
Abstract
Background
This study aimed to determine the prevalence and antibiotic resistance patterns in Staphylococcus aureus isolated from patients with cystic fibrosis in Middle Eastern countries.
Methods
A systematic search was conducted in the PubMed, Web of Science (ISI), and Scopus databases for studies presenting the prevalence of MRSA strains, antibiotic resistance pattern in S. aureus strains isolated from patients who suffered from cystic fibrosis in Middle Eastern countries from 1999 to 10 June 2020. The following terms were used; prevalence, antibiotic resistance, antimicrobial drug resistance, drug resistance, Staphylococcus aureus, S. aureus, Methicillin-resistant Staphylococcus aureus, MRSA, cystic fibrosis, CF, and the Middle East. The meta-analysis was performed using Comprehensive Meta-analysis software (Version 3.3.070).
Results
Patients’ age ranged from 1.6 to 18 years. Females were more than males. The prevalence of S. aureus was varied between 5.6 and 77.8%. The prevalence of S. aureus was varied between 5.6 and 77.8% in different countries. The combined prevalence of S. aureus in Middle East countries from 1999 to 2020 was reported by 40.9% (95% CI 29.6–53.1). The pooled prevalence of MRSA was reported at 18.6% (95% CI 1.1–82.6), Z = 0.9, I2 = 98.6, Q = 146.7. The highest combined resistance in S. aureus strains was reported to Penicillin G (94%), followed by Ciprofloxacin (54.9%).
Conclusion
Regarding a quite prevalence of S. aureus and an intermediate prevalence of MRSA in CF patients, preventive measures and health policies should be implemented in the Middle East area to prevent the spread of infections caused by MRSA strains in CF patients.
Similar content being viewed by others

Background
Cystic fibrosis (CF) is an inherited multisystem dysfunction determined by abnormalities in exocrine gland function. A mutation in the cystic fibrosis conductance regulator (CFTR) gene sited on chromosome 7 in humans is the cause of cystic fibrosis (CF) [1]. Chronic sinopulmonary disease, pancreatic exocrine impairment, elevated sweat chloride, and male infertility are common disorders that resulted from CF [2]. Cystic fibrosis is the most frequent, lethal, genetic mutation which affects more than 70,000 people globally [3, 4]. In recent decades, advancements in disease management and new therapeutic developments have led to improved patients’ survival, with surviving into the late thirties, as around 50% of all persons with CF are now 18 years of age or older [2].
Significant advances have been made in the lives of people with CF over the past six decades, which was once a life-threatening disease of infants and young children. However, life expectancy for people with CF has gradually increased, However, the disease still affects the survival and quality of people’s lives and imposes a heavy health burden on patients and their families [5]. According to reports, most patients with CF acquire pathogens from the environment, especially medical settings when they stay in these centers for a long time [1].
Staphylococcus aureus and Pseudomonas aeruginosa, Achromobacter xylosoxidans, Burkholderia cepacia complex, and Stenotrophomonas maltophilia are the most common isolates retrieved from CF patients [6]. S. aureus is one of the first respiratory colonizers in people with CF [7]. This microorganism causes opportunistic infections in people with underlying diseases such as CF [8, 9]. MRSA; a type of bacteria that causes an infection that does not respond to common antibiotics, including methicillin, amoxicillin, and penicillin as opposed to methicillin-susceptible Staphylococcus aureus (MSSA) [10]. The findings suggest that not only it is difficult to treat infections caused by MRSA strains, but it is also now known that MRSA infection may exacerbate lung function [11, 12].
The Middle East region is a vast area with several countries of different ethnicities, races, cultures, and climatic diversity [13]. The local prevalence in countries in the Middle East area is changing, due to the outline of new strains with the intercontinental exchange of several clones [14]. Several studies from this region reported a prevalence rate between 10 and 35% [15,16,17]. MRSA is endemic in this district, and this causes an increase in the risk of domestic and global transmission [14].
Therefore, due to the widespread prevalence of S. aureus in cystic fibrosis patients, the determination of the prevalence of this bacterium and its antibiotic resistance pattern is of special importance. So, this study aimed to determine the prevalence of MRSA strains, antibiotic resistance patterns in S. aureus strains isolated from patients with cystic fibrosis in Middle Eastern countries.
Material and methods
Literature search
A systematic search was conducted in PubMed, Web of Science (ISI), and Scopus databases for studies presenting the prevalence of MRSA strains, antibiotic resistance pattern in S. aureus strains isolated from patients with CF in some Middle Eastern countries from 1999 to 10 June 2020. The following search terms were used: prevalence, antibiotic resistance, antimicrobial drug resistance, drug resistance, Staphylococcus aureus, S. aureus, Methicillin-resistant Staphylococcus aureus, MRSA, cystic fibrosis, CF, and the Middle East, Iran, Palestine, Kuwait, Qatar, Emirate United Arab, Saudi Arabia, Lebanon, Turkey, Yemen, Oman, Bahrain, Egypt, Iraq, Jordan, Syria, and Cyprus.
Search strategy in PubMed was as follows; (prevalence [MeSH Terms]) AND (Drug Resistance [MeSH Terms] OR Antimicrobial Drug Resistance [MeSH Terms] OR Antibiotic Resistance [MeSH Terms]) AND (Staphylococcus aureus [MeSH Terms] OR S. aureus [MeSH Terms]), AND (Methicillin-resistant Staphylococcus aureus [MeSH Terms] OR MRSA [MeSH Terms]), AND (cystic fibrosis [MeSH Terms] OR CF [Title/Abstract]), AND (Middle East [MeSH Terms]). The bibliographic section of pertinent studies was also hand-searched to recognize further potentially eligible articles. Articles published in languages other than English were not evaluated.
Inclusion and exclusion criteria
Study inclusion criteria were cross-sectional and cohort studies that presented the prevalence of S. aures, antibiotic resistance pattern, MRSA prevalence in CF patients from the Middle East were included. Also, articles that use standardized tests to determine antibiotic susceptibility were included. Studies before 1999, studies other than Middle East countries, studies with missed data, unclear data, abstracts, conferences, case reports, editorials, meetings, and reviews were excluded. As well, studies were written in languages other than English and also published before 1999 were deleted.
Quality assessment
Selection bias was assessed with the Critical Appraisal Skills Programme (CASP) checklist for cross-sectional studies (www.casp-uk.net). For each study, 10 questions were asked. So, the questions that were answered "yes" were given a score of 1, and if there was “no answer or doubts," the score was 0. According to this scoring system, studies were divided into three categories: poor (1–4), intermediate (6–8), and strong (> 8). In the end, poor studies were eliminated (Additional file 1).
Data extraction
Two investigators independently reviewed the selected articles and extracted the pertinent data regarding the characteristics of each study. Data were first author, location (country), study’s time, publication time, sample size, age, genus (male, female), and cystic fibrosis prevalence (n).
Statistical data analysis
Meta-analysis was performed using Comprehensive meta-analysis software (Version 3.3.070). The prevalence was calculated by 95% confidence intervals (CIs). Statistical heterogeneity between studies was assessed using Cochran's Q-test (p < 0.05 was defined to indicate the presence of heterogeneity) and the I2 (for assessing the degree of heterogeneity). The random-effect model was used because there was significant statistical heterogeneity between the studies. Also, publication bias was checked by Egger's regression asymmetry test and Funnel plot. As well, subgroup analysis was done for MRSA strains and antibiotic resistance patterns.
Results
Study selection and characteristics of included studies
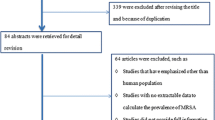
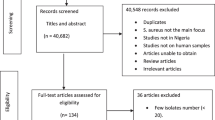
A total of 1003 studies were recognized in the primary search. After assessing titles, abstracts and full-texts, 12 studies met eligibility criteria for inclusion (Fig. 1). The frequency of studies from different countries was as follows; Turkey (n = 3), Iran (n = 3), Qatar (n = 4), Egypt (n = 1), and the United Arab Emirates (n = 1). Patients’ age ranged from 1.6 to 18 years. Females were more than males. The most samples used were sputum, deep pharyngeal swabs, and Bronchoalveolar lavage (BAL) (Table 1).

Flowchart of inclusion process for studies
Overall effects
As it is observed in Table 1 and Fig. 2, the prevalence of S. aureus was varied between 5.6 and 77.8% in different countries included in this review. In general, the combined prevalence of S. aureus in some Middle East countries from 1999 to 2020 was reported by 40.9% (95% CI 29.6–53.1). Findings from selected studies showed that apart from Egypt, there is no significant difference in the prevalence of S. aureus in Middle Eastern countries and they are almost in the same range (Fig. 2). Also, comparing the prevalence of S. aureus based on the year of study showed that the prevalence of this microorganism hasn’t changed much since the beginning (1999) until now (2020), and its isolation from cystic fibrosis patients has been constant (Table 1).

Forest plot of the meta-analysis of prevalence of S. aureus isolated from patients suffered from cystic fibrosis
Heterogeneity and publication bias
Regarding data achieved in the present study, heterogeneity was seen (Q = 185.9 and Z = 1.4, and I2 = 94). Visual survey of Funnel plot showed the bias in the studies. Egger's linear regression test was performed to further investigate this subject. According to the findings, there was no publication bias among studies due to p = 0.31 (Fig. 3).

Funnel plot of the meta-analysis of prevalence of S. aureus isolated from patients suffered from cystic fibrosis
Subgroup analysis
Prevalence of MRSA
As summarized in Table 2, the pooled prevalence of MRSA strains was reported at 18.6% (95% CI 1.1–82.6), Z = 0.9, I2 = 98.6, Q = 146.7.
Antibiotic resistance pattern
The pooled prevalence of resistance for each antibiotic was calculated. All isolates were resistant against Cefoxitin and Oxacillin, that’s why they all were MRSA. The highest combined resistance of S. aureus strains was reported against Penicillin G, followed by Ciprofloxacin with resistance rates 94% (95% CI 70.1–99.1), and 54.9% (95% CI 2.5–98.3), respectively. All strains displayed susceptibility to Tigecycline, Clarithromycin, Telithromycin, Teicoplanin, Linezolid, and Vancomycin.
Discussion
Bacteria as the most important pathogens still play a significant role in aggravating lung complications in patients with cystic fibrosis [18]. Many organisms isolated from the sputum of CF patients are normal flora of the nose (S. aureus) or opportunistic pathogens such as P. aeruginosa which is a common environmental organism [19]. Due to the importance of S. aureus especially MRSA isolates in CF patients, in the current review, the prevalence of this microorganism and its antibiotic resistance pattern was investigated. In our study, the prevalence of S. aureus in different countries varied between 5.6 and 77.8%. In general, the combined prevalence of S. aureus in some Middle East countries from 1999 to 2020 was reported by 40.9%. Also, the pooled prevalence of MRSA strains was reported at 18.6%. So, based on data obtained from the current meta-analysis, S. aureus was isolated at a high rate from CF patients. Finding S. aureus in the lower respiratory tract certainly indicates a pathological situation that has never been adequately investigated [20, 21]. Our results are in accordance with reports from the USA, where the US Patient Registry Annual Data Report presented the prevalence of S. aureus 70.3% in CF patients [22]. Also, accordingly, the report of the prevalence among European countries was varied between 60 and 75% [23,24,25].
According to the results of included studies, there is no significant difference in the prevalence of S. aureus in Middle Eastern countries except Egypt and they all are almost in the same range. Also, comparing the prevalence of S. aureus based on the year of study showed that the prevalence of this microorganism has not changed much since the beginning (1999) until now (2020), and its isolation from cystic fibrosis patients has been constant. The stability of prevalence of S. aureus is possibly owing to improved awareness and infection prevention and control strategies [22]. If we look at it from another angle, the lack of new molecular techniques and the constant use of phenotypic methods or the lack of proper health policies in this area may have caused the prevalence of these microorganisms in these patients over the years to be almost constant which this requires a change in health policy attitudes. We reported the prevalence rate about of 18.6% of MRSA, similarly, USA Patient Registry Annual Data Report showed a prevalence rate of around 25% for MRSA [22], and Argentina (25.9%) [26]. But in contrast to our study, this rate was lower in Poland (6%) [27] and Germany (4%) [28]. We surely know MRSA strains will bring up more problems for patients with CF [2].
In the present systematic review and meta-analysis, the highest combined resistance in S. aureus strains was reported against Penicillin G, followed by Ciprofloxacin with resistance rates of 94%, and 54.9%, respectively. Therefore, according to results achieved, most antibiotics used in included studies except Penicillin G and Ciprofloxacin were effective against S. aureus isolates. This must be taken into consideration in line with our results, a study conducted by Cafiso et al. All strains were susceptible to Linezolid and Tigecycline [8]. Regarding the identification of the clinical significance of S. aureus pulmonary infection particularly MRSA in CF and the restricted data available to guide present therapeutic regimes [2, 29], in the current review, most antibiotics especially Tigecycline, Clarithromycin, Telithromycin, Teicoplanin, Linezolid, and Vancomycin showed a good impact on S. aureues isolates. Therefore, it can use the mentioned antibiotics in MRSA pulmonary infection in CF patients in the Middle East area.
The main limitation of the present study is that we search only studies published in English and other languages such as Persian, Turkish, and Arabic that didn’t include. Also, the sample size used here was small and the number of studies enrolled unfortunately did not cover all Middle Eastern countries.
In summary, our review reported a high prevalence of S. aureus and an intermediate prevalence of MRSA strains in pulmonary specimens achieved from CF patients. The prevalence in most of the countries included in this study was almost the same and showed a steady trend within a few years from 1999 to 2020. Due to these facts, it is necessary to use new molecular methods to identify this microorganism.
Conclusion
Preventive measures and health policies should be implemented in the Middle East region to prevent the spread of infection caused by this microorganism, specifically MRSA in CF patients.
Availability of data and materials
All data used and analyzed during this study are based on an original article and is available from the corresponding author, by request.
Abbreviations
- ISI:
-
Web of Science
- CF:
-
Cystic fibrosis
- CFTR:
-
Cystic fibrosis conductance regulator
- MSSA:
-
Methicillin-susceptible staph
- CASP:
-
Critical Appraisal Skills Programme
- CIs:
-
Confidence intervals
References
Sousa AM, Pereira MO. Pseudomonas aeruginosa diversification during infection development in cystic fibrosis lungs-a review. Pathogens. 2014;3(3):680–703. https://doi.org/10.3390/pathogens3030680.
Jennings MT, Riekert KA, Boyle MP. Update on key emerging challenges in cystic fibrosis. Med Princ Pract. 2014;5(23):393–402. https://doi.org/10.1159/000357646.
Bernardy EE, Petit RA, Moller AG, Blumenthal JA, McAdam AJ, Priebe GP, et al. Whole-genome sequences of Staphylococcus aureus isolates from cystic fibrosis lung infections. Microbiol Resour Announc. 2019;3(8):e01564-e1618. https://doi.org/10.1128/MRA.01564-18.
Lavelle GM, White MM, Browne N, McElvaney NG, Reeves EP. Animal models of cystic fibrosis pathology: phenotypic parallels and divergences. BioMed Res Int. 2016. https://doi.org/10.1155/2016/5258727.
Bell SC, Mall MA, Gutierrez H, Macek M, Madge S, Davies JC, et al. The future of cystic fibrosis care: a global perspective. Lancet Respir Med. 2020;1(8):65–124. https://doi.org/10.1016/S2213-2600(19)30337-6.
Yagci S, Hascelik G, Dogru D, Ozcelik U, Sener B. Prevalence and genetic diversity of Staphylococcus aureus small-colony variants in cystic fibrosis patients. Clin Microbiol Infect. 2013;1(19):77–84. https://doi.org/10.1111/j.1469-0691.2011.03742.x.
Stone A, Saiman L. Update on the epidemiology and management of Staphylococcus aureus, including methicillin-resistant Staphylococcus aureus, in patients with cystic fibrosis. Curr Opin Pulm Med. 2007;6(13):515–21. https://doi.org/10.1097/MCP.0b013e3282efbbac.
Cafiso V, Bertuccio T, Spina D, Campanile F, Bongiorno D, Santagati M, et al. Methicillin resistance and vancomycin heteroresistance in Staphylococcus aureus in cystic fibrosis patients. Eur J Clin Microbiol Infect Dis. 2010;10(29):1277–85. https://doi.org/10.1007/s10096-010-1000-5.
Goodrich JS, Sutton-Shields TN, Kerr A, Wedd JP, Miller MB, Gilligan PH. Prevalence of community-associated methicillin-resistant Staphylococcus aureus in patients with cystic fibrosis. J Clin Microbiol. 2009;4(47):1231–3. https://doi.org/10.1128/JCM.00255-09.
Gemmell CG, Edwards DI, Fraise AP, Gould FK, Ridgway GL, Warren RE. Guidelines for the prophylaxis and treatment of methicillin-resistant Staphylococcus aureus (MRSA) infections in the UK. J Antimicrob Chemother. 2006;4(57):589–608. https://doi.org/10.1093/jac/dkl017.
Alexander B, Petren E, Rizvi S, Fink A, Ostrenga J, Sewall A, et al. Cystic Fibrosis Foundation patient registry annual data report. Bethesda, MD: Cystic Fibrosis Foundation; 2016.
De Vrankrijker A, Wolfs T, Van der Ent C. Challenging and emerging pathogens in cystic fibrosis. Paediatr Respir Rev. 2010;4(11):246–54.
Desmet K, Ortuño-Ortín I, Wacziarg R. Culture, ethnicity, and diversity. Am Econ Rev. 2017;9(107):2479–513.
Tokajian S. New epidemiology of Staphylococcus aureus infections in the Middle East. Clin Microbiol Infect. 2014;7(20):624–8. https://doi.org/10.1111/1469-0691.12691.
Enany S, Yaoita E, Yoshida Y, Enany M, Yamamoto T. Molecular characterization of Panton-Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus isolates in Egypt. Microbiol Res. 2010;2(165):152–62. https://doi.org/10.1016/j.micres.2009.03.005.
Biber A, Abuelaish I, Rahav G, Raz M, Cohen L, Valinsky L, et al. A typical hospital-acquired methicillin-resistant Staphylococcus aureus clone is widespread in the community in the Gaza strip. PLoS ONE. 2012;8(7):e42864. https://doi.org/10.1371/journal.pone.0042864.
Kaibni MH, Farraj MA, Adwan K, Essawi TA. Community-acquired meticillin-resistant Staphylococcus aureus in Palestine. J Med Microbiol. 2009;5(58):644–7. https://doi.org/10.1099/jmm.0.007617-0.
Boutin S, Dalpke AH. Acquisition and adaptation of the airway microbiota in the early life of cystic fibrosis patients. Mol Cell Paediatr. 2017;1(4):1–9. https://doi.org/10.1186/s40348-016-0067-1.
Lyczak JB, Cannon CL, Pier GB. Lung infections associated with cystic fibrosis. Clin Microbiol Rev. 2002;2(15):194–222. https://doi.org/10.1128/CMR.15.2.194-222.2002.
Wahab AA, Janahi I, Marafia M, El-Shafie S. Microbiological identification in cystic fibrosis patients with CFTR I1234V mutation. J Trop Paediatr. 2004;4(50):229–33. https://doi.org/10.1093/tropej/50.4.229.
Khaledi A, Khademi F, Esmaeili D, Esmaeili S, Rostami H. The role of HPaA protein as candidate vaccine against Helicobacter pylori. Der Pharma Chemica. 2016;8:235–7.
Marshall B, Fink A, Loeffler D, Elbert A, O’Neil T, Rush T, et al. Patient registry annual data report. Cystic Fibrosis Foundation; 2018.
Kahl BC, Duebbers A, Lubritz G, Haeberle J, Koch HG, Ritzerfeld B, et al. Population dynamics of persistent Staphylococcus aureus isolated from the airways of cystic fibrosis patients during a 6-year prospective study. J Clin Microbiol. 2003;9(41):4424–7. https://doi.org/10.1128/JCM.41.9.4424-4427.2003.
Vergison A, Denis O, Deplano A, Casimir G, Claeys G, DeBaets F, et al. National survey of molecular epidemiology of Staphylococcus aureus colonization in Belgian cystic fibrosis patients. J Antimicrob Chemother. 2007;5(59):893–9. https://doi.org/10.1093/jac/dkm037.
Goss CH, Muhlebach MS. Staphylococcus aureus and MRSA in cystic fibrosis. J Cyst Fibros. 2011;5(10):298–306. https://doi.org/10.1016/j.jcf.2011.06.002.
Anzaudo M, Busquets N, Ronchi S, Mayoral C. Isolated pathogen microorganisms in respiratory samples from children with cystic fibrosis. Rev Argent Microbiol. 2005;3(37):129–34.
Semczuk K, Dmeńska H, Dzierżanowska D, Kołodziejczyk M, Gabińska E, Zaręba H. The analysis of the isolated microorganisms from the respiratory tract of cystic fibrosis patients treated in Children’s Memorial Health Institute 1999–2002. Adv Respir Med. 2005;1–2(73):41–7.
Valenza G, Tappe D, Turnwald D, Frosch M, König C, Hebestreit H, et al. Prevalence and antimicrobial susceptibility of microorganisms isolated from sputa of patients with cystic fibrosis. J Cyst Fibros. 2008;2(7):123–7. https://doi.org/10.1016/j.jcf.2007.06.006.
Khaledi A, Khademi F, Esmaeili D, Esmaeili S-A, Rostami H. The role of HPaA protein as candidate vaccine against Helicobacter pylori. Der Pharma Chemica. 2016;3(8):235–7.
Nobandegani NM, Mahmoudi S, Pourakbari B, Sadeghi RH, Sani MN, Farahmand F, et al. Antimicrobial susceptibility of microorganisms isolated from sputum culture of patients with cystic fibrosis: methicillin-resistant Staphylococcus aureus as a serious concern. Microb Pathog. 2016;100:201–4. https://doi.org/10.1016/j.micpath.2016.09.015.
Khanbabaee G, Akbarizadeh M, Sayyari A, Ashayeri-Panah M, Abdollahgorji F, Sheibani K, et al. A survey on pulmonary pathogens and their antibiotic susceptibility among cystic fibrosis patients. Braz J Infect Dis. 2012;2(16):122–8.
Aghamohammadi A, Keivanfar M, Navaei S, Shirzadi R, Masiha F, Allameh Z, et al. First cystic fibrosis patient registry annual data report-cystic fibrosis foundation of Iran. Acta Med Iran. 2019;1(57):33–41.
Wahab AA, Taj-Aldeen SJ, Kolecka A, ElGindi M, Finkel JS, Boekhout T. High prevalence of Candida dubliniensis in lower respiratory tract secretions from cystic fibrosis patients may be related to increased adherence properties. Int J Infect Dis. 2014;24:14–9. https://doi.org/10.1016/j.ijid.2014.03.1380.
Thomas M, Raja M, Albakri M, Najim M, Chandra P, Allangawi M. CT score and correlation with lung function and microbiology of adult patients with cystic fibrosis with predominant I1234V genotype in Qatar. Qatar Med J. 2020. https://doi.org/10.5339/qmj.2020.4.
Elshafie SS, Wahab AA, Al Janahi I. Antimicrobial resistance of bacterial strains isolated from respiratory tract of cystic fibrosis patients with CFTR I1234V mutation. J Pediatr Infect Dis. 2007;01(2):039–43.
Pakasticali N, Kaya G, Senel U, Kipritci O, Tamay Z, Guler N, et al. Prevalence, antibiotic and pulsed-field gel electrophoresis patterns of Staphylococcus aureus small-colony variants in cystic fibrosis patients. Southeast Asian J Trop Med Public Health. 2016;3(47):475–84.
Yurdakul P, Ocal HY, Gulmez D, Yalcin E, Dogru D, Cinel G, et al. Predominance of hospital-associated MRSA among cystic fibrosis patients in a Turkish reference cystic fibrosis centre. J Chemother. 2012;4(24):195–200. https://doi.org/10.1179/1973947812Y.0000000024.
Frossard P, Hertecant J, Bossaert Y, Dawson K. Genotype-phenotype correlations in cystic fibrosis: clinical severity of mutation S549R (T–> G). Eur Respir J. 1999;1(13):100–2. https://doi.org/10.1183/09031936.99.13110099.
El-Falaki MM, Shahin WA, El-Basha NR, Ali AA, Mehaney DA, El-Attar MM. Profile of cystic fibrosis in a single referral center in Egypt. J Adv Res. 2014;5(5):563–8. https://doi.org/10.1016/j.jare.2013.07.005.
Acknowledgements
We would like to thank our colleagues for their help in this study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YN and AFA conducted data extraction, analysis, and wrote the first draft of the paper; PA and MRT conducted data Extraction; PS, EN and AK designed the study, analyses, and drafting of the article. All authors contributed to discuss results and writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2020 Checklist for reporting systematic reviews.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nikmanesh, Y., Foolady Azarnaminy, A., Avishan, P. et al. A Middle East systematic review and meta-analysis of prevalence and antibiotic susceptibility pattern in MRSA Staphylococcus aureus isolated from patients with cystic fibrosis. J Health Popul Nutr 41, 26 (2022). https://doi.org/10.1186/s41043-022-00305-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-022-00305-x