
Abstract
Background
Diabetes mellitus is the third most prevalent chronic metabolic disorder and a significant contributor to disability and impaired quality of life globally. Diabetes self-management coaching is an emerging empowerment strategy for individuals with type 2 diabetes, enabling them to achieve their health and wellness goals. The current study aims to determine the feasibility of a diabetes self-management coaching program and its preliminary effectiveness on the clinical and psychosocial outcomes in the Ethiopian primary healthcare context.
Methods
The study will employ a mixed-method feasibility randomized controlled trial design. Forty individuals with type 2 diabetes will be randomly allocated to treatment and control groups using block randomization. The primary feasibility outcomes include acceptability, eligibility, recruitment, and participant retention rates, which will be computed using descriptive analysis. The secondary outcomes are self-efficacy, self-care activity, quality of life, and glycated hemoglobin A1c. For normally distributed continuous variables, the mean difference within and between the groups will be determined by paired sample Student t-test and independent sample Student t-test, respectively. Non-parametric tests such as the Mann-Whitney U test, the Wilcoxon signed rank test, and the Friedman analysis of variance test will determine the median difference for variables that violated the normality assumption. A repeated measure analysis of variance will be considered to estimate the variance between the baseline, post-intervention, and post-follow-up measurements. A sample of 10 volunteers in the treatment group will participate in the qualitative interview to explore their experience with the diabetes self-management coaching program and overall feasibility. The study will follow a qualitative content analysis approach to analyze the qualitative data. Qualitative and quantitative findings will be integrated using a joint display technique.
Discussion
Evidence reveals diabetes self-management coaching programs effectively improve HbA1c, self-efficacy, self-care activity, and quality of life. This study will determine the feasibility of a future large-scale randomized controlled trial on diabetes self-management coaching. The study will also provide evidence on the preliminary outcomes and contribute to improving the diabetes self-management experience and quality of life of individuals with type 2 diabetes.
Trial registration
The trial was registered online at ClinicalTrials.gov on 12/04/2022 and received a unique registration number, NCT05336019, and the URL of the registry is https://beta.clinicaltrials.gov/study/NCT05336019.
Similar content being viewed by others

Introduction
Diabetes is one of the leading global causes of morbidity and mortality [1]. The prevalence of diabetes is increasing at alarming rates,according to the [2] International Diabetes Federation (IDF) report, more than half a billion people live with diabetes globally, and this number will increase to 783.2 million by 2045 [3]. Approximately 80% of individuals with diabetes live in low- and middle-income countries (LMIC) [4, 5] and Ethiopia is one of the four African countries with the highest population of adults with diabetes [6]. According to IDF IDF [2], the IDF reported the prevalence of diabetes in Ethiopia is 3.3%. A systematic review and meta-analysis study in 2021 found a 6.5% pooled prevalence of diabetes in Ethiopia, ranging between 2% in the Tigray region and 14% in Dire Dawa [7]. Ethiopia does not have evidence-based national diabetes guidelines or standard referral criteria for diabetes management [8]. As a result, individuals with diabetes may receive substandard care. Notably, a systematic review and meta-analysis study revealed more than half of individuals with type 2 diabetes have poor self-care practices [9]. Furthermore, many people with type 2 diabetes in Ethiopia visit traditional healers and religious therapies like holy water to get a cure for diabetes mellitus [10] which makes self-management challenging.
An earlier cross-sectional study conducted in Addis Ababa, the capital of Ethiopia, showed that 87% of diabetic patients had regular clinical follow-up; however, 75% of participants required hospital admissions and did not receive diabetic education, and 95% of patients failed to monitor their blood glucose regularly [11]. A recent population-based cross-sectional study from Addis Ababa found that three-fourths of individuals with type 2 diabetes have glycated hemoglobin A1c (HbA1c) > 7.0% [12], indicating ongoing poor diabetes self-management. Furthermore, another hospital-based cross-sectional study in Southern Ethiopia revealed that 50% of individuals with diabetes suffered from one or more chronic complications: of these, 35%, 25%, and 15% acquire neuropathy, retinopathy, and nephropathy, respectively [13].
Although self-management is often used interchangeably with self-regulation, self-care, patient education, and patient counseling, it is beyond merely providing information and increasing awareness [14]. Self-management is recognized as tertiary prevention aiming to prevent the deterioration of health among individuals with chronic illness [14]. Self-management programs enable individuals to be active, responsible, informed, and autonomous in managing chronic illness’s physical, social, and emotional impact through collaboration with family, friends, and the healthcare provider(s) [15].
In recent years, Diabetes Self-Management (DSM) coaching, also called diabetes health coaching, has demonstrated a substantial effect on improving health [16]. The DSM coaching is a client-centered empowerment approach that enables individuals to self-manage diabetes (Radwan, [17]. It focuses on individual preferences, experiences, and values and engages participants in decision-making [18]. Studies in Taiwan, Indonesia, and Canada found that diabetes health coaching interventions can significantly improve HbA1c [19,20,21]. Systematic review and meta-analysis studies also demonstrate diabetes health coaching is an effective strategy to improve HbA1c [16, 17, 22, 23]. In addition, evidence suggests diabetes health coaching can lead to improvements in self-efficacy [24], self-care practice [19, 20], and quality of life [22, 25]. Despite the above evidence, culturally appropriate and effective DSM programs are lacking in most LMICs (Iregbu & Iregbu, [26], including Ethiopia.
In Ethiopia, an effective, patient-centered empowerment strategy to enhance diabetes self-management, build self-efficacy, improve quality of life, and control blood glucose is lacking, notably in the primary care setting. The DSM coaching program, which shows promising health outcomes in different settings, could be a practical approach in the primary care context of Ethiopia. Hence, the study will adapt a DSM coaching program from an evidence-based health coaching intervention [20] informed by an I-change model [27]. The study’s overarching goal is to determine the feasibility of implementing the DSM coaching program among individuals with type 2 diabetes in the primary care setting of Ethiopia and assess the program’s preliminary effectiveness in improving behavioral and clinical outcomes.
Methods and materials of the study
Primary objective
To determine the feasibility and acceptability of implementing an adapted DSM coaching program for individuals with type 2 diabetes in Ethiopia’s primary care settings.
Secondary objective
To evaluate the potential effectiveness of the DSM coaching program on self-care activity, self-efficacy, quality of life, and HbA1c among individuals with type 2 diabetes.
Phases of study
The study will have three phases: adaptation, implementation, and evaluation of the DSM coaching program.
Phase I: Adaptation of the DSM coaching intervention
This study will adapt an evidence-based intervention informed by the I-change model [20]. A purposively selected panel of experts will be invited to participate in adapting the DSM coaching program through the recommendation of selected departments. The Principal Investigator (PI) will ask the selected professionals to participate in the intervention adaptation process through a formal letter. A panel of multidisciplinary teams consisting of ten professionals and a patient representative will sit together to discuss and adapt the DSM coaching program and fidelity assessment tool at three-panel discussions.
The adaptation team will include one nurse, one internist (senior specialist doctor), two nurse researchers, two occupational therapists, two public health nutritionists, one physiotherapist, one epidemiologist (chronic disease researcher), and a patient representative.
The adaptation process will be iterative and will take 4 months. Panel members will review the candidate intervention manual before the panel discussion. The first panel discussion will focus on collecting feedback on the intervention component, reviewing each intervention component, and selecting potential intervention components for the DSM coaching program. A nominal group technique will be used to reach a consensus among panelists [28]. Accordingly, panelists will discuss thoroughly each intervention component based on the merits and demerits of incorporating it into the manual. Panel members will vote on the inclusion or exclusion of the intervention component and justify their decision. A consensus will be reached by a majority vote and supported by justification. The second panel discussion will emphasize revising selected intervention components and delivery methods. Two individuals with type 2 diabetes will participate in the adaptation process. During the third panel discussion, the panel members will review the draft DSM coaching intervention manual and approve the document. Furthermore, the adaptation process will use expert opinion and rating feedback to identify potential intervention components and delivery methods. The research team will prepare the content of the DSM coaching intervention manual by reviewing the literature and feedback from experts and the target population.
Phase II: Feasibility RCT
Study design
A convergent mixed-methods, single-blind feasibility randomized controlled trial (RCT) will be employed to assess the feasibility of the DSM coaching program. The study will adhere to the SPIRIT guideline for pilot and feasibility randomized trials [29]. The trial was registered online at ClinicalTrials.gov on 12/04/2022, and registration number NCT05336019 was received.
Study setting
The study will be conducted in the primary care settings of Gondar City, Amhara region, Ethiopia. Gondar City is about 740 km away from Addis Ababa, the capital of Ethiopia [30]. Christianity is the dominant religion, followed by Islam. The most common staple diet in Ethiopia is Injera, made up of teff flour after a consecutive date of fermentation. Almost all Ethiopians eat Injera with a stew of lentils or meat at least once daily [31]. People consume organic food items due to limited access to processed food items. Fasting is a common practice during Lent and Ramadan,hence, the study period will exclude these seasons. Gondar City has one referral hospital, nine primary care centers, and additional private health facilities.
According to unpublished Gondar City Health District reports, more than 10,000 individuals attend regular diabetes clinics in Gondar City health facilities. Individuals with diabetes received diabetes care at the referral hospital, private clinics, and primary care health centers. The hospital serves more than 2600 diabetes patients in the chronic disease clinic, and around 1312 patients have type 2 diabetes [32]. The hospital is a point of referral for newly diagnosed individuals with diabetes from health centers, individuals with complicated diabetes, and individuals with uncontrolled diabetes. Because of the absence of a district or a zonal hospital in the city, the city’s health system is inconsistent with the national referral system. As a result, the hospital provides primary, secondary, and tertiary care for individuals with diabetes. Most individuals with uncontrolled diabetes bypass the health centers and get care at the hospital. In addition, health centers also refer uncontrolled diabetes cases to the hospital. As a result, the study subjects will be recruited from the hospital. The research assistant will take informed consent from volunteers with type 2 diabetes who fulfill the screening criteria. Once the recruitment and baseline assessment are completed, the intervention will be administered in the selected health centers.
Participant eligibility
Inclusion criteria
The study includes individuals who have been attending the diabetes clinic for at least 6 months, are living in Gondar City, are taking anti-diabetic medications, have a recent HbA1c ≥ 7% (within 3 months), and are between 18 and 65 years old.
Exclusion criteria
The study will exclude individuals with clinically confirmed mental illness, pregnancy [33], and cardio-vascular diabetes complications (neuropathy, nephropathy, retinopathy, stroke, gangrene, cancer, and cardiovascular disease). Individuals who are seriously ill and hospitalized during screening will also be excluded. Furthermore, as the DSM coaching program demands participants be physically active, individuals with physical impairment (visual deficit, hearing deficit) and lower extremity amputation or palsy will be excluded.
Sample size determination
A formal sample size calculation will not be applied for a feasibility RCT study [34]. Hertzog [35] suggests that a sample size of 10–40 participants per group is enough for feasibility studies (Hertzog, [35]. Hence, considering the study’s pilot nature, the intervention’s high intensity, and the limited research fund, we will recruit 40 participants. Twenty participants will be allocated to each arm of the study with a 1:1 ratio.
Participant recruitment procedure
A 3-min audio record that briefly explains the purpose of the study and the recruitment process will be prepared in Amharic and played in the waiting area of the chronic disease clinic during working hours. In addition, a 1.5 m × 2 m poster describing the study objectives and the recruitment process will be prepared in Amharic and displayed in the waiting area. Nurses in the chronic disease clinic will receive a half-day training about the study, the screening material, and how to connect eligible individuals with the research assistant. Nurses working in the clinic will screen all individuals with type 2 diabetes and connect them with the research assistant. The research assistant will meet eligible individuals in a separate office in the clinic to discuss the study participation, information sheet, and informed consent.
Randomization, allocation, and blinding
Participants will be assigned to the treatment and control groups using a block randomization technique with a block size of four [36]. An external researcher with no other role in the study will manually generate the random allocation sequence [37]. From a block of four, six possible combinations using treatment “T” and control “C” will be generated (TTCC, TCTC, TCCT, CCTT, CTTC, and CTCT). A nurse working outside the chronic disease clinic will draw the lottery 10 times from these six potential combinations to allocate 40 participants. The external researcher will document the sequence drawn by the nurse and prepare 40 opaque sealed envelopes to conceal the group allocation [37, 38]. The research assistant will receive the prepared envelopes, randomly allocate participants by opening the envelope in front of the participant, and inform participants of their allocation. All participants will be registered in the master linkage log sheet and informed of the next meeting date.
Blinding
Because of the nature of the intervention, it is impossible to mask study participants and the interventionist. However, the study assessors will be masked to the group allocation. To prevent accidental disclosure by study participants, the research assistant will provide a 5-min orientation for each participant just before each data collection period. To ensure the blinding of the assessors, three data collectors who are academic staff at the University of Gondar will be recruited for each assessment time (T1, T2, and T3). One data collector will be assigned for each phase and will not have contact with the study data and participants.
Intervention arms of the study
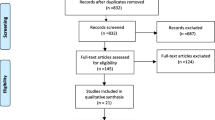
The study will have two arms: the treatment group will receive the DSM coaching program, and the control group will continue receiving the usual care (see Fig. 1).

Study participant flow diagram based on the CONSORT guideline [29]. Key: T1, T2, T3 represent time of assessment, n number
Treatment group: The treatment group will attend a 12-week DSM coaching program culturally adapted from the I-change model [27], an evidence-based health coaching intervention [20]. The DSM coaching program will have six interactive group sessions, including an overview of diabetes, goal setting, dietary management, exercise, blood glucose monitoring and medication, and foot care. In addition, the DSM coaching will also include four individual home-based coaching sessions. Furthermore, a family member who is a direct care provider will have a 10-min orientation after every individual home-based coaching session with the participants.
The principal investigator, who has completed a coaching and counseling course at Queen’s University, Kingston, Canada, will facilitate the DSM coaching sessions. The coach will deliver six 2-h group coaching sessions every 2 weeks for 3 months. The coach will use interactive discussions, experience sharing, demonstration, and home-take assignments to address the program goals. The intervention group will also continue receiving the usual care in the clinic (see Additional file 1: the DSM coaching program).
Control group
The control group will continue receiving the usual care in the chronic disease clinic. The usual care is biweekly or monthly clinical appointments, depending on the severity of the illness. Services provided during these clinical visits include history taking, physical examination, laboratory investigation, and medication refills. The available treatments for type 2 diabetes may include oral hypoglycemic agents such as metformin, glipizide, and nateglinide, and injectable insulin. Depending on the severity of the illness and the blood glucose level, doctors may prescribe an oral hypoglycemic agent, insulin, or a combination of both.
Outcome measures
Primary outcomes
Feasibility outcomes
The current study will address the eligibility rate, recruitment rate, retention rates, adherence rate, and the acceptability of the DSM coaching program. The progression criteria will determine the success of the DSM coaching program (Table 1).
Eligibility rate
The eligibility rate is the proportion of individuals who fulfill inclusion criteria among those screened. It will be calculated as Eligibility rate = (NE/NS) × 100, where NE is the number of eligible participants, and NS is the number of participants screened.
Recruitment rate
The recruitment rate is the proportion of people enrolled (randomized) in the program. It will be computed as Recruitment rate = (NR/NE) × 100, where NR is the number of randomized participants, and NE is the number of eligible participants.
Retention rate
The retention rate is the proportion of participants who complete the intervention. The retention rates can be computed as Retention rate = (NA/NR) × 100, where NA is the number of participants assessed at T3, and NR is the number of randomized participants.
Adherence rate
The adherence rate is the proportion of participants who attended 80% of the DSM coaching (group + individual) sessions. Adherence rate will be calculated as Adherence rate = (NA/NP) × 100, where NA is the number of participants who attended 80% of the sessions, and NP is the total number of participants.
Acceptability
Acceptability determines how well the target population receives a program and how it meets the needs of the target population [39]. Acceptability of the DSM coaching program will be assessed using the Treatment Acceptability/Adherence Scale (TAAS) [40]. The TAAS is a 10-item Likert scale with a value ranging between 1 and 7.
Fidelity of the DSM coaching program
The fidelity of the DSM coaching program will be assessed using the Comprehensive Intervention Fidelity Guide (CIFG) designed by Gearing. The CIFG is a guide with four core elements: design, training, delivery, and receipt fidelity proposed to examine an overall intervention fidelity [41]. The DSM Coaching Fidelity Measure (DSMC-FM) will assess the fidelity of the DSM coaching sessions. The DSMC-FM is informed by the Occupational Performance Coaching-Fidelity Measure (OPC-FM) [42]. The DSMC-FM has 23 items, of which 16 are critical components that focus on the coach’s behavior and practices. Four items address the client’s responses and behavior,the rest (3 are distinguished items needing improvement. An occupational therapist will review the recordings of the DSM coaching individual sessions and assess the fidelity of the coaching sessions.
Secondary outcomes
The secondary outcomes of the study encompass self-efficacy, self-care activity, quality of life, and HbA1c. These outcomes will be assessed at baseline (T1), post-intervention (T2), and post-follow-up period (T3) (Table 2).
-
A. Self-care activity
The diabetes self-care activity is the ability of an individual with type 2 diabetes to follow a healthy eating plan, perform regular exercise, monitor blood glucose, perform foot care, adhere to diabetes medication/s, and cease cigarette smoking [43]. Self-care activity will be measured using the Summary of Diabetes Self-Care Activity tool (SDSCA) [43]. The tool will be culturally translated and validated for face and content validity by a panel of experts.
-
B. Self-efficacy
Self-efficacy is an individual’s belief and confidence in their ability to perform intended activities that affect their life and control over how these activities are experienced [44, 45]. Self-efficacy will be measured using the Stanford Self-Management Resource Center (SMRC) diabetes self-efficacy scale, which has an eight-item Likert Scale [46]. The tool will be translated into the local language, Amharic, and undergo content validation by a panel of experts.
-
C. Quality of life
As defined by the WHO, quality of life is an individual’s perception of their position in life in the context of the culture and value systems in which they live and their goals, expectations, standards, and concerns [47]. The quality of life of individuals with type 2 diabetes will be assessed by a valid and reliable WHOQOL-BREF tool [48]. The tool has demonstrated reliability and construct validity [48]. The WHOQOL-BREF tool has 26 items addressing the physical, psychological, social, and environmental health domains with five ordinal scales [48].
-
D. Glycated hemoglobin A1C
HbA1C is a reliable measure of long-term glucose monitoring recommended by the WHO and the American Diabetes Association (ADA) [49]. HbA1c < 7% is considered good glycemic control, and HbA1c equal to or greater than 7% will be regarded as an uncontrolled glucose level [50].
Data collection
Data on participants’ demographic, behavioral, and clinical characteristics will be collected through interviews and reviewing patient medical records. Clinical characteristics such as HbA1c and blood pressure will be retrieved using a chart review form. The weight and height of participants will be measured during their clinical visit to compute body mass index.
Data on self-care activities, self-efficacy, and quality-of-life will be collected using an interviewer-administered data collection technique at baseline (T1), at the end of the intervention (T2), and at the end of the follow-up period (T3). All three data collection periods will be scheduled at least 2 weeks after the holidays as the dietary practice during holidays affects study outcomes. Three MSc nurse data collectors will receive a 1-day training on questionnaire administration procedures, the study instruments, study blinding, and ethical issues related to data collection. Each data collector will work only once to keep the data collectors masked about group allocation. Additionally, all study participants will attend a 5-min orientation to ensure they do not disclose their group to the data collector during the interview. Data related to the quantitative feasibility outcomes: eligibility, recruitment, adherence, and retention rate, will be collected from the recruitment documents, session attendance sheets, and assessment reports throughout the study process. The TAAS assessment will be carried out along with post-follow-up data collection. However, only the treatment group participants will be asked about the program’s acceptability.
Study participant retention
Retaining adequate study participants is challenging for many interventional studies involving human subjects. Studies suggest different strategies to increase the retention rate [51, 52]. One of the strategies to retain participants in this study is building effective relationships and treating participants respectfully and compassionately. Hence, the research assistants and data collectors will demonstrate respect and compassion for the study participants. A close follow-up throughout the study period will be the other mechanism to ensure participant retention. The research assistant will closely follow participants through regular attendance and make reminder calls before each session. The research assistant, principal investigator, and participants will discuss and arrange meeting schedules for the group coaching and individual home-based coaching sessions. Participant transport costs will be covered to encourage their participation. In addition, with tangible evidence, any cost incurred by the participant for the purpose of the study will be refunded. The group session will be designed to create active participation through discussion, role play, and demonstration, which will make the sessions attractive and enhance participation.
Data analysis and management
An independent statistician will enter, code, and clean the data using Epi-Info version 7.3.2. The data will be imported to SPSS version 29 for analysis. The principal investigator will analyze the data in consultation with statisticians and the research team. An intention-to-treat (ITT) analysis technique will be followed to analyze the quantitative data [53]. An ITT analysis will run data of all participants irrespective of their adherence to the program [54], and missing values will be filled using multiple imputation techniques [55]. Baseline differences between the treatment and control groups will be examined using t-tests. Frequencies, percentages, mean, median, standard deviation, and interquartile range will be computed to describe the population. A p-value < 0.05% with a 95% confidence level will be used to determine statistical significance.
Differences in the effect size of the secondary outcomes of the study will be computed following a test of assumptions. For normally distributed continuous outcomes, the mean difference within and between the groups will be determined by paired sample Student t-test and independent sample Student t-test, respectively. Non-parametric tests such as the Mann–Whitney U test, Wilcoxon signed rank test, and Friedman analysis of variance test will be computed to determine the median difference for variables that violate the normality assumption. A repeated measure analysis of variance will be considered to estimate the variance between the baseline, post-intervention, and post-follow-up measurements. If a difference is detected between the two groups, a covariate analysis approach or multivariate analysis technique will be considered to rule out the effect of covariates using the pretest score and age of the participant as the covariate.
Phase III: Qualitative study
Study design
A qualitative description [56] approach will be followed to examine the acceptability of the DSM coaching program. This approach allows the researcher to explore participants’ perspectives and understand the barriers and facilitators of a given phenomenon [56, 57]. Hence, the study will explore the acceptability of the DSM coaching program, including the participants’ perspectives on the program, the challenges, and the enablers of implementing the program in the primary care context.
Sampling procedure and sample size
A purposive sampling method with a maximum variation technique [58] will be used to include participants of different genders, duration of diabetes, educational status, and program adherence level. The study will recruit ten individuals with type 2 diabetes who participated in the DSM coaching program.
Recruitment of participants
At the end of the group DSM coaching session, the principal investigator and the research assistant will invite eligible participants to participate in the in-depth interview.
Data collection
An experienced qualitative researcher will conduct the interviews. Study participants will sign an informed consent form and have the option to decide on the recording of the interview before the start of the session. A semi-structured interview question addressing the acceptability of the DSM coaching program will be prepared in Amharic to explore the experience of individuals with the DSM coaching program. Interviews will be audio-recorded, transcribed verbatim by a transcriber, and translated into English for analysis.
Qualitative data analysis and management
Data will be analyzed using qualitative content analysis [56]. An experienced transcriber will transcribe all the interview records in Amharic. Two of these transcripts will be translated into English by a professional translator and used by the research team to prepare a codebook. The data analysis will follow a three-step inductive content analysis approach: preparation, organization, and reporting of the analysis process [59]. The preparation phase includes selecting the unit of analysis and making sense of the data. The organization phase includes open coding, grouping codes, categorizing, and abstraction. The third step is reporting the findings using a model or conceptual system. NVivo software version 14 will be used to code, categorize, and recategorize the qualitative data [60].
Data integration
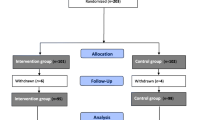
The qualitative and quantitative findings will be integrated at the resulting level [61] and interpreted to answer the feasibility research questions. Data will be presented in a joint display technique to interpret findings (Fig. 2).

A flow diagram showing the mixed-method data integration process of the DSM coaching program
Discussion
Self-management strategies rely on individuals’ preferences, build on prior knowledge, recognize contextual factors, and encourage active engagement in chronic illness care [62]. Establishing collaboration between patients, health care providers, family members, and the community at the primary care level is a means for successful self-management of chronic illness [63]. Diabetes self-management in the primary care of Ethiopia is problematic due to poor linkage within the health systems, poor quality of services, and lack of public awareness. Individuals with diabetes may live with the illness for many years and are supposed to manage a significant portion of the self-care activities such as diet, exercise, medication, foot care, and blood glucose monitoring by themselves [63].
In resource-limited settings where community support programs and linkage are lacking, primary care agencies need to think of alternative schemes to address the self-management needs of individuals with diabetes. The practice of self-management strategies like goal setting in the primary care settings is challenged by patient readiness, skill, and attitude, provider’s attitude and skill, and lack of time [64]. Diabetes self-management coaching has shown significant improvement in self-efficacy, self-care behavior, quality of life, and clinical parameters among individuals with type 2 diabetes in developed countries. However, one of the challenges in adapting and tailoring a complex health intervention in resource-limited countries is the program’s acceptability and implementation feasibility. Hence, the current study will explore the acceptability of the DSM coaching program. Furthermore, the study will evaluate the preliminary effectiveness of the DSM coaching program on self-efficacy, self-care activity, quality of life, and HbA1c. Evidence generated from this feasibility/pilot study will be used to design and implement a definitive RCT among individuals with type 2 diabetes.
Strengths and limitations of the study
The study will introduce a culturally adapted and contextually tailored DSM coaching program through an iterative process supported by a supervisory committee and a panel of multidisciplinary experts. In addition, the study will be the first to introduce coaching as an intervention in the Ethiopian primary care context; hence, it will be a foundation for future definitive trials in the area. Furthermore, the preliminary outcomes of the study will be used to design DSM coaching programs in the context of low-income countries. Due to the nature of the study, the trial implementor, research assistant, and study participants will not be blinded regarding group allocation. The short follow-up period of the study might make it challenging to make a meaningful conclusion on the long-term behavioral outcomes. Furthermore, the lack of adequate information about the amount, type, and effect of processed diets on diabetes management and the effect of religious and cultural practices on diabetes management limits our ability to characterize the study population.
Availability of data and materials
All required data will be available upon request; please contact the principal investigator.
Abbreviations
- ADA:
-
American Diabetes Association
- ANOVA:
-
Analysis of Variance
- CIFG:
-
Comprehensive Intervention Fidelity Guide
- DSM:
-
Diabetes Self-Management
- DSMC-FM:
-
Diabetes Self-Management Coaching Fidelity Measure
- HbA1c:
-
Glycated Hemoglobin A1c
- IDF:
-
International Diabetes Federation
- ITT:
-
Intention to Treat
- LMIC:
-
Low- and Middle- Income Countries
- WHO:
-
World Health Organization
- OPC-FM:
-
Occupational Performance Coaching-Fidelity Measure
- RCT:
-
Randomized Controlled Trial
- SDSCA:
-
Summary of Diabetes Self-Care Activity
- SMRC:
-
Stanford Self-Management Resource Center
- SPIRIT:
-
Standard Protocol Item: Recommendations for Interventional Trials
- SPSS:
-
Statistical Package for the Social Sciences
- TAAS:
-
Treatment Acceptability/Adherence Scale
- UGCSH:
-
University of Gondar Comprehensive Specialized Hospital
- WHO:
-
World Health Organization
- WHO-QoL:
-
World Health Organization-Quality of life
References
Raghupathi W, Raghupathi V. An empirical study of chronic diseases in the United States: a visual analytics approach. Int J Environ Res Public Health. 2018;15(3):431. https://doi.org/10.3390/ijerph15030431.
IDF. (2021). International Diabetes Federations Diabetes Atlas (10th_Edition) [Annual report]. https://diabetesatlas.org/.
Ogurtsova K, Guariguata L, Barengo N, Ruiz P, Sacre J, Karuranga S, Sun H, Boyko E, Magliano D. IDF diabetes Atlas: Global estimates of undiagnosed diabetes in adults for 2021. Diabetes research and clinical practice. 2021. https://doi.org/10.1016/j.diabres.2021.109118.
Cho N, Shaw J, Karuranga S, Huang Y, da Rocha Fernandes J, Ohlrogge A, Malanda B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–81. https://doi.org/10.1016/j.diabres.2018.02.023.
Werfalli, M., Raubenheimer, P., Engel, M., Peer, N., Kalula, S., Kengne, A., & Levitt, N. (2015). Effectiveness of community-based peer-led diabetes self-management programmes (COMP-DSMP) for improving clinical outcomes and quality of life of adults with diabetes in primary care settings in low and middle-income countries (LMIC): a systematic review and meta-analysis. BMJ Open,5(7). https://doi.org/10.1136/bmjopen-2015-007635.
Abebe N, Kebede T, Addise D. Diabetes in Ethiopia 2000–2016 prevalence and related acute and chronic complications; a systematic review. African Journal of Diabetes Medicine. 2017;25(2):7–12.
Zeru M, Tesfa E, Mitiku A, Seyoum A, Bokoro T. Prevalence and risk factors of type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Scientific Reports. 2021;11(1):21733–21733. https://doi.org/10.1038/s41598-021-01256-9.
Desse TA, Mc Namara K, Yifter H, Manias E. Current practices and future preferences of type 2 diabetes care in Ethiopia: A qualitative study on the perspectives of patients, health professionals, and policymakers. Diabetes Metab Syndr: Clin Res Rev. 2022;16(8):102585. https://doi.org/10.1016/j.dsx.2022.102585.
Yehualashet F, Tegegne E, Ayele A, Takele W. Do adult patients with diabetes mellitus living in rural part of Ethiopia and having poor social support have disproportionately poor self-care practice? A systematic review and meta-analysis. Prim Care Diabetes. 2021;15(4):642–52. https://doi.org/10.1016/j.pcd.2021.02.010.
Diriba C, Leung D, Suen L. A nurse-led, community-based self management program for people living with type 2 diabetes in Western Ethiopia: A feasibility and pilot study protocol. Diabet Med. 2021;38(8): e14587. https://doi.org/10.1111/dme.14587.
Feleke Y, Enqueselassie F. An assessment of the health care system for diabetes in Addis Ababa. Ethiopia Ethiopian Journal of Health Development. 2006;19(3):203–10. https://doi.org/10.4314/ejhd.v19i3.9999.
Abera R, Demesse E, Boko W. Evaluation of glycemic control and related factors among outpatients with type 2 diabetes at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: a cross-sectional study. BMC Endocrine Disorders. 2022;22(1):1–11. https://doi.org/10.1186/s12902-022-00974-z.
Nigatu T. Epidemiology, complications and management of diabetes in Ethiopia: a systematic review. J Diabetes. 2012;4(2):174–80. https://doi.org/10.1111/j.1753-0407.2011.00181.x.
Grady P, Gough L. Self-management: a comprehensive approach to management of chronic conditions. American journal of public health. 2014;104(8):e25-31. https://doi.org/10.2105/ajph.2014.302041.
Van de Velde D, De Zutter F, Satink T, Costa U, Janquart S, Senn D, De Vriendt P. Delineating the concept of self-management in chronic conditions: a concept analysis. BMJ Open. 2019;9(7): e027775. https://doi.org/10.1136/bmjopen-2018-027775.
Pirbaglou M, Katz J, Motamed M, Pludwinski S, Walker K, Ritvo P. Personal health coaching as a type 2 diabetes mellitus self-management strategy: a systematic review and meta-analysis of randomized controlled trials. Am J Health Promot. 2018;32(7):1613–26. https://doi.org/10.1177/0890117118758234.
Radwan, N. (2019). Effectiveness of health coaching on diabetic patients: a systematic review and meta-analysis. Traditional Medicine Research,4(6), 314. https://doi.org/10.12032/TMR20191024143
Jutterström L, Hörnsten Å, Sandström H, Stenlund H, Isaksson U. Nurse-led patient-centered self-management support improves HbA1c in patients with type 2 diabetes—a randomized study. Patient Educ Couns. 2016;99(11):1821–9. https://doi.org/10.1016/j.pec.2016.06.016.
Chen, R., Huang, L., Su, C., Chang, Y., Chu, C., Chang, C., & Lin, C. (2019). Effectiveness of short-term health coaching on diabetes control and self-management efficacy: a quasi-experimental trial [https://doi.org/10.3389/fpubh.2019.00314]. Frontiers in Public Health, 7, 314. https://doi.org/10.3389/fpubh.2019.00314.
Pamungkas R, Chamroonsawasdi K. Self-management based coaching program to improve diabetes mellitus self-management practice and metabolic markers among uncontrolled type 2 diabetes mellitus in Indonesia: a quasi-experimental study. Diabetes Metab Syndr. 2020;14(1):53–61. https://doi.org/10.1016/j.dsx.2019.12.002.
Wayne N, Perez D, Kaplan D, Ritvo P. Health coaching reduces HbA1c in type 2 diabetic patients from a lower-socioeconomic status community: a randomized controlled trial. J Med Internet Res. 2015;17(10): e224. https://doi.org/10.2196/jmir.4871.
Kim M, Kim K, Huh B, Nguyen T, Han H, Bone L, Levine D. The effect of a community-based self-help intervention: Korean Americans with type 2 diabetes. Am J Prev Med. 2015;49(5):726–37. https://doi.org/10.1016/j.amepre.2015.04.033.
Sherifali D, Viscardi V, Bai J, Ali R. Evaluating the effect of a diabetes health coach in individuals with type 2 diabetes. Can J Diabetes. 2016;40(1):84–94. https://doi.org/10.1016/j.jcjd.2015.10.006.
Campos B, Kieffer E, Sinco B, Palmisano G, Spencer M, Piatt G. Effectiveness of a community health worker-led diabetes intervention among older and younger Latino participants: results from a randomized controlled trial. Geriatrics (Basel, Switzerland). 2018;3(3):47. https://doi.org/10.3390/geriatrics3030047.
Sherifali D, Brozic A, Agema P, Punthakee Z, McInnes N, O’Reilly D, Usman Ali RM, Ibrahim S, Gerstein HC. Effect of diabetes health coaching on glycemic control and quality of life in adults living with type 2 diabetes: a community-based, randomized, controlled trial. Can J Diabetes. 2021;45(7):594–600. https://doi.org/10.1016/j.jcjd.2020.11.012.
Iregbu, S., & Iregbu, F. (2016). A review of self-management of diabetes in Africa. Afri J Diabetes Med, 24(2). https://www.openaccessjournals.com/articles/AJDM-613%20(Iregbu).pdf.
Iraola, B., Sánchez, Á., Hors-Fraile, S., Petsani, D., Timoleon, M., Díaz-Orueta, U., Carroll, J., Hopper, L., Epelde, G., Kerexeta, J., Bamidis, P., & Konstantinidis, E. (2021). User centered virtual coaching for older adults at home using SMART goal plans and I-change model. Int J Environ Res Public Health, 18(13). https://doi.org/10.3390/ijerph18136868.
Harvey N, Holmes CA. Nominal group technique: an effective method for obtaining group consensus. Int J Nurs Pract. 2012;18(2):188–94. https://doi.org/10.1111/j.1440-172X.2012.02017.x.
Eldridge S, Chan C, Campbell M, Bond C, Hopewell S, Thabane L, Lancaster G. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355: i5239. https://doi.org/10.1136/bmj.i5239.
Yalew, A., Terefe, B., Alem, M., & Enawgaw, B. (2016). Hematological reference intervals determination in adults at Gondar university hospital, Northwest Ethiopia. BMC research notes,9, 1-9. https://doi.org/10.1186/s13104-016-2288-8.
Neela S, Fanta SW. Injera (An ethnic, traditional staple food of Ethiopia): a review on traditional practice to scientific developments. Journal of Ethnic Foods. 2020;7(1):32.
Amdie F, Luctkar M, Snelgrove E, Sawhney M, Alemu S, Woo K. Feasibility of virtual simulation-based diabetes foot care education in patients with diabetes in Ethiopia: protocol for a randomized controlled trial. Diabetes, Metabolic Syndrome and Obesity. 2022;15:995–1009. https://doi.org/10.2147/dmso.S345722.
Radin M. Pitfalls in hemoglobin A1c measurement: when results may be misleading. J Gen Intern Medi. 2014;29(2):388–94. https://doi.org/10.1007/s11606-013-2595-x.
Billingham S, Whitehead A, Julious S. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC medical research methodology. 2013;13:104–104. https://doi.org/10.1186/1471-2288-13-104.
Hertzog M. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31(2):180–91. https://doi.org/10.1002/nur.20247.
Efird J. Blocked randomization with randomly selected block sizes. Int J Environ Res Public Health. 2011;8(1):15–20. https://doi.org/10.3390/ijerph8010015.
Doig G, Simpson F. Randomization and allocation concealment: a practical guide for researchers. Journal of Critical Care. 2005;20(2):187–91. https://doi.org/10.1016/j.jcrc.2005.04.005.
Spieth P, Kubasch A, Penzlin A, Illigens B, Barlinn K, Siepmann T. Randomized controlled trials - a matter of design. Neuropsychiatric disease and treatment. 2016;12:1341–9. https://doi.org/10.2147/NDT.S101938.
Ayala, G., & Elder, J. (2011). Qualitative methods to ensure acceptability of behavioral and social interventions to the target population. J Public Health Dent, 71 Suppl 1(0 1), S69-79. https://doi.org/10.1111/j.1752-7325.2011.00241.x.
Milosevic I, Levy H, Alcolado G, Radomsky A. The treatment acceptability/adherence scale: moving beyond the assessment of treatment effectiveness. Cogn Behav Ther. 2015;44(6):456–69. https://doi.org/10.1080/16506073.2015.1053407.
Gearing R, El-Bassel N, Ghesquiere A, Baldwin S, Gillies J, Ngeow E. Major ingredients of fidelity: a review and scientific guide to improving quality of intervention research implementation. Clin Psychol Rev. 2011;31(1):79–88. https://doi.org/10.1016/j.cpr.2010.09.007.
Kennedy B, Ziviani J. Occupational performance coaching (OPC): a manual for practitioners and researchers. Routledge; 2021.
Toobert D, Hampson S, Glasgow R. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–50. https://doi.org/10.2337/diacare.23.7.943.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. https://doi.org/10.1037//0033-295x.84.2.191.
Saghaee A, Ghahari S, Nasli-Esfahani E, Sharifi F, Alizadeh-Khoei M, Rezaee M. Evaluation of the effectiveness of Persian diabetes self-management education in older adults with type 2 diabetes at a diabetes outpatient clinic in Tehran: a pilot randomized control trial. J Diabetes Metab Disord. 2020;19(2):1491–504. https://doi.org/10.1007/s40200-020-00684-0.
Hailu F, Moen A, Hjortdahl P. Diabetes self-management education (DSME) - effect on knowledge, self-care behavior, and self-efficacy among type 2 diabetes patients in Ethiopia: a controlled clinical trial. Diabetes Metab Syndr Obes. 2019;12:2489–99. https://doi.org/10.2147/dmso.S223123.
WHO. (1998). Programme on mental health: WHOQOL user manual. https://apps.who.int/iris/handle/10665/77932.
Reba K, Birhane B, Gutema H. Validity and reliability of the Amharic version of the World Health Organization’s Quality of Life Questionnaire (WHOQOL-BREF) in patients with diagnosed type 2 diabetes in Felege Hiwot Referral Hospital. Ethiopia Journal of Diabetes Research. 2019;2019:3513159. https://doi.org/10.1155/2019/3513159.
Fonseca V, Inzucchi S, Ferrannini E. Redefining the diagnosis of diabetes using glycated hemoglobin. Diabetes Care. 2009;32(7):1344–5. https://doi.org/10.2337/dc09-9034.
ADA. Glycemic targets: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S66-s76. https://doi.org/10.2337/dc20-S006.
Brueton V, Tierney J, Stenning S, Meredith S, Harding S, Nazareth I, Rait G. Strategies to improve retention in randomised trials: a Cochrane systematic review and meta-analysis. BMJ Open. 2014;4(2): e003821. https://doi.org/10.1136/bmjopen-2013-003821.
Catherine N, Lever R, Marcellus L, Tallon C, Sheehan D, MacMillan H, Gonzalez A, Jack SM, Waddell C. Retaining participants in community-based health research: a case example on standardized planning and reporting. Trials. 2020;21(1):393. https://doi.org/10.1186/s13063-020-04328-9.
Montori, V., & Guyatt, G. (2001). Intention-to-treat principle. Canadian Medical Association Journal, 165(10), 1339-1341. https://pubmed.ncbi.nlm.nih.gov/11760981.
Hollis S, Campbell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ. 1999;319(7211):670. https://doi.org/10.1136/bmj.319.7211.670.
Jakobsen J, Gluud C, Wetterslev J, Winkel P. When and how should multiple imputation be used for handling missing data in randomised clinical trials – a practical guide with flowcharts. BMC medical research methodology. 2017;17(1):162. https://doi.org/10.1186/s12874-017-0442-1.
Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–40. https://doi.org/10.1002/1098-240x(200008)23:4%3c334::aid-nur9%3e3.0.co;2-g.
Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Global qualitative nursing research. 2017;4:1–8. https://doi.org/10.1177/2333393617742282.
Suri H. Purposeful sampling in qualitative research synthesis. Qualitative Research Journal. 2011;11(2):63–75.
Elo S, Kyngäs H. The qualitative content analysis process. Journal of Advanced Nursing. 2008;62(1):107–15. https://doi.org/10.1111/j.1365-2648.2007.04569.x.
Zamawe F. The implication of using NVivo software in qualitative data analysis: evidence-based reflections. Malawi medical journal : the journal of Medical Association of Malawi. 2015;27(1):13–5. https://doi.org/10.4314/mmj.v27i1.4.
Creswell, J., & Creswell, D. (2018). Research design : qualitative, quantitative, and mixed methods approaches (Fifth ed.).
Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj S. Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PloS one. 2019;14(8): e0220116. https://doi.org/10.1371/journal.pone.0220116.
Bodenheimer T, Wagner E, Grumbach K. Improving primary care for patients with chronic illness. Jama. 2002;288(14):1775–9. https://doi.org/10.1001/jama.288.14.1775.
Lenzen S, Van Dongen J, Daniëls R, Van Bokhoven M, Van der Weijden T, Beurskens A. What does it take to set goals for self-management in primary care? A qualitative study Fam Pract. 2016;33(6):698–703. https://doi.org/10.1093/fampra/cmw054.
Acknowledgements
I want to express my deepest gratitude to my supervisor, Dr. Catherine Donnelly, and the supervisory committee, Dr. Dorothy Kessler and Dr. Segenet Bizunehi, for their support, encouragement, mentorship, and valuable comments throughout the proposal development process. I would also like to take this opportunity to thank Queen’s University School of Rehabilitation Therapy, the University of Gondar, and the Master Card Foundation for providing me with the opportunity to join this doctoral program and exercise research in the local context of Ethiopia. My heartfelt appreciation goes to PC lab members and friends who provided comments, suggestions, and encouragement.
Funding
The Mastercard Foundation Scholars’ program and Queen’s University will fund the study. The funding organizations are responsible for providing technical support, monitoring the successful completion of the project, and ensuring the incorporation of the organization’s name in the study’s publications. Besides this, they have no role in the study’s design, collection, analysis, and write-up. They have no conflict of interest in the study.
Author information
Authors and Affiliations
Contributions
FAY and CD participated in the conception, writing the method section, protocol writing, and reviewing the draft protocol. DK and SB participated in reviewing the manuscript. The advisory team, which incorporates the supervisor, CD, and the supervisory committee DK and SB, will supervise the study and monitor the intervention development, implementation, data collection process, analysis, and write-up.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical process of the study was reviewed and approved by the Queen’s University Health Sciences Research Ethics Board in Kingston, Canada, and the Institutional Review Board of the University of Gondar, Ethiopia. The study will adhere to the principles and policies of Queen’s University and the University of Gondar. Necessary amendments to the protocol will be communicated to the Ethics board. All study participants will sign a written consent form to participate in the intervention and for data collection interview. Participants will be informed about their rights and responsibilities during the study time. The study findings will be communicated with the local community, the target population, the Queen’s University, the University of Gondar, and the Ethiopia Federal Ministry of Health and published in peer-reviewed open-accessed journals to reach the international scholarly community.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: The DSM coaching program.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yehualashet, F.A., Kessler, D., Bizuneh, S. et al. Feasibility of diabetes self-management coaching program for individuals with type 2 diabetes in the Ethiopian primary care setting: a protocol for a feasibility mixed-methods parallel-group randomized controlled trial. Pilot Feasibility Stud 10, 59 (2024). https://doi.org/10.1186/s40814-024-01487-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40814-024-01487-3