
Abstract
Hypertension is one of the most common comorbidity and the leading cause of cancer-related death in cancer patients. The prevalence of hypertension in cancer patients is much higher than that of the general population. In the older population of cancer patients, specific cancer treatments such as new tyrosine kinase inhibitors and Vascular endothelial growth factor inhibitor drugs give rise to hypertension in cancer patients; The aim of present study is to provide a detailed discussion etiologies of cancer treatment-induced hypertension and explore the most innovative diagnostic and management approaches. This review will address the optimal approach to hypertension treatment, covering treatment initiation thresholds, targets, and the selection of anti-hypertensive agents. The lack of evidence in recent guidelines for managing cardiovascular toxicities in cancer patients can create uncertainty in clinicians' therapeutic and clinical decisions. This review aims to enhance our understanding of hypertension etiology in cancer patients and provide a practical guide to current treatment approaches.
Similar content being viewed by others


Background
Improvements in early diagnosis and novel cancer treatments have increased the survival rate of cancer patients [1]. Decreased cancer mortality due to novel cancer therapies resulting from novel cancer therapies has led to an increase in short- and long-term cardiovascular complications in these patients [2]. Cardiovascular disease is one of the most common cause of mortality and morbidity in cancer patients [3]. Among cancer patients, cardiovascular adverse events such as heart failure, coronary artery disease, valvular heart disease, and hypertension are prevalent [4, 5]. Previous studies have shown that hypertension is associated with an increased risk of developing certain malignancies, and hypertensive patient experienced higher rates of cancer-related mortality [6,7,8]. In the older population of cancer patients, specific cancer treatments such as new tyrosine kinase-targeting and Vascular endothelial growth factor inhibitor (VEGFi) drugs can lead to hypertension in cancer patients [9, 10]. Certain pieces of evidence in recent guidelines on managing cardiovascular toxicities in cancer patients may create uncertainty in clinicians' therapeutic and clinical decisions [11, 12]. Hypertension management in cardio-oncology presents significant challenges [13]. Our review aims to provide an updated understanding of the etiology and management of hypertension in cancer patients and offer a practical guide to current treatment approaches. Given the high prevalence of various cancer patients, hypertension management in oncology is applicable not only to cardio-oncologists but would be an essential part of practice among oncologists, general cardiologists, and primary care physicians in the near future. This review has the potential to be a reference guide for clinicians who care for cancer patients with hypertension.
Etiologies of cancer treatment-induced Hypertension
Vascular endothelial growth factor inhibitors
Vascular endothelial growth factor inhibitors (VEGFi) drugs are effective and safe components of the anti-cancer treatment for patients with solid malignancy tumors [14]. Next, we will discuss the mention most commonly used VEGFi drugs in cancer treatment. Bevacizumab (Avastin) is utilized in the treatment of various cancers, including colorectal, lung, kidney, and ovarian cancer [15]. Sorafenib (Nexavar) is also commonly used to treat Renal cell carcinoma, hepatocellular carcinoma, and advanced thyroid carcinoma [16]. Sunitinib (Sutent) is another drug used to treat kidney cancer (renal cell carcinoma) and gastrointestinal stromal tumors (GISTs) [17, 18].
Notably, VEGFi increases blood pressure in almost all patients [19]. VEGFi-induced hypertension is dose-dependent and is associated with these drugs' anti-cancer effects [20]. VEGFi increases blood pressure by increasing endothelin-1(ET-1), reducing NO bioavailability, and increasing salt sensitivity by activating the renal epithelial sodium channels(ENaC) [20]. Moreover, some new findings indicate the critical roles of prostacyclin and endothelial microparticles in VEGFi-induced hypertension [21,22,23,24,25].
The primary mechanism of VEGFi-induced hypertension is increased ET-1, leading to vasoconstriction and hypertension [26, 27]. VEGFi increases ET-1 with several mechanisms, including the inactivation of ETB receptors, endothelial dysfunction, and producing vasoconstrictor prostanoids [14, 23, 28, 29]. VEGFi decreases Nitric Oxide(NO) by inactivating the endothelial nitric oxide synthase (eNOS) enzyme and subsequently reduces the bioavailability of NO [30]. As mentioned above, increased vasoconstrictors, mainly ET-1 and decreased vasodilators, especially NO, are two key mechanisms of VEGFi-induced hypertension.
The incidence of VEGFi-induced hypertension varies based on differences in genetics, dosage, and duration of treatment [13]. Axitinib and Sorafenib induce hypertension in 40.4% and 29.0% of patients with renal cell carcinoma, respectively [31]. Recent studies have reported the incidence and relative risk of VEGFi-induced hypertension to be ranging from 4% to 84% and 3 to 9%, respectively [13, 20].
Immunotherapeutic agents
Mammalian target rapamycin (mTOR) inhibitors
Mammalian target rapamycin (mTOR) inhibitors are used as an effective anti-cancer treatment in various solid organ neoplasms like pancreatic neuroendocrine tumors, mantle cell lymphoma, and renal cancer [32, 33]. mTOR inhibitors may induce hypertension through various mechanisms, including increased oxidative stress and sympathetic activation, leading to afferent arteriolar vasoconstriction and hypertension [34].
Everolimus (mTOR inhibitor) in combination with lenvatinib causes hypertension in 42% of metastatic renal cell carcinoma patients [35]. Notably, the incidence of hypertension with everolimus and sirolimus ranges between 17%-30% and 21%-38%, respectively. Hypertension is a common side effect of mTOR inhibitors, whereas some clinical trials demonstrate no significant hypertension increase compared to comparator agents [34, 36, 37].
Proteasome inhibitor
Dysregulation of The ubiquitin-proteasome system by proteasome inhibitors like bortezomib and carfilzomib has been tested in different cancers, such as multiple myeloma [38]. Proteasome inhibition in cardiomyocytes and smooth muscle endothelium, resulting in dysregulated NO hemostasis and vasoconstriction are possible mechanisms of hypertension induced by these drugs [39, 40]. Carfilzomib is strongly associated with increased cardiovascular adverse events, including heart failure, hypertension, cardiac ischemia, arrhythmia, and cardiac arrest [41]. Carfilzomib, a first-generation proteasome inhibitor, is associated with the risk of hypertension in multiple myeloma patients (HR= 3.33, p < 0.0001) [42].
Traditional chemotherapeutic agents
Alkylating agents, the earliest drugs used in cancer treatment, work by ultimately creating cross-linkage between two DNA strands, leading to cell death [43]. These drugs are frequently used in the treatment of leukemia, lymphoma, head and neck cancers, and genitourinary cancers [44]. The connection between Alkylating agents and hypertension remains unclear because they are usually used in combination with other drugs for cancer treatment [45]. Cyclophosphamide has a wide range of complications, such as nephrotoxicity, endothelial injury, and abnormalities in the renin-angiotensin system leading to hypertension [46, 47]. While the mechanisms mentioned above could potentionally render Cyclophosphamide-associated Hypertension possible, it has not yet been recognized as an independent risk factor for hypertension in cancer patients. Hypertension was reported in pediatric cancer patients who were treated with ifosfamide [48].
Recent studies do not indicate hypertension as one of the complications in cancer treatment field [49]. Notably, in the meta-analysis of Zhang et al., Hypertension (OR: 2.95, 95%CI: 1.75-4.97, p < 0.0001) is one of the risk factors of anthracycline-induced cardiotoxicity [50].
Since the first time cisplatin was used for cancer treatment, platinum-based cancer therapy drugs have been one of the most popular and widespread of their kind for cancer treatment [51]. Platinum-based drugs are used in the treatment of lymphomas, sarcomas, breast, colorectal, germ cell, ovarian, lung, gastro-oesophageal, and bladder cancers [52]. In a study by Herradón et al., the administration of cisplatin for five weeks caused a decrease in systolic and diastolic blood pressure in rats [53]. After ten weeks of treatment, blood pressure decreased significantly after cisplatin- and bleomycin-containing chemotherapy for testicular cancer [54]. Notably, after a median follow-up time of 11.2 years in patients with testicular cancer, the ones treated with cisplatin had higher systolic and diastolic blood pressure levels than those treated with surgery [55]. Therefore, it can be concluded that cisplatin treatment may cause a decrease in blood pressure in early stages of treatment, but, in the long run, it will bring about an upsurge in systolic and diastolic blood pressure.
BCR-ABL tyrosine-kinase inhibitors (TKIs)
BCR-ABL tyrosine kinase inhibitors (TKIs) are a type of targeted therapy agents used in cancer treatment, particularly in chronic myeloid leukemia (CML). BCR-ABL TKIs block the function of the BCR-ABL1 protein, causing CML cells to die. The first-line of treatment for CML is BCR-ABL TKI therapy, which includes imatinib mesylate, dasatinib, nilotinib, and bosutinib. BCR-ABL TKIs have been developed as a targeted treatment for BCR-ABL1 kinase activity suppression and are used to treat various malignancies. Second-generation BCR-ABL TKIs have been developed to overcome mutations. Drug resistance is the main challenge in BCR-ABL TKI therapy, and designing treatment strategies targeting epigenetic pathways is a potential solution [56, 57].
Limited data available suggests that BCR-ABL tyrosine-kinase inhibitors (TKIs) are associated with multiple cardiovascular and pulmonary adverse events, including pulmonary hypertension, potentially attributable to the fact that the inhibition of the tyrosine kinase BCR-ABL1 is not specific to cancer cells, but rather can affect healthy cells. Renovascular hypertension has been reported as a rare side effect of BCR-ABL TKIs that inhibits vascular endothelial growth factors. However, edema and fluid retention are reported as more common side effects of BCR-ABL TKIs. Recent evidence suggests that tyrosine kinase has a particular role in cardiovascular calcification, specifically the calcification of heart vessels and valves [58, 59].
BRAF and MEK inhibitors
BRAF and MEK inhibitors are targeted therapies used in cancer treatment, targeting the MAPK signaling pathway. Trametinib was the first FDA-approved MEK inhibitor for cancer therapy which has the property of BRAF/MEK heterodimer breaker and binds to the interface of MEK and BRAF [60]. These groups of drugs are effective in the treatment of various types of cancer, particularly those accociated with RAS or BRAF mutations [61]. BRAF and MEK inhibitors have several side effects, including skin rash, diarrhea, nausea, vomiting, fatigue, and liver toxicity. MEK inhibitors monotherapy or in combination with other targeted drugs harboring the MAPK pathway is becoming a promising strategy for non-small cell lung cancer (NSCLC) patients with BRAF or KRAS mutations [62]. It is noteworthy to mention that 19.5% of hypertension incidence is observed in patients who have used BRAF and MEK inhibitors [63]. In a meta-analysis on the incidence of treatment-related adverse events of BRAF and MEK inhibitors, for patients receiving Dabrafenib + Trametinib, the predominant grade 3 or higher adverse events were pyrexia, rash, and hypertension, collectively accounting for 6% of cases. Also individuals undergoing Encorafenib + Binimetinib regimen encountered incidences of rash and hypertension, amounting to 6% [64].
Vinca alkaloids
Vinca alkaloids are effective microtubule-targeting agents used in treating hematological and lymphatic neoplasms [65]. Recent studies suggest Vinca Alkaloids are associated with cardiovascular adverse events, such as hypertension [66, 67]. The mechanism of Vinca Alkaloids-induced hypertension is unclear, however, mitosis-mediated inhibition of endothelial cell proliferation and endothelial cell caspase-mediated apoptosis are the possible routes [44]. Considering Vinca Alkaloids are usually used in combination with other chemotherapy agents, the specific effects of these drugs on patients' blood pressure are not well defined.
Endocrine therapy
Recent improvements in understanding how tumors evolve during treatment with endocrine agents have identified changes in gene expression and mutational profiles in the primary cancer cells as well as in circulating tumor cells. Endocrine therapy is a standard treatment for hormone receptor-positive breast cancer [68].
Anti-androgen therapy, including Cyproterone acetate, Flutamide, Bicalutamide, and Enzalutamide, is adjuvant chemotherapy used to treat different cancer types, such as prostate, breast, kidney, and ovarian cancer [69]. Abiraterone and enzalutamide are novel anti-cancer agents used in the treatment of prostate cancer. Based on a meta-analysis of 7 articles, Abiraterone has induced hypertension in 20% of patients. It was associated with an increased risk of cardiotoxicity [70]. Notably, enzalutamide was associated with increased risks of any grade (RR = 2.66, 95% CI = 1.93-3.66) and severe grade hypertension (RR = 2.79, 95% CI = 1.86-4.18) [71]. Anti-androgen agents cause hypertension by blocking the cytochrome P450 17A1, leading to a decrease in androgen synthesis and an increase in ACTH, resulting in increased mineralocorticoid production. Increased production of mineralocorticoids will lead to hypertension [72].
Adjuvant therapies
Corticosteroids are used in cancer treatment as adjuvant therapy for pain alleviation or as an antineoplastic agent in treating brain tumors [73, 74]. Corticosteroids such as hydrocortisone, methylprednisone, and prednisone cause dose-dependent hypertension because of their mineralocorticoid effect, especially at high doses [75]. They cause salt and water retention and increase sensitivity to other vasoconstrictive drugs, eventually leading to hypertension [13].
Calcineurin inhibitors like cyclosporine and tacrolimus are essential immunosuppressive drugs used in oncology, almost as adjuvant therapy [76, 77]. They cause salt and water retention and increase sensitivity to other vasoconstrictive drugs, eventually leading to hypertension [78]. They suppressed the transcription of IL-2 and several other cytokines in T lymphocytes [79].
Hypertension is a common side effect of erythropoietin-stimulating agents in healthy individuals, especially in patients with chronic kidney disease [80,81,82]. Based on a meta-analysis of 52 clinical trials, using erythropoietin-stimulating agents to treat cancer-related anemia causes hypertension and increases adverse events such as mortality [83]. Vasoconstriction of vessels by rising levels of ET-1 and constrictor prostanoids, calcium influx in smooth muscle cells of blood vessels, and anti-natriuresis are underlying mechanisms of erythropoietin-stimulating agents-induced hypertension [84].
30% to 50% of individuals with cancer will experience moderate to severe pain, and non-steroidal anti-inflammatory drugs (NSAIDs) are widely used for chronic pain control in cancer patients [85, 86]. Hypertension is one of the side effects of regular NSAID use because they inhibit the production of prostaglandins; a decrease in prostaglandins I2 and E2 results in vasoconstriction and sodium retention, provoking hypertension [87, 88].
Radiotherapy
Head and neck radiotherapy may subsequently cause baroreflex failure, leading to resistant hypertension and hypertension crisis [89, 90]. Conversely, in an analysis of 19 patients undergoing head and neck radiation, the systolic and diastolic blood pressure was significantly reduced 90 days after surgery [91].
The baroreceptors regulate blood pressure by transmitting signals to the central nervous system, altering peripheral vascular resistance and cardiac output. Development of labile or paroxysmal hypertension in some individuals after receiving radiation treatment were observed in some studies [92]. Labile hypertension is defined as occasional asymptomatic blood pressure variations, usually attributable to emotional distress [93]. Paroxysmal hypertension is characterized by a sudden rise of blood pressure, passing over 200/110 mmHg, combined with an abrupt onset of physical symptoms, such as headache, chest discomfort, dizziness, nausea, palpitations, flushing, and sweating, taking anywhere between 10 minutes to several hours [94]. On the other hand, baroreceptors' damage can lead to hypotension. Low blood pressure can occur as a result of peripheral, autonomic nervous, and carotid baroreceptor system damage, leading to orthostatic hypotension, presented by dizziness in an upright position after sitting or lying down for a while [95, 96].
Radiation nephropathy is a renal injury caused by ionizing radiation [97]. Besides hypertension, hypertensive crisis and encephalopathy may happen as a result of renal injury [97]. Renal artery stenosis is one of the abdominal radiation complications leading to hypertension [98]. Table 1 summarizes the mechanisms of action responsible for hypertension and other side effects of each anti-cancer agents. Figure 1 illustrates these mechanisms in detail.

mechanisms of anti-cancer agents in inducing hypertension. Anti-cancer agents induce hypertension through various mechanisms. A better understanding of these mechanisms can help physicians to choose the proper therapeutic strategies for hypertension treatment in cancer patients. ACTH= Adrenocorticotropic Hormone, CVD=Cardiovascular disease, ET= Endothelin, ET-1 = Endothelin-1, NO=Nitric oxide, RAAS= Renin-angiotensin-aldosterone system VEGFi = Vascular endothelial growth factor inhibitor
Assessment, diagnosis, and management of cancer treatment-induced hypertension
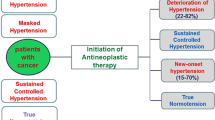
Based on recent studies, cancer patients are considered at a higher risk of hypertension compared to the general population [6]. Hypertension in cancer patients may sometimes occur just after the initiation of chemotherapies and sometimes, years after; hence, both short and long-term management approaches should be considered [118].
Hypertension is associated with an increased risk of mortality among cancer patients [8]. Recent studies have demonstrated that untreated hypertension is strongly associated with the risk of heart failure during treatments with anthracyclines, ibrutinib, and VEGFi [118,119,120,121]. Hypertension is an independent risk factor for coronary artery disease, heart failure, valvular heart disease, and arrhythmias in cancer patients [122].
Therefore, Timely diagnosis and proper management of hypertension in cancer patients is a substantial issue for increasing the quality of life and decreasing mortality and morbidity in these patients. Risk assessment for cardiovascular toxicity prior to treatment is essential in cancer patients. Blood pressure should be monitored and assessed before the initiation of chemotherapy [123].
Assessment and diagnosis
2022 ESC Guidelines on cardio-oncology suggest treatment of hypertension in cancer patients based on 2018 ESC/European Society of Hypertension (ESH) Guidelines [12, 124]. Special cofounders for in-office hypertention in cancer patients are pain, anxiety-driven sympathetic overactivity, NSAIDs, or steroids as adjuvant therapies. Also, it has been noted that both white-coat hypertension and masked hypertension are much more prevalent among cancer patients compared to the general population [125]. Based on 2021 European Society of Hypertension practice guidelines, standard condition, posture, measurement frequency, and interval should be considered to minimizing confounders in in-office hypertention [126].
The 2013 ESH guideline recommended only in-office BP measurement for hypertention diagnosis, however, the 2018 ESH guideline suggested out-of-office BP measurements such as Ambulatory Blood Pressure Monitoring (ABPM) and home blood pressure monitoring (HBPM) [124].
After detecting the initial episodes of increased blood pressure, it is suggested to perform ambulatory blood pressure monitoring for twenty-four hours, but it has its limitations, and it is not feasible for the majority of the patients. Situations in which frequent blood pressure measurements are required over longer periods (during treatment initiation or dose changes in patients receiving anti-cancer treatments) makes the patients susceptible to hypertensive crisis. Worsening of hypertension can occur in a matter of days and can progress to a hypertensive emergency. Hence, home blood pressure monitoring (also known as self-monitoring of blood pressure) with a validated device is an appropriate choice to prevent this situation. This type of monitoring can be done by the patient and is quite feasible. It has less accuracy compared to ambulatory blood pressure monitoring but can be cost-effective in preventing neglected hypertension [63, 127, 128]. It is indicated that cancer patients should take their blood pressure twice a day, once before medication use and bedtime [129]. The threshold for initation of anti-hypertensive agents and how to select the proper anti-hypertensive agents are explained in Figs. 2 and 3. It is recommended to check the blood pressure for a second time 2 weeks after the initiation of the hypertension treatment. If the goals of the treatment are not met, clinicians should take the next step by changing the anti-hypertensive agents, increasing the dose of dihydropyridine CCB or beta-blocker, and perform a sleep study [130].

Thresholds for asymptomatic hypertension treatment in cancer patients. The threshold for initiating the hypertension treatment increases as the patient has a worse prognosis. Starting the hypertension treatment at the proper time is crucial in managing hypertension in cancer patients, especially in patients under treatment of VEGFi, because it has been indicated that the efficacy of these drugs is related to blood pressure increase in these patients

Pharmacological management of hypertension in cancer patients. Choosing the proper anti-hypertensive agent for cancer patients is essential in managing hypertension in these patients. ACE or ARB and CCB are the first-line treatment in hypertension treatment. In patients with resistant hypertention, beta-blockers, diuretics, and nitrates can be added to the therapeutic drugs. Beta-blockers are a good choice if cancer patients have high sympathetic tone, tumors with beta-receptor expression (such as angiosarcoma and multiple myeloma), and other cardiovascular comorbidities
Treatment
Treatment thresholds for asymptomatic hypertension in cancer patients are determined by the prognosis, metastasis, and chemotherapy status of the patients. As the prognosis worsens, treatment thresholds for asymptomatic hypertension increase, as shown in Fig. 2.
Lifestyle modification as a part of hypertension treatment:
Lifestyle modifications can be an important part of hypertension treatment for cancer patients. The following is an overview of findings that can help manage hypertensive disorders in non-pharmacological treatments.
Various types of anti-cancer medications have been accociated with the developement of hypertension in patients without a prior history of the condition, or with an aggravation of hypertension that was previously under control. Consequently, individuals diagnosed with cancer may be advised to modify their lifestyle in order to assist in managing their hypertension [7].
Modifications in daily life, such as maintaining a healthy weight and exercising regularly, can contribute to reducing blood pressure levels. One may significantly improve their health by following a diet that is low in salt and abundant in fruits, vegetables, and whole grains. Adhering to a consistent schedule of physical activity, limiting alcohol consumption, and cessasion of smoking also have a considerable impact on the prevention of hypertensive disorders [131]. Various classes of medications used for the treatment of cancer have been associated with the development of new-onset hypertension or exacerbation of previously well-controlled hypertension. Management of hypertension in patients on anti-cancer therapy is primarily empirical, with no current trial data supporting specific agents or strategies [63]. Although anti-hypertensive medication use has no consistent evidence of any impact on cancer risk, lifestyle modifications can still be an important part of hypertension treatment in cancer patients [132] Therefore, these modifications are recommended in order to help manage hypertension in cancer patients [133].
Pharmacological treatments
Notably, hypertension is an independent risk factor for developing cancer therapy-related cardiac dysfunction; Therefore, Angiotensin-converting enzyme (ACE) inhibitors and Angiotensin receptor blockers (ARBs) are the first choices in the treatment of hypertension in these patients [134]. It has been indicated that using renin-angiotensin system blockers may improve survival in cancer patients. To put it in more detail, in metastatic renal cell carcinoma, patients treated with sunitinib, the use of ACEIs or ARBs was associated with an improved overall survival rates [135,136,137,138]. In cases of proteinuria presence, ACEIs or ARBs are recommended as the first line of treatment [139,140,141].
Dihydropyridine Calcium channel blockers (CCBs) can be used for patients with uncontrolled hypertention despite the treatment with ACE/ ARBs [12, 122]. Notably, hepatotoxicity occurs using some VEGF inhibitors such as Pazopanib, Ponatinib, Regorafenib, Sorafenib, Sunitinib, and Vandetanib. Thus, the use of CCBs should be approached with caution [142].
Non-dihydropyridine calcium channel blockers use cytochrome p450 3A4, possibly leading to decreased metabolism of chemotherapy agents. Therefore, they are not suggested in the treatment of hypertension in cancer patients [143].
The blood pressure target for hypertension treatment in cancer patients is 140/90. Blood pressure targets for patients with chronic kidney disease and diabetes should be 130/80 mmHg [144]. 2022 ESC Guidelines on cardio-oncology suggest a blood pressure target of 140-160/90-100 mmHg for asymptomatic patients suffering from metastatic cancer [12]. Individualized blood pressure targets based on the prognosis of diabetes or kidney disease should be considered in managing hypertension in the cardio-oncology clinics.
If the patient's blood pressure is above 180/110 mmHg, any associated cancer treatment should be withheld tunill the blood pressure is below 160/100 mmHg [3, 12].
Diuretics, nitrates, and beta blockers are suggested for resistant hypertension as first-line Treatments (ACEIs, ARBs, and CCBs ) [12, 145]. Proper anti-hypertensive medication selection depends on various factors, as Fig. 3 demonstrates the approach to hypertension therapy in cancer patients.
Patient education
Cancer patients should be educated about the importance of blood pressure control and the potential risks of uncontrolled hypertension, such as target organ damage and cardiovascular adverse events. In this regard, patients should be informed about the causes of hypertension in cancer patients, including various anti-cancer therapies, and the potential side effects of anti-hypertensive drugs. The caregiver must educate them on which anti-cancer therapies have potential risks for developing malignant hypertension [7, 63, 131, 133, 144]. Patients should be educated about lifestyle modifications that can help lower blood pressure, such as weight loss, regular exercise, a healthy diet, and stress reduction. They need to be advised to monitor their blood pressure regularly at home and keep a record of their readings to share with their healthcare providers [7, 92].
Patient adherence to treatment
Patients should be encouraged to take their anti-hypertensive medications as prescribed and not to skip doses or discontinue them without consulting with their healthcare providers. Patients should be informed about the potential side effects of anti-hypertensive drugs and how to manage them [7, 144]. Also, they have to be educated to report any symptoms of uncontrolled hypertension to their healthcare providers, such as headache, chest pain, shortness of breath, or vision changes, immediately [131] . They need to be reminded to attend regular follow-up appointments with their physicians to monitor their blood pressure and adjust their treatment if necessary [7, 63, 131, 133, 144].
Summary and conclusion
Hypertension is a common cardiovascular complication in cancer patients, especially those who are treated with angiogenesis inhibitors. Chemotherapeutic agents, Radiation, Adjuvant therapies, and other causes such as pain, renal dysfunction, alcohol consumption, and even untreated sleep apnea cause hypertension in cancer patients. The burden of hypertention in cancer patients is much higher than the general population. Therefore, blood pressure assessment before chemotherapy initiation, timely diagnosis, and appropriate treatment are critical in these patients. In this review, we focused on the details of the appropriate approach for the treatment of hypertension, including thresholds for initiating the treatment, targets, and meticulous selection of anti-hypertensive agents for hypertension management. Figure 4 demonstrates the summary of the etiology, assessment, and management of hypertension in the cardio-oncology clinic.

Etiology, Assessment, Diagnosis, and Management of Hypertension in Cancer patients. Anti-cancer agents induce hypertension by different mechanisms, including vasoconstriction, salt and water retention, RAAS dysfunction, baroreflex failure and other mechanisms illustrated in the figure. Physicians should initiate the treatment at the right time by choosing the proper anti-hypertension drug
Main message
-
Hypertension is a common cardiovascular complication with a significant impact on the mortality and morbidity of cancer patients.
-
Blood pressure assessment before chemotherapy initiation, timely diagnosis, and appropriate treatment are critical in these patients.
-
Further studies are needed to clarify the benefits of hypertension control in cancer patients in detail.
Abbreviations
- AKI:
-
Acute kidney injury
- ENaC:
-
Epithelial sodium channel
- eNOS:
-
Endothelial nitric oxide synthase
- ET-1:
-
Endothelin-1
- mTOR:
-
Mammalian target rapamycin
- NO:
-
Nitric oxide
- TKI:
-
Tyrosine kinase inhibitors
- VEGFi:
-
Vascular endothelial growth factor inhibitor
- VEGF-TKIs:
-
Vascular endothelial growth factor tyrosine kinase inhibitors
References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33.
Ahmed T, Marmagkiolis K, Ploch M, Irizarry-Caro JA, Amatullah A, Desai S, et al. The Year in Cardio-oncology 2022. Curr Probl Cardiol. 2023;48(1):101435.
Essa H, Dobson R, Wright D, Lip GYH. Hypertension management in cardio-oncology. J Hum Hypertens. 2020;34(10):673–81.
Chang HM, Moudgil R, Scarabelli T, Okwuosa TM, Yeh ETH. Cardiovascular Complications of Cancer Therapy: Best Practices in Diagnosis, Prevention, and Management: Part 1. J Am Coll Cardiol. 2017;70(20):2536–51.
Totzeck M, Schuler M, Stuschke M, Heusch G, Rassaf T. Cardio-oncology - strategies for management of cancer-therapy related cardiovascular disease. Int J Cardiol. 2019;280:163–75.
Kibret AA, Aragie H, Belay DG, Molla MD, Teferi ET, Melese EB, et al. Hypertension and Its Associated Factors Among Cancer Patients at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: Hospital-Based Cross-Sectional Study. J Multidiscip Healthc. 2022;15:793–803.
Mohammed T, Singh M, Tiu JG, Kim AS. Etiology and management of hypertension in patients with cancer. Cardiooncology. 2021;7(1):14.
Grossman E, Messerli FH, Boyko V, Goldbourt U. Is there an association between hypertension and cancer mortality? Am J Med. 2002;112(6):479–86.
Fraeman KH, Nordstrom BL, Luo W, Landis SH, Shantakumar S. Incidence of new-onset hypertension in cancer patients: a retrospective cohort study. Int J Hypertens. 2013;2013:379252. https://doi.org/10.1155/2013/379252.
Duvillier P. Hypertension and cancer : Dangerous Liaisons. Ann Cardiol Angeiol. 2022;71(5):317–20.
Alexandre J, Cautela J, Ederhy S, Damaj GL, Salem JE, Barlesi F, et al. Cardiovascular Toxicity Related to Cancer Treatment: A Pragmatic Approach to the American and European Cardio-Oncology Guidelines. J Am Heart Assoc. 2020;9(18):e018403.
Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43(41):4229–361.
Gudsoorkar P, Ruf R, Adnani H, Safdar K, Sparks MA. Onco-hypertension: An Emerging Specialty. Adv Chronic Kidney Dis. 2021;28(5):477–89.e1.
Camarda N, Travers R, Yang VK, London C, Jaffe IZ. VEGF Receptor Inhibitor-Induced Hypertension: Emerging Mechanisms and Clinical Implications. Curr Oncol Rep. 2022;24(4):463–74.
Garcia J, Hurwitz HI, Sandler AB, Miles D, Coleman RL, Deurloo R, et al. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat Rev. 2020;86:102017.
Ben MA. Sorafenib in the treatment of advanced hepatocellular carcinoma. Saudi J Gastroenterol. 2008;14(1):40–2.
Kollmannsberger C, Soulieres D, Wong R, Scalera A, Gaspo R, Bjarnason G. Sunitinib therapy for metastatic renal cell carcinoma: recommendations for management of side effects. Can Urol Assoc J. 2007;1(2 Suppl):S41–54.
Wang D, Xiao F, Feng Z, Li M, Kong L, Huang L, et al. Sunitinib facilitates metastatic breast cancer spreading by inducing endothelial cell senescence. Breast Cancer Res. 2020;22(1):103.
Abdel-Qadir H, Ethier JL, Lee DS, Thavendiranathan P, Amir E. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: A systematic review and meta-analysis. Cancer Treat Rev. 2017;53:120–7.
Versmissen J, Mirabito Colafella KM, Koolen SLW, Danser AHJ. Vascular Cardio-Oncology: Vascular Endothelial Growth Factor inhibitors and hypertension. Cardiovasc Res. 2019;115(5):904–14.
Lugo-Gavidia LM, Burger D, Matthews VB, Nolde JM, Kiuchi MG, Carnagarin R, et al. Role of Microparticles in Cardiovascular Disease: Implications for Endothelial Dysfunction, Thrombosis, and Inflammation. Hypertension. 2021;77(6):1825–44.
Sansone R, Baaken M, Horn P, Schuler D, Westenfeld R, Amabile N, et al. Release of endothelial microparticles in patients with arterial hypertension, hypertensive emergencies and catheter-related injury. Atherosclerosis. 2018;273:67–74.
Amraoui F, Spijkers L, Hassani Lahsinoui H, Vogt L, van der Post J, Peters S, et al. SFlt-1 elevates blood pressure by augmenting endothelin-1-mediated vasoconstriction in mice. PloS One. 2014;9(3):e91897.
Mirabito Colafella KM, Neves KB, Montezano AC, Garrelds IM, van Veghel R, de Vries R, et al. Selective ETA vs. dual ETA/B receptor blockade for the prevention of sunitinib-induced hypertension and albuminuria in WKY rats. Cardiovasc Res. 2020;116(10):1779–90.
Steeghs N, Gelderblom H, Roodt JO, Christensen O, Rajagopalan P, Hovens M, et al. Hypertension and rarefaction during treatment with telatinib, a small molecule angiogenesis inhibitor. Clin Cancer Res. 2008;14(11):3470–6.
Kappers MH, van Esch JH, Sluiter W, Sleijfer S, Danser AJ, van den Meiracker AH. Hypertension induced by the tyrosine kinase inhibitor sunitinib is associated with increased circulating endothelin-1 levels. Hypertension. 2010;56(4):675–81.
Banfor PN, Franklin PA, Segreti JA, Widomski DL, Davidsen SK, Albert DH, et al. ETA receptor blockade with atrasentan prevents hypertension with the multitargeted tyrosine kinase inhibitor ABT-869 in telemetry-instrumented rats. J Cardiovasc Pharmacol. 2009;53(2):173–8.
Saleh L, Verdonk K, Visser W, van den Meiracker AH, Danser AJ. The emerging role of endothelin-1 in the pathogenesis of pre-eclampsia. Ther Adv Cardiovasc Dis. 2016;10(5):282–93.
Lee S, Chen TT, Barber CL, Jordan MC, Murdock J, Desai S, et al. Autocrine VEGF signaling is required for vascular homeostasis. Cell. 2007;130(4):691–703.
Neves KB, Rios FJ, van der Mey L, Alves-Lopes R, Cameron AC, Volpe M, et al. VEGFR (Vascular Endothelial Growth Factor Receptor) Inhibition Induces Cardiovascular Damage via Redox-Sensitive Processes. Hypertension. 2018;71(4):638–47.
Rini BI, Quinn DI, Baum M, Wood LS, Tarazi J, Rosbrook B, et al. Hypertension among patients with renal cell carcinoma receiving axitinib or sorafenib: analysis from the randomized phase III AXIS trial. Target Oncol. 2015;10(1):45–53.
Gasparri ML, Bardhi E, Ruscito I, Papadia A, Farooqi AA, Marchetti C, et al. PI3K/AKT/mTOR pathway in ovarian cancer treatment: are we on the right track? Geburtshilfe Frauenheilkd. 2017;77(10):1095–103.
Chiarini F, Evangelisti C, McCubrey JA, Martelli AM. Current treatment strategies for inhibiting mTOR in cancer. Trends Pharmacol Sci. 2015;36(2):124–35.
Kaplan B, Qazi Y, Wellen JR. Strategies for the management of adverse events associated with mTOR inhibitors. Transplant Rev. 2014;28(3):126–33.
Bendtsen MAF, Grimm D, Bauer J, Wehland M, Wise P, Magnusson NE, Infanger M, Krüger M. Hypertension Caused by Lenvatinib and Everolimus in the Treatment of Metastatic Renal Cell Carcinoma. Int J Mol Sci. 2017;18(8). https://doi.org/10.3390/ijms18081736.
De Simone P, Nevens F, De Carlis L, Metselaar HJ, Beckebaum S, Saliba F, et al. Everolimus With Reduced Tacrolimus Improves Renal Function in De Novo Liver Transplant Recipients: A Randomized Controlled Trial. Am J Transplant. 2012;12(11):3008–20.
Tsai M-K, Wu F-LL, Lai L-R, Lee C-Y, Hu R-H, Lee P-H. Decreased Acute Rejection and Improved Renal Allograft Survival Using Sirolimus and Low-Dose Calcineurin Inhibitors without Induction Therapy. Int J Artif Organs. 2009;32(6):371–80.
Park J, Cho J, Song EJ. Ubiquitin-proteasome system (UPS) as a target for anticancer treatment. Arch Pharm Res. 2020;43(11):1144–61.
Wu P, Oren O, Gertz MA, Yang EH. Proteasome Inhibitor-Related Cardiotoxicity: Mechanisms, Diagnosis, and Management. Curr Oncol Rep. 2020;22(7):66.
Chari A, Hajje D. Case series discussion of cardiac and vascular events following carfilzomib treatment: possible mechanism, screening, and monitoring. BMC Cancer. 2014;14(1):1–9.
Waxman AJ, Clasen S, Hwang WT, Garfall A, Vogl DT, Carver J, O'Quinn R, Cohen AD, Stadtmauer EA, Ky B, Weiss BM. Carfilzomib-associated cardiovascular adverse events: A systematic review and meta-analysis. JAMA Oncol. 2018;4(3):e174519. https://doi.org/10.1001/jamaoncol.2017.4519/.
Bishnoi R, Xie Z, Shah C, Bian J, Murthy HS, Wingard JR, et al. Real-world experience of carfilzomib-associated cardiovascular adverse events: SEER-Medicare data set analysis. Cancer Med. 2021;10(1):70–8.
Karati D, Mahadik KR, Trivedi P, Kumar D. Alkylating Agents, the Road Less Traversed, Changing Anticancer Therapy. Anticancer Agents Med Chem. 2022;22(8):1478–95.
Soultati A, Mountzios G, Avgerinou C, Papaxoinis G, Pectasides D, Dimopoulos MA, et al. Endothelial vascular toxicity from chemotherapeutic agents: preclinical evidence and clinical implications. Cancer Treat Rev. 2012;38(5):473–83.
Ruf R, Yarandi N, Ortiz-Melo DI, Sparks MA. Onco-hypertension: Overview of hypertension with anti-cancer agents. Journal of Onco-Nephrology. 2021;5(1):57–69.
Alshahrani S, Ali Thubab HM, Ali Zaeri AM, Anwer T, Ahmed RA, Jali AM, et al. The Protective Effects of Sesamin against Cyclophosphamide-Induced Nephrotoxicity through Modulation of Oxidative Stress, Inflammatory-Cytokines and Apoptosis in Rats. Int J Mol Sci. 2022;23(19):11615.
Al-Hashmi S, Boels PJ, Zadjali F, Sadeghi B, Sällström J, Hultenby K, et al. Busulphan-cyclophosphamide cause endothelial injury, remodeling of resistance arteries and enhanced expression of endothelial nitric oxide synthase. PloS One. 2012;7(1):e30897.
Hsiao W, Lapite A, Faig W, Abdel-Megid M, Carlson C, Hobbie W, Ginsberg J, Laskin B, Denburg M. Long- term kidney and cardiovascular complications in pediatric cancer survivors. J Pediatr. 2023;255:89–97.e1. https://doi.org/10.1016/j.jpeds.2022.10.029.
Hassen LJ, Lenihan DJ, Baliga RR. Hypertension in the Cardio-Oncology Clinic. Heart Fail Clin. 2019;15(4):487–95.
Zhang M, Yang H, Xu C, Jin F, Zheng A. Risk Factors for Anthracycline-Induced Cardiotoxicity in Breast Cancer Treatment: A Meta-Analysis. Front Oncol. 2022;12:899782.
Rottenberg S, Disler C, Perego P. The rediscovery of platinum-based cancer therapy. Nat Rev Cancer. 2021;21(1):37–50.
Grant CH, Gourley C. Chapter 2 - Relevant Cancer Diagnoses, Commonly Used Chemotherapy Agents and Their Biochemical Mechanisms of Action. In: Anderson RA, Spears N, editors. Cancer Treatment and the Ovary. Boston: Academic Press; 2015. p. 21–33.
Herradón E, González C, Uranga JA, Abalo R, Martín MI, López-Miranda V. Characterization of Cardiovascular Alterations Induced by Different Chronic Cisplatin Treatments. Front Pharmacol. 2017;8:196.
Nuver J, Smit AJ, van der Meer J, van den Berg MP, van der Graaf WT, Meinardi MT, et al. Acute chemotherapy-induced cardiovascular changes in patients with testicular cancer. J Clin Oncol. 2005;23(36):9130–7.
Sagstuen H, Aass N, Fosså SD, Dahl O, Klepp O, Wist EA, et al. Blood pressure and body mass index in long-term survivors of testicular cancer. J Clin Oncol. 2005;23(22):4980–90.
Rossari F, Minutolo F, Orciuolo E. Past, present, and future of Bcr-Abl inhibitors: from chemical development to clinical efficacy. J Hematol Oncol. 2018;11(1):84.
Amir M, Javed S. A review on the therapeutic role of TKIs in case of CML in combination with epigenetic drugs. Front Genet. 2021;12:742802. https://doi.org/10.3389/fgene.2021.742802.
Roa-Chamorro R, Jaén-Águila F, Puerta-Puerta JM, Torres-Quintero L, González-Bustos P, Mediavilla-García JD. Arterial hypertension assessment in a population with chronic myeloid leukemia. Sci Rep. 2021;11(1):14637.
Amin SO, Ruzicka M, Burns KD, Bence-Bruckler IA, Ryan SE, Hadziomerovic A, et al. Renovascular hypertension from the BCR-ABL tyrosine kinase inhibitor ponatinib. J Clin Hypertens. 2020;22(4):678–82.
Ufuk D, Jiajun Y, Yuen Rong MS, Shiru Q, Jiancheng H. Drug resistance in targeted cancer therapies with RAF inhibitors. Cancer Drug Resist. 2021;4(3):665–83.
Adamopoulos C, Ahmed TA, Tucker MR, Ung PMU, Xiao M, Karoulia Z, et al. Exploiting Allosteric Properties of RAF and MEK Inhibitors to Target Therapy-Resistant Tumors Driven by Oncogenic BRAF Signaling. Cancer Discov. 2021;11(7):1716–35.
Han J, Liu Y, Yang S, Wu X, Li H, Wang Q. MEK inhibitors for the treatment of non-small cell lung cancer. J Hematol Oncol. 2021;14(1):1.
Cohen JB, Brown NJ, Brown S-A, Dent S, Van Dorst DC, Herrmann SM, et al. Cancer Therapy–Related Hypertension: A Scientific Statement From the American Heart Association. Hypertension. 2023;80(3):e46–57.
Garutti M, Bergnach M, Polesel J, Palmero L, Pizzichetta MA, Puglisi F. BRAF and MEK inhibitors and their toxicities: A meta-analysis. Cancers (Basel). 2022;15(1):141. https://doi.org/10.3390/cancers15010141.
Martino E, Casamassima G, Castiglione S, Cellupica E, Pantalone S, Papagni F, et al. Vinca alkaloids and analogues as anti-cancer agents: Looking back, peering ahead. Bioorg Med Chem Lett. 2018;28(17):2816–26.
Batra A, Patel B, Addison D, Baldassarre LA, Desai N, Weintraub N, et al. Cardiovascular safety profile of taxanes and vinca alkaloids: 30 years FDA registry experience. Open Heart. 2021;8(2):e001849.
Bokemeyer C, Berger CC, Kuczyk MA, Schmoll H-J. Evaluation of long-term toxicity after chemotherapy for testicular cancer. J Clin Oncol. 1996;14(11):2923–32.
Selli C, Dixon JM, Sims AH. Accurate prediction of response to endocrine therapy in breast cancer patients: current and future biomarkers. Breast Cancer Res. 2016;18(1):118.
Student S, Hejmo T, Poterała-Hejmo A, Leśniak A, Bułdak R. Anti-androgen hormonal therapy for cancer and other diseases. Eur J Pharmacol. 2020;866:172783.
Iacovelli R, Ciccarese C, Bria E, Romano M, Fantinel E, Bimbatti D, et al. The Cardiovascular Toxicity of Abiraterone and Enzalutamide in Prostate Cancer. Clin Genitourin Cancer. 2018;16(3):e645–e53.
Lee HY, Chen HL, Teoh JY, Chen TC, Hao SY, Tsai HY, et al. Abiraterone and enzalutamide had different adverse effects on the cardiovascular system: a systematic review with pairwise and network meta-analyses. Prostate Cancer Prostatic Dis. 2021;24(1):244–52.
Zhu X, Wu S. Risk of hypertension in Cancer patients treated with Abiraterone: a meta-analysis. Clin Hypertens. 2019;25:5.
Wooldridge JE, Anderson CM, Perry MC. Corticosteroids in advanced cancer. Oncology (Williston Park, NY). 2001;15(2):225-234.
Dietrich J, Rao K, Pastorino S, Kesari S. Corticosteroids in brain cancer patients: benefits and pitfalls. Expert Rev Clin Pharmacol. 2011;4(2):233–42.
Kassel LE, Odum LE. Our Own Worst Enemy: Pharmacologic Mechanisms of Hypertension. Adv Chronic Kidney Dis. 2015;22(3):245–52.
Kaye D, Thompson J, Jennings G, Esler M. Cyclosporine therapy after cardiac transplantation causes hypertension and renal vasoconstriction without sympathetic activation. Circulation. 1993;88(3):1101–9.
Lassila M. Interaction of cyclosporine A and the renin-angiotensin system; new perspectives. Curr Drug Metab. 2002;3(1):61–71.
Safarini OA, Patel J. Calcineurin inhibitors; 2020.
Crouch Z, DeSantis ERH. Use of erythropoietin-stimulating agents in breast cancer patients: A risk review. Am J Health Syst Pharm. 2009;66(13):1180–5.
Lundby C, Thomsen JJ, Boushel R, Koskolou M, Warberg J, Calbet JA, et al. Erythropoietin treatment elevates haemoglobin concentration by increasing red cell volume and depressing plasma volume. J Physiol. 2007;578(Pt 1):309–14.
Berglund B, Ekblom B. Effect of recombinant human erythropoietin treatment on blood pressure and some haematological parameters in healthy men. J Intern Med. 1991;229(2):125–30.
Lundby C, Olsen NV. Effects of recombinant human erythropoietin in normal humans. J. Physiol. 2011;589(Pt 6):1265–71.
Tonelli M, Hemmelgarn B, Reiman T, Manns B, Reaume MN, Lloyd A, et al. Benefits and harms of erythropoiesis-stimulating agents for anemia related to cancer: a meta-analysis. Cmaj. 2009;180(11):E62–71.
Brar SK, Perveen S, Chaudhry MR, AlBabtain S, Amreen S, Khan S. Erythropoietin-Induced Hypertension: A Review of Pathogenesis, Treatment, and Role of Blood Viscosity. Cureus. 2021;13(1):e12804.
Basha R, Baker CH, Sankpal UT, Ahmad S, Safe S, Abbruzzese JL, et al. Therapeutic applications of NSAIDS in cancer: special emphasis on tolfenamic acid. Front Biosci-Sch. 2011;3(2):797–805.
Derry S, Wiffen PJ, Moore RA, McNicol ED, Bell RF, Carr DB, McIntyre M, Wee B. Oral nonsteroidal antiinflammatory drugs (NSAIDs) for cancer pain in adults. Cochrane Database Syst Rev. 2017;7(7):CD012638. https://doi.org/10.1002/14651858.
Lovell AR, Ernst ME. Drug-Induced Hypertension: Focus on Mechanisms and Management. Curr HypertensRep. 2017;19(5):39.
Albishri J. NSAIDs and hypertension. Anaesth Pain Intensive Care. 2019;171–3.
Timmers HJ, Wieling W, Karemaker JM, Lenders JW. Baroreflex failure: a neglected type of secondary hypertension. Neth J Med. 2004;62(5):151–5.
Ketch T, Biaggioni I, Robertson R, Robertson D. Four faces of baroreflex failure: hypertensive crisis, volatile hypertension, orthostatic tachycardia, and malignant vagotonia. Circulation. 2002;105(21):2518–23.
Leibowitz A, Grossman E, Berkovitch A, Levartovski M, Appel S, Sharabi Y, et al. The Effect of Head and Neck Radiotherapy on Blood Pressure and Orthostatic Hypotension in Patients With Head and Neck Tumors. Am J Hypertens. 2018;31(2):235–9.
Brook I. Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J. 2020;38(2):84–92.
Hayat A, Whittam D. Baroreceptor failure related to bilateral carotid artery disease: an uncommon cause of labile hypertension. Intern Med J. 2014;44(1):105–6.
Mann SJ. Labile and Paroxysmal Hypertension: Common Clinical Dilemmas in Need of Treatment Studies. Curr Cardiol Rep. 2015;17(11):99.
Shah-Becker S, Pennock M, Sinoway L, Goldenberg D, Goyal N. Baroreceptor reflex failure: Review of the literature and the potential impact on patients with head and neck cancer. Head Neck. 2017;39(10):2135–41.
Giannopoulos S, Texakalidis P, Jonnalagadda AK, Karasavvidis T, Giannopoulos S, Kokkinidis DG. Revascularization of radiation-induced carotid artery stenosis with carotid endarterectomy vs. carotid artery stenting: A systematic review and meta-analysis. Cardiovasc Revasc Med. 2018;19(5 Pt B):638–44.
Klaus R, Niyazi M, Lange-Sperandio B. Radiation-induced kidney toxicity: molecular and cellular pathogenesis. Radiat Oncol. 2021;16(1):43.
Fakhouri F, Alanore ALB, Rrolle J-P, Gury B, Raynaud A, Plouin P-F. Presentation and revascularization outcomes in patients with radiation-induced renal artery stenosis. Am J Kidney Dis. 2001;38(2):302–9.
Kadowaki H, Akazawa H, Ishida J, Komuro I. Mechanisms and Management of Immune Checkpoint Inhibitor-Related Cardiac Adverse Events. JMA J. 2021;4(2):91–8.
Ball S, Ghosh RK, Wongsaengsak S, Bandyopadhyay D, Ghosh GC, Aronow WS, et al. Cardiovascular toxicities of immune checkpoint inhibitors: JACC review topic of the week. J Am Coll Cardiol. 2019;74(13):1714–27.
Meraz-Muñoz A, Amir E, Ng P, Avila-Casado C, Ragobar C, Chan C, Kim J, Wald R, Kitchlu A. Acute kidney injury associated with immune checkpoint inhibitor therapy: incidence, risk factors and outcomes. J Immunother Cancer. 2020;8(1):e000467. https://doi.org/10.1136/jitc-2019-000467.
Minegishi S, Kinguchi S, Horita N, Namkoong H, Briasoulis A, Ishigami T, et al. Immune Checkpoint Inhibitors Do Not Increase Short-Term Risk of Hypertension in Cancer Patients: a Systematic Literature Review and Meta-Analysis. Hypertension. 2022;79(11):2611–21.
Achim A, Liblik K, Gevaert S. Immune checkpoint inhibitors - the revolutionary cancer immunotherapy comes with a cardiotoxic price. Trends Cardiovasc Med. 2022. https://doi.org/10.1016/j.tcm.2022.09.004.
van Dorst DCH, van Doorn L, Mirabito Colafella KM, Manintveld OC, Hassing HC, Danser AHJ, et al. Cardiovascular toxicity of angiogenesis inhibitors and immune checkpoint inhibitors: synergistic anti-tumour effects at the cost of increased cardiovascular risk? Clin Sci (Lond.). 2021;135(14):1649–68.
Sivendran S, Agarwal N, Gartrell B, Ying J, Boucher KM, Choueiri TK, et al. Metabolic complications with the use of mTOR inhibitors for cancer therapy. Cancer Treat Rev. 2014;40(1):190–6.
Schubert M-L, Schmitt M, Wang L, Ramos C, Jordan K, Müller-Tidow C, et al. Side-effect management of chimeric antigen receptor (CAR) T-cell therapy. Ann Oncol. 2021;32(1):34–48.
Thawani SP, Tanji K, De Sousa EA, Weimer LH, Brannagan TH III. Bortezomib-associated demyelinating neuropathy—clinical and pathologic features. J Clin Neuromuscul Dis. 2015;16(4):202–9.
Haguet H, Douxfils J, Chatelain C, Graux C, Mullier F, Dogné JM. BCR-ABL Tyrosine Kinase Inhibitors: Which Mechanism(s) May Explain the Risk of Thrombosis? TH Open. 2018;2(1):e68–88.
Weisberg E, Manley P, Mestan J, Cowan-Jacob S, Ray A, Griffin J. AMN107 (nilotinib): a novel and selective inhibitor of BCR-ABL. Br J Cancer. 2006;94(12):1765–9.
Tampellini M, La Salvia A, Scagliotti GV. Novel investigational therapies for treating biliary tract carcinoma. Expert Opin Investig Drugs. 2016;25(12):1423–36.
Keller G, Schafhausen P, Brümmendorf TH. Bosutinib. Small Mol Oncol. 2010:119–27.
Massaro F, Molica M, Breccia M. Ponatinib: a review of efficacy and safety. Curr Cancer Drug Targets. 2018;18(9):847–56.
Deininger MW. Nilotinib. Clin Cancer Res. 2008;14(13):4027–31.
Infante JR, Fecher LA, Falchook GS, Nallapareddy S, Gordon MS, Becerra C, et al. Safety, pharmacokinetic, pharmacodynamic, and efficacy data for the oral MEK inhibitor trametinib: a phase 1 dose-escalation trial. Lancet Oncol. 2012;13(8):773–81.
Roca E, Bruera E, Politi P, Barugel M, Cedaro L, Carraro S, et al. Vinca alkaloid-induced cardiovascular autonomic neuropathy. Cancer Treat Rep. 1985;69(2):149–51.
Moudi M, Go R, Yien CYS, Nazre M. Vinca alkaloids. Int J Prev Med. 2013;4(11):1231.
Noor B, Akhavan S, Leuchter M, Yang EH, Ajijola OA. Quantitative assessment of cardiovascular autonomic impairment in cancer survivors: a single center case series. Cardio-Oncology. 2020;6(1):1–8.
Group SR. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–16.
Di Lorenzo G, Autorino R, Bruni G, Carteni G, Ricevuto E, Tudini M, et al. Cardiovascular toxicity following sunitinib therapy in metastatic renal cell carcinoma: a multicenter analysis. Ann Oncol. 2009;20(9):1535–42.
Dickerson T, Wiczer T, Waller A, Philippon J, Porter K, Haddad D, et al. Hypertension and incident cardiovascular events following ibrutinib initiation. Blood. 2019;134(22):1919–28.
Szmit S, Jurczak W, Zaucha JM, Drozd-Sokołowska J, Spychałowicz W, Joks M, et al. Pre-existing arterial hypertension as a risk factor for early left ventricular systolic dysfunction following (R)-CHOP chemotherapy in patients with lymphoma. J Am Soc Hypertens. 2014;8(11):791–9.
Cohen JB, Geara AS, Hogan JJ, Townsend RR. Hypertension in cancer patients and survivors: epidemiology, diagnosis, and management. Cardio Oncology. 2019;1(2):238–51.
Rossello X, Dorresteijn JA, Janssen A, Lambrinou E, Scherrenberg M, Bonnefoy-Cudraz E, et al. Risk prediction tools in cardiovascular disease prevention: A report from the ESC Prevention of CVD Programme led by the European Association of Preventive Cardiology (EAPC) in collaboration with the Acute Cardiovascular Care Association (ACCA) and the Association of Cardiovascular Nursing and Allied Professions (ACNAP). Eur J Cardiovasc Nurs. 2019;18(7):534–44.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39(33):3021–104.
Costa L, Varella P, Del Giglio A. White coat effect in breast cancer patients undergoing chemotherapy. Eur J Cancer Care. 2003;12(4):372–3.
Stergiou GS, Palatini P, Parati G, O’Brien E, Januszewicz A, Lurbe E, et al. European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens. 2021;2021:39(7).
Touyz RM, Herrmann SM, Herrmann J. Vascular toxicities with VEGF inhibitor therapies–focus on hypertension and arterial thrombotic events. J Am Soc Hypertens. 2018;12(6):409–25.
Herrmann J, Lenihan D, Armenian S, Barac A, Blaes A, Cardinale D, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. Eur Heart J. 2022;43(4):280–99.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127–248.
Rao VU, Reeves DJ, Chugh AR, O’Quinn R, Fradley MG, Raghavendra M, et al. Clinical approach to cardiovascular toxicity of oral antineoplastic agents: JACC state-of-the-art review. J Am Coll Cardiol. 2021;77(21):2693–716.
Zhu X, Wu S. Risks and management of hypertension in cancer patients undergoing targeted therapy: a review. Clin Hypertens. 2022;28(1):14.
Copland E, Canoy D, Nazarzadeh M, Bidel Z, Ramakrishnan R, Woodward M, et al. Antihypertensive treatment and risk of cancer: an individual participant data meta-analysis. Lancet Oncol. 2021;22(4):558–70.
Cohen JB, Geara AS, Hogan JJ, Townsend RR. Hypertension in Cancer Patients and Survivors. JACC: CardioOncol. 2019;1(2):238–51.
Philip LJ, Findlay SG, Gill JH. Baseline blood pressure and development of cardiotoxicity in patients treated with anthracyclines: A systematic review. Int J Cardiol Cardiovasc Risk Prev. 2022;15:200153.
Li X, Sun J, Hu S. The renin-angiotensin system blockers as adjunctive therapy for cancer: a meta-analysis of survival outcome. Eur Rev Med Pharmacol Sci. 2017;21(6):1375–83.
Cheung KS, Chan EW, Seto WK, Wong IC, Leung WK. ACE (angiotensin-converting enzyme) inhibitors/angiotensin receptor blockers are associated with lower colorectal cancer risk: A territory-wide study with propensity score analysis. Hypertension. 2020;76(3):968–75.
Perini MV, Dmello RS, Nero TL, Chand AL. Evaluating the benefits of renin-angiotensin system inhibitors as cancer treatments. Pharmacol Ther. 2020;211:107527.
Sipahi I, Debanne SM, Rowland DY, Simon DI, Fang JC. Angiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trials. Lancet Oncol. 2010;11(7):627–36.
Budolfsen C, Faber J, Grimm D, Krüger M, Bauer J, Wehland M, et al. Tyrosine kinase inhibitor-induced hypertension: role of hypertension as a biomarker in cancer treatment. Curr Vasc Pharmacol. 2019;17(6):618–34.
Holden RM, Mustafa RA, Alexander RT, Battistella M, Bevilacqua MU, Knoll G, et al. Canadian society of nephrology commentary on the kidney disease improving global outcomes 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder. Can J Kidney Health Dis. 2020;7:2054358120944271.
Wright JT Jr, Bakris G, Greene T, Agodoa LY, Appel LJ, Charleston J, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: results from the AASK trial. Jama. 2002;288(19):2421–31.
Patel S, Dushenkov A, Jungsuwadee P, Krishnaswami A, Barac A. Team-based approach to management of hypertension associated with angiogenesis inhibitors. J Cardiovasc Transl Res. 2020;13(3):463–77.
Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(36):2768–801.
Mouhayar E, Salahudeen A. Hypertension in cancer patients. Tex Heart Inst J. 2011;38(3):263–5.
MacDonald TM, Williams B, Webb DJ, Morant S, Caulfield M, Cruickshank JK, et al. Combination therapy is superior to sequential monotherapy for the initial treatment of hypertension: a double-blind randomized controlled trial. J Am Heart Assoc. 2017;6(11):e006986.
Author information
Authors and Affiliations
Contributions
Azin Alizadeh: Conceptualization, and Final Revision, Amir Askari nejad : Data curation, Writing- Original draft preparation. Amir Ghaffari : Visualization, Table Preperation, Validation Sara Adimi : Writing- Reviewing and Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Askarinejad, A., Alizadehasl, A., Jolfayi, A.G. et al. Hypertension in Cardio-Oncology Clinic: an update on etiology, assessment, and management. Cardio-Oncology 9, 46 (2023). https://doi.org/10.1186/s40959-023-00197-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40959-023-00197-8