
Abstract
Background
Cardiovascular diseases (CVDs) were the number one cause of death in Iran. The main risk factors of CVDs include unhealthy lifestyles, insulin resistance, hypertension (HTN), and hyperlipidemia. Given that there are modifiable risk factors for CVDs, this cross-sectional study aimed to evaluate the prevalence of CVDs and their risk factors among adults.
Methods
The present cross-sectional study was conducted on 9828 adults 35–70 years (both sexes). The demographic data, lifestyle habits, anthropometric data, and clinical and biochemical parameters were collected from the baseline data of the Hoveyzeh Cohort Study. The odds ratio (OR) of CVDs was assessed by multivariable logistic regression.
Results
The prevalence of CVDs was higher in females than males (16.2 vs. 12.6, p ≤ 0.001). The prevalence of CVDs was related to age, gender, marital status, lifestyle, anthropometric measurements, cholesterol, high-density lipoprotein, HTN, and fasting plasma glucose (FPG) (p ≤ 0.05). The participants aged 65–70 y showed the highest odds of CVDs (OR: 3.97, 95% CI: (3.14, 5.01), (p ≤ 0.001)). Males (OR: 1.76, 95% CI: (1.51, 2.05), p ≤ 0.001), married status (OR: 1.63, 95% CI: (1.08, 2.47), p = 0.021), more using a mobile phone (OR: 1.26, 95% CI: (1.09, 1.46), p ≤ 0.002), and smoking cigarettes (OR: 1.44, 95% CI: (1.24, 1.68), p ≤ 0.001) associated with CVDs. Higher odds of CVDs were related to low physical activity (PA) (OR: 1.56, 95% CI: (1.34, 1.8), p ≤ 0.001), body mass index > 30 (OR: 1.68, 95% CI: (1.01, 2.8), p ≤ 0.047). Moreover, odds of CVDs were related to systolic blood pressure (SBP) ≥ 140 mm Hg (OR: 1.25, 95% CI: (1.04, 1.51), p = 0.017), FPG = 100–126 mg/dl (OR: 1.24, 95% CI: (1.07, 1.43), p = 0.003), and FPG > 126 mg/dl (OR: 1.71, 95% CI: (1.47, 1. 98), p ≤ 0.001).
Conclusion
The present study showed the main risk factors of CVDs were older age, married status, using a mobile phone, low PA, smoking, obesity, and abnormal FPG and SBP. The lower odds of CVDs were found in the participants with normal cholesterol.
Similar content being viewed by others


Introduction
Cardiovascular diseases (CVDs) are a group of disorders of the heart and blood vessels, including coronary heart disease, cerebrovascular disease, rheumatic heart disease, and other conditions. They are the leading cause of death globally [1]. Their Symptoms may be caused anywhere in the body and vary depending on the specific situation. According to the World Health Organization (WHO), an estimated 17.9 million lives are taken by CVDs each year. More than 80% of CVD deaths are due to heart attacks and strokes, and one-third of these deaths occur prematurely in people under 70 years of age [1, 2].
The first leading cause of mortality and a million disability-adjusted life years (DALYs) in Iran emanated from CVDs. Moreover, CVDs can lead to 46% of all deaths and 20%-23% of the burden of disease in Iran [3]. Compared to 2005, DALYs related to CVDs are predicted twofold in 2025 among Iranians aged ≥ 30 years. However, the prevalence among men will still be higher than among women; the difference will be less in 2025 [4].
The risk factors of CVDs are a variety. Some of them include inappropriate diet, physical inactivity, smoking, harmful use of alcohol, industrialization, urbanization, cultural changes, socioeconomic status, wealth index, and increasing life expectancy [1, 3, 5, 6]. In addition, people with high glucose, hypertension (HTN), hyperlipidemia, and increased body mass index (BMI) may be more exposed to the risk factors of CVDs [2, 5].
Although the evidence for the association between some risk factors and CVDs is relatively strong, clarifying the high-risk patients, the trend of prevalence and risk factors of CVDs seem necessary based on the demographic characteristics, history of diseases, socioeconomic status, and lifestyle behaviors in the different populations [1, 5, 7]. On the other hand, as was previously published, some non-communicable diseases (obesity, prediabetes, dyslipidemia, and HTN) were high among adults from Hoveyzeh [8]. So, the present study was designed to determine the prevalence and risk factors of CVDs among adults aged 35–70 years from southwest Iran (Baseline data from Hoveyzeh Cohort Study).
Methods
Study population and sampling methods
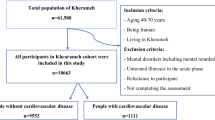
The present cross-sectional study was conducted on the baseline data from the Prospective Epidemiological Studies of the Iranian Adult and Neonates (PERSIAN), Hoveyzeh Cohort Study (HCS). ‘in the HCS, it was targeted to sample the entire study population (adults aged 35–70), but only 85.16% agreed to respond to the survey. However, the total adults aged 35–70 years was 12,103 in Hoveyzeh (Arab community), Khuzestan Province, southwest Iran,. Therefore, 10,009 people (85.16%) were recruited in HCS [8]. Data collection was from May 23, 2016, to August 28, 2018. The Non-responder of the study were 2094 people (Responders = 10,009) (the causes were mentioned in Fig. 1). The pregnant women (n = 163) and women who were unaware of pregnancy (n = 17) were excluded from the study N = 180 excluded population (Fig. 1). Therefore, 9829of 10,009 had the criteria for the present study. The pregnant women (n = 163) and women who were unaware of pregnancy (n = 17) were excluded from the survey N = 180 excluded population (Fig. 1).

Flowchart of the participation in the present study (Hoveyzeh Cohort Study)
A voluntary and written informed consent was obtained from the research participants. The details of their recruitments were previously published [8]. The Ethics Committee of Ahvaz Jundishapur University of Medical Sciences has approved the present study (Ethical code: IR.AJUMS.REC.1398.761).
Measurements
The following information was obtained from all participants:
-
Demographic data (sex, age, marital status) in the past year and Wealth index in the past and current.
-
Physical activity (PA) in the past year and personal habits (using a cell phone (mobile phone), drinking alcohol habit, smoking status, and drug use) in the past and current
-
History of diseases (cardiac ischemic (CI), myocardial infarction (MI), stroke, HTN, prediabetes, and type 2 diabetes mellitus (T2DM)).
-
Anthropometric measurements (BMI, waist circumference (WC), high waist-to-hip ratio (WHR), and hip circumferences (HC))
-
Clinical measures (systolic blood pressure (SBP), and diastolic blood pressure (DBP)), biochemical parameters (fasting plasma glucose (FPG), triglyceride (TG), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C)).
Some information was gathered through interviewer-administered questionnaires by the trained interviewers. CVDs were defined as stroke, CI, and MI in the present study.
The self-reported daily physical activity questionnaire was used to measure metabolic equivalent rates (METs) for all participants' activities [9] (Additional file 1: Table S1). It was categorized into three groups (quantile): the less quantile (inactive), the moderate quantile (moderately active), and the most quantile (active). The questionnaire details are available in (Additional file 1: Table S.1).
The international wealth index was used to measure the socio-economic status of households and calculated by a principal component analysis (PCA), including the means of information on households’ possession (freezers, TV, motorbike, cell phone, car, vacuum cleaners, access to the internet, washing machines, and computers) and household utilities (house ownership and the number of rooms per capita). The wealth index score was categorized into five groups: poorest, poor, moderate, rich, and richest [10].
Anthropometric data were measured in a fasting state in the morning. Height (cm) was measured using a stadiometer (Seca 206), weight (kg) was measured using a standing scale (Seca 755), and WC and HC (cm) were measured using Seca locked tape meters. The WHR and BMI (kg/m2) were calculated by dividing WC (cm) by HC (cm) and body weight (kg) by the square of the height (m2), respectively. BMI were categorized four groups: (a) underweight: BMI < 18.5; (b) normal range: BMI = 18.5 to 24.9, (c) overweight: BMI = 25.0–29.9; obese: BMI > 30. Abnormal WC was defined as ≥ 102 cm in men and ≥ 88 cm in women. A healthy WHR was considered as ≤ 0.85 and ≤ 0.90 for women and men, respectively.
The measures of DBP and SBP were conducted twice (10 min intervals) on each arm, following standard guidelines by Riester Sphygmomanometers. HTN was considered to have an SBP ≥ 140 mm Hg and a DBP ≥ 90 mm Hg at the baseline, have a self-reported history of physician-diagnosed HTN or take antihypertensive medication [11].
The trained laboratory staff collected blood samples at 10–12 h of fasting. First, the serums were obtained by centrifuging the blood samples for 10 min at 3000 rpm at room temperature (Sigma, Germany). Then, the autoanalyzer (BT 1500, Biotecnica Instruments, Italy) was used to measure the required serum levels.
Statistical analysis
The analysis of continuous and categorical variables was conducted by means ± standard deviations (SD) and frequency (number (%)), respectively. In addition, the Chi-square test was used to compare the sociodemographic and lifestyle characteristics by gender. Further, the Chi-square test examined the association of sociodemographic and lifestyle factors with CVD. Finally, the multivariable logistic regression analysis explored all studied risk factors for CVD. The potential cofounders have included sociodemographic and lifestyle characteristics (age, gender, wealth score, marital status, using a mobile phone, smoking cigarettes, drinking alcohol, PA, anthropometric measurements (BMI, WC, WHR), and lipid profiles (TG, cholesterol, HDL)). The backward approach (starting with a full model and dropping the variables) was used for a variable selection. Parameters of the model were estimated through the maximum likelihood. The unadjusted analyses were performed for the potential confounders, and the variables with p < 0.25 in the unadjusted analyses were considered as confounders and included in the final model. The statistical analyses were conducted using the SPSS statistical software package, version 16.0 (SPSS, Inc, Chicago, Illinois, USA). P < 0.05 was considered statistically significant using 2-tailed tests.
Results
Gender-specific sociodemographic and lifestyle characteristics of the respondents
An overall of 9829 participants was included in the present study, of whom 59% were female, and 41% were male. All sociodemographic and lifestyle characteristics of the study population except MI (p = 0.056) and stroke ((p = 0.39) were shown a significant difference between the sexes (Table 1). Only 7.2% of the study population was 65–70 years. The prevalence of history of HTN (26.5%), CI (13.6%), prediabetes (23%), and diabetes (17%) was common in Hoveyzeh.
The distribution of respondents was similar in terms of wealth scores and PA levels. Most of the surveyed population (76%) showed abnormal BMI (overweight (37.2%) and obesity (38.8%)).
The history of HTN, CI, prediabetes, and diabetes in females was significantly higher than in males (p ≤ 0.001). More mobile phone use was shown significantly in females than males (p ≤ 0.001). The history of smoking, drinking alcohol, and using drug abuse was significantly higher in males than females (p ≤ 0.001). Based on the PA levels, there was a significant difference between genders. However, most females (42.1%) had moderate levels of PA, and the percent of women with inactive and active PA levels were similar (29.8 and 28.1%, respectively). Only 20.9% of males had moderate PA levels, while 38.4 and 40.7% were inactive and active, respectively. The prevalence of overweight or obesity was significantly higher in females than in males (p ≤ 0.001).
The prevalence of CVDs by the studied characteristics
Table 2 presents the prevalence of CVDs by the studied characteristics. The increasing trend in age showed a higher prevalence of CVDs (7.5% (35–45 y) vs. 27.9% (65–70 y), p ≤ 0.001). The prevalence of CVDs was higher in females than in males (16.5% vs. 12.6%, p ≤ 0.001). The most and less prevalence of CVDs were reported in widow (24.8%) and single (7.6%) participants (p ≤ 0.001).
The results showed a higher prevalence of inactivity than being active among participants with CVDs (20.7% vs. 10.7%, (p ≤ 0.001). The most prevalence of CVDs was found in participants with obesity (BMI > 30) (17.5%, p ≤ 0.001). In addition, there was a higher prevalence of abnormal compared to the normal WC and WHR (17.5 vs. 11%, p ≤ 0.001 and 15.6% vs. 8.2%, p ≤ 0.001, respectively) among participants with CVDs.
A lower prevalence of abnormal compared to normal cholesterol was shown among participants with CVDs (13.5% vs. 15.7%, p = 0.003). Conversely, a higher prevalence of abnormal compared to normal HDL was shown in CVDs (16.5% vs. 13.9%, p ≤ 0.001).
The prevalence of abnormal SBP (23.1% vs. 14.2%, p ≤ 0.001) and DBP (19.1% vs. 14.6%, p = 0.002) was more common in CVDs. The most prevalence of CVDs was among participants with FPG (> 126 mg/dl) compared to FPG (≤ 100 mg/dl) (23.7% vs. 11.5%, p = 0.001) compared to the normal FPG.
There were no significant differences between using a mobile (p = 0.243), drinking alcohol (p = 0.888), the levels of wealth index (p = 0.22) or TG levels in participants with CVDs (p = 0.521).
Association of risk factors with CVD
The crude and adjusted analysis for evaluating the association between all characteristics and CVDs was presented in Table 3. The results of crude analyses were not presented in this part.
In the adjusted analyses, the participants aged 65–70 y showed the most odds of CVDs (OR: 3.97, 95% CI: (3.14, 5.01), (p ≤ 0.001)). The higher odds of CVDs were reported in the participants age 45–55 y (OR: 3.35, 95% CI: (2.82, 3.99), (p ≤ 0.001)) and 55–65 y (OR: 2.02, 95% CI: (1.72, 2.37), (p ≤ 0.001)) in comparison with the participants aged 35–45 y.
In addition, CVDs were associated with males (OR: 1.76, 95% CI: (1.51, 2.05), p ≤ 0.001), married status (OR: 1.63, 95% CI: (1.08, 2.47), p = 0.021), more using a mobile phone (OR: 1.26, 95% CI: (1.09, 1.46), p ≤ 0.002), and smoking cigarettes (OR: 1.44, 95% CI: (1.24, 1.68), p ≤ 0.001). Moreover, higher odds of CVDs were found in the participants with low PA (OR: 1.56, 95% CI: (1.34, 1.8), p ≤ 0.001) and BMI > 30 (kg/m2) (OR: 1.68, 95% CI: (1.01, 2.8), p ≤ 0.047). Further, SBP ≥ 140 mm Hg (OR: 1.25, 95% CI: (1.04, 1.51), p = 0.017), FPG = 100–126 mg/dl (OR: 1.24, 95% CI: (1.07, 1.43), p = 0.003), and FPG > 126 mg/dl (OR: 1.71, 95% CI: (1.47, 1. 98), p ≤ 0.001) were associated to CVDs. People with cholesterol < 200 mg/dl (OR: 0.69, 95% CI: (0.61, 0.79), p ≤ 0.001) showed lower odds of CVDs compared to whom with cholesterol > 200 mg/dl. It was found no odds of CVD with other factors, including wealth index, alcohol drinking, moderate PA, normal and overweight, WC, WHR, TG, HDL-C, DBP, widow, and divorced status.
Discussion
The present findings showed: (1) the main risk factors of CVDs were age, married status, mobile phone use, low PA, smoking, obesity, and abnormal FPG and SBP; (2) lower odds of CVDs were shown in participants with normal cholesterol; (3) there was a high prevalence of the components of CVDs (CI, MI, and stroke), HTN, prediabetes, T2DM, overweight, and obesity in Hoveyzeh, especially among females; (4) The prevalence of CVDs was related to older age, female, widow, smoking cigarettes, low PA, DBP ≥ 90 mmHg, SBP ≥ 140 mmHg, abnormal WC, WHR, and FPG, and obesity.
In agreement with the present study, the previous studies reported the prevalence of CVDs was higher in Iranians with dyslipidemia [12]. Moreover, the prevalence of dyslipidemia, overweight, obesity, HTN, prediabetes, low PA, and current smoking was high in the Gulf region (Iran, Kuwait, Oman, United Arab Emirates, Bahrain, etc.) [13,14,15], which was similar the present findings. A meta-analysis (2018) conducted by Akbartabar Toori showed that dyslipidemia was high in the Iranian population of different races [12]. The present study showed the prevalence and risk factors of CVDs in the Arab community.
In the United Arab Emirates, a greater risk of CVDs was reported in men than women. According to the previous studies, the risk factors of CVDs include overweight, obesity, smoking, HTN, low PA, and DM in the United Arab Emirates and the Eastern Mediterranean region [12, 15, 16], which were similar to the result of the present study.
Higher odds of CVDs were related to an unhealthy lifestyle (smoking, mobile phone use, obesity, and low PA). However, the previous findings showed the positive effects of PA in reducing risk factors and the initiation of CVDs [16, 17], and details on the mechanism remain largely unclear.
The regular and appropriate PA and the type and amount of PA, regardless of gender and age, are the critical factors in CVDs that should be considered [18,19,20].
The protective effect of PA on CVDs might be mediated by improving metabolic and inflammatory risk markers and balance in energy expenditure, which finally leads to controlling HTN, diabetes, obesity, and reducing the risk of stroke, both ischemic and hemorrhagic [21, 22].
Apart from active smoking, passive smoking (exposure to environmental tobacco smoke) plays a significant role in CVDs [23]. Unfortunately, inactive smokers were not identified in the present research. Smoking cigarettes develop some risk factors for CVDs following as glucose intolerance, dyslipidemia, thrombus formation, inflammation, and oxidative stress as a potential mechanism for directly initiating CVDs [23, 24]. However, in the present study, higher odds of CVDs were related to BMI ≥ 30 kg/m2, the p-value was negligible (p = 0.047). The previous findings also showed obesity and, especially, severe obesity (BMI ≥ 35 kg/m2) were consistently and strongly related to a higher risk of CVDs [25]; still, the duration of obesity or delaying the onset of obesity may have significant CV health benefits. Therefore, it should not be assumed that only obesity is the leading risk factor for CVDs regardless of other metabolic profiles.
A meta-analysis showed overall correlations between CVD risk factors and anthropometric adiposity measures, including BMI, WC, WHR, waist-to-height ratio, and body fat percentage, had little significance. Moreover, the measurement of WC was more related to CVD risk factors in men and women than BMI [24] in disagrees with the present results.
However, the previous studies showed that increased TG [25] and low HDL-C were associated with an increased risk of CVDs, [25, 26]; TG and HDL-C did not have any significant changes related to CVDs risk in the present study. Moreover, the higher prevalence of CVDs was not shown in participants with abnormal TG. It may be due to taking medications from the participants with CVDs.
Therefore, it seems necessary to evaluate other lipid profiles such as total cholesterol/HDL-C and TG/HDL-C ratio and Apolipoproteins [25].
Insulin resistance is a major feature of T2DM. Moreover, it is associated with several metabolic abnormalities such as elevated CVDs risk. Therefore, independent of glucose control, improving insulin sensitivity is expected to reduce dysglycemia, which is considered the risk of CVDs in patients with T2DM [27].
Limitations and strengths
The present study had some limitations, including (1) the age of the participants was restricted to the 35–70-year age group; therefore, the results cannot be generalized to younger or older age groups; (2) the estimated prevalence of CVDs may be reported less than reality due to only CI, MI, and stroke were considered as CVDs (other types of CVDs include coronary heart disease, peripheral arterial disease, rheumatic heart disease, congenital heart disease, etc. were not evaluated); (3) As it was a cross-sectional study, the causal relationships could not have been established between the risk factors and CVDs; (4) sociodemographic information may induce measurement error due to self-reported collection. However, it is noteworthy that it was tried to minimize the errors with strict quality control of data collection procedures by extensively the trained collectors (5) the evaluation of other lipid profiles (total cholesterol/HDL-C and TG/HDL-C ratio and Apolipoproteins) may be to more accurately estimate CVD risk factors [25]
The strengths of the present studies were the large sample size, which includes both males and females, and a wide range of variables, including demographic, socioeconomic, lifestyle, clinical, and biochemical factors likely to be associated with CVDs was collected from the participants. In addition, it was the first time a large sample size from the Arab community of Iran was evaluated. Moreover, the participants were from Iran, a country in the Gulf area, the Middle East, where the publication of CVD papers still lags behind developed countries and needs to conduct more excellent research [28].
It is no secret that there are other risk factors such as dietary intake [25], resting heart rate [29], other biochemical parameters (insulin resistance [27], LDL, total cholesterol/HDL-C and TG/HDL-C ratio and Apolipoproteins [25]) that should be evaluated in this population. Furthermore, the present findings can have generalized to a large area of southwestern Iran and southern Iraq due to having similarities in terms of race, ethnicity, culture, and lifestyle. Furthermore, the findings controlled multiple potential confounders using multivariable logistic regression models. Finally, our results provided valuable information for the health policymakers to prevent and control CVDs by identifying the risk factors for CVDs.
Given that some risk factors were controllable and preventable; health policymakers should pay further attention to amending them to reduce the prevalence of CVDs in Iran. Moreover, the role of gender in the incidence of CVDs is notable due to the function of various genes which regulate telomerase activity and sexual hormones (estrogens) [17].
Conclusion
Among Hoveyzeh adults, the greater odds of CVDs were related to older age, married status, mobile phone use, low PA, smoking, obesity, and abnormal FPG and SBP. Moreover, lower odds of CVDs were related to normal cholesterol; 3) The prevalence of CVDs was related to older age, female, widow, smoking cigarettes, low PA, DBP ≥ 90 mmHg, SBP ≥ 140 mmHg, abnormal WC, WHR, and FPG, and obesity. The present findings showed that the preventable risk factors of CVDs, including unhealthy lifestyles, play a sustainable role. Hence, the health ministry's agenda should be to design and implement long-term public health programs to achieve a healthy lifestyle. It also suggests that similar studies will be conducted in neighborhood countries on the Arab community to identify the role of race, ethnicity, and culture.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Cardiac ischemic
- CVDs:
-
Cardiovascular diseases
- DBP:
-
Diastolic blood pressure
- DALYs:
-
Disability-adjusted life years
- FPG:
-
Fasting plasma glucose
- HC:
-
Hip circumferences
- HCS:
-
Hoveyzeh Cohort Study
- HDL-C:
-
High-density lipoprotein cholesterol
- MI:
-
Myocardial infarction
- PA:
-
Physical activity
- PERSIAN:
-
Prospective epidemiological studies of the Iranian Adult and Neonates
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviations
- T2DM:
-
Type 2 diabetes mellitus
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- WC:
-
Waist circumference
- WHO:
-
World health organization
- WHR:
-
High waist-to-hip ratio
References
https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) World Health Organization: World Health Organization; 2021
https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 World Health Organization2021
Sarrafzadegan N, Mohammmadifard N. Cardiovascular disease in Iran in the last 40 years: prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran Med. 2019;22(4):204–10.
Sadeghi M, Haghdoost AA, Bahrampour A, Dehghani M. Modeling the burden of cardiovascular diseases in Iran from 2005 to 2025: the impact of demographic changes. Iran J Public Health. 2017;46(4):506.
Balakumar P, Maung-U K, Jagadeesh G. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharmacol Res. 2016;113:600–9.
Rarau P, Pulford J, Gouda H, Phuanukoonon S, Bullen C, Scragg R, et al. Socio-economic status and behavioural and cardiovascular risk factors in Papua New Guinea: A cross-sectional survey. PLoS ONE. 2019;14(1): e0211068.
Yan R, Li W, Yin L, Wang Y, Bo J, Investigators PC, et al. Cardiovascular diseases and risk-factor burden in urban and rural communities in high-, middle-, and low-income regions of china: a large community-based epidemiological study. J Am Heart Assoc. 2017;6(2): e004445.
Cheraghian B, Hashemi SJ, Hosseini SA, Poustchi H, Rahimi Z, Sarvandian S, et al. Cohort profile: The Hoveyzeh Cohort Study (HCS): A prospective population-based study on non-communicable diseases in an Arab community of Southwest Iran. Med J Islam Repub Iran. 2020;34:141.
Kazemi Karyani A, Karmi Matin B, Soltani S, Rezaei S, Soofi M, Salimi Y, et al. Socioeconomic gradient in physical activity: findings from the PERSIAN cohort study. BMC Public Health. 2019;19(1):1–11.
Smits J, Steendijk R. The international wealth index (IWI). Soc Indic Res. 2015;122(1):65–85.
Kanegae H, Oikawa T, Okawara Y, Hoshide S, Kario K. Which blood pressure measurement, systolic or diastolic, better predicts future hypertension in normotensive young adults? J Clin Hypertens (Greenwich). 2017;19(6):603–10.
Akbartabar Toori MP, Kiani FM, Sayehmiri FP, Sayehmiri KP, Mohsenzadeh YM, Ostovar RP, et al. Prevalence of Hypercholesterolemia, High LDL, and Low HDL in Iran: A systematic review and meta-analysis. Iran J Med Sci. 2018;43(5):449–65.
Sadeghi M, Talaei M, Oveisgharan S, Rabiei K, Dianatkhah M, Bahonar A, et al. The cumulative incidence of conventional risk factors of cardiovascular disease and their population attributable risk in an Iranian population: The Isfahan Cohort Study. Adv Biomed Res. 2014;3(242):1–9.
Hashemi SJ, Karandish M, Cheraghian B, Azhdari M. Prevalence of prediabetes and associated factors in southwest iran: results from Hoveyzeh cohort study. BMC Endocr Disord. 2022;22(1):1–10.
Aljefree N, Ahmed F. Prevalence of cardiovascular disease and associated risk factors among adult population in the Gulf region: a systematic review. Adv Publ Health. 2015;2015:1–23.
Zhuo C, Zhao J, Chen M, Lu Y. Physical activity and risks of cardiovascular diseases: a mendelian randomization study. Front Cardiovasc Med. 2021;8(722154):1–9.
Aminian O, Saraei M, Najieb Pour S, Eftekhari S. Association between type of physical activity and risk factors for cardiovascular disease, Islamic Republic of Iran. Eastern mediterranean health journal = La revue de sante de la Mediterranee orientale = al-Majallah al-sihhiyah li-sharq al-mutawassit. 2021;27(11):1061–8.
Al-Shamsi S, Regmi D, Govender RD. Incidence of cardiovascular disease and its associated risk factors in at-risk men and women in the United Arab Emirates: a 9-year retrospective cohort study. BMC Cardiovasc Disord. 2019;19(1):1–9.
Razzak HA, Harbi A, Shelpai W, Qawas A. Prevalence and risk factors of cardiovascular disease in the United Arab Emirates. Hamdan Medical Journal. 2018;11(3):105–11.
Mikkola TS, Gissler M, Merikukka M, Tuomikoski P, Ylikorkala O. Sex differences in age-related cardiovascular mortality. PLoS ONE. 2013;8(5): e63347.
Hamer M, Ingle L, Carroll S, Stamatakis E. Physical activity and cardiovascular mortality risk: possible protective mechanisms. Med Sci Sports Exerc. 2012;44(1):84–8.
Cheng S-J, Yu H-K, Chen Y-C, Chen C-Y, Lien W-C, Yang P-Y, et al. Physical activity and risk of cardiovascular disease among older adults. Int J Gerontol. 2013;7(3):133–6.
Lee PN, Thornton AJ, Forey BA, Hamling JS. Environmental tobacco smoke exposure and risk of stroke in never smokers: an updated review with meta-analysis. J Stroke Cerebrovasc Dis. 2017;26(1):204–16.
Van Dijk S, Takken T, Prinsen E, Wittink H. Different anthropometric adiposity measures and their association with cardiovascular disease risk factors: a meta-analysis. Neth Hear J. 2012;20(5):208–18.
Orozco-Beltran D, Gil-Guillen VF, Redon J, Martin-Moreno JM, Pallares-Carratala V, Navarro-Perez J, et al. Lipid profile, cardiovascular disease and mortality in a Mediterranean high-risk population: The ESCARVAL-RISK study. PLoS ONE. 2017;12(10): e0186196.
Zhao X, Wang D, Qin L. Lipid profile and prognosis in patients with coronary heart disease: a meta-analysis of prospective cohort studies. BMC Cardiovasc Disord. 2021;21(1):1–15.
Abdul-Ghani MA, Jayyousi A, DeFronzo RA, Asaad N, Al-Suwaidi J. Insulin resistance the link between T2DM and CVD: basic mechanisms and clinical implications. Curr Vasc Pharmacol. 2019;17(2):153–63.
Al-Kindi S, Al-Juhaishi T, Haddad F, Taheri S, Abi KC. Cardiovascular disease research activity in the Middle East: a bibliometric analysis. Ther Adv Cardiovasc Dis. 2015;9(3):70–6.
Seviiri M, Lynch BM, Hodge AM, Yang Y, Liew D, English DR, et al. Resting heart rate, temporal changes in resting heart rate, and overall and cause-specific mortality. Heart. 2018;104(13):1076–85.
Acknowledgements
This large population-based study was executed by the cooperation of Iranian Ministry of Health and Medical Education and Ahvaz Jundishapur University of Medical Sciences. The authors sincerely thank all subjects participating in this study. The authors would like to thank all staffs of the Prospective Epidemiological Studies of the Iranian Adult and Neonates (PERSIAN), Hoveyzeh Cohort Study.
Funding
The Iranian Ministry of Health and Medical Education and Ahvaz Jundishapur University of Medical Sciences have contributed to the funding used in the Hoveyzeh Cohort through Grant no. 700/534.
Author information
Authors and Affiliations
Contributions
B.C, M.K, and M.A contributed to designing, supervising, and coordinating the project. SJ.H, B.C, N.D, and H.H contributed to material preparation and data collection. B.C analyzed the data. B.C and M.A contributed to the interpretation of the analyses of data. SJ.H, N.D, H.H, and M.K supervised the project and were responsible for quality control. The first draft of the manuscript was written by M.A. All authors commented on the previous versions of the manuscript and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The study protocol was approved by the Research Ethical Committee of Ahvaz Jundishapur University of Medical Sciences (Ethical code: IR.AJUMS.REC.1398.761) in accordance with the Helsinki Declaration. The written informed consent was obtained from all subjects who participated in Hoveyzeh Cohort.
Consent for publication
The authors confirm that human research participants provided informed consent for publication of their data.
Competing interests
The authors declare that they have any competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file1: Table S1:
General questionnaire including demographic, socioeconomic status, behavior habits, and medical history.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Saki, N., Karandish, M., Cheraghian, B. et al. Prevalence of cardiovascular diseases and associated factors among adults from southwest Iran: Baseline data from Hoveyzeh Cohort Study. BMC Cardiovasc Disord 22, 309 (2022). https://doi.org/10.1186/s12872-022-02746-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02746-y