
Abstract
Background
Empirical antibiotic treatment against peritoneal dialysis (PD)-related peritonitis should be immediately initiated before PD effluent culture results are obtained. As culture results guide the choice of antibiotics, culture-negative peritonitis (CNP) is a serious issue. In addition, the identification of the causative organism often indicates a possible source of infection. This study aimed to clarify the predictors of CNP.
Methods
This single-center, retrospective study was conducted from November 2007–December 2018 in patients undergoing PD with peritonitis at our institution, where 204 peritonitis episodes (57 culture-negative, 147 culture-positive) were investigated based on demographics, and clinical parameters. CNP predictors were investigated using logistic regression.
Results
CNP rate was significantly higher in female and in patients with higher platelet counts, lower dialysate cell counts at peritonitis diagnosis, and higher serum β2-microglobulin levels. In multivariate logistic regression, female sex (odds ratio [OR] 2.69, 95% confidence interval [CI] 1.31–5.54), dialysate cell count at diagnosis (OR0.99, 95% CI 0.99–0.99), and serum β2-microglobulin level (OR 1.04, 95% CI 1.00–1.07) were significantly associated with CNP. The areas under the receiver operating characteristic curve for female patients, dialysate cell counts at diagnosis of peritonitis, serum β2-microglobulin level, and female patients + dialysate cell counts at diagnosis of peritonitis + serum β2-microglobulin level were 0.604, 0.694, 0.603, and 0.751, respectively.
Conclusions
Female sex, dialysate cell counts at peritonitis diagnosis, and serum β2-microglobulin levels may be predictors of CNP.
Similar content being viewed by others


Background
Peritonitis is a major cause of morbidity and mortality in patients undergoing peritoneal dialysis (PD) [1]. Empirical antibiotic treatment against both gram-positive and gram-negative microorganisms should be immediately initiated before PD effluent culture results are obtained. As culture results guide the choice of antibiotics, culture-negative peritonitis (CNP) is a serious issue. In addition, the identification of the causative organism often indicates a possible source of infection. The International Society for Peritoneal Dialysis (ISPD) guidelines recommend that the CNP rate should not exceed 15% [2]. However, few studies have reported the predictors of CNP [3,4,5,6,7]. The objective of this study was to identify the predictors of CNP.
Methods
Study population
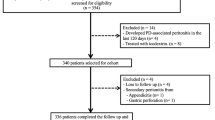
Based on medical records, there were 243 episodes of PD-associated peritonitis between November 2007 and December 2018 at our institution, of which we excluded 39 episodes: 27 episodes had PD-related peritonitis within 3 months after PD initiation; five episodes, malignancy; four episodes, peritonitis with other infections; one episode, liver cirrhosis; one episode, interferon therapy; and, one episode, immunosuppression therapy. Finally, 204 episodes were registered in our database and have been previously reported [8]. In this study, we used this database to investigate predictors of culture-negative PD-associated peritonitis. CNP was defined by clinical features including peritonitis, dialysate leukocytosis (white blood cell count > 100/µL with neutrophils > 50%), and negative dialysate culture [2]. This study was approved by the Ethical Committee of our institution (approval no. 1129) and was conducted in accordance with the principles of the Declaration of Helsinki and Japanese ethical guidelines.
Data collection
Data including age, sex, body mass index, number of peritonitis episodes per patient-year, recent antibiotic use within 30 days, microorganisms in dialysate cultures, presence of diabetes mellitus and cardiovascular disease, body temperature, blood pressure, and laboratory data at the time of visit diagnosed with peritonitis were collected by reviewing the patients’ medical records. Laboratory data included white blood cell count; hemoglobin, platelet, total protein, serum albumin, serum aspartate aminotransferase, alkaline phosphatase, lactate dehydrogenase, uric acid, sodium, potassium, corrected calcium, phosphate, and C-reactive protein levels; dialysate cell counts; dialysate and plasma creatinine ratio; Kt/V urea per week; and β2-microglobulin level. The second dialysate cell count was evaluated 3–5 d after initiating antibiotics.
PD effluent culture
We inoculated 5 to 10 mL of PD effluent in two (aerobic and anaerobic) blood culture bottles, as recommended by the ISPD guidelines [2]. Then, we transfer the inoculated bottles to the microbiology laboratories outside the hospital.
Statistical analysis
Data are expressed as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables were evaluated using the chi-squared test or Fisher exact test. Continuous variables were compared using Student’s t test or Mann–Whitney U test, as appropriate. A multivariate logistic regression analysis was performed to determine the independent variables associated with CNP. Odds ratios (ORs) were calculated with their respective 95% confidence intervals (CIs). Receiver operating characteristic (ROC) curves were used to evaluate the strength of the predictive factors. All analyses were performed using JMP, version 16 (SAS Institute Inc., Cary, NC, USA). P < 0.05 was considered to be statistically significant.
Results
Patients' clinical and laboratory characteristics
There were 57 culture-negative among a total of 204 peritonitis episodes. The baseline clinical and laboratory characteristics of the patients undergoing PD having culture-negative and culture-positive peritonitis are listed in Tables 1 and 2. Compared with culture-positive peritonitis, CNP episodes were significantly more frequent among female patients (43.9 vs. 23.1%; p = 0.0055) and patients with higher platelet counts (23.7 × 104/µL [19.6 × 104/µL–30.2 × 104/µL] vs. 20.3 × 104/µL [16.3 × 104/µL–26.4 × 104/µL]; p = 0.0102), lower dialysate cell counts at peritonitis diagnosis (724/µL [354/µL–1601/µL] vs. 1959/µL [709/µL–5230/µL]; p < 0.0001), and higher serum β2-microglobulin levels (29.8 µg/L [24.1–34.9 µg/L] vs. 26.5 µg/L [19.9–33.2 µg/L]; p = 0.0235). No significant differences were found among the other characteristics.
Initial antibiotic regimens
The initial antibiotic regimens for CNP and culture-positive peritonitis are shown in Fig. 1. All CNP episodes were treated with at least two antibiotics. 47 peritonitis episodes were treated with either cefazolin or vancomycin in combination with aminoglycosides.

Initial antibiotic regimens of a CNP, and b culture-positive peritonitis. CEZ, cefazoline; ISP, isepamicin sulfate; VCM, vancomycin; MEPM, meropenem; CAZ, ceftazidime; RFP, rifampicin; DAP, daptomycin; FCZ, fluconazole; LVFX, levofloxacin; FOM, fosfomycin; MINO, minocycline; PZFX, pazufloxacin; ST, sulfamethoxazole trimethoprim; LZD, linezolid
Outcomes of culture-negative peritonitis
The PD withdrawal and mortality rates were similar between culture-negative and culture-positive peritonitis (15.8 vs. 19.7%; p = 0.69, 3.5 vs. 1.4%; p = 0.31, respectively) episodes. All deaths were attributed to peritonitis (Table 3).
Predictors of culture-negative peritonitis
We performed a multivariate logistic regression analysis to investigate the predictors of CNP. Female sex (OR 2.69, 95% CI 1.31–5.54), dialysate cell counts at peritonitis diagnosis (OR 0.99, 95% CI 0.99–0.99), and serum β2-microglobulin level (OR 1.04, 95% CI 1.00–1.07) were significantly associated with CNP (Table 4). Furthermore, we evaluated the strength of the predictors of CNP by using ROC curve analysis. The areas under the ROC curve for female patients, dialysate cell counts at diagnosis of peritonitis, serum β2-microglobulin level, and female patients + dialysate cell counts at diagnosis of peritonitis + serum β2-microglobulin level were 0.604, 0.694, 0.603, and 0.751, respectively (Fig. 2).

The area under the ROC curve for female patients, cell counts of dialysate at diagnosis of peritonitis, serum β2-microglobulin, and female patients + cell counts of dialysate at diagnosis of peritonitis + serum β2-microglobulin
Sub-analysis
We should consider the retrograde menstruation and other gynecologic causes such as ovulation, especially in female patients, which might be related to a lower diagnostic and culture-negative rate [9, 10]. Therefore, we select postmenopausal female cases for sub-analysis. The results were shown in Additional file 1. CNP rate was also significantly higher in female and in patients with higher platelet counts, lower dialysate cell counts at peritonitis diagnosis, and higher serum β2-microglobulin levels (Additional file 1: Table S1 and S2). In multivariate logistic regression, female sex and dialysate cell count at diagnosis were significantly associated with CNP (Additional file 1: Table S3).
Discussion
To the best of our knowledge, this is the first report revealing a significant relationship between culture-negative PD-related peritonitis, sex, dialysate cell counts at peritonitis diagnosis, and serum β2-microglobulin level. Female patients with diabetes had a higher CNP rate as well as higher rates of gram-positive and streptococcal peritonitis [11]. In this study, we revealed the effect of sex alone on CNP. The culture-negative rate in female patients without diabetes was similar to that in female patients with diabetes (data not shown). The discrepancy among studies may be related to the smaller sample size and adjustments for comorbidities in our study. The noninfectious causes of CNP were reported due to visceral inflammation, drug reactions, malignancy, and retroperitoneal inflammation [9]. Considering the possible gynecologic causes of CNP [9, 10], we selected postmenopausal female cases and assessed for sub-analysis. The sub-analysis similarly revealed that female sex may be an independent predictor of CNP.
Although the mechanism remains unclear, we revealed that the dialysate cell count at peritonitis diagnosis and the serum β2-microglobulin level were independently associated with CNP. Automated PD (APD) utilization and extra peritoneal retention for culture sampling often shorten the peritoneal retention time, which may affect lower cell counts and higher CNP rate. However, in this study, APD was not associated with higher rates of CNP. Cytokine release was reported to be significantly lower in CNP than that in culture-positive peritonitis [12]. Therefore, there may be microbiological and immunological differences between culture-negative and culture-positive peritonitis. Serum β2-microglobulin level has been used as a predictor of residual renal function and all-cause mortality in patients undergoing hemodialysis [13, 14]. It is also a marker for cellular immune system activation [15]. In patients with PD, a lower serum β2-microglobulin level, which represents impaired immunity, was independently associated with overall and infection-related mortality [16]. Although the mechanisms responsible for the observations in our study remain unclear, microbiological and immunological alterations in CNP might affect serum β2-microglobulin levels. Further studies are needed to confirm the relationship between the serum β2-microglobulin level and CNP.
The major limitation of this study is that CNP accounted for 27.9% of all cases during the study period, which was higher than the proportion reported in previous studies [3, 6, 17, 18]. Most cases of CNP can be explained by recent antibiotic treatment or technical problems during PD effluent culture [4]. Cefazolin sodium and isepamicin sulfate were used in our institution for the empirical treatment of peritonitis, as in the case of CNP. The response to antibiotics and outcomes did not significantly differ between culture-negative and culture-positive peritonitis episodes, supporting bacterial infection as the cause of CNP in this study. A history of antibiotic use within 30 days before peritonitis occurrence was reported as a reason for CNP [3], although this was not the case in our study. We inoculated 5–10 mL of effluent in two (aerobic and anaerobic) blood culture bottles, as recommended by the ISPD guidelines [2]. However, this technique for culture has reasonable sensitivity, and the culture-negative rate is typically about 10–20% [19, 20], which is lower than that of our institution. The facility-specific reason for the high culture-negative rate may be the delay due to the time taken to transfer the inoculated bottles to the microbiology laboratories because the tests were ordered outside the hospital. The ISPD guidelines recommend the immediate transfer of inoculated bottles to laboratories within 6 h, as this was associated with lower CNP rates [2, 7]. However, at our institution, the inoculated bottles were stored at room temperature for more than 6 h, which may have led to a high culture-negative rate.
Conclusions
Our study revealed that female sex, dialysate cell counts at diagnosis of peritonitis, and serum β2-microglobulin levels were independent predictors of culture-negative PD-related peritonitis.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- PD:
-
Peritoneal dialysis
- CNP:
-
Culture-negative peritonitis
- ISPD:
-
International Society for Peritoneal Dialysis
- ORs:
-
Odds ratios
- CI:
-
CIs confidence intervals
- ROC:
-
Receiver operating characteristic
References
Higuchi C, Ito M, Masakane I, Sakura H. Peritonitis in peritoneal dialysis patients in Japan: a 2013 retrospective questionnaire survey of Japanese Society for Peritoneal Dialysis member institutions. Renal Replacement Therapy. 2016;2(1).
Li PK, Chow KM, Cho Y, Fan S, Figueiredo AE, Harris T, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit Dial Int. 2022;42(2):110–53.
Szeto CC, Wong TY, Chow KM, Leung CB, Li PK. The clinical course of culture-negative peritonitis complicating peritoneal dialysis. Am J Kidney Dis. 2003;42(3):567–74.
Chen KH, Chang CT, Weng SM, Yu CC, Fang JT, Huang JY, et al. Culture-negative peritonitis: a fifteen-year review. Ren Fail. 2007;29(2):177–81.
Fahim M, Hawley CM, McDonald SP, Brown FG, Rosman JB, Wiggins KJ, et al. Culture-negative peritonitis in peritoneal dialysis patients in Australia: predictors, treatment, and outcomes in 435 cases. Am J Kidney Dis. 2010;55(4):690–7.
Htay H, Cho Y, Pascoe EM, Hawley C, Clayton PA, Borlace M, et al. Multicentre registry data analysis comparing outcomes of culture-negative peritonitis and different subtypes of culture-positive peritonitis in peritoneal dialysis patients. Perit Dial Int. 2020;40(1):47–56.
Kanjanabuch T, Chatsuwan T, Udomsantisuk N, Nopsopon T, Puapatanakul P, Halue G, et al. Association of local unit sampling and microbiology laboratory culture practices with the ability to identify causative pathogens in peritoneal dialysis-associated peritonitis in Thailand. Kidney Int Rep. 2021;6(4):1118–29.
Banno T, Shima H, Kawahara K, Okada K, Minakuchi J. Risk factors for peritoneal dialysis withdrawal due to peritoneal dialysis-related peritonitis. Nephrol Ther. 2021;17(2):108–13.
Rocklin MA, Teitelbaum I. Noninfectious causes of cloudy peritoneal dialysate. Semin Dial. 2001;14:37–40.
Yaseen O, El Nekidy WS, Ibrahim AR, Jasey BB, Guignard M, Kadri A. Cyclic pseudoperitonitis secondary to endometriosis in a peritoneal dialysis patient. Perit Dial Int. 2012;32:662–4.
Nessim SJ, Bargman JM, Austin PC, Nisenbaum R, Jassal SV. Predictors of peritonitis in patients on peritoneal dialysis: results of a large, prospective Canadian database. Clin J Am Soc Nephrol. 2009;4(7):1195–200.
Lin C-Y, Roberts GW, Kift-Morgan A, Donovan KL, Topley N, Eberl M. Pathogen-specific local immune fingerprints diagnose bacterial infection in peritoneal dialysis patients. J Am Soc Nephrol. 2013;24(12):2002–9.
Jaques DA, Davenport A. Serum beta2-microglobulin as a predictor of residual kidney function in peritoneal dialysis patients. J Nephrol. 2021;34(2):473–81.
Maruyama Y, Nakayama M, Abe M, Yokoo T, Minakuchi J, Nitta K. Association between serum beta2-microglobulin and mortality in Japanese peritoneal dialysis patients: a cohort study. PLoS ONE. 2022;17(4):e0266882.
Vincent C, Revillard JP. Beta-2-microglobulin and HLA-related glycoproteins in human urine and serum. Contrib Nephrol. 1981;26:66–88.
Chang TI, Lim H, Park CH, Park KS, Park JT, Kang EW, et al. Lower serum beta-2 microglobulin levels are associated with worse survival in incident peritoneal dialysis patients. Nephrol Dial Transplant. 2019;34(1):138–45.
Nishina M, Yanagi H, Kakuta T, Endoh M, Fukagawa M, Takagi A. A 10-year retrospective cohort study on the risk factors for peritoneal dialysis-related peritonitis: a single-center study at Tokai University Hospital. Clin Exp Nephrol. 2014;18(4):649–54.
Vychytil A, Remon C, Michel C, Williams P, Rodriguez-Carmona A, Marron B, et al. Icodextrin does not impact infectious and culture-negative peritonitis rates in peritoneal dialysis patients: a 2-year multicentre, comparative, prospective cohort study. Nephrol Dial Transplant. 2008;23(11):3711–9.
Alfa MJ, Degagne P, Olson N, Harding GK. Improved detection of bacterial growth in continuous ambulatory peritoneal dialysis effluent by use of BacT/Alert FAN bottles. J Clin Microbiol. 1997;35(4):862–6.
Azap OK, Timurkaynak F, Sezer S, Cağir U, Yapar G, Arslan H, et al. Value of automatized blood culture systems in the diagnosis of continuous ambulatory peritoneal dialysis peritonitis. Transplant Proc. 2006;38(2):411–2.
Acknowledgements
We thank Taro Banno (Department of Urology, Tokyo Women's Medical University, Tokyo, Japan) for valuable discussion. We thank Editage for their technical assistance in editing a draft of this manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
HS drafted the first manuscript. HS, TO, MT, TI, SW, HB, HA, NI, TO, TD, KO, and JM performed the literature search. TO, MT, TI, MI, SW, TD, KO, and JM coordinated the data analysis and critically commented on the manuscript. HB, HA, NI, TO, TD, KO, and JM helped with writing the manuscript. All authors participated in discussions, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Committee of Kawashima Hospital (approval no. 1129) and was conducted in accordance with the principles of the Declaration of Helsinki and Japanese ethical guidelines. All patients gave informed consent for their data to be included in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1
Clinical characteristics in PD patients with culture-negative or culture-positive peritonitis (male and postmenopausal female). Table S2 Laboratory characteristics in PD patients with culture-negative or culture-positive peritonitis (male and postmenopausal female). Table S3 Multivariate logistic regression analyses of predictors for culture-negative peritonitis (male and postmenopausal female).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shima, H., Okamoto, T., Tashiro, M. et al. Predictors of culture-negative peritoneal dialysis-associated peritonitis: a single center, retrospective study. Ren Replace Ther 9, 55 (2023). https://doi.org/10.1186/s41100-023-00498-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-023-00498-9