
Abstract
Background
Exercise intensities are prescribed using specific intensity zones (moderate, heavy, and severe) determined by a ‘lower’ and a ‘higher’ threshold. Typically, ventilatory (VT) or blood lactate thresholds (LT), and critical power/speed concepts (CP/CS) are used. Various heart rate variability-derived thresholds (HRVTs) using different HRV indices may constitute applicable alternatives, but a systematic review of the proximity of HRVTs to established threshold concepts is lacking.
Objective
This systematic review aims to provide an overview of studies that determined HRVTs during endurance exercise in healthy adults in comparison with a reference VT and/or LT concept.
Methods
A systematic literature search for studies determining HRVTs in healthy individuals during endurance exercise and comparing them with VTs or LTs was conducted in Scopus, PubMed and Web of Science (until January 2022). Studies claiming to describe similar physiological boundaries to delineate moderate from heavy (HRVTlow vs. VTlow and/or LTlow), and heavy from severe intensity zone (HRVThigh vs. VThigh and/or LThigh) were grouped and their results synthesized.
Results
Twenty-seven included studies (461 participants) showed a mean difference in relative HR between HRVTlow and VTlow of − 0.6%bpm in weighted means and 0.02%bpm between HRVTlow and LTlow. Bias between HR at HRVTlow and VTlow was 1 bpm (limits of agreement (LoA): − 10.9 to 12.8 bpm) and 2.7 bpm (LoA: − 20.4 to 25.8 bpm) between HRVTlow and LTlow. Mean difference in HR between HRVThigh and VThigh was 0.3%bpm in weighted means and 2.9%bpm between HRVThigh and LThigh while bias between HR at HRVThigh and VThigh was − 4 bpm (LoA: − 17.9 to 9.9 bpm) and 2.5 bpm (LoA: − 12.1 to 17.1 bpm) between HRVThigh and LThigh.
Conclusion
HRVTlow seems to be a promising approach for the determination of a ‘lower’ threshold comparable to VTlow and potentially for HRVThigh compared to VThigh, although the latter needs further empirical evaluation. LoA for both intensity zone boundaries indicates bias of HRVTs on an individual level. Taken together, HRVTs can be a promising alternative for prescribing exercise intensity in healthy, male athletes undertaking endurance activities but due to the heterogeneity of study design, threshold concepts, standardization, and lack of female participants, further research is necessary to draw more robust and nuanced conclusions.
Similar content being viewed by others

Key points
-
The present systematic review is the first one that systematically compares methods of intensity zone determination derived from heart rate variability (HRVTlow/HRVThigh) with more traditional concepts derived from ventilatory measurements (VTlow/VThigh) and blood lactate concentration (LTlow/LThigh).
-
The findings of our data synthesis reveal that HRVTs for healthy, male adults participating in endurance-type activities show in general a high overall correlation but a very heterogeneous level of agreement with established VTs and/or LTs as the agreement strongly varies with the chosen reference method and/or HRVT approach.
-
HRVTlow seems a promising approach for the determination of a ‘lower’ threshold comparable to VTlow that could be used to demarcate the boundary between moderate and heavy exercise intensity. This may also be the case for HRVThigh compared to VThigh to denote the boundary between the heavy and severe exercise domain but needs further evaluation. Limits of agreement denote potential bias on an individual level.
-
HRVT validation studies used very heterogeneous methodologies, which limit the comparability of results. Evidence for female athletes is scarce, and for some HRVT-approaches not available at all. Thus, more high-quality research in this direction is urgently needed.
Background
The training intensity distribution framework divides exercise intensity into predetermined zones and plays a crucial role in training monitoring for both performance enhancement and health preservation of individuals performing endurance exercise [1, 2]. In general, these exercise intensity zones are discrete domains defined by internal (e.g., ventilatory/metabolic/cardiorespiratory/perceptive) and/or external (e.g., power/speed) load indices that aim to demarcate exercise-induced homeostatic perturbations and delineate a gradual transition from steady-state to non-steady-state organismic functioning [3, 4]. Within the exercise intensity distribution model of endurance sports, at least three zones are typically used [1, 5, 6]. These zones are traditionally inferred from “threshold-like” approaches in accordance with physiologic boundaries of internal load measures such as blood lactate concentration and/or ventilatory/gas exchange values [5, 7,8,9].
Exercise Intensity Zones: ‘Traditional’ Concepts in Science and Practice
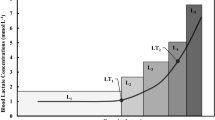
Zone 1 typically represents a moderate exercise intensity which induces a plateau in VO2 with blood lactate concentrations close to baseline that are indicative of predominantly oxidative re-phosphorylation of ATP. Zone 2 characterizes the heavy intensity zone in which a ‘slow component’ and a delayed steady state of VO2, as well as a rise in blood lactate above baseline that stabilizes over time are present, while zone 3 corresponds to a severe exercise intensity with the ‘VO2-slow component’ that drives towards VO2max in accordance with the continuous and substantial increase in blood lactate that exceeds lactate clearance capabilities [1, 5, 8, 9]. Traditional approaches to the determination of exercise intensity zones use physiological thresholds that are based on blood lactate [4, 9, 10] and ventilatory measurements [7]. Within this context, a large body of threshold concepts evolved and has been the subject of a vibrant scientific debate for more than 50 years [4, 8]. From a practical point of view, a ‘first (lower)’ and a ‘second (higher) threshold’ are typically used to differentiate between the three exercise intensity domains [4, 11] and provide the opportunity to determine the amount of time spent within a specific zone (i.e., training intensity distribution) [6, 12]. In this context, the most frequently applied threshold concepts in training practice demarcate zones 1 and 2 based on the first lactate threshold (LT1), the gas exchange threshold (GET) and/or a (first) ventilatory threshold (VT1/VT) [1, 5, 6, 9]. In addition, zones 2 and 3 are commonly determined by the respiratory compensation point (RCP), the maximal lactate steady state (MLSS) or a second lactate threshold (LT2) as a proxy for MLSS [1, 5, 9]. However, given the fact that there is a large heterogeneity of (i) testing protocols (e.g., slope, stage duration and increment of graded exercise or ramp tests) and (ii) determination methods (e.g., linear vs. nonlinear regression models, amount of data points used, fixed or variable threshold concepts), as well as (iii) a plethora of definitions and names of thresholds (e.g., blood lactate: LT/LT1, LT2, (individual) anaerobic threshold, MLSS; ventilatory: VT/VT1/GET, VT2/RCP), a general confusion within the scientific and practical debate on threshold concepts in exercise science is still present [8]. Most recent views on exercise intensity prescription point towards the primary use of LT/GET (and VT) for the demarcation of the boundary of moderate to heavy exercise intensity domain, while the separation of heavy and severe exercise intensity might be best determined using the critical power/speed (CP/CS) concept [4, 8, 10, 13, 14]. The latter concept of CP/CS uses the hyperbolic power/speed–duration relationship to define exercise tolerance for endurance exercise and likely represents the threshold above which there is a continuous obligatory glycolytic contribution with substantial net lactate accumulation making it well-situated to differentiate between heavy and severe exercise intensity [8, 14,15,16]. However, besides the ongoing debate on ‘traditional’ threshold concepts, the ‘results-proven training practice’ still uses a large variety of VT and/or LT concepts to yield training intensity distribution boundaries [6, 17]. Additionally, threshold concepts based on, e.g., concentration changes of deoxygenated hemoglobin and myoglobin determined by muscle oximetry [18], as well as on heart rate (HR) [19, 20] and HR variability (HRV) [21,22,23], have been developed and evaluated in numerous method comparison studies.
Heart Rate Variability Thresholds (HRVT): Perspectives for Exercise Intensity Prescription
In this context, especially HRV thresholds (HRVT) have shown promise as an applicable and economical way to determine exercise intensity zones [23, 24], because HRV can be tracked noninvasively and continuously in real time by relatively inexpensive and miniaturized wearable devices (e.g., chest belt connected with a smartwatch or smartphone application) [25, 26]. Generally, changes in HRV with increasing exercise intensity mirror the complex interplay between parasympathetic withdrawal, concomitant rise in sympathetic activity, and other related (non-neural) factors [21, 27,28,29]. Therefore, comparable to traditional threshold concepts, HRVTs aim to capture fundamental ‘tipping points’ of complex neuro-autonomic regulation processes by using specific time, frequency/time–frequency and/or nonlinear HRV-metrics to determine a first, rather lower (HRVTlow) and a second, higher (HRVThigh) threshold that, in turn, allow differentiation of moderate from heavy and heavy from severe exercise intensity, respectively [30]. Specifically, HRVTlow methods are mainly characterized by the rapid reduction of HRV indices from rest to moderate exercise intensity with a subsequent minimum or plateau around 50–60% of maximal oxygen uptake [23]. This transitional process can be captured by several linear HRV parameters in time and frequency domain. In particular, indices reflecting parasympathetic activity such as the root mean square of successive differences (RMSSD), standard deviation one of Poincaré Plot analysis (SD1) or high-frequency power (HF, typically 0.15–0.4 Hz) of spectral analysis may be suitable indices [23, 31,32,33]. Hence, different methodological approaches including several time and frequency-based analysis methods were developed to identify HRVTlow that corresponds to traditional approaches of blood lactate (LTlow) and/or ventilatory/gas exchange thresholds (VTlow) [23, 34, 35]. From a physiological perspective, the strong reduction of time and frequency indices of HRV during moderate exercise with a minimum or plateau around 50–60% of maximal oxygen uptake [23] seems to appear just before the onset of blood lactate accumulation and an increase in minute ventilation due to a corresponding excess of CO2 [23, 35, 36], which suggests a common involvement of higher cardiovascular and metabolic control systems [37]. Moreover, these findings imply that direct physiological links between feed-forward mechanisms from higher brain centers and feedback mechanisms from muscle mechanoreceptors exist that drive, on the one hand, initial vagal withdrawal as well as an initial reduction in cardiac sympathetic neural activity due to loading of the cardiopulmonary baroreceptors [38] and, on the other hand, metabolic/ventilatory changes defining the transition from moderate to heavy exercise intensity.
With a further increase in exercise intensity, a second threshold-like behavior of HRV (HRVThigh) has been observed by time–frequency analysis and displays an abrupt re-increase in high-frequency power (HF), peak frequency of HF (HFpeak) or a product of both when plotted against work rate [21, 22, 36]. This physiological observation seems to be directly related to the disproportional rise in breathing frequency once the exercise intensity corresponds to a second ventilatory ‘tipping point’ (VThigh)—in particular, when the boundary of heavy-to-severe exercise is exceeded [36]. Theoretically, the observed re-rise in indices of (time-) frequency analysis is probably driven by a complex physiological interplay of mechanisms of vagal withdrawal and sympathetic activation that are related to (i) muscle mechano- and/or metaboreceptors and an increased central command, (ii) a concomitant increase of the mechanical influence of venous return on the stretch of the sinus node caused by elevated breathing frequency and/or volume and muscle pump as well as a cardio-respiratory-locomotor coupling, and (iii) the increase of circulating catecholamines [36, 38, 39]. Regarding the frequency content of HRV during non-stationary exercise conditions, it is noteworthy that traditional spectral methods like the fast Fourier transform (FFT) or autoregressive modeling (AR) show conflicting results and thus may not be reliable approaches to determine a HRVThigh [28]. In this context, time–frequency methods such as short-time Fourier transformation [39] and smoothed pseudo-Wigner–Ville distribution [40] seem to be more promising approaches as these methods may properly track instantaneous changes in the HRV frequency content. In addition, an extension of the HF-band up to maximum breathing frequency or 1–2 Hz seems necessary when heavy to severe exercise intensities are involved because in this particular case the breathing frequency typically exceeds the upper HF-boundary (0.4 Hz) of resting conditions to a considerable extent [28, 30]. In addition to spectral approaches to HRVThigh, the aforementioned re-increase of HRV fluctuations has also been reported for Poincaré Plot analysis using the standard deviation two (SD2) [41, 42], which displays the dispersion of points along the line-of-identity of the plot and indicates the level of long-term variability in the HRV signal. However, regarding all HRVT approaches that are based on time and (time-)frequency domain it has to be considered that the magnitudes of all linear HRV markers above intensities of 50–60% of maximal oxygen uptake are low to very low and therefore strongly reduce signal-to-noise ratio, which may influence both the validity and reliability of HRVT assessment [30].
In addition to linear HRV time- and frequency-domain analysis, recent exercise studies have used methods of nonlinear dynamics to further elucidate complex cardiovascular regulation and to overcome some of the drawbacks of linear HRV analysis [43,44,45]. Among these methods, detrended fluctuation analysis (DFA) [46], recurrence quantification analysis (RQA) [47], sample entropy (SampEn), and compression entropy (CEn) [45, 48, 49] have been used for HRVT detection. These nonlinear methods have strong origins in signal theory and evaluate complex dynamics, regularity, and self-similarity of the HRV signal and display corresponding interrelations of underlying physiological regulation processes, rather than quantify HRV signal amplitude and frequency content [43, 49, 50]. In this regard, recent studies demonstrated that these methods are promising to demarcate exercise intensity transitions by identifying breakpoints and/or saturation behavior of HR dynamics [24, 51,52,53,54]. In particular, the short-term scaling exponent alpha1 of DFA (DFAa1) exhibits a broad dynamic range from moderate to severe exercise intensities [43, 55] and has a great potential for HRVT detection using fixed DFAa1 values of 0.75 and 0.5 that show moderate-to-high correlations with VTlow/LTlow and VThigh/LThigh [24, 51, 56], respectively. From a signal theory perspective, DFAa1 approaches to HRVT track the intensity-dependent loss of HRV correlation properties from the trade-off point between fractional Brownian motion and fractional Gaussian noise (1.0) occurring at moderate intensities over a half-way loss of correlation properties (0.75) that coincides with the transition to heavy exercise, towards uncorrelated/stochastic (0.5) or anti-correlated (< 0.5) HR dynamics at severe intensities [49, 55, 57,58,59,60]. From a physiological point of view, these changes in correlation properties are possibly caused by changes in the coupling strength and interaction of higher-order regulatory processes in the central autonomic network [37] that integrate the antagonistic interaction of vagal withdrawal and sympathetic activation [30, 43, 49], intracardiac biochemical changes and/or coupling mechanisms of different other cardiorespiratory and metabolic pathways [57], and feedback from muscle mechano-/-metaboreceptors [38]. Thus, changes in correlation properties of HR dynamics could be a promising tool for displaying the regulation quality of common cardiovascular and metabolic control systems [43].
Taken together, several linear and nonlinear HRVT methods using time, (time)–frequency and nonlinear domain measures have been utilized to demarcate exercise intensity zones based on the complex interplay of vagal withdrawal, increased sympathetic activity and other non-neural factors. In this regard, numerous studies investigated whether HRVTs are comparable to traditional threshold concepts based on VT and LT measurements that denote the transition from moderate to heavy (VTlow/LTlow) and heavy to severe (LThigh/VThigh) exercise, respectively. However, the current state of the literature in this research field has not been systematically evaluated. A lack of a systematic analysis of the available evidence on the capability of HRVT concepts to reflect commonly used threshold approaches can impede progress in both research and the practical application of HRVT concepts. Therefore, the aim of this review is to provide a systematic overview of all studies that determined HRVTs in healthy adults during endurance exercise and compared HRVTs to most common concepts using blood lactate- and/or ventilatory-derived thresholds. As far as possible, recommendations for specific settings will be given, which may help assist sports practitioners and scientists when using HRVT approaches to performance testing or prescription of exercise intensity zones.
Methods
Search Strategy
The systematic review was conceptualized and carried out in July–September 2021 (with the last update conducted in January 2022) according to the guidelines for the Preferred Reporting Items for systematic Reviews and Meta-Analyses (PRISMA) [61] and registered at Open Science Framework (OSF) (https://osf.io/z63wv/). The electronic databases searched included Scopus, PubMed and Web of Science (with no restriction concerning publication date), and the following search string was used: (HRV OR heart rate variability OR autonomic nervous system) AND (threshold OR zone) AND (endurance OR exercise OR running OR cycling). This search string allows to find studies involving various endurance-type exercise modalities.
Inclusion and Exclusion Criteria
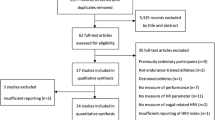
This systematic review aims to identify and group all scientific studies that assessed HRVT exercise zone boundaries and compared HRVTs with threshold concepts derived from ventilatory (VT) and/or blood lactate (LT) measurements. To identify eligible studies, we followed the PICOS-principle (“PICOS” stands for participants (P), intervention (I), comparisons (C), outcomes (O), and study design (S)) [62, 63]. Accordingly, we included all studies that met the following criteria: (P) only studies dealing with healthy adults (> 18 years) regardless of age or performance level are considered as relevant, (I) we applied all endurance-type cyclic movements (e.g., running, cycling, cross-country skiing, swimming) during an incremental or graded exercise test concerning the intervention, (C) all considered studies needed to compare HRV-derived thresholds (HRVTlow and/or HRVThigh) with commonly used threshold approaches using ventilatory (VTlow and/or VThigh) or/and blood lactate (LTlow and/or LThigh) parameters, (O) we considered all studies as relevant that assessed time domain, (time-)frequency domain and/or nonlinear domain HRV metrics, and (S) no specific restrictions in study design were applied. In addition to the PICOS principle, our search was limited to original articles published in peer-reviewed journals and written in English. References being cited by the retrieved articles were also examined for potential relevance. Conference abstracts, dissertations, theses, and other non-peer-reviewed articles were excluded. Figure 1 illustrates the screening and selection process employed.

Flow chart of article selection process from article identification using a search string, over screening and eligibility testing to inclusion in the review. Number of studies is displayed as n
Study Selection
In the first step, all duplicates were removed by the first author (SK). In the second step, a title—and abstract—screening was performed by two independent reviewers (SK and TG) to identify eligible studies. Afterward, the full texts of remaining studies were screened by the same reviewers and 15 studies were excluded with reason (see Fig. 1 for a detailed overview). In a subsequent step, the reference lists of the relevant studies were searched for additional publications not having been identified during the electronic database search but meeting our inclusion criteria. In case of a disagreement between the two reviewers, a consensus was achieved by a discussion or input from a third author (OH). A flow chart illustrating the selection procedure is provided in Fig. 1.
Data Extraction and Synthesis
From the relevant articles, the following information was extracted and entered in an Excel sheet (Microsoft Corporation. (2018). Redmont, WA, Microsoft Excel. Retrieved from https://office.microsoft.com/excel) by the first author (SK) and confirmed by another author (FH): (i) details of publication (i.e., authors, year, journal, publication date), (ii) characteristics of the study population (i.e., age, sample size, sex), (iii) study design (i.e., design of the incremental/graded exercise test, type of exercise, description of HRV measurements (incl. preprocessing) and threshold determination, information about validation with other threshold concepts), and (iv) study results.
As a major outcome of the included studies the mean ± standard deviation of the HR at the respective threshold are reported. Based on these values, Cohen’s d was calculated to display an effect size as additional indicator of difference between means. Cohen’s d was calculated based on [64, 65]. In addition, bias as mean difference between HRVT and reference threshold (VT or LT) was extracted from Bland and Altman analyses [66], as well as lower and upper limits of agreement. If HR data are not provided in the main manuscript or in Additional file 1, running speed, power and/or oxygen uptake at the respective threshold are reported instead (reported parameters depend on the availability/reporting of data in the original study). Additionally, if available, correlation coefficients between performance indicators at each threshold were extracted. If a study experimented with different HRVT methods, the one with the best agreement was included in the synthesis.
Further, a synthesis was generated from the extracted data from the included studies. Firstly, weighted pooling of systematic error (bias) and standard deviation was conducted for HR and/or power/running speed at the specific thresholds, respectively. Since not all studies provided data on absolute reliability (i.e., Bland and Altman analyses), additionally weighted mean and standard deviations for HR, power and running speed at HRVTs and/or VTs, LTs were determined. This weighted mean is reported as difference in percent of the mean result of the reference test. Finally, a weighted Pearson correlation coefficient was calculated in the case that the original study reported correlation coefficients. Due to the large heterogeneity concerning data presentation in the included studies, we had to refrain from conducting further meta-analytical calculations. All statistical tests were deemed to be statistically significant at p ≤ 0.05 and are presented as mean ± standard deviation. Effect sizes were denoted by Cohen’s d (low: 0.2 < d < 0.5, moderate: 0.5 < d < 0.8, high: 0.8 < d [65]. The weighted Pearson correlation coefficients (r) were classified according to recommendations for reliability measures [67].
Assessment of Methodological Quality of Included Studies
The methodological quality of the included studies was assessed using the revised tool Quality Assessment of Diagnostic Accuracy Studies (QUADAS2) [68]. The risk of bias and applicability concerns for the review question were independently assessed by two authors (SK and OH). Due to the complexity of HRV methodology, we also rated the methodological quality by using a HRV-specific tool (Standard for Reporting Diagnostic Accuracy Studies (STARDHRV, Table 1 [69]), which is a modified version of the original STARD [70]. The methodological quality assessment by the means of STARDHRV was performed by two authors (SK and OH), and STARDHRV was slightly adapted in items 1, 9, 19 and 21, see Additional file 1: Table S1, to best fit the purpose of this systematic review. Any disagreement concerning the ratings of methodological quality was resolved by consensus or a discussion with a third author (TG).
Results
Literature Search
Initial search terms yielded 1206 potentially relevant articles of which 701 were screened after the removal of duplicates. Finally, 27 studies were included in the review process (Fig. 1).
Methodological Study Quality: QUADAS2
Details of the risk of bias assessment are provided in Fig. 2. Ten out of the 27 studies achieved a low risk of bias across all categories. Four studies are rated as suffering from high risk of bias in one out of the four domains and another eleven studies are rated as having “an unclear risk of bias” in two or more domains. The scoring outcomes are shown in detail in Fig. 2. All studies included in this systematic review used a within-subject design, but participant groups, reference and index tests varied considerably based upon the methodologies and parameters chosen for threshold determination.

Risk of bias and applicability of included studies as assessed by QUADAS2 [68]. Relative amount of low, high and unclear risk of bias among the included studies for the domains flow and timing, reference standard, index test and patient selection
Methodological Study Quality: STARDHRV
The 27 studies being included in this systematic review reached an average rating of 75 ± 7% using the adapted STARDHRV protocol. The highest rating achieved was 86% and the lowest 56%, while 8 studies reached ≥ 80%, 5 studies achieved ≤ 70%. While the items 1, 2, 3, 5, 7, 20 and 24 were fulfilled by all the studies, a sufficient description of the sample size determination (item 6) was only provided by one study (4%) and a stabilization period prior to the test was only addressed (item 11) in 26% of the studies. In a comparable manner, breathing rate was acknowledged (item 13) in 37% of the studies. All other items were fulfilled by 54–98% of the studies (see Additional file 1: Table S2).
Results of Individual Studies
The result presentation in the reviewed studies was highly heterogeneous. Table 1 provides a brief overview of the included studies and their primary results. From studies that used more than one method to determine HRVT, the data of the method with the closest proximity to or best agreement with the reference method are reported both in individual results and in the synthesis, respectively.
Results of Syntheses
In summary, 17 studies compared HRVTlow versus VTlow, 11 studies compared HRVThigh versus VThigh, six studies compared HRVTlow versus LTlow and five studies compared HRVThigh versus LThigh, respectively. Fourteen determined HRVTs based on frequency or time–frequency indices and 12 based on time-domain metrics. This includes studies that used differentapproaches/indices for HRVTlow and HRVThigh assessment. Furthermore, four studies used different nonlinear analyses for HRVT determination (Table 1).
As stated above, the result presentation in the original studies is heterogeneous, and thus, the included sample size for each part of the synthesis is reported. Weighted differences of means relative to the reference test mean of HR, power and/or speed at the lower and higher thresholds are reported in Tables 2 and 3, respectively. Further, Tables 4 and 5 show the agreement of HR, power and/or speed between VTlow and/or LTlow and HRVTlow, and between VThigh and/or LThigh and HRVThigh, respectively.
Concerning the comparison of VTlow and HRVTlow, which is based on pooled sample of 205 subjects from nine studies, we observed a mean correlation of r = 0.84 (CI 0.77–0.91) using HR in beats per minute. A correlation between HR at LTlow and HRVTlow including 59 subjects from three studies yielded r = 0.92 (CI 0.86–0.97). Using power in Watts for LTlow and HRVTlow including 31 subjects from two studies, the correlation coefficient was r = 0.87 (CI 0.86–0.87). With respect to VThigh compared to HRVThigh, a mean correlation of r = 0.79 (CI 0.76–0.83) was determined (i.e., based on a pooled sample of 93 subjects from four studies). Due to a lack of data in the original studies, no further pooled correlations could be determined; data from original studies can be found in Table 1.
Discussion
This systematic review aims to provide an overview on HRVTs and their interrelations and agreements with traditional concepts of ventilatory and blood lactate thresholds. Due to the large heterogeneity of the results from 27 reviewed studies, it was not possible to include all studies in every sub-analysis of our synthesis. Overall, HRVTlow and HRVThigh show a small systematic bias compared to VTlow and VThigh, respectively. However, the limits of agreement appear to be relatively wide, especially when HR, power, and speed at the higher thresholds are considered (see Tables 4, 5). The results from the few studies that included both the comparison of HRVTlow versus LTlow and HRVThigh versus LThigh show a small systematic bias for HR and power, and a moderate systematic bias for speed at the respective thresholds, but rather larger limits of agreement. Furthermore, HRVTs seem to better reflect VTs than LTs, but this likely depends on the LT methodology and the corresponding exercise protocol [4, 9] and will be discussed in more detail afterwards. All in all, the correlations and agreements of the different HRVTs with VTs and LTs are within the range of the values that have been reported for comparisons of the latter two approaches (i.e., VTs and LTs) [71,72,73,74] and in a recent review on the relative proximity of VTs and LTs to the CP/CS concept [75]. Furthermore, it should be noted that female athletes are highly underrepresented in all method comparison studies that consider HRVTs and VTs/LTs. Thus, we are not able to draw conclusions concerning female athletes which, in turn, necessitates further threshold comparison studies in this population.
Specification of Levels of Agreement Between HRV-Derived Thresholds and Ventilatory and/or Blood Lactate Thresholds
In general, the level of agreement of different exercise intensity thresholds that were mainly based on comparisons of HR, but also power, and speed at the respective thresholds is difficult to determine because the smallest worthwhile/meaningful change of exercise intensity in the respective intensity zone that will lead to a different training stimulus and/or have a different impact on recovery duration is ambiguous [76, 77]. For example, HR is likely to drift during any exercise bout with different amplitudes depending on exercise intensity and duration [78] and acute internal load responses to exercise are not always predictive of chronic adaptations [4]. Moreover, the markers for intensity prescription that were used in the reviewed studies (mainly HR, power, and speed) are relatively susceptible to be influenced by variability arising from different sources that may interact in complex ways. In this regard, day-to-day variability of HR has been shown to decrease with increasing exercise intensity and values vary for example in a range of 3.1–4.1% at lower running speeds and lie within 1.4–2.7% at higher running speeds, respectively [79]. In addition, the day-to-day variability in running economy is 1.77% for highly trained and 2.00% for moderately trained athletes (i.e., operationalized by the coefficients of variation [CV]) [80], and the gross efficiency of trained cyclists may vary by up to 10% (CV of 7.8–9.8% depending on exercise intensity [81]), which in both cases certainly alters the workload-HR/VO2 relation and therefore complicates the issue of variability of the common markers used for exercise intensity prescription. Moreover, these and other factors (e.g., temperature, oxygen partial pressure) can influence the actual physiological stimulus being triggered by a given exercise intensity [82, 83]. Thus, it seems reasonable to assume that the agreement of a certain HRVT and a corresponding reference threshold should be as good as possible and lie within the range of the basic physiological variation of the chosen exercise prescriptor (HR, VO2, speed/power), and/or the day-to-day variability in movement economy. In addition, it needs to be taken into account that in training practice of, e.g., well-trained athletes whose ‘lower’ and ‘higher’ thresholds occur at a high percentage of HRmax the corresponding HR-based exercise intensity zones may only comprise 4–8% of HRmax (i.e., 10 bpm for HRmax of 200 bpm) for heavy-to-severe domain and 10–12% of HRmax (24–20 bpm for HRmax of 200 bpm) for moderate domain, respectively [17, 84]. In this case, even a moderate level of inaccuracy (e.g., 3–5% HRmax), especially in ‘higher’ threshold determination, can/cannot induce a frequent training stimulus with a(n) (un)desirable continuous obligatory glycolytic contribution. Furthermore, a high accuracy of the ‘lower’ threshold is also desirable as endurance athletes (especially professional athletes) typically spend a very high training volume in the moderate-intensity domain [1, 12]. Considering these issues, the following sections will discuss correlations and agreement of the different HRVTs with LT and VT approaches for ‘lower’ and ‘higher’ thresholds separately as the different reference methods (VTs and LTs) by themselves may show subtle to substantial differences depending on the different methodological settings and the sport-specific context [4, 8, 75].
HRVTlow Versus VTlow
Seventeen studies compared HRVTlow against VTlow. Of these studies, eight used time–frequency metrics, eight time-domain metrics and one study used a nonlinear approach (DFA), while the reference methods used for VTlow were five times V-slope method, eight times based on VE/VO2 and three times a combination of both methods and one study used VE versus power. Our synthesis of these studies shows (i) a high mean correlation between HR at HRVTlow versus VTlow (r = 0.83), (ii) a small difference in weighted means, and (iii) a small bias for HR, speed and power at both thresholds, while the LoA for HR was moderately wide and acceptably wide for power and speed, respectively (see Table 4). However, when LoA for power in Watts is contextualized within the ranges of reliability measures of VTlow or LTlow, these values appear to be in the same range or are even narrower [72]. In addition, when the relative differences are used to gauge the agreement between HRVTlow and VTlow (CV of 2.0–3.5%) [71, 72], the difference between HRVTlow and VTlow may be negligible for practical applications. However, power and speed at HRVTlow seem to be slightly above those values from VTlow, while HR at HRVTlow seems to be slightly lower in the weighted mean comparison with a positive mean bias of below 1 bpm. Thus, our findings suggest that HRVTlow determination is accurate enough to set up exercise intensity zones regardless of the individual performance level [39] or training specialization [85, 86]. Moreover, HRVTlow is applicable to a variety of movement patterns such as cycling, running, walking or cross-country skiing techniques [36, 40, 86, 87]. A possible limitation of this HRVT approach may arise from movements in which the upper body activity is dominant or significantly involved in propulsion as such a movement behavior may lead to a high incidence of movement artefacts [88] and a ‘competing’ growing mechanical influence of respiratory sinus arrhythmia (RSA), muscle pump activity and cardio-locomotor coupling [33, 38, 89] that may hamper the accuracy of HRVTlow detection [86]. In this context, threshold determination based on HRV time–frequency methods might be advantageous, as the locomotor component may be separated from ventilatory activity using a specified very-high-frequency band above respiratory frequency, but our literature analysis indicated that this method has yet only been used to determine HRVThigh [89, 90]. However, despite the issue that excessive upper body movements can confound the determination of HRVTlow based on time domain metrics, no relevant systematic difference between HRVTlow determination based on time-domain or time–frequency-domain metrics has been observed. In addition, the only study that utilized a nonlinear analysis of HRVT by applying a time-varying DFA algorithm with a fixed threshold at DFAa1 = 0.75 [24], reported a small bias, acceptable limits of agreement, and a high correlation of HR and relative oxygen consumption between HRVTlow and VTlow.
In summary, exercise prescription based on HRVTlow denotes exercise intensities close to those from reference methods of VTlow over a variety of methodological settings, athletic performance levels, and endurance activities.
HRVTlow Versus LTlow
From the six studies that compared HRVTlow against LTlow four used time-domain based approaches [35, 41, 91, 92], one used a time–frequency approach [93], and one used a nonlinear methodology [56], while the reference methods used for LTlow utilized three times the first increase from baseline, as well as baseline plus 0.2 mmol/l blood lactate concentration, Dickhuth-method [94] and 2 mmol/l blood lactate concentration, once each. The agreement between running speed at HRVTlow and LTlow was assessed in two studies and showed a moderate bias but relatively wide LoA (see Table 4). Furthermore, two studies that used a SD1-based method from Poincaré Plot analysis of HRV reported high ICC values, minimal bias but very wide LoA (see Table 1), although not all participants appeared to be included in the Bland–Altman analysis of the corresponding studies [41, 92]. Moreover, agreement of power at HRVTlow and LTlow showed a minimal bias, which is further supported by a high correlation coefficient (r = 87) [91]. These findings are supported by minimal, small, and moderate differences in weighted relative means for HR, power and speed at HRVTlow and LTlow, respectively (see Table 3). However, LoA were moderate for power and relatively wide for HR and speed (see Table 5). A potential reason for wider LoA is the large heterogeneity in LTlow concepts that have been used in the reviewed studies. This idea is supported by the fact that these LTlow concepts are known to differ substantially from each other [4]. Therefore, HRVTlow could be a promising approach to estimate LTlow in cycling and running for many healthy participants, but it should be considered that the individual bias can be as high as − 20 to 26 bpm [35, 93]. Based on the low number of studies that used LTlow as a reference test and the large heterogeneity in LT assessment, we are not able to derive a recommendation concerning the issue which HRVTlow method shows the closest proximity to LTlow. In general, it should be noted that the determination of lactate thresholds strongly depends on the specific lactate threshold concept and the selected exercise protocol [4, 9]. Thus, our results from the cross-comparison of different studies using different LT reference methods warrant a cautious interpretation. Interestingly, two studies [35, 93] that compared the outcomes of HRVTlow against both LTlow and VTlow observed high to very high correlations, but the correlations between HRVTlow and VTlow were slightly higher than those between HRVTlow and LTlow. This observation might be related to the direct physiological connection between breathing mechanics, respiratory sinus arrhythmia (RSA), and HRVTlow [36, 39], while the connection with LTlow is moderated by the mechanism of isocapnic buffering [95] and is therefore less straightforward. The comparison of HRVTlow and VTlow as well as HRVTlow and LTlow were comparable in terms of bias and LoA (see Table 4). Further, in both studies [35, 93] the interrelations between HRVTlow and LTlow, HRVTlow and VTlow as well as the corresponding LoAs are in a comparable range to those between LTlow and VTlow [72].
Taken together, our findings suggest that HRVTlow has a promising potential to yield a prescription of exercise intensity that is comparable to those obtained from LTlow. However, the large individual differences that may occur because of the plethora of LTlow concepts that have been used as reference methods impedes a more robust and nuanced conclusion. The above-mentioned methodological issues and the fact that women were highly underrepresented in the reviewed method comparison studies necessitates further empirically research to substantiate the evidence concerning the proximity of HRVTlow and LTlow.
HRVThigh Versus VThigh
Our systematic review identified and included 11 studies that validated HRVThigh against VThigh. Of these studies, nine studies used time–frequency metrics [36, 39, 40, 85, 86, 89, 90, 96,97,98], one study used a time-domain metric [42] and one study utilized a nonlinear approach (DFA, [51]). To comapre HRVThigh to VThigh, VE/VCO2 was applied seven times, and two times by combining three methods, one time using VCO2 vs Workload and respiratory exchange ratio and one time using a web service (http://oxynetresearch.promfacility.eu) [51, 73, 99, 100]. The exercise modes in these studies include running and cycling, but also ski-mountaineering [89, 96], and cross-country skiing [86]. Furthermore, in one study a continuous 20 m shuttle-run protocol [101] was used in addition to a standard graded exercise test [98]. In general, agreement between HRVThigh and VThigh can be rated as good with moderate bias in HR, and a minimal systematic bias in power and speed. In addition, minimal differences in relative weighted means were observed. LoA were acceptable for HR and power, and small for speed (see Table 5). Only HR appears to be slightly lower at HRVThigh as compared to VThigh. The majority of studies used time–frequency methods to derive HRVThigh by determining the product of the pHF and HF plotted against exercise time. This index emphasizes the re-rise in HRV-outcome when VThigh, as operationalized by the second ventilatory threshold (VT2), is surpassed [36, 89]. Despite the high agreement between time–frequency based HRVThigh determination and VThigh in cycling and running, this method seems to be susceptible to artefacts arising from upper body movements. We noticed that, especially when the upper body was substantially involved in propulsion (e.g., cross-country skiing), the agreement between HRVThigh and VThigh was either notably lower than in other studies [86] or the detection of HRVThigh was even not possible in a considerable number of participants [96]. As mentioned earlier regarding the comparison of HRVTlow with VTlow, there is some evidence in the literature suggesting that in this specific application case advanced time-varying spectral analysis approaches (e.g., STFT, SPWVD) need to be considered to separate locomotor and respiratory frequency within the HF-band and a an extension of the HF-band of up to 2 Hz is required to be able to properly detect HRVThigh [89]. In addition to the time–frequency assessment of HRVThigh, one study [42] used a re-increase in RMSSD after the plateau that occurs around HRVTlow as a proxy for HRVThigh [42]. This time-domain based method reported a distinguishable HRVThigh for all participants under normoxic conditions and a high agreement between power at HRVThigh and VThigh, but relatively wide LoA (see Table 5. Despite these promising results, the small sample size, and the low signal-to-noise ratio in linear HRV-indices at high exercise intensities should be further evaluated to draw more robust conclusions for a practical implementation. Finally, a novel approach using nonlinear HRV-analysis in a recent study compared a fixed threshold value of DFAa1 = 0.5 as a proxy of HRVThigh with VThigh [51]. The results showed a slight systematic underestimation of HR at HRVThigh compared to VThigh (− 4 bpm) and relatively wide LoA (− 24 to 16 bpm), and a high correlation (r = 0.78) between HR at HRVThigh and VThigh.
Taken together, our results suggest that HRVThigh can be determined by three different approaches that yield mean values in HR, power, and speed that are comparable to and highly correlated with those obtained from VThigh approaches. However, agreement with the values obtained from VThigh is rather moderate with a more substantial individual bias as compared to the reviewed studies on method comparison studies for the ‘lower’ threshold. In addition, the methodological setting to determine heavy to severe exercise intensity seems to be more challenging for HRVT assessment, especially when upper body movement is involved [89]. Most importantly, one need to consider that recent reviews recommend the CP/CS concept as promising approach for the demarcation of the heavy to severe exercise boundary [4, 8], and that VThigh assessed by VT2 or RCP most likely overestimates CP by 6–21% [75]. As to date no study directly compared HRVThigh with CP/CS, the existing evidence derived from the reviewed studies is, in our opinion, insufficient to draw a robust conclusion on whether HRVThigh can be used to accurately separate the heavy from the severe intensity domain. Cognizant of this gap in the literature, we recommend that future method comparison studies should also incorporate CP/CS as a reference method to broaden our knowledge in this direction.
HRVThigh Versus LThigh
Only five studies compared HRVThigh against LThigh and used a large variety of methodological approaches [41, 54, 56, 90, 92] which limits the generalizability of our conclusions. Of these studies, one used a time–frequency approach [41, 54, 56, 90, 92], two used Poincaré Plot analysis [41, 92] with direct relation to time-domain metrics [102] and two studies used a nonlinear approach [51, 56], while the reference methods used for LThigh were two times LTlow plus 1.5 mmol/l blood lactate, and once each baseline lactate plus 2 mmol/l, a fixed blood lactate value of 3.5 mmol/l and the turn point of the blood lactate curve. The threshold values that could be obtained from HRVThigh in comparison to LThigh show a small to moderate positive mean bias and differences in weighted means for HR and power (see Table 5). With regard to speed, one study used an incremental swimming test to determine time–frequency based HRVThigh by the calculation of HF power from an extended HF-band (0.4–2.0 Hz), while the mechanical influences of stroke rate and RSA were separated [90]. In comparison to LThigh, the mean difference between HR and speed at HRVThigh was small, while LoA were small to moderate (see Table 5). None of the other studies used a (time-) frequency domain-based approach for HRVThigh in comparison with LThigh and none of the other studies included female participants.
In addition, two studies conducted by the same research group used two different SD2 based methods—extracted from the corresponding Poincaré Plot—to determine HRVThigh [41, 92]. These authors then applied the Dmax-method to the SD2 curve, which is known from lactate threshold determination [103]. In comparison to LThigh the mean difference in running speed for HRVThigh was slightly above 1 km/h, and revealed substantially lower values of HR at HRVThigh (see Table 1) as well as relatively wide LoA for both running speed and HR [92]. Finally, two studies used approaches based on nonlinear HRV-analysis, namely compression entropy (HC) and DFAa1. Within the entropy approach [54], HRVThigh was determined as the minimum of a third order polynomial fit applied to HC time series, and power at HRVThigh compared to power at LThigh (Dickhuth-method [94]) showed a small bias, rather wide LoA, and a high correlation (see Table 1). A similar pattern was reported in a study using linear regression analysis of time-varying DFAa1 and a threshold value of 0.5 to determine HRVThigh [56]. In addition, the systematic bias between HR at HRVThigh and LThigh was small and correlation was high, whereas the LoA were rather wide ([56], see also Table 1). The above-presented findings suggest that in some individuals both thresholds did not accurately match. However, it remains unclear whether this difference is an issue of the LThigh or HRVThigh concept in general or whether the chosen exercise protocol plays the particularly decisive role. Principally, the specific concept of LThigh determination and the exercise protocol play an important role and are known to strongly influence the level of agreement between parameters derived from these threshold concepts [4, 8, 9]. In this context, even wider LoA were found when comparing results from VThigh and several different LThigh determination methods [72]. Furthermore, the complex interaction of various methodologies in nonlinear HRV analysis with different recording devices and artefact correction methods [43, 94, 104] might influence the accuracy of the threshold determination. Based on the above-mentioned issues and gaps in the literature, HRVThigh concepts utilizing a nonlinear analysis of HRV need a further evaluation to ensure that they can be accurately and reliably applied in a larger number of individuals, including female participants.
In summary, HRVThigh that is determined by different linear and nonlinear HRV-metrics show heterogeneous results and moderate agreement in comparison with LThigh. Compared to the other threshold comparisons being conducted in this systematic review, HRVThigh and LThigh showed the lowest level of agreement. In this regard, our systematic analysis of the literature suggests that especially the specific LThigh concept being used in comparison with HRVThigh can strongly influence the level of agreement. Additionally, in line with the comparison of HRVThigh and VThigh, it needs to be considered that no study directly compared HRVThigh with the promising reference standard of the CP/CS concept as mentioned above [4, 8]. Taking into account that LThigh compared to MLSS is likely biased by 0.5–8% at least for running exercise [74] and MLSS, in turn, is likely to underestimate CP by 11% [75], it needs to be pointed out that the existing evidence does not allow for robust conclusions on whether HRVThigh can be used to demarcate the boundary of the heavy and severe intensity domains. As proposed for the comparison of HRVThigh and VThigh, future efforts and method comparison studies that (i) incorporate CP/CS as a reference method and (ii) include female participants being currently highly underrepresented in the existing studies on the ‘higher’ threshold comparisons, are urgently needed for more reliable and nuanced conclusions on the applicability of HRVThigh.
Practical Applications
Based on the findings of our systematic review, the utilization of HRVTs as an alternative to VTs and LTs within the exercise intensity distribution model of endurance training is ambiguous. Our review supports the notion that HRVTlow is a promising approach for healthy, male adults participating in endurance-type activities for the determination of a ‘lower’ threshold comparable to VTlow that can be used to demarcate the boundary between moderate and heavy exercise intensity. Whether HRVThigh also constitutes a promising approach to denote the boundary between the heavy and severe exercise domain, needs further evaluation by direct method comparison studies using the CP/CS approach as a reference method.
With regard to a practical application, in a best-case scenario a trained male endurance athlete with a HRmax of 200 bpm will train almost exactly in the same intensity zone as when the exercise intensity would have been determined using VT approaches. Theoretically, the boundary would be about 0.5% of HRmax higher at the lower threshold and around 1.5% higher of HRmax at the higher threshold. Such small differences are negligible for practical application [72]. Nevertheless, in a worst-case scenario the boundary between moderate and heavy exercise can be over- or underestimated by 6% of HRmax, and thus, the boundary between heavy and severe exercise would be off by about 6.8% of HRmax. Consequently, the athlete would at least partly train in the wrong intensity zone when the aim is to train at a moderate intensity but would train entirely in the wrong zone when the aim is to train at severe exercise intensity. From a theoretical point of view, such inaccuracies would even be exacerbated when a five-intensity zone training model is applied. Thus, the applied intensity will, depending on the scenario and used training intensity model, considerably over- or undershoot the desired training load and thus probably not provoke the acute physiological responses aimed for according to the targeted exercise intensity zones [1, 9].
Finally, our systematic review does not support the use of HRVTs as proxies for LTlow and LThigh, respectively. This observation is mainly related to the plethora of methodologies that have been used in both HRVT and LT assessment. Thus, future high-quality studies with larger and more diverse populations (i.e., including female participants) and more standardized methodological procedures including the use of CP/CS concept as a reference method [4, 8] are necessary to broaden our knowledge in this direction and to allow for more robust and nuanced conclusions. Considering the findings of our systematic review on HRVT methods, we recommend the application of sophisticated time–frequency methods considering both RSA and locomotor frequency, especially for the comparison with ‘higher’ thresholds from ventilatory and/or blood lactate measurements when the upper body is involved in propulsion [89, 90]. However, our summary of the current state of the literature does not allow determination of a specific exercise protocol that suits best for a specific HRVT. Consequently, further efforts are necessary to establish generally accepted exercise protocol(s) that can be used to determine specific HRVTs. Whether HRVT-based metrics represent a useful instrument that can be utilized for a real-time prescription of exercise intensity [25] or to conduct a remote performance testing (e.g., in tele-healthcare settings), and whether this holds true for female participants or different groups of patients, is a promising area of research for future high-quality studies.
Limitations
Based on the risk of bias assessment, the overall methodological quality of the included studies appears to be limited, which, in turn, necessitates the need for more high-quality research on HRVT to draw reliable conclusions. In general, it should be kept in mind that research involving physical exercises, to a certain degree, suffers from a selection bias as only volunteers are tested, and thus, individuals being not motivated to participate in physical exercise studies are likely to be underrepresented in the samples. Furthermore, a major limitation of the reviewed studies is that female participants are underrepresented. Thus future studies are strongly encouraged to include them to evaluate whether our findings are generalizable to females. Based on the variety of HRV-threshold concepts, further research including larger cohorts and comparing different threshold approaches is warranted. Additionally, as there is no extensive research on test–retest reliabilities of the different HRVT-methods, future studies should seek to address this gap to facilitate the application of HRVT in different settings. Similarly, stability of the HRV indices used in the original investigations and their interaction with corresponding exercise protocols and types of physical exercise need to be further evaluated. Finally, HRVTs were only validated against other threshold concepts of VT and/or LT but data on the direct relation with CP/CS are lacking. In addition, data on the HRVT-based exercise prescription during constant load exercise or regarding the longitudinal effectiveness of HRVT-based intensity zones are mandatory to evaluate whether acute HRV responses to exercise are predictive of chronic adaptations. Cognizant of the above-presented limitations and gaps in the literature, the following recommendations for future investigations are given.
Recommendations for Future Research
-
We advise upcoming studies to consider a high methodological standardization and to take all aspects of the STARDHRV tool [69] into account. In this context, especially when more sophisticated HRV approaches (e.g., time–frequency and/or nonlinear methods) are used, an entirely transparent reporting including sufficient information on data processing steps should be conducted.
-
Except for HRVTlow VTlow, female participants were highly underrepresented in the studies included in this systematic review. Therefore, future method comparison studies should aim to evaluate HRVT determination in females.
-
Based on the limited number of available high-quality studies and being aware of their limitations, further research should investigate the influence of different exercise protocols and types of physical exercise on HRVTs. Additionally, more research on test–retest-reliability of HRVTs is needed.
-
Concerning the validity of HRVTs for exercise prescription, future studies should seek to elucidate whether VT and/or LT concepts represent an adequate reference standard for a method comparison study with HRVTs, especially when the ‘higher’ threshold to partition the heavy from the severe exercise intensity domain is addressed [4, 8]. In this regard, it should also be noted that threshold concepts use transition points from specific physiological subsystems (e.g., metabolism, ventilation), and therefore related thresholds derived from different subsystems might not necessarily need to show a close agreement [105]. On the basis of “network physiology” approaches [106] a gold standard internal load metric for organismic system demands as a more comparable construct for ANS-derived thresholds like HRVT is still missing. Comparable to recent comparisons of ventilatory- and HR-based training studies [107, 108], we recommend that future high-quality longitudinal studies aim to elucidate the effectiveness of HRVTs for training prescription by comparing them with established LT-, VT- and/or CP/CS-based training prescription.
Conclusion
In summary, the findings of our systematic review and data synthesis reveal that HRVTs for healthy, male adults participating in endurance-type activities show a general high overall correlation but very heterogeneous degree of agreement with established VTs and/or LTs. The agreement strongly varies with the chosen reference method and/or HRVT approach. Due to the large overall heterogeneity in methodological quality and the rather small sample sizes in the reviewed method comparison studies, HRVT cannot be used interchangeably with traditional threshold concepts of VT and/or LT. However, based on the evidence of the current systematic review, it seems reasonable to conclude that HRVTlow is a promising approach for the determination of a ‘lower’ threshold comparable to VTlow that could be used to demarcate the boundary between moderate and heavy exercise intensity. Considering only VT approaches, HRVThigh is also able to denote the boundary between the heavy and severe exercise domain, although this assumption needs further empirical evaluation. Based on the plethora of methodological approaches that have been used to establish LT and HRVT, the use of HRVTs as proxies for LTlow and LThigh cannot be supported yet. In particular, the lack of evaluation by direct method comparison studies with the CP/CS approach impedes the evaluation of HRVT methods for ‘higher’ threshold determination and therefore reliable conclusions on its usefulness to delineate the heavy from the severe intensity domain. Thus, to further substantiate the available evidence on HRVTs and to allow for a generalization of our findings (e.g., to females), future rigorously standardized high-quality trials with larger samples, more diverse subjects and more standardized reference approaches are required.
Availability of data and materials
Data are available from the corresponding author on reasonable request.
Abbreviations
- ANS:
-
Autonomic nervous system
- AR:
-
Autoregressive modeling
- CEn:
-
Compression entropy
- CP:
-
Critical power
- CS:
-
Critical speed
- CV:
-
Coefficient of variation
- DFA:
-
Detrended fluctuation analysis
- DFAa1:
-
Short-term scaling exponent alpha 1 of detrended fluctuation analysis
- FFT:
-
Fast Fourier transformation
- GET:
-
Gas exchange threshold to indicate an excess production of CO2 (most often V-slope of VCO2/VO2) as a boundary between moderate and heavy intensity exercise [100]
- HF:
-
High-frequency power
- HR:
-
Heart rate
- HRV:
-
Heart rate variability
- HRVT:
-
Heart rate variability-derived threshold for exercise intensity distribution
- HRVThigh:
-
Group of ‘higher’ heart rate variability-derived threshold as a boundary between heavy and severe intensity exercises
- HRVTlow:
-
Group of ‘lower’ heart rate variability-derived threshold as a boundary between moderate and heavy intensity exercises
- LoA:
-
Limits of agreement
- LTlow:
-
‘Lower’ lactate threshold based on different approaches to denote onset of blood lactate concentration above baseline (e.g., LT, LT1 (baseline + 0.5, log-logLT)) as a boundary between moderate and heavy intensity exercise [4, 8]
- LThigh:
-
‘Higher’ lactate threshold based on different approaches to denote an equilibrium of blood lactate production and elimination (e.g., IAT, LT2, MLSS), as a boundary between heavy and severe intensity exercise [4, 8]
- MLSS:
-
Maximum lactate steady state to indicate the maximum sustainable intensity that induces an equilibrium of blood lactate production and elimination (< 1 mmol/l increase in last 20 min of 30 min constant load exercise) as a boundary between heavy and severe intensity exercise [109]
- OSF:
-
Open Science Framework
- pHF:
-
Peak high frequency
- PICOS:
-
PICOS-principle (“PICOS” stands for participants (P), intervention (I), comparisons (C), outcomes (O), and study design (S))
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QUADAS:
-
Quality Assessment of Diagnostic Accuracy Studies
- RCP/VT2:
-
Respiratory compensation point/‘second’ ventilatory threshold to denote hyperventilation as a consequent to a concomitant increase in blood lactate and H+ above disposal (most often second breakpoint in VE, clear one in VE/VCO2, fall of PETCO2) as a boundary between heavy and severe intensity exercise [4, 8]
- RMSSD:
-
Root mean square of successive differences
- RQA:
-
Recurrence quantification analysis
- RSA:
-
Respiratory sinus arrhythmia
- SampEn:
-
Sample entropy
- SD1:
-
Standard deviation one of Poincaré Plot
- SD2:
-
Standard deviation two of Poincaré Plot
- SPWVD:
-
Smoothed-pseudo Wigner–Ville distribution
- STARD:
-
Standard for Reporting of Diagnostic Accuracy Studies
- STFT:
-
Short-term Fourier transform
- VT/VT1:
-
(‘First’) ventilatory threshold based on different ventilatory methods to indicate a (‘first’) nonlinear increase in minute ventilation (VE) (most often considering VE/VO2, PETO2 and PETCO2) as a boundary between moderate and heavy intensity exercise [4]
- VThigh:
-
‘Higher’ ventilatory threshold to denote hyperventilation as a consequent to a concomitant increase in blood lactate and H+ above disposal (e.g., RCP, VT2) as a boundary between heavy and severe intensity exercise [4, 8]
- VTlow:
-
‘Lower’ ventilatory threshold based on different ventilatory/gas exchange methods to indicate an excess production of CO2 (e.g., VT, GET (V-slope of VCO2/VO2)) as a boundary between moderate and heavy intensity exercise [4]
References
Seiler KS, Kjerland GØ. Quantifying training intensity distribution in elite endurance athletes: is there evidence for an “optimal” distribution? Scand J Med Sci Sports. 2006;16(1):49–56.
Esteve-Lanao J, Foster C, Seiler S, Lucia A. Impact of training intensity distribution on performance in endurance athletes. J Strength Cond Res. 2007;21(3):943–9.
Vanhatalo A, Black MI, DiMenna FJ, Blackwell JR, Schmidt JF, Thompson C, et al. The mechanistic bases of the power–time relationship: muscle metabolic responses and relationships to muscle fibre type. J Physiol. 2016;594(15):4407–23.
Jamnick NA, Pettitt RW, Granata C, Pyne DB, Bishop DJ. An examination and critique of current methods to determine exercise intensity. Sports Med. 2020;50:1–28.
Seiler S. What is best practice for training intensity and duration distribution in endurance athletes? Int J Sports Physiol Perform. 2010;5(3):276–91.
Casado A, Foster C, Bakken M, Tjelta LI. Does lactate-guided threshold interval training within a high-volume low-intensity approach represent the “next step” in the evolution of distance running training? Int J Environ Res Public Health. 2023;20(5):3782.
Meyer T, Lucia A, Earnest CP, Kindermann W. A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters-theory and application. Int J Sports Med. 2005;26(S1):S38–48.
Poole DC, Rossiter HB, Brooks GA, Gladden LB. The anaerobic threshold: 50+ years of controversy. J Physiol. 2021;599(3):737–67.
Beneke R, Leithäuser RM, Ochentel O. Blood lactate diagnostics in exercise testing and training. Int J Sports Physiol Perform. 2011;6(1):8–24.
Heck H, Beneke R. 30 Jahre Laktatschwellen–was bleibt zu tun? Dtsche Z Sportmed. 2008;59(12):297.
Mann T, Lamberts RP, Lambert MI. Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med. 2013;43(7):613–25.
Stöggl TL, Sperlich B. The training intensity distribution among well-trained and elite endurance athletes. Front Physiol. 2015;6:295.
Wackerhage H, Gehlert S, Schulz H, Weber S, Ring-Dimitriou S, Heine O. Lactate thresholds and the simulation of human energy metabolism: contributions by the cologne sports medicine group in the 1970s and 1980s. Front Physiol. 2022;13:1308.
Vanhatalo A, Jones AM, Burnley M. Application of critical power in sport. Int J Sports Physiol Perform. 2011;6(1):128–36.
Allen H, Coggan AR, McGregor S. Training and racing with a power meter. 2nd ed. Boulder: VeloPress; 2019.
Borszcz FK, Tramontin AF, Costa VP. Is the functional threshold power interchangeable with the maximal lactate steady state in trained cyclists? Int J Sports Physiol Perform. 2019;14(8):1029–35.
Haugen T, Sandbakk Ø, Seiler S, Tønnessen E. The training characteristics of world-class distance runners: an integration of scientific literature and results-proven practice. Sports Med-Open. 2022;8(1):1–18.
Bhambhani YN, Buckley SM, Susaki T. Detection of ventilatory threshold using near infrared spectroscopy in men and women. Med Sci Sports Exerc. 1997;29(3):402–9.
Bodner ME, Rhodes EC. A review of the concept of the heart rate deflection point. Sports Med. 2000;30(1):31–46.
Hofmann P, Pokan R. Value of the application of the heart rate performance curve in sports. Int J Sports Physiol Perform. 2010;5(4):437–47.
Yamamoto Y, Hughson RL, Peterson JC. Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol. 1991;71(3):1136–42.
Yamamoto Y, Hughson RL, Nakamura Y. Aotonomic nervous-system responses to exercise in relation to ventilatory threshold. Chest. 1992;101(5):S206–10.
Tulppo MP, Makikallio TH, Takala T, Seppanen T, Huikuri HV. Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am J Physiol Heart Circ Physiol. 1996;271(1):H244–52.
Rogers B, Giles D, Draper N, Hoos O, Gronwald T. A New detection method defining the aerobic threshold for endurance exercise and training prescription based on fractal correlation properties of heart rate variability. Front Physiol. 2021;11:596567.
Gronwald T, Berk S, Altini M, Mourot L, Hoos O, Rogers B. Real-time estimation of aerobic threshold and exercise intensity distribution using fractal correlation properties of heart rate variability: a single-case field application in a former Olympic triathlete. Front Sports Act Living. 2021;3:148.
Laukkanen R, Maijanen S, Tulppo M. Determination of heart rates for training using Polar Smartedge heart rate monitor. Med Sci Sports Exerc. 1998;30(5):251.
Bernardi L, Piepoli M. Autonomic nervous system adaptation during physical exercise. Ital Heart J Suppl. 2001;2(8):831–9.
Sandercock G, Brodie D. The use of heart rate variability measures to assess autonomic control during exercise. Scand J Med Sci Sports. 2006;16(5):302–13.
White DW, Raven PB. Autonomic neural control of heart rate during dynamic exercise: revisited. J Physiol. 2014;592(12):2491–500.
Hottenrott K, Hoos O. Heart rate variability analysis in exercise physiology. ECG time series variability analysis. Boca Raton: CRC Press; 2017. p. 249–80.
Shaffer F, McCraty R, Zerr C. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front Psychol. 2014;5:1040.
Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. 2017;5:258.
Grossman P, Taylor EW. Toward understanding respiratory sinus arrhythmia: relations to cardiac vagal tone, evolution and biobehavioral functions. Biol Psychol. 2007;74(2):263–85.
Anosov O, Patzak A, Kononovich Y, Persson PB. High-frequency oscillations of the heart rate during ramp load reflect the human anaerobic threshold. Eur J Appl Physiol. 2000;83(4–5):388–94.
Karapetian GK, Engels HJ, Gretebeck RJ. Use of heart rate variability to estimate LT and VT. Int J Sports Med. 2008;29(8):652–7.
Cottin F, Leprêtre PM, Lopes P, Papelier Y, Médigue C, Billat V. Assessment of ventilatory thresholds from heart rate variability in well-trained subjects during cycling. Int J Sports Med. 2006;27(12):959–67.
Benarroch EE. The central autonomic network: functional organization, dysfunction, and perspective. Mayo Clin Proc. 1993;68:988–1001.
Michael S, Graham KS, Davis GMO. Cardiac autonomic responses during exercise and post-exercise recovery using heart rate variability and systolic time intervals-a review. Front Physiol. 2017;8:301.
Blain G, Meste O, Bouchard T, Bermon S. Assessment of ventilatory thresholds during graded and maximal exercise test using time varying analysis of respiratory sinus arrhythmia. Br J Sports Med. 2005;39(7):448–52.
Cottin F, Médigue C, Lopes P, Leprêtre PM, Heubert R, Billat V. Ventilatory thresholds assessment from heart rate variability during an incremental exhaustive running test. Int J Sports Med. 2007;28(4):287–94.
Nascimento F, Marcel E, Augusta Pedutti Dal Molin Kiss M, Meireles Santos T, Lambert M, Pires FO. Determination of lactate thresholds in maximal running test by heart rate variability data set. Asian J Sports Med. 2017;8(3):1–8.
Mankowski RT, Michael S, Rozenberg R, Stokla S, Stam HJ, Praet SF. Heart-rate variability threshold as an alternative for spiro-ergometry testing: a validation study. J Strength Cond Res. 2017;31(2):474–9.
Gronwald T, Hoos O. Correlation properties of heart rate variability during endurance exercise: a systematic review. Ann Noninvasive Electrocardiol. 2020;25(1):e12697.
Lewis M, Short A. Sample entropy of electrocardiographic RR and QT time-series data during rest and exercise. Physiol Meas. 2007;28(6):731.
Weippert M, Behrens M, Rieger A, Behrens K. Sample entropy and traditional measures of heart rate dynamics reveal different modes of cardiovascular control during low intensity exercise. Entropy. 2014;16(11):5698–711.
Peng CK, Havlin S, Stanley HE, Goldberger AL. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos. 1995;5(1):82–7.
Giuliani A, Piccirillo G, Marigliano V, Colosimo A. A nonlinear explanation of aging-induced changes in heartbeat dynamics. Am J Physiol Heart Circ Physiol. 1998;275(4):H1455–61.
Baumert M, Baier V, Haueisen J, Wessel N, Meyerfeldt U, Schirdewan A, et al. Forecasting of life threatening arrhythmias using the compression entropy of heart rate. Methods Inf Med. 2004;43(02):202–6.
Platisa MM, Mazic S, Nestorovic Z, Gal V. Complexity of heartbeat interval series in young healthy trained and untrained men. Physiol Meas. 2008;29(4):439.
Webber C, Marwan N. Recurrence quantification analysis. Theory and best practices. Cham: Springer; 2015.
Rogers B, Giles D, Draper N, Mourot L, Gronwald T. Detection of the anaerobic threshold in endurance sports: validation of a new method using correlation properties of heart rate variability. J Funct Morphol Kinesiol. 2021;6(2):38.
Zimatore G, Falcioni L, Gallotta MC, Bonavolontà V, Campanella M, De Spirito M, et al. Recurrence quantification analysis of heart rate variability to detect both ventilatory thresholds. PLoS ONE. 2021;16(10):e0249504.
Zimatore G, Gallotta M, Innocenti L, Bonavolontà V, Ciasca G, De Spirito M, et al. Recurrence quantification analysis of heart rate variability during continuous incremental exercise test in obese subjects. Chaos. 2020;30(3):033135.
Hamdan AR, Schumann A, Herbsleb M, Schmidt M, Rose G, Bär K-J, et al. Determining cardiac vagal threshold from short term heart rate complexity. Curr Dir Biomed Eng. 2016;2(1):155–9.
Gronwald T, Rogers B, Hoos O. Fractal correlation properties of heart rate variability: a new biomarker for intensity distribution in endurance exercise and training prescription? Front Physiol. 2020;11:1152.
Mateo-March M, Moya-Ramón M, Javaloyes A, Sánchez-Muñoz C, Clemente-Suárez VJ. Validity of detrended fluctuation analysis of heart rate variability to determine intensity thresholds in professional cyclists. Eur J Sport Sci. 2022:1–20 (just-accepted).
Casties J-F, Mottet D, Le Gallais D. Non-linear analyses of heart rate variability during heavy exercise and recovery in cyclists. Int J Sports Med. 2006;27(10):780–5.
Hautala AJ, Mäkikallio TH, Seppänen T, Huikuri HV, Tulppo MP. Short-term correlation properties of R-R interval dynamics at different exercise intensity levels. Clin Physiol Funct Imaging. 2003;23(4):215–23.
Karavirta L, Tulppo MP, Nyman K, Laaksonen DE, Pullinen T, Laukkanen RT, et al. Estimation of maximal heart rate using the relationship between heart rate variability and exercise intensity in 40–67 years old men. Eur J Appl Physiol. 2008;103(1):25–32.
Blasco-Lafarga C, Camarena B, Mateo-March M. Cardiovascular and autonomic responses to a maximal exercise test in elite youngsters. Int J Sports Med. 2017;38(09):666–74.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372.
Harris JD, Quatman CE, Manring MM, Siston RA, Flanigan DC. How to write a systematic review. Am J Sports Med. 2014;42(11):2761–8.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
McGraw KO, Wong SP. A common language effect size statistic. Psychol Bull. 1992;111(2):361.
Cohen J. The effect size Statistical power analysis for the behavioral sciences. Hillsdale: L. Erlbaum Associates; 1988. p. 77–83.
Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135–60.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63.
Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36.
Dobbs WC, Fedewa MV, MacDonald HV, Holmes CJ, Cicone ZS, Plews DJ, et al. The accuracy of acquiring heart rate variability from portable devices: a systematic review and meta-analysis. Sports Med. 2019;49(3):417–35.
Cohen JF, Korevaar DA, Altman DG, Bruns DE, Gatsonis CA, Hooft L, et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: explanation and elaboration. BMJ Open. 2016;6(11):e012799.
Cerezuela-Espejo V, Courel-Ibáñez J, Morán-Navarro R, Martínez-Cava A, Pallarés JG. The relationship between lactate and ventilatory thresholds in runners: validity and reliability of exercise test performance parameters. Front Physiol. 2018;9:1320.
Pallarés JG, Morán-Navarro R, Ortega JF, Fernández-Elías VE, Mora-Rodriguez R. Validity and reliability of ventilatory and blood lactate thresholds in well-trained cyclists. PLoS ONE. 2016;11(9):e0163389.
Gaskill SE, Ruby BC, Walker AJ, Sanchez OA, Serfass RC, Leon AS. Validity and reliability of combining three methods to determine ventilatory threshold. Med Sci Sports Exerc. 2001;33(11):1841–8.
Faude O, Kindermann W, Meyer T. Lactate threshold concepts: how valid are they? Sports Med. 2009;39:469–90.
Galán-Rioja MÁ, Gonzalez-Mohino F, Poole DC, González-Ravé JM. Relative proximity of critical power and metabolic/ventilatory thresholds: systematic review and meta-analysis. Sports Med. 2020;50:1771–83.
Coffey VG, Zhong Z, Shield A, Canny BJ, Chibalin AV, Zierath JR, et al. Early signaling responses to divergent exercise stimuli in skeletal muscle from well-trained humans. FASEB J. 2006;20(1):190–2.
Camera DM, Smiles WJ, Hawley JA. Exercise-induced skeletal muscle signaling pathways and human athletic performance. Free Radic Biol Med. 2016;98:131–43.
Teso M, Colosio AL, Pogliaghi S. An intensity-dependent slow component of HR interferes with accurate exercise implementation in postmenopausal women. Med Sci Sports Exerc. 2022;54(4):655.
Lamberts RP, Lambert MI. Day-to-day variation in heart rate at different levels of submaximal exertion: implications for monitoring training. J Strength Cond Res. 2009;23(3):1005–10.
Pereira M, Freedson P. Intraindividual variation of running economy in highly trained and moderately trained males. Int J Sports Med. 1997;18(02):118–24.
Ebreo R, Passfield L, Hopker J. The reliability of measuring gross efficiency during high-intensity cycling exercise. Int J Sports Physiol Perform. 2020;15(1):126–32.
Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669–82.
Mazzeo RS. Physiological responses to exercise at altitude. Sports Med. 2008;38(1):1–8.
Sylta Ø, Tønnessen E, Seiler S. Do elite endurance athletes report their training accurately? Int J Sports Physiol Perform. 2014;9(1):85–92.
Ramos-Campo DJ, Rubio-Arias JA, Ávila-Gandía V, Marín-Pagán C, Luque A, Alcaraz PE. Heart rate variability to assess ventilatory thresholds in professional basketball players. J Sport Health Sci. 2017;6(4):468–73.
Mendia-Iztueta I, Monahan K, Kyröläinen H, Hynynen E. Assessment of heart rate variability thresholds from incremental treadmill tests in five cross-country skiing techniques. PLoS ONE. 2016;11(1):e0145875.
Cunha FA, Montenegro RA, Midgley AW, Vasconcellos F, Soares PP, Farinatti P. Influence of exercise modality on agreement between gas exchange and heart rate variability thresholds. Braz J Med Biol Res. 2014;47(8):706–14.
Lilienthal J, Dargie W. Spectral characteristics of motion artifacts in wireless ECG and their correlation with reference motion sensors. Annu Int Conf IEEE Eng Med Biol Soc. 2021;2021:517–21.
Mourot L, Fabre N, Savoldelli A, Schena F. Second ventilatory threshold from heart-rate variability: valid when the upper body is involved? Int J Sports Physiol Perform. 2014;9(4):695–701.
Di Michele R, Gatta G, Di Leo A, Cortesi M, Andina F, Tam E, et al. Estimation of the anaerobic threshold from heart rate variability in an incremental swimming test. J Strength Cond Res. 2012;26(11):3059–66.
Garcia-Tabar I, Sánchez-Medina L, Aramendi JF, Ruesta M, Ibañez J, Gorostiaga EM. Heart rate variability thresholds predict lactate thresholds in professional world-class road cyclists. J Exerc Physiol Online. 2013;16(5):38–50.
Nascimento F, Antunes D, do Nascimento Salvador PC, Borszcz FK, de Lucas RD. Applicability of Dmax method on heart rate variability to estimate the lactate thresholds in male runners. J Sports Med. 2019;2019:2075371.
Shiraishi Y, Katsumata Y, Sadahiro T, Azuma K, Akita K, Isobe S, et al. Real-time analysis of the heart rate variability during incremental exercise for the detection of the ventilatory threshold. J Am Heart Assoc. 2018;7(1):e006612.
Dickhuth H-H, Röcker K, Mayer F, Nieß A, Horstmann T, Heitkamp H-C. Bedeutung der Leistungsdiagnostik und Trainingssteuerung bei Ausdauer-und Spielsportarten. Dtsch Z für Sportmed. 1996;47:183–9.
Whipp BJ, Davis JA, Wasserman K. Ventilatory control of the ‘isocapnic buffering’ region in rapidly-incremental exercise. Respir Physiol. 1989;76(3):357–67.
Cassirame J, Tordi N, Fabre N, Duc S, Durand F, Mourot L. Heart rate variability to assess ventilatory threshold in ski-mountaineering. Eur J Sport Sci. 2015;15(7):615–22.
García-Manso JM, Sarmiento-Montesdeoca S, Martín-González JM, Calderón-Montero EJ, Da Silva-Grigoletto ME. Wavelet transform analysis of heart rate variability for determining ventilatory thresholds in cyclists. Rev Andaluza Med Deporte. 2008;1(3):90–7.
Stergiopoulos DC, Kounalakis SN, Miliotis PG, Geladas ND. Second ventilatory threshold assessed by heart rate variability in a multiple shuttle run test. Int J Sports Med. 2021;42(1):48–55.
Wasserman K, Hansen J, Sue D, Casaburi R, Whipp B. The anaerobic threshold (AT) concept. In: Principles of exercise testing and interpretation; 1999. p. 63–77.
Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol. 1986;60(6):2020–7.
Leger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci. 1988;6(2):93–101.
Ciccone AB, Siedlik JA, Wecht JM, Deckert JA, Nguyen ND, Weir JP. Reminder: RMSSD and SD1 are identical heart rate variability metrics. Muscle Nerve. 2017;56(4):674–8.
Cheng B, Kuipers H, Snyder A, Keizer H, Jeukendrup A, Hesselink M. A new approach for the determination of ventilatory and lactate thresholds. Int J Sports Med. 1992;13(07):518–22.
Rogers B, Giles D, Draper N, Mourot L, Gronwald T. Influence of artefact correction and recording device type on the practical application of a non-linear heart rate variability biomarker for aerobic threshold determination. Sensors. 2021;21(3):821.
Rogers B, Gronwald T. Fractal correlation properties of heart rate variability as a biomarker for intensity distribution and training prescription in endurance exercise: an update. Front Physiol. 2022;13:879071.
Balagué N, Hristovski R, Almarcha MDC, Garcia-Retortillo S, Ivanov PC. Network physiology of exercise: vision and perspectives. Front Physiol. 2020;11:1607.
Weatherwax RM, Harris NK, Kilding AE, Dalleck LC. Incidence of V˙ O2max responders to personalized versus standardized exercise prescription. Med Sci Sports Exerc. 2019;51(4):681–91.
Wolpern AE, Burgos DJ, Janot JM, Dalleck LC. Is a threshold-based model a superior method to the relative percent concept for establishing individual exercise intensity? a randomized controlled trial. BMC Sports Sci Med Rehabil. 2015;7:1–9.
Billat VL, Sirvent P, Py G, Koralsztein J-P, Mercier J. The concept of maximal lactate steady state: a bridge between biochemistry, physiology and sport science. Sports Med. 2003;33:407–26.
Dourado VZ, Banov MC, Marino MC, De Souza VL, Antunes LCDO, McBurnie MA. A Simple approach to assess VT during a field walk test. Int J Sports Med. 2010;31(10):698–703.
Dourado VZ, Guerra RL. Reliability and validity of heart rate variability threshold assessment during an incremental shuttle-walk test in middle-aged and older adults. Braz J Med Biol Res. 2013;46(2):194–9.
Grannell A, De Vito G. An investigation into the relationship between heart rate variability and the ventilatory threshold in healthy moderately trained males. Clin Physiol Funct Imaging. 2018;38(3):455–61.
Park SW, Brenneman M, Cooke WH, Cordova A, Fogt D. Determination of anaerobic threshold by heart rate or heart rate variability using discontinuous cycle ergometry. Int J Exerc Sci. 2014;7(1):45–53.
Queiroz MG, de Araujo JA, Rezende DAN, Dias ARL, Novelli FI, Tricot GK, et al. Heart rate variability threshold estimates ventilatory threshold in young people with different body mass index. Med Sci Sports Exerc. 2016;48(5):415.
Acknowledgements
The results of the present study do not constitute endorsement of the product by the authors or the journal.
Funding
Open Access funding was enabled and organized by Projekt DEAL. None of the authors received funding for this work from any organization, other than salary support for the authors from their respective institutions. Open-access was funded by Project-DEAL.
Author information
Authors and Affiliations
Contributions
SK, OH and TG designed the research. SK and TG conducted the systematic literature search and selected articles that met the criteria of the review. OH supported the process. SK and FH extracted the data, and SK and OH compiled the synthesis. SK and TG drafted the manuscript. OH and FH critically reviewed the manuscript. SK, TG and OH drafted the final version of the manuscript. All authors read and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the standards of ethics outlined in the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
Sebastian Kaufmann, Thomas Gronwald, Fabian Herold and Olaf Hoos declare that they have no potential conflicts of interest that might be relevant to the contents of this manuscript. This also includes professional interests, personal relationships or personal beliefs.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaufmann, S., Gronwald, T., Herold, F. et al. Heart Rate Variability-Derived Thresholds for Exercise Intensity Prescription in Endurance Sports: A Systematic Review of Interrelations and Agreement with Different Ventilatory and Blood Lactate Thresholds. Sports Med - Open 9, 59 (2023). https://doi.org/10.1186/s40798-023-00607-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-023-00607-2