, Ghazizadeh H, Ghaffarian-Zirak R, Nosrati-Tirkani A, Mohammadi-Bajgiran M, Rohban M, Sadabadi F, Rahimi HR, Ghalandari M, Ghaffari MS, Yousefi A, Pouresmaeili E, Besharatlou MR, Moohebati M, Ferns GA, Esmaily H, Ghayour-Mobarhan M. Dyslipidemia and cardiovascular disease risk among the MASHAD study population. Lipids Health Dis. 2020;19(1):42. https://doi.org/10.1186/s12944-020-01204-y.
Wallace C, Newhouse SJ, Braund P, Zhang F, Tobin M, Falchi M, Ahmadi K, Dobson RJ, Marçano ACB, Hajat C. Genome-wide association study identifies genes for biomarkers of cardiovascular disease: serum urate and dyslipidemia. Am J Med Genet A. 2008;82(1):139–49.
Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circ. 1998;97(18):1837–47.
Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, Kuder JF, Wang H, Liu T, Wasserman SM. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med Overseas. 2017;376(18):1713–22.
Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, Edelberg JM, Goodman SG, Hanotin C, Harrington RA. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med Overseas. 2018;379(22):2097–107.
Dhingra R, Vasan RS. Age as a risk factor. Med Clin. 2012;96(1):87–91.
Baeradeh N, Ghoddusi Johari M, Moftakhar L, Rezaeianzadeh R, Hosseini SV, Rezaianzadeh A. The prevalence and predictors of cardiovascular diseases in Kherameh cohort study: a population-based study on 10,663 people in southern Iran. BMC Cardiovasc Disord. 2022;22(1):1–12.
Eckel N, Li Y, Kuxhaus O, Stefan N, Hu FB, Schulze MB. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses’ Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018;6(9):714–24.
Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, Kannel WB, Vasan RS. Obesity and the risk of heart failure. N Engl J Med Overseas. 2002;347(5):305–13.
Silventoinen K, Magnusson PK, Tynelius P, Batty GD, Rasmussen F. Association of body size and muscle strength with incidence of coronary heart disease and cerebrovascular diseases: a population-based cohort study of one million Swedish men. Int J Epidemiol. 2009;38(1):110–8.
Lavie CJ, De Schutter A, Parto P, Jahangir E, Kokkinos P, Ortega FB, Arena R, Milani RV. Obesity and prevalence of cardiovascular diseases and prognosis—the obesity paradox updated. Prog Cardiovasc Dis. 2016;58(5):537–47.
Mandviwala T, Khalid U, Deswal A. Obesity and cardiovascular disease: a risk factor or a risk marker? Curr Atheroscler Rep. 2016;18(5):1–10.
Acknowledgements
The authors are grateful to the officers and data management staff of Kharameh cohort.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Gh.M was responsible for the field working including data collection and management. R.A analyzed the data and wrote the method and parts of manuscript. H.SV collected the data. S.M checked all analyses, graphs and tables and managed how to analyze them. M. L, H.SV, and D. SS also wrote a part of manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
PERSIAN Cohort Study is being performed in 18 geographical regions of Iran. PERSIAN Cohort Study was approved by the Ethics Committee of the Ministry of Health and Medical Education. This study was done in accordance with the Helsinki Declaration and Iranian national guidelines for ethics in research. This research is extracted from a Ph.D. dissertation under the supervision of Dr. Abbas Rezaianzadeh. It has also been approved by the ethics committee of Shiraz University of Medical Sciences. (IR.SUMS.SCHEANUT.REC.1400.046)
Consent for publication
Written informed consent for publication was obtained from each participant.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rezaianzadeh, A., Moftakhar, L., Seif, M. et al. Incidence and risk factors of cardiovascular disease among population aged 40–70 years: a population-based cohort study in the South of Iran. Trop Med Health 51, 35 (2023). https://doi.org/10.1186/s41182-023-00527-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41182-023-00527-7