
Abstract
Background
Sustained motivation is essential for effective use of contraceptive methods by women in low- and middle-income countries as many women are likely to abandon contraceptives, especially when they continually experience episodes of failure. We aimed to determine the prevalence of discontinuation of contraceptives due to failure and its associated factors among Ugandan women aged 14–49 years.
Methods
A cross sectional study was conducted using the UDHS 2016 data. Multi stage stratified sampling was used to select participants. All eligible women aged 15 to 49 years at the time of the survey were enrolled. Bivariable and Multivariable logistic regression analysis were used to determine the factors associated with contraceptive failure. All analysis were done using Stata version 13. Contraceptive failure (getting pregnant while on contraceptives) within five years preceding the survey was the dependent variable.
Results
A total of 9061 women were included in the study. The overall prevalence of contraceptive failure was 5.6% [n = 506, 95% CI: 5.1–6.1] and was higher (6.2%) among women aged 20–29 years or had completed secondary education (6.1%). Having informed choice on contraceptives [aOR = 0.59, 95% CI: 0.49 – 0.72] and older age [aOR = 0.46, 95% CI: 0.24–0.89] were associated with lower odds of contraceptive failure.
Conclusion
The burden of contraceptive failure among women of reproductive age in Uganda is substantial and significantly varied by women's age, level of education, exposure to the internet, mass media, and informed choice. These findings highlight the need for improved counseling services and contraceptive quality to help women and couples use methods correctly and consistently.
Similar content being viewed by others


Background
Improving access to family planning (FP) services is fundamental to achieving the Sustainable Development Goals (SDGs) because it is strongly related with women’s and children's health, poverty reduction, education, gender equality, and human rights [1]. Access to family planning contributes up to a 44% reduction in maternal deaths [2], as most unplanned pregnancies and abortions occur in women who were either not using contraception or not using it consistently [3,4,5,6].Greater access to contraception and more consistent use are crucial in reducing unplanned pregnancies and abortions [7, 8].
The reasons for discontinuation of contraceptives can be grouped by whether they represent discontinuations due to reduced need (not in need) or discontinuations while women are presumably still exposed to the risk of pregnancy and do not want to become pregnant (in need) [9]. Among the not in-use discontinuations, wanting to become pregnant is the common reason while becoming pregnant yet using contraceptives (i.e. contraceptive failure) and side effects are the common reasons for in-need discontinuations [9].
Discontinuation of contraceptives for reasons other than the desire for pregnancy is problematic because of it’s association with several adverse reproductive health outcomes [10]. In countries with moderate to high contraceptive prevalence, most unintended pregnancies result from contraceptive failure [4, 11, 12]. Several studies have associated contraceptive discontinuation for reasons other than the desire to become pregnant with an unmet need for contraception and induced abortion [9, 13, 14]. Unintended pregnancies have been associated with an increased risk of maternal morbidity, health behaviors during pregnancy that are associated with adverse maternal health, and adverse fetal, infant, and child health outcomes [15]. Additionally, unintended pregnancies have negative psychological effects on women and their children [16].
In developing countries, 74 million unintended pregnancies occur annually, and nearly a third 30%, are due to contraceptive failure among women using some type of contraceptive method (whether traditional or modern).This includes both method-related failures (i.e., failure of a method to work as expected) and user-related failures (i.e., failure due to incorrect or inconsistent use of a method) [17].
About 44% of pregnancies in Uganda are unintended [18], with the occurrence of unsafe abortions estimated at 62% per 1000 women aged 15-49 years [19]. These undesirable maternal and child health outcomes associated with a high total fertility rate of 6.2 [20]could be substantially reduced by meeting the family planning needs of women in developing countries [21]. Moreover, a number of studies in Uganda have reported several obstacles to continuous contraceptive use among women of reproductive age, among which are method-related failures [8, 22,23,24].
Sustained motivation is essential for the effective use of contraceptive methods by women in low- and middle-income countries, as many women are likely to abandon the use of contraceptives, especially when they continually experience episodes of failure. A study exploring the predictors of contraceptive adherence among women seeking family planning services at a Reproductive Health Clinic in Uganda reported that lower educational level, lower self-efficacy, and lack of male partner support were predictive of reporting short birth intervals of less than 2 years [25]. Most Studies in Uganda have reported on the association between contraceptive use and discontinuation as a result of side effects, partner influence, and service quality, with limited literature on contraceptive failure [26,27,28]. Assessing contraceptive failure among demographic and socio-economic groups is important to inform efforts to improve contraceptive information, services and use, and to minimize contraceptive failures. Additionally, detailed information on contraceptive discontinuation due to unintended pregnancy is critical to inform improvements in the provision of contraceptive information, supplies, and services, which can help women and couples use methods correctly and consistently.
This study aimed to determine the prevalence of discontinuation of contraceptives due to failure among women aged 14–49 years using the 2016 UDHS data.
Methods
Study sampling and participants
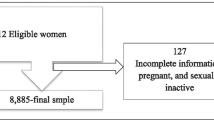
This was a cross-sectional study. We analyzed data collected during the UDHS conducted in 2016. "The Demographic and Health Surveys (DHS) are internationally comparable household surveys that collect information on demographic, socioeconomic, and health-related variables among nationally representative samples of households in developing countries. The DHS employs a two-stage sample design, with the first stage involving cluster selection consisting of enumeration areas (EAs). The second stage involves the systematic sampling of households in all the selected EAs” [29]. In this study, we used the women's recode file, which included women aged 15 to 49 years at the time of the survey. Out of the 18,505 women included in the UDHS women recode file, we included only women who had ever or were current users of contraceptives within the 5 year period preceding the survey to our study giving a total of 9,061 study participants.
Study variables
Dependent variable
Discontinuation of contraceptive use due to failure within a five-year period preceding the survey was the dependent variable. The DHS does not have a variable that records the discontinuation of contraceptive use due to failure. This was derived from the variable v360 which records the various reasons for discontinuation i.e., why did you stop using (Method)? The options/responses were 1) became pregnant, 2) wanted to become pregnant, 3) husband disapproved and 4) side effects among others. In this study, a woman becoming pregnant while on contraceptives was termed as a method failure and was coded as the outcome variable, while discontinuation due to another reason was coded for those who did not have the outcome of interest.
Independent variables
We included possible determinants of contraceptive use and discontinuation based on the available literature [7, 27, 30, 31]. Twenty-one (21) variables were considered and grouped as follows. Demographic factors which included (1) age in years (categorized as > 20, 20–29, 30–39, and 40–49), and the number of children delivered (categorized as none, 1,2,3,4 and 5 or more). Socio-economic factors which include (1) type of place of residence (rural vs. urban), (2) wealth index (categorized as lowest, second, middle, fourth, and highest), (3) Women's education attainment (Categorized as no formal education, primary education, secondary education, and higher), (4) phone ownership (yes vs. no), (6) internet use (categorized as Never, yes-last 12 months and yes –before last 12 months), (7) region of residence (Categorized as Northern, Eastern, Western and Southern), (8) work status (categorized as not currently employed and currently employed), (9) received information on family planning from mass media like radio, telephone, television and newspaper or magazine, (10) heard of family planning from field worker (Yes vs. no), and (11) heard of family planning from a healthcare facility (yes vs no). Cultural factors like 1) women's participation in decision-making for using contraceptives (categorized as woman only, husband only, joint decision and other), and informed choice (yes vs. no),Lastly, we also included the variable on the method of contraception (Modern vs. traditional) that was discontinued over the 5-year period preceding the survey.
Informed choice was a new variable created from five variables measured in the UDHS. These measured whether the woman was (1) told how about the side effects of contraceptives, (2) told about the side effects of contraceptives by a health or family planning worker, (3) told how to deal with side effects, (4) told about other family planning methods, and (5) told about other family planning methods by health or family planning worker. A woman was considered to have an informed choice if they responded with yes to any of the five variables.
Statistical analysis
The data used were obtained after receiving permission from the DHS program website. The dataset for the Uganda DHS 2016 was then downloaded from the DHS program website. The women's recode file, readable by Stata version 15 was selected for use.
To calculate the prevalence of discontinuation due to contraceptive failure, we created a new variable for which the denominator would be the total of the women who were currently using contraceptives at time of the survey interview and those who were not using at the time of the survey because they had discontinued.
All the analysis in this study was performed in Stata 13 (StataCorp LP 2013). Weighting was performed for all the descriptive statistics and for regression analysis.
For the categorical variables, we summarized them as weighted proportions. Variables that were numeric like age, were summarized as weighted means reporting standard deviations and 95% confidence intervals.
Bivariable logistic regression was used to determine the association between discontinuation due to contraceptive failure and the independent variables. From this, independent variables with p-values less than 0.2 were subjected to a test to assess for multi-collinearity using “variance inflation factor (VIF)” on Stata software. There was no multi-collinearity as the VIF were less than 3 for all the included variables.
Multivariable logistic regression was used, including the variables that had a p-value of less than 0.200 and variables that have been shown by literature to influence failure related contraceptive discontinuations [25, 32] i.e., age group, number of children a woman has, frequency of using the internet last month, heard about family planning from mass media, education and informed choice among others. We reported crude odds ratios (bi-variable), adjusted odds ratios (multi-variable), p-values, and 95% confidence intervals.
Results
Characteristics of the women
Table 1 shows the socio-demographic characteristics of the sample of women aged 15–49 who were current users/had ever used a contraceptive method within five years before the 2016 UDHS (n = 9061). The majority of the women (46.4%, n = 4204) were between age 20–29 years, and only 7.5% of the women had no formal education. Majority (80.3%) of the women were employed, and about 70.7% lived in rural areas of Uganda. Majority of women who used contraceptives had never been exposed to the internet in the last 12 months (89.0%, n = 8067). Additionally, 56.8% (n = 5153) of the women who used contraceptives owned a mobile phone. Among cultural factors, about two-thirds (61.2%) of the women made a joint decision with their partners on contraceptive use. 41.8% (n = 3788) of the women using contraceptives made an informed choice, while 58.2% (n = 5273) of the women did not make an informed choice. The most common methods used and discontinued in the past 5 years were injectable (54.8%), followed by implants (10.5%).
Current users or ever used contraceptives in past 5 years (9061).
Prevalence of discontinuation due to contraceptive failure
As shown in Table 2, the overall prevalence of contraceptive failure among Ugandan women aged 15–49 years during the 5-year period by demographic, socio-economic, and cultural factors was 5.6% (n = 506, 95% CI: 5.1—6.1). Among demographic factors, Contraceptive failure was prevalent in women aged 20–29 years (6.2%) and in those with five or more children (6.4%). For socioeconomic factors, the highest prevalence rates were seen in women who used the internet almost every day in the one month (7.8%, n = 426), owned a mobile phone (5.7%, n = 294), completed higher education (7.0%, n = 63), unemployed (5.8%, n = 104) and lived in a rural area (5.7%, n = 364).
Among cultural factors, women who had a joint decision for contraceptive use with their partner had the highest failure of the 5.0% (n = 134). Women who made an informed choice on contraceptive use experienced low contraceptive failure (4.4%, n = 168) as compared to those who didn't make an informed choice (6.4%, n = 338).
Table 3 shows the contraceptive failure in Uganda by the method used. Generally, traditional methods had the highest failure. Of this, withdrawal (36.3%, n = 134) was the single most common reason for failure. For modern contraceptive methods, short-term methods like emergency contraception (20.9%, n = 4) and pills (10.7%, n = 59) had higher failure when compared to long- term modern contraceptives like IUD (1.6%, n = 3) and implants (2.6%, n = 15) which had a very low failure.
Factors associated with contraceptive failure
Results from Bivariable analysis with their respective crudes odds ratios are detailed in Table 4. From multivariable analysis, women aged 40 to 49 years [Adjusted Odds ratio (aOR), 0.46; 95% CI: 0.24 – 0.89] were less likely to discontinue contraceptives due to failure compared to those aged less than 20 years.
Also, women with four children [aOR, 2.18; 95% CI: 1.11 – 4.28] and five or more children [aOR, 3.62; 95% CI: 1.84 – 7.13] were more likely to experience a contraceptive failure compared to those with no child.
Women who had secondary education [aOR, 1.57; 95% CI: 1.04 – 2.35] and higher education [aOR, 1.84; 95% CI, 1.09 – 3.09] were more likely to discontinue contraceptives due to failure compared to those who had no formal education. Women who currently in union/living with a man [aOR, 1.77; 95% CI: 1.04 – 3.01] were more likely to discontinue contraceptives due to failure compared to those who had never been in union.
Women who had an informed choice on contraceptives were less likely to discontinue contraceptives due to failure [aOR, 0.59; 95% CI: 0.49 – 0.72] compared to those who did not have an informed choice (Table 4).
Discussion
Contraceptive discontinuations contribute sustainably to the total fertility rate, unwanted pregnancies, and induced abortions [25]. This study aimed to establish and describe the prevalence of discontinuation of contraceptives due to failure among women aged 14–49 years in Uganda. Overall, the prevalence of failure-related discontinuation among Ugandan women was (5.6%) and varied by age, type of place of residence, phone ownership, access to mass media, Level of education, and marital status. We also found failure-related discontinuation to be strongly associated with the type of contraceptive method used [33].
In this study, women with access to the internet and mass media had high failure-related contraceptive discontinuation. This could be because women with access to the internet and mass media can easily access information on the different contraceptive methods and are, therefore, more likely to stop or switch to better contraceptive methods when they experience side effects [34].
Failure-related contraceptive discontinuation by methods were high in women who used traditional methods than in those who used modern contraceptive methods [35,36,37]. For modern contraceptive methods, women using short-term methods like pills and Injectables were more likely to experience failure than those using long-term contraceptive methods. This could be because of inconsistency when using short-term contraceptive methods, which expose women to increased failure rates. Similar findings were reported in [9, 33, 38]. Thus, information and counseling should be emphasized for short-term method users to prevent failure.
In multivariable analysis, the most important factors associated with contraceptive failure were women's age and informed choice. Women who were provided with adequate information about a particular contraceptive method and given an opportunity to make an informed choice were less likely to experience failure-related contraceptive discontinuation than women who did not make an informed choice. This could be because a woman who made an informed choice had adequate information about the contraceptive method of her choice and was able to effectively deal with its side effects without necessarily halting contraceptive use [39, 40]. This finding suggests that more time should be dedicated by clinicians to providing information on contraceptives to women before use. Furthermore, Women above 40 years had lower failure-related contraceptive discontinuation than women of other age brackets. This could be because women above 40 years are more likely than younger women to desire a permanent form of contraception [41, 42]. This could also be explained by lower fecundity, less frequent sexual intercourse, and higher compliance with contraceptive regimens, as evidenced by previous studies [43].
Lastly, multivariable analysis also showed that women with a higher level of education, five or more children and women who were currently in union/living with a man were more likely to experience failure related contraceptive discontinuation. This findings are in agreement with previous studies on contraceptive discontinuation in different countries [32, 33, 44,45,46,47].
We acknowledge that there are other reasons for discontinuing contraceptives, such as partner refusal, side effects, and method unavailability [9, 33, 48].
This study used retrospective data from the DHS. The DHS follows a rigorous methodology employing a two-stage cluster randomized sampling. We used sample weights to provide estimates reported in this study. However, we acknowledge that contraceptive failure could best be studied using cohort studies. Additionally, because the replies are self-reported and cannot be verified, there is a risk of information bias due to the sensitive nature of sexually related topics. But this study provides further information about the current state of the prevalence of discontinuation of contraceptives due to failure among women of reproductive age in Uganda.
Conclusion
Our study found that there was a significant prevalence of discontinuation of contraceptives due to failure among women of reproductive age in Uganda and that it varied by women's age, level of education, exposure to the internet and mass media, and informed choice. These findings highlight the need for improved counseling services and contraceptive quality to help women and couples use methods correctly and consistently.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the Demographic and Health Survey program website, https://dhsprogram.com/data/available-datasets.cfm and can be accessed after obtaining approval.
References
Goli S, James Moradhvaj KS, Singh D, Srinivasan V. Road to family planning and RMNCHN related SDGs: Tracing the role of public health spending in India. Glob Public Health. 2021;16:546–62.
Starbird E, Norton M, Marcus R. Investing in family planning: Key to achieving the sustainable development goals. Glob Heal Sci Pract. 2016;4:191–210. https://doi.org/10.9745/GHSP-D-15-00374.
Delbanco S, Lundy J, Hoff T, Parker M, Smith MD. Public knowledge and perceptions about unplanned pregnancy and contraception in three countries. Fam Plann Perspect. 1997;29:70–5.
Black KI, Stephens C, Haber PS, Lintzeris N. Unplanned pregnancy and contraceptive use in women attending drug treatment services. Aust New Zeal J Obstet Gynaecol. 2012;52:146–50.
Lotke PS. Increasing use of long-acting reversible contraception to decrease unplanned pregnancy. Obstet Gynecol Clin. 2015;42:557–67.
Matteson KA, Peipert JF, Allsworth J, Phipps MG, Redding CA. Unplanned pregnancy: does past experience influence the use of a contraceptive method? Obstet Gynecol. 2006;107:121–7.
Kawuki J, Gatasi G, Sserwanja Q, Mukunya D, Musaba MW. Utilisation of modern contraceptives by sexually active adolescent girls in Rwanda: a nationwide cross-sectional study. BMC Womens Health. 2022;22:1–10.
Sserwanja Q, Musaba MW, Mukunya D. Prevalence and factors associated with modern contraceptives utilization among female adolescents in Uganda. BMC Womens Health. 2021;21:1–7.
Ali MM, Cleland JG, Shah IH, Organization WH. Causes and consequences of contraceptive discontinuation: evidence from 60 demographic and health surveys. 2012.
Safari W, Urassa M, Mtenga B, Changalucha J, Beard J, Church K, et al. Contraceptive use and discontinuation among women in rural North-West Tanzania. Contracept Reprod Med. 2019;4:1–10.
Littlejohn KE. Hormonal contraceptive use and discontinuation because of dissatisfaction: differences by race and education. Demography. 2012;49:1433–52.
Moreau C, Bouyer J, Bajos N, Rodríguez G, Trussell J. Frequency of discontinuation of contraceptive use: results from a French population-based cohort. Hum Reprod. 2009;24:1387–92.
Black KI, Gupta S, Rassi A, Kubba A. Why do women experience untimed pregnancies? A review of contraceptive failure rates. Best Pract Res Clin Obstet Gynaecol. 2010;24:443–55.
Polis CB, Bradley SEK, Bankole A, Onda T, Croft T, Singh S. Contraceptive Failure Rates in the Developing World: An Analysis of Demographic and Health Survey Data in 43 Countries. Contraception. 2016;94: 11–17. Available: https://linkinghub.elsevier.com/retrieve/pii/S0010782416001037.
Yazdkhasti M, Pourreza A, Pirak A, Abdi F. Unintended pregnancy and its adverse social and economic consequences on health system: a narrative review article. Iran J Public Health. 2015;44:12.
Gipson JD, Koenig MA, Hindin MJ. The effects of unintended pregnancy on infant, child, and parental health: a review of the literature. Stud Fam Plann. 2008;39:18–38.
Polis C, Bradley SEK, Bankole A, Onda T, Croft TN, Singh S. Contraceptive failure rates in the developing world: an analysis of demographic and health survey data in 43 countries. 2016.
Statistics UB of, (Programme) ORCMM. Uganda Demographic and Health Survey, 2006. Uganda Bureau of Statistics; 2007.
Singh S, Prada E, Mirembe F, Kiggundu C. The incidence of induced abortion in Uganda. Int Fam Plan Perspect. 2005; 183–191.
Kaneda T, Bietsch K. World population data sheet. Washingt Popul Ref Bur. 2015.
Paul VK, Sachdev HS, Mavalankar D, Ramachandran P, Sankar MJ, Bhandari N, et al. Reproductive health, and child health and nutrition in India: meeting the challenge. Lancet. 2011;377:332–49.
Nalwadda G, Mirembe F, Byamugisha J, Faxelid E. Persistent high fertility in Uganda: young people recount obstacles and enabling factors to use of contraceptives. BMC Public Health. 2010;10:1–13.
Hyttel M, Rasanathan JJK, Tellier M, Taremwa W. Use of injectable hormonal contraceptives: diverging perspectives of women and men, service providers and policymakers in Uganda. Reprod Health Matters. 2012;20:148–57.
Anguzu R, Tweheyo R, Sekandi JN, Zalwango V, Muhumuza C, Tusiime S, et al. Knowledge and attitudes towards use of long acting reversible contraceptives among women of reproductive age in Lubaga division, Kampala district. Uganda BMC Res Notes. 2014;7:1–9.
Muhindo R, Okonya JN, Groves S, Chenault M. Predictors of Contraceptive Adherence among Women Seeking Family Planning Services at Reproductive Health Uganda. Mityana Branch Int J Popul Res. 2015;2015:1–8. https://doi.org/10.1155/2015/574329.
Sarnak DO, Wood SN, Zimmerman LA, Karp C, Makumbi F, Kibira SPS, et al. The role of partner influence in contraceptive adoption, discontinuation, and switching in a nationally representative cohort of Ugandan women. PLoS One. 2021;16:1–15. https://doi.org/10.1371/journal.pone.0238662.
Wasswa R, Kabagenyi A, Atuhaire L. Determinants of unintended pregnancies among currently married women in Uganda. J Heal Popul Nutr. 2020;39:1–17. https://doi.org/10.1186/s41043-020-00218-7.
Chang KT, Chakraborty NM, Kalamar AM, Hameed W, Bellows B, Grépin KA, et al. Measuring service quality and assessing its relationship to contraceptive discontinuation: A prospective cohort study in pakistan and uganda. Glob Heal Sci Pract. 2020;8:442–54. https://doi.org/10.9745/GHSP-D-20-00105.
Corsi DJ, Neuman M, Finlay JE, Subramanian SV. Demographic and health surveys: a profile. Int J Epidemiol. 2012;41:1602–13.
Ngerageze I, Mukeshimana M, Nkurunziza A, Bikorimana E, Uwishimye E, Mukamuhirwa D, et al. Knowledge and Utilization of Contraceptive Methods among Secondary School Female Adolescents in Rwamagana District. Rwanda Rwanda J Med Heal Sci. 2022;5:71–84.
Marrone G, Abdul-Rahman L, De Coninck Z, Johansson A. Predictors of contraceptive use among female adolescents in Ghana. Afr J Reprod Health. 2014;18:102–9.
Handebo S. Informed Choice of Contraceptive Methods among Women in Ethiopia: Further Analysis of the 2016 Ethiopian Demographic Health Survey. Open Access J Contracept. 2021;12:83.
Bradley SEK, Schwandt H, Khan S. Levels, trends, and reasons for contraceptive discontinuation. DHS Anal Stud. 2009;20:29–47.
Samosir OB, Kiting AS, Aninditya F. Role of information and communication technology and women’s empowerment in contraceptive discontinuation in Indonesia. J Prev Med Public Heal. 2020;53:117.
Festin MPR, Kiarie J, Solo J, Spieler J, Malarcher S, Van Look PFA, et al. Moving towards the goals of FP2020—classifying contraceptives. Contraception. 2016;94:289–94.
Ajayi AI, Adeniyi OV, Akpan W. Use of traditional and modern contraceptives among childbearing women: findings from a mixed methods study in two southwestern Nigerian states. BMC Public Health. 2018;18:1–9.
Marquez MP, Kabamalan MM, Laguna E. Traditional and modern contraceptive method use in the Philippines: trends and determinants 2003–2013. Stud Fam Plann. 2018;49:95–113.
Westhoff CL, Heartwell S, Edwards S, Zieman M, Stuart G, Cwiak C, et al. Oral contraceptive discontinuation: do side effects matter? Am J Obstet Gynecol. 2007;196:412-e1.
Pradhan MR, Patel SK, Saraf AA. Informed choice in modern contraceptive method use: pattern and predictors among young women in India. J Biosoc Sci. 2020;52:846–59.
Hilger DJ, Raviele KM, Hilgers TA. Hormonal contraception and the informed consent. Linacre Q. 2018;85:375–84.
Alemayehu M, Belachew T, Tilahun T. Factors associated with utilization of long acting and permanent contraceptive methods among married women of reproductive age in Mekelle town, Tigray region, north Ethiopia. BMC Pregnancy Childbirth. 2012;12:1–9.
Azmoude E, Behnam H, Barati-Far S, Aradmehr M. Factors affecting the use of long-acting and permanent contraceptive methods among married women of reproductive age in East of Iran. Women’s Heal Bull. 2017;4:1–8.
Allen RH, Cwiak CA, Kaunitz AM. Contraception in women over 40 years of age. CMAJ. 2013;185:565–73.
Lun CN, Aung T, Mya KS. Utilization of modern contraceptive methods and its determinants among youth in Myanmar: Analysis of Myanmar Demographic and Health Survey (2015–2016). PLoS ONE. 2021;16:e0258142.
Tin KN, Maung TM, Win T. Factors that affect the discontinuation of family planning methods in Myanmar: analysis of the 2015–16 Myanmar Demographic and Health Survey. Contracept Reprod Med. 2020;5:1–11.
Curtis S, Evens E, Sambisa W. Contraceptive discontinuation and unintended pregnancy: an imperfect relationship. Int Perspect Sex Reprod Health. 2011;37:58.
Zimmerman LA, Sarnak DO, Karp C, Wood SN, Ahmed S, Makumbi F, et al. Association between experience of specific side-effects and contraceptive switching and discontinuation in Uganda: results from a longitudinal study. Reprod Health. 2021;18:1–12. https://doi.org/10.1186/s12978-021-01287-5.
Rosenberg MJ, Waugh MS. Oral contraceptive discontinuation: a prospective evaluation of frequency and reasons. Am J Obstet Gynecol. 1998;179:577–82.
Acknowledgements
We thank the Demographic and Health Survey (DHS) program for granting us access to the DHS datasets used in this study
Funding
The authors did not receive any funding for this work.
Author information
Authors and Affiliations
Contributions
DBA and RKK conceived the study. DBA and RKK requested data from the DHS program website, performed statistical analysis, interpretation of data and spearheaded the writing of the manuscript. RKK and DBA discussed the relevant results. DBA, RKK, SK, FB and CGO contributed to the writing of the manuscript, read, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for the Demographic and Health Surveys is obtained from relevant research ethical approval committees and research regulatory bodies before data collection. We obtained permission to use the DHS survey datasets from the DHS program website. No personally identifiable information is available in the used datasets.
Competing interests
The authors declare that they do not have any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kisuza, R.K., Kicaber, S., Abila, D.B. et al. Prevalence of discontinuation of contraceptives due to failure among women aged 14 to 49 years in Uganda: a nation wide cross-sectional survey. Contracept Reprod Med 8, 12 (2023). https://doi.org/10.1186/s40834-022-00210-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40834-022-00210-y