
Abstract
Introduction
Chloramphenicol is a broad-spectrum antibiotic widely used for treating ophthalmic infections, but concerns about rising bacterial resistance to chloramphenicol have been observed due to its frequent use as an over-the-counter medication. This review assessed the common ophthalmic bacterial pathogens, their chloramphenicol resistance mechanisms, and rates of drug resistance.
Methods
PubMed and Google Scholar databases were searched for relevant publications from the years 2000 to 2022, bordering on ophthalmic bacterial infections, chloramphenicol susceptibility profiles, and drug resistance mechanisms against chloramphenicol. A total of 53 journal publications met the inclusion criteria, with data on the antibiotic susceptibility profiles available in 44 of the reviewed studies, which were extracted and analyzed.
Results
The mean resistance rates to chloramphenicol from antibiotic susceptibility profiles varied between 0% and 74.1%, with the majority of the studies (86.4%) showing chloramphenicol resistance rates below 50%, and more than half (23 out of 44) of the studies showed resistance rates lower than 20%. The majority of the publications (n = 27; 61.4%) were from developed nations, compared to developing nations (n = 14; 31.8%), while a fraction (n = 3; 6.8%) of the studies were regional cohort studies in Europe, with no country-specific drug resistance rates. No pattern of cumulative increase or decrease in ophthalmic bacterial resistance to chloramphenicol was observed.
Conclusions
Chloramphenicol is still active against ophthalmic bacterial infections and is suitable as a topical antibiotic for ophthalmic infections. However, concerns remain about the drug becoming unsuitable in the long run due to some proof of high drug resistance rates.
Similar content being viewed by others


Background
Chloramphenicol is a common ophthalmic drug for treating bacterial eye infections in several countries worldwide. However, in the United States of America (USA) and certain other developed countries, chloramphenicol was banned due to its association with adverse effects, such as aplastic anaemia, acute leukaemia, contact dermatitis and anaphylaxis [1, 2]. It has also been associated with vision loss [3], and as of 2017, the European Medicines Agency (EMA) moved to prohibit the use of chloramphenicol eye drops in children under 2 years of age [4]. However, chloramphenicol is still very much in use in many developing countries, as it is cost-effective and easily accessible. The drug, originally called Chloromycetin, is a broad-spectrum antibiotic that was isolated from the soil bacterium Streptomyces venezuelae in 1947 and is known to function as an inhibitor of protein synthesis, possessing bacteriostatic action [5]. Chloramphenicol belongs to its own antibiotic class, along with its derivates, Florfenicol, Thiamphenicol and Azidamphenicol, which were synthesized by chemical substitutions with fluoro and sulfomethyl groups at specific positions of the primary chloramphenicol molecule [6]. The derivatives thiamphenicol and azidamphenicol are used alongside chloramphenicol in human medicine, while the fluorinated derivative florfenicol is used only in veterinary medicine. As a broad-spectrum antibiotic, chloramphenicol spectrum of activity includes Gram-positive, Gram-negative, anaerobic and aerobic bacteria, as well as other unconventional bacteria, such as mycoplasmas, rickettsia and chlamydia [6].
Chloramphenicol is available in eye drops for treating ophthalmic infections; however, some proof of drug resistance against chloramphenicol have been observed over the years, with some other antibiotics being considered as alternatives for more effective ophthalmic treatment. Ophthalmic chloramphenicol is useful as an over-the-counter medication, because it helps provide quick relief from the discomfort of ocular infections and also reduces the need for clinical consultations over mild ophthalmic infections. This was the rationale behind the decision by the Medicines and Healthcare Products Regulatory Agency (MHRA) of the United Kingdom (UK) to reclassify chloramphenicol eye drops, such that they could be more easily accessible in pharmacy outlets without needing a doctor’s prescription [7]. This move to increase access to safe and effective treatment with chloramphenicol led to a 15.5% fall in the number of doctors’ prescriptions of the drug, from 2.3 million in 2004 to 1.94 million in 2007, and was accompanied by a concomitant rise in over-the-counter pharmacist prescriptions of the drug from 0.68 million in 2005 to 1.46 million in 2007. This further led to a 47.8% increase in total chloramphenicol use between 2004 and 2007 [7]. As a result, the frequent and unregulated use of the drug has been said to be a driving factor for the emergence of chloramphenicol resistance, with growing opinions that there is a high rate of drug resistance to chloramphenicol in the treatment of both ophthalmic and systemic infections [8]. Chloramphenicol is known for its potent inhibitory effect on protein biosynthesis in bacteria, and due to its overuse in the treatment of ophthalmic infections, various mechanisms of resistance to the drug have emerged, either intrinsically developed or acquired through the dispersion of mobile genetic elements conveying chloramphenicol resistance genes, such as plasmids and transposons [9].
The objective of this review is to assess the bacterial pathogens commonly involved in ophthalmic infections, their resistance mechanisms against chloramphenicol, and the rates of drug resistance to chloramphenicol over the years. The research question is to ascertain if chloramphenicol resistance is highly prevalent or not.
Methods
PubMed and Google Scholar databases were searched for relevant publications bordering on ophthalmic bacterial infections, chloramphenicol use, and drug resistance mechanisms associated with chloramphenicol. The search terms used were; chloramphenicol resistance, ophthalmic infections, bacterial pathogens, antibiotic resistance, antibiotic susceptibility, eye treatment, drug efficacy, and drug resistance mechanisms. The inclusion criteria included accessible articles published from 2000 to 2022, related to ophthalmic infections in humans only, specific chloramphenicol resistance mechanisms, and involved chloramphenicol use for susceptibility tests or treatment. Only papers published in the English language were reviewed. Unpublished manuscripts were not included in the review. All publications falling short of these criteria were excluded. The review timeline of 2000–2022 was chosen, because most of the elaborate multicohort studies detailing chloramphenicol drug resistance rates were carried out within this time frame, as opposed to prior years when the topic of chloramphenicol resistance was not regularly explored. A total of 53 journal publications met the inclusion criteria, spanning the prevalent ophthalmic bacterial pathogens, resistance mechanisms, and resistance rates to chloramphenicol. Data on the antibiotic susceptibility and resistance profiles of ophthalmic bacterial pathogens to chloramphenicol were available in 44 of the reviewed studies, which were extracted, analyzed, and discussed to explore the aim of the study. A PRISMA flow diagram of the review and literature selection process is outlined in Fig. 1.

PRISMA flow diagram detailing the steps in obtaining literature for the review
Results
Common bacterial pathogens involved in ophthalmic infections
A number of ocular bacterial infections exist, which include ophthalmic keratitis, conjunctivitis, blepharitis, endophthalmitis, dacryocystitis and orbital cellulitis [6]. It was observed from the reviewed publications that certain genera and species of bacteria were specifically associated with ophthalmic infections and drug resistance patterns. The types of bacterial ophthalmic infections and their commonly associated bacterial pathogens have been outlined in Table 1. Bacterial conjunctivitis was said to be the most prevalent ophthalmic infection, and Staphylococcus spp. was the most common causative bacterial agent in adults, while ophthalmic infections in children were more often caused by Haemophilus influenzae and Streptococcus pneumoniae [10, 11].
Resistance mechanisms against chloramphenicol
A total of 37 chloramphenicol resistance markers were identified among the various ophthalmic bacterial pathogens, of which 23 (62.2%), 9 (24.3%), and 5 (13.5%) were borne on plasmids, transposons and chromosomes, respectively. Two types of chloramphenicol resistance mechanisms were prevalent, which included chloramphenicol acetyltransferase enzymes used to inactivate chloramphenicol by acetylation, and chloramphenicol efflux/export pumps used to actively expel the drug upon its entry into the bacterial cell. The identified genes encoding for chloramphenicol acetyltransferases (cat) were cat I, II, B2–B8, P, and S, while the genes encoding for chloramphenicol exporters (cml) were cml A1, A4, A5, A6, and A7. These resistance mechanisms were either intrinsically developed or acquired by the bacteria through the dispersion of mobile genetic elements conveying the said resistance genes. The details of the identified drug resistance mechanisms are outlined in Table 2.
The rates of drug resistance to chloramphenicol
To assess drug resistance patterns over time, data on the mean susceptibility and resistance rates to chloramphenicol from antimicrobial susceptibility tests (ASTs) were drawn from the reviewed literature, along with information on the country or region and the year in which the studies were carried out or published. Varying rates of drug resistance were observed in various ophthalmic bacterial infections from the reviewed literature, which are outlined in Table 3.
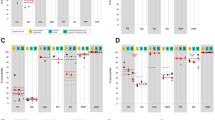
Based on the data from the above reviewed studies, a summary table (Table 4) and graph (Fig. 2) representing the drug resistance rates by country/region from the reviewed literature is depicted below.

Graphical representation of the mean resistance rate to chloramphenicol by country/region
The majority of the publications (n = 27; 61.4%) on drug resistance to chloramphenicol and other antibiotics came from developed nations, which could be attributed to higher research output and frequency of drug resistance monitoring activities, compared to developing nations (n = 14; 31.8%). A fraction (n = 3; 6.8%) of the reviewed studies were regional cohort studies in Europe, which mostly involved the developed European countries, but no country-specific drug resistance rates were given. Among the developing countries, high resistance rates were observed in Iran (69.8%), Nigeria (69.6%) and Ethiopia (68.5%), while the developed countries with high resistance rates were the United Kingdom (74.1%), United States of America (60%) and China (51%). This is in line with similar results from some other publications, which depicted higher antibiotic resistance rates in developing countries than in developed ones due to the overuse of over-the-counter antibiotics-like chloramphenicol that are affordable and easily accessible [5, 8]. Overall, the mean resistance rates to chloramphenicol varied between 0% and 74.1%, with the majority of the studies (86.4%) showing chloramphenicol resistance rates below 50%, and more than half (23 out of 44) of the studies showed resistance rates lower than 20%.. This depicts that high resistance to chloramphenicol was not common among the reviewed studies.
Discussion
The drug resistance markers in the ophthalmic bacterial pathogens identified from the review were present on three genetic elements—plasmids, transposons, and chromosomes. In terms of the resistance mechanisms, the first and most prevalent drug resistance mechanism to chloramphenicol is the enzymatic inactivation of the drug by acetylation via chloramphenicol acetyltransferases (CATs) [56]. These enzymes are genetically encoded on the cat gene and are borne on mobile genetic elements, hence, their role in plasmid-mediated antibiotic resistance [57]. Three types of CATs are known to exist, which include type A, B and C. The type A CATs play important roles in drug resistance against Chloramphenicol and Fusidic acid, while type B CATs, also called xenobiotic acetyltransferases, are known to mediate resistance to chloramphenicol and Streptogramin. Type C CATs are also capable of chloramphenicol acetylation, but their roles in antibiotic resistance are understudied and largely unknown [57]. Many other chloramphenicol resistance mechanisms also exist, such as efflux pump systems, permeability barriers, target site mutations, and inactivation by phosphotransferases [6, 58].
In terms of the drug resistance rates, the linear trend line is indicative of a higher mean resistance rate of ophthalmic bacterial infections to chloramphenicol in developing countries; however, this is inconclusive due to the lack of adequate studies in these areas. This suggests a requirement for more research in the context of developing nations. Differences in the bacterial resistance to chloramphenicol in ophthalmic infections over the period of 2000–2022 could be attributed to variations in the resistance patterns of the causative bacterial strains, geographical differences (countries and region) of the studies, and factors, such as frequency of antimicrobial resistance monitoring and research output. Most of the bacterial pathogens implicated in ophthalmic infections showed a good level of susceptibility (over 60%) to chloramphenicol, except in the case of Pseudomonas spp. (P. aeruginosa and P. putida), which were intrinsically resistant to chloramphenicol and had low susceptibility rates in all the reviewed publications. Our work had some limitations, such as the fact that the reviewed publications were pooled from PubMed and Google Scholar only, leaving out other databases, such as Web of Science, Scopus, Embase, etc., which may also feature publications that might have provided additional insight concerning chloramphenicol resistance. In addition, as much as our review involved studies from various countries and continents globally, the drug resistance rates observed were only study-specific and were not definitive figures representing the actual summation of chloramphenicol resistance in each country.
Overall, the results from the reviewed literature depict that chloramphenicol is still quite active as a topical antibiotic against ophthalmic bacterial infections, as most of the bacterial strains had decent levels of susceptibility to chloramphenicol from their antimicrobial susceptibility profiles. This is similar to various publications that hold the same view [16, 34, 40, 56, 59]. As much as chloramphenicol susceptibility rates were high in the majority of the publications, concerns about increasing chloramphenicol resistance have been raised, such as the study by Lee et al., where increasing drug resistance against chloramphenicol was observed across primary, secondary and tertiary healthcare settings in London, United Kingdom [49]. Some publications hold a view contrary to ours, of chloramphenicol being unsuitable as an empirical eye drop treatment due to increasing rates of drug resistance from frequent prescription and overuse [29, 35, 52]. In light of the observed resistance rates, recommendations were made by Ogbolu et al. and Adebayo et al. for the replacement of topical antibiotics-like chloramphenicol with the third-generation fluoroquinolones (moxifloxacin, gatifloxacin and levofloxacin), due to their improved spectrum of activity and efficacy, as well as the slow rate of emergence of drug resistance due to the double-step mutation required for resistance to develop against these antibiotics [29, 60, 61]. In addition to the above calls for limiting the use of chloramphenicol, the results from a placebo-controlled clinical trial showed that most children with cases of acute infective conjunctivitis were capable of recovering by themselves without the use of chloramphenicol eye drops for therapy [62]. This depicts the need for a reduction in the unnecessary use of antibiotics-like chloramphenicol for relief in mild ophthalmic infections and common ocular irritations.
We recommend enhanced antimicrobial resistance surveillance for the early detection of chloramphenicol-resistant bacterial strains circulating locally in a region or health facility, with the goal of administering more effective second-line therapies once treatment failures are observed. It is also pertinent for antimicrobial guidelines to be regularly reviewed in accordance with local and international drug resistance patterns, for the approval and use of the most effective antibiotics as first-line therapy. In addition, empirical prescription of systemic and ophthalmic antibiotics must be discouraged, and an evidence-based approach of isolation and susceptibility testing of causative bacterial agents must be employed before proceeding to drug prescription. Regulatory policies by appropriate pharmaceutical and health-related bodies are required to control the availability and rate of consumption of over-the-counter medications, such as chloramphenicol eye drops, to lessen the risk of drug resistance.
Conclusion
Chloramphenicol still appears to be a suitable topical antibiotic for the treatment of ophthalmic bacterial infections; however, rising concerns remain about the drug becoming unsuitable in the long run due to growing rates of drug resistance. Efforts in research and antimicrobial resistance surveillance for chloramphenicol (and other ophthalmic antibiotics) should be intensified in developing countries, as higher rates of chloramphenicol resistance appear to occur in such regions. Overall, antimicrobial stewardship remains vital in combating the trend of drug resistance.
Availability of data and materials
Not applicable.
Abbreviations
- USA:
-
United States of America
- UK:
-
United Kingdom
- EMA:
-
European Medicines Agency
- MHRA:
-
Medicines and Healthcare Products Regulatory Agency
- ASTs:
-
Antimicrobial Susceptibility Tests
- CATs:
-
Chloramphenicol Acetyltransferases
References
Livingston RJ, Butterworth JW, Belt P. Reaction or infection: topic chloramphenicol treatment. Ann R Coll Surg Engl. 2013;95:e20–1.
Doshi B, Sarkar S. Topical administration of chloramphenicol can induce acute hepatitis. BMJ. 2009;338: b1699.
McDerby N, Watson SL, Robaei D, Naunton M. Inappropriate use of topical chloramphenicol results in vision loss. Clin Exp Ophthalmol. 2015;43(2):192–3.
Kmietowicz Z. Chloramphenicol eye drops: GPs criticise lack of guidance over use in under 2s. BMJ. 2021;373: n1252.
Sharma S. Antibiotic resistance in ocular bacterial pathogens. Indian J Med Microbiol. 2011;29(3):218–22.
Schwarz S, Kehrenberg C, Doublet B, Cloeckaert A. Molecular basis of bacterial resistance to chloramphenicol and florfenicol. FEMS Microbiol Rev. 2004;28:519–42.
Davis H, Mant D, Scott C, Lasserson D, Rose PW. Relative impact of clinical evidence and over-the-counter prescribing on topical antibiotic use for acute infective conjunctivitis. Br J Gen Pract. 2009;59(569):897–900.
Brown L. Resistance to ocular antibiotics: an overview. Clin Exp Optom. 2007;90(4):258–62.
Civljak R, Giannella M, Di Bella S, Petrosillo N. Could chloramphenicol be used against ESKAPE pathogens? A review of in vitro data in the literature from the 21st century. Expert Rev Anti Infect Ther. 2014;12(2):249–64.
Hovding G. Acute bacterial conjunctivitis. Acta Ophthalmol. 2008;86(1):5–17.
Cavuoto K, Zutshi D, Karp CL, Miller D, Feuer W. Update on bacterial conjunctivitis in South Florida. Ophthalmology. 2008;115(1):51–6.
Tuft SJ, Matheson M. In vitro antibiotic resistance in bacterial keratitis in London. Br J Ophthalmol. 2000;84(7):687–91.
Egger SF, Ruckhofer J, Alzner E, Hell M, Hitzl W, Huber-Spitzy V, Grabner G. In vitro susceptibilities to topical antibiotics of bacteria isolated from the surface of clinically symptomatic eyes. Ophthalmic Res. 2001;33:117–20.
Schaefer F, Bruttin O, Zografos L, Guex-Crosier Y. Bacterial keratitis: a prospective clinical and microbiological study. Br J Ophthalmol. 2001;85(7):842–7.
Morrissey I, Burnett R, Viljoen L, Robbins M. Surveillance of the susceptibility of ocular bacterial pathogens to the fluoroquinolones, vancomycin and gatifloxacin in Europe during 2001–2002. J Infect. 2002;49:109–14.
Fukuda M, Ohashi H, Matsumoto C, Mishima S, Shimomura Y. Methicillin-resistant Staphylococcus aureus and methicillin-resistant coagulase-negative Staphylococcus ocular surface infection: efficacy of chloramphenicol eye drops. Cornea. 2002;21(Suppl 1):S86–9.
Bharathi MJ, Ramakrishnan R, Vasu S, Meenakshi R, Palaniappan R. In-vitro efficacy of antibacterials against bacterial isolates from corneal ulcers. Indian J Ophthalmol. 2002;50(2):109–14.
Ta CN, Chang RT, Singh K, Egbert PR, Shriver EM, Blumenkranz MS, et al. Antibiotic resistance patterns of ocular bacterial flora: a prospective study of patients undergoing anterior segment surgery. Ophthalmology. 2003;110(10):1946–51.
Chalita MR, Belfort R. Shifting trends in in vitro antibiotic susceptibilities for common ocular isolates during a period of 15 years. Am J Ophthalmol. 2004;137(1):43–51.
Sharma V, Sharma S, Garg P, Rao GN. Clinical resistance of Staphylococcus keratitis to ciprofloxacin monotherapy. Indian J Ophthalmol. 2004;52(4):287–92.
Shanmuganathan VA, Armstrong M, Buller A, Tullo AB. External ocular infections due to methicillin-resistant Staphylococcus aureus (MRSA). Eye. 2005;19:284–91.
Arantes TEF, Cavalcanti RF, Diniz MFA, Severo MS, Neto JL, de Castro CMMB. Conjunctival bacterial flora ad antibiotic resistance pattern in patients undergoing cataract surgery. Arq Bras Oftalmol. 2006;69(1):33–6.
Aghadoost D, Khorshidi A. Antibiotic resistance patterns of ocular surface bacterial flora. Iran J Clin Infect Dis. 2007;2(3):133–7.
Fernandez-Rubio E, Urcelay J, Cuesta-Rodriguez T. The antibiotic resistance pattern of conjunctival bacteria: a key for designing a cataract surgery prophylaxis. Eye. 2009;23:1321–8.
Chung JL, Seo KY, Yong DE, Mah FS, Kim T, Kim EK, et al. Antibiotic susceptibility of conjunctival bacterial isolates from refractive surgery patients. Ophthalmology. 2009;116(6):1067–74.
Bertino JS. Impact of antibiotic resistance in the management of ocular infections: the role of current and future antibiotics. Clin Ophthalmol. 2009;3:507–21.
Ubani UA. Bacteriology of external ocular infections in Aba, South Eastern Nigeria. Clin Exp Optom. 2009;92(6):482–9.
Sueke H, Kaye S, Neal T, Murphy C, Hall A, Whittaker D, et al. Minimum inhibitory concentrations of standard and novel antimicrobials for isolates from bacterial keratitis. Invest Ophthalmol Vis Sci. 2010;51(5):2519–24.
Ogbolu DO, Alli OAT, Ephraim IE, Olabiyi FA, Daini OA. In-vitro efficacy of antimicrobial agents used in the treatment of bacterial eye infections in ibadan, Nigeria. Afr J Cln Exper Microbiol. 2011;12(3):124–7.
Haas W, Pillar CM, Torres M, Morris TW, Sahm DF. Monitoring antibiotic resistance in ocular microorganisms: results from the Antibiotic Resistance Monitoring in Ocular MicRorganisms (ARMOR) 2009 surveillance study. Am J Ophthalmol. 2011;152(4):567–74.
Shalchi Z, Gurbaxani A, Baker M, Nash J. Antibiotic resistance in microbial keratitis: ten-year experience of corneal scrapes in the united kingdom. Ophthalmology. 2011;118(11):2161–5.
Orlans HO, Hornby SJ, Bowler ICJW. In vitro antibiotic susceptibility patterns of bacterial keratitis isolates in Oxford, UK: a 10-year review. Eye. 2011;25:489–93.
Keshav BR, Basu S. Normal conjunctival flora and their antibiotic sensitivity in Omanis undergoing cataract surgery. Oman J Ophthalmol. 2012;5(1):16–8.
Mantadakis E, Maraki S, Michailidis L, Gitti Z, Pallikaris IG, Samonis G. Antimicrobial susceptibility of Gram-positive cocci isolated from patients with conjunctivitis and keratitis in Crete, Greece. J Microbiol Immunol Infect. 2013;46(1):41–7.
Blanco AR, Roccaro AS, Spoto CG, Papa V. Susceptibility of methicillin-resistant staphylococci clinical isolates to netilmicin and other antibiotics commonly used in ophthalmic therapy. Curr Eye Res. 2013;38(8):811–6.
Abera B, Kibret M. Azithromycin, fluoroquinolone and chloramphenicol resistance of non-chlamydia conjunctival bacteria in rural community of Ethiopia. Indian J Ophthalmol. 2014;62(2):236–9.
Karcic E, Aljicevic M, Bektas S, Karcic B. Antimicrobial susceptibility/resistance of Streptococcus pneumoniae. Mater Sociomed. 2015;27(3):180–4.
Sanfilippo CM, Morrissey I, Janes R, Morris TW. Surveillance of the activity of aminoglycosides and fluoroquinolones against ophthalmic pathogens from Europe in 2010–2011. Curr Eye Res. 2015;41(5):581–9.
Papa V, Blanco AR, Santocono M. Ocular flora and their antibiotic susceptibility in patients having cataract surgery in Italy. J Cataract Refract Surg. 2016;42(9):1312–7.
Wong ES, Chow CWY, Luk WK, Fung KSC, Li KKW. A 10-year review of ocular methicillin-resistant Staphylococcus aureus infections: epidemiology, clinical features, and treatment. Cornea. 2016;36(1):92–7.
Silvester A, Neal T, Czanner G, Briggs M, Harding S, Kaye S. Adult bacterial conjunctivitis: resistance patterns over 12 years in patients attending a large primary eye care centre in the UK. BMJ Open Ophth. 2016;1: e000006.
Wang N, Huang Q, Tan YW, Lin LP, Wu KL. Bacterial spectrum and resistance patterns in corneal infections at a Tertiary Eye Care Center in South China. Int J Ophthalmol. 2016;9(3):384–9.
Watson S, Cabrera-Aguas M, Khoo P, Pratama R, Gatus BJ, Gulholm T, et al. Keratitis antimicrobial resistance surveillance program, Sydney, Australia: 2016 Annual Report. Clin Experiment Ophthalmol. 2018;47(1):20–5.
Getahun E, Gelaw B, Assefa A, Assefa Y, Amsalu A. Bacterial pathogens associated with external ocular infections alongside eminent proportion of multidrug resistant isolates at the University of Gondar Hospital, northwest Ethiopia. BMC Ophthalmol. 2017;17(1):151.
Teweldemedhin M, Saravanan M, Gebreyesus A, Gebreegziabiher D. Ocular bacterial infections at Quiha Ophthalmic Hospital, Northern Ethiopia: an evaluation according to the risk factors and the antimicrobial susceptibility of bacterial isolates. BMC Infect Dis. 2017;17(1):207.
Deguchi H, Kitazawa K, Kayukawa K, Kondoh E, Fukumoto A, Yamasaki T, et al. The trend of resistance to antibiotics for ocular infection of Staphylococcus aureus, coagulase negative staphylococci, and Corynebacterium compared with 10-years previous: a retrospective observational study. PLoS ONE. 2018;13(9): e0203705.
Belyhun Y, Moges F, Endris M, Asmare B, Amare B, Bekele D, et al. Ocular bacterial infections and antibiotic resistance patterns in patients attending Gondar Teaching Hospital, Northwest Ethiopia. BMC Res Notes. 2018;11(597):1–7.
Croghan C, Lockington D. Management of MRSA-positive eye swabs and the potential advantages of chloramphenicol availability in the United Kingdom. Eye. 2018;32:157–9.
Alter SJ, Sanfilippo CM, Asbell PA, DeCory HH. Antibiotic resistance among pediatric-sourced ocular pathogens: 8-year findings from the antibiotic resistance monitoring in ocular microorganisms (ARMOR) surveillance study. Pediatr Infect Dis J. 2019;38(2):138–45.
Lee AE, Niruttan K, Rawson TM, Moore LSP. Antibacterial resistance in ophthalmic infections: a multi-centre analysis across UK care settings. BMC Infect Dis. 2019;19:768.
Thomas RK, Melton R, Asbell PA. Antibiotic resistance among ocular pathogens: current trends from the ARMOR surveillance study (2009–2016). Clin Optom. 2019;11:15–26.
Nithya V, Rathinam S, Karthikeyan RSG, Lalitha P. A ten-year study of prevalence, antimicrobial susceptibility pattern, and genotypic characterization of Methicillin resistant Staphylococcus aureus causing ocular infections in a tertiary eye care hospital in South India. Infect Genet Evol. 2019;69:203–10.
Hatami-Mazinani N, Nejabat M, Bazargani A, Khoshroo J, Vazin A. A study on the most prevalent bacterial cause of corneal ulcer and their susceptibility to five common types of ophthalmic antibiotics. Trends Pharm Sci. 2020;6(2):121–30.
Harford DA, Greenan E, Knowles SJ, Fitzgerald S, Murphy CC. The burden of methicillin-resistant Staphylococcus aureus in the delivery of eye care. Eye. 2021;25:1–5.
Woreta AN, Kebede HB, Tilahun Y, Teklegiorgis SG, Abegaz WE. Antibiotic susceptibility pattern and bacterial spectrum among patients with external eye infections at Menelik II referral hospital in Addis Ababa, Ethiopia. Infect Drug Resist. 2022;15:765–79.
Wareham DW, Wilson P. Chloramphenicol in the 21st century. Hosp Med. 2002;63(3):157–61.
Alcala A, Ramirez G, Solis A, Kim Y, Tan K, Luna O, et al. Structural and functional characterization of three Type B and C chloramphenicol acetyltransferases from Vibrio species. Protein Sci. 2020;29(3):695–710.
Rajesh T, Sung C, Kim H, Song E, Park HY, Jeon JM, et al. Phosphorylation of chloramphenicol by a recombinant protein Yhr2 from Streptomyces avermitilis MA4680. Bioorganic Med Chem Lett. 2013;23(12):3614–9.
Andaluz-Scher L, Medow NB. Chloramphenicol eye drops: an old dog in a new house. Ophthalmology. 2020;127(10):P1289–91.
Adebayo A, Parikh JG, McCormick SA, Shah MK, Huerto RS, Yu G, et al. Shifting trends in in vitro antibiotic susceptibilities for common bacterial conjunctival isolates in the last decade at the New York eye and ear Infirmary. Graefes Arch Clin Exp Ophthalmol. 2011;249(1):111–9.
Benitez-Del-Castillo J, Verboven Y, Stroman D, Kodjikian L. The role of topical moxifloxacin, a new antibacterial in Europe, in the treatment of bacterial conjunctivitis. Clin Drug Investig. 2011;31:543–57.
Rose PW, Harnden A, Brueggemann AB, Perera R, Sheikh A, Crook D, et al. Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial. Lancet. 2005;366(9479):37–43.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
BIB, EEE and PM were responsible for the manuscript conception, design, literature search and analysis. FOA, IOO, DELP and AUS contributed extensively to the drafting and revision of the work. All authors approved the final version of the manuscript and take responsibility for it. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bale, B.I., Elebesunu, E.E., Manikavasagar, P. et al. Antibiotic resistance in ocular bacterial infections: an integrative review of ophthalmic chloramphenicol. Trop Med Health 51, 15 (2023). https://doi.org/10.1186/s41182-023-00496-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41182-023-00496-x