
Abstract
Background
A persistent Müllerian duct syndrome is a rare disorder of sexual differentiation characterized by the presence of the female reproductive system in a normal male.
Case presentation
Herein, we report a case of a 35-year-old father with persistent Müllerian duct syndrome and seminoma in the right undescended testis. The exploratory laparotomy was performed and revealed a mass in the right undescended testis and Müllerian duct structures.
Conclusions
For patients with cryptorchidism and inguinal hernia, the persistent Müllerian duct syndrome should be considered, and radiological evaluation of the genitourinary system is recommended for early diagnosis of persistent Müllerian duct syndrome. The persistent Müllerian duct syndrome is usually detected during a surgical operation, and it is considered a risk factor for developing testicular malignancies.
Similar content being viewed by others


Background
Persistent Müllerian duct syndrome (PMDS) is a sexual development disorder characterized by the presence of female reproductive organs in individuals with both normal chromosomes (46, XY) and a normal phenotype of a male. It could be accidentally found during orchidopexy, laparotomy, or routine inguinal hernia repair in patients presenting with cryptorchidism (undescended testis).
Usually, one testis is typically positioned, and the other is undescended. However, it is conceivable to be bilateral as well [1, 2]. The persistence of Müllerian ducts (MD) in these genetically normal males may be explained by the incapacity to produce the anti-Müllerian hormone (AMH) by Sertoli cells or a defect in AMH type II receptor (AMHR-II), since this hormone causes MD regression [3]. Cryptorchidism is a risk factor for developing testicular cancers, and it was reported to be associated with PMDs [4, 5]. So far, few cases of PMDs associated with seminoma have been reported.
Case presentation
A 35-year-old mute father with one child presented to the Department of General Surgery with persistent spastic abdominal pain in the right iliac fossa (RIF) treated with antispasmodic and analgesic medications. The patient has a typical male appearance with regular secondary sexual characteristics and a medical history of right inguinal hernia repair 15 years ago. Apart from the abovementioned medical history, an ultrasound (US) demonstrated a large echogenic mass located in the RIF. No clinical signs of acute appendicitis were found which excluded the diagnosis of appendicitis. Consequently, a computed tomography (CT) scan was performed and revealed a hypodense homogeneous mass between the cecum and the urinary bladder with a diameter of 8 cm compressing the latter and allowing the diffusion of the contrast product (Fig. 1).

A, B Axial pelvis CT scan with intravenous injection of contrast material shows the pelvic cyst (red arrow)
A large internal iliac lymph node exceeding 1 cm of diameter was also observed. Furthermore, evaluating the right upper hypochondriac region with a CT scan demonstrated a gallbladder containing a small stone. A laparotomy procedure was performed. Exploring the abdominal iliac fossa revealed a dermoid cyst in an undescended right-sided testis, resulting in a perioperative diagnosis of an undescended testis tumor. Moreover, during laparotomy, a globular structure resembling the uterus with the cervix, Fallopian tubes, and vagina were found (Fig. 2).

A Pelvic cyst mass in the Iliac fossa and B uterus found during the laparotomy procedure
However, ovaries were not found. A uterine catheter with a radio-contrast agent to explore the uterus depth was introduced, and a right infundibulum was discovered attached to the visceral abdominal wall (Fig. 3). An orchiectomy for the right undescended testis was performed, as well as resection of the associated mass. Lymphadenectomy was not performed due to the proximity of the node to the iliac artery. Ten days later after obtaining the written patient content. The second surgery was performed, total excision of the uterus with the Fallopian tube, cervix, infundibulum, and cholecystectomy, were conducted.

Uteroscopy image shows uterus and right infundibulum attached to the visceral abdominal wall
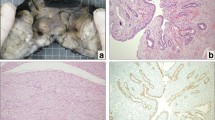
During surgery, a mucous liquid in the uterus cavity, not exceeding 50 ml, and a swollen pouch of Douglas were found. The specimen showed a mass of well-circumscribed testis, with smooth gray mass, and an attached tube-like structure. Weighs 239 gm measured ~ 10 × 75 cm (Fig. 4). Cut sections revealed a tan/white friable surface. Cut sections of the mass showed sheets and lobular configuration of germ cells with hyperchromatic nuclei and prominent nucleoli surrounded by thin fibrous septa infiltrated by lymphocytes. No hemorrhage or necrosis was noticed. The nearby regions showed hyalinized seminiferous tubules.

A Mass of the well-circumscribed testis, with smooth gray mass, and attached tube-like structure. B Rudimentary uterus
The histopathological study confirmed the features of a classical seminoma stage T1b. The tunica albuginea and the epididymis were free (Fig. 5). Throughout second surgery, the specimen of the pelvic mass-like uterus shape revealed a rudimentary uterus with a cervix that weighs 60 gm and measures ~ 11 × 5 × 3 cm, the body ~ 5 × 5 × 3 cm, and the cervix ~ 6 × 2 cm (Fig. 4). Cut sections revealed an endometrial-like surface. The histopathological study demonstrated atrophic endometrium and myometrium of the uterus. In the cervix, an ulcerated endocervical mucosa was observed.

A Sheets and lobular configuration of germ cells with hyperchromatic nuclei and prominent nucleoli surrounded by thin fibrous septa infiltrated by lymphocytes. B Hyalinized seminiferous tubules. C Fallopian tube tissue surrounded by fibro-fatty tissue contains rete testis and efferent ductules. D Atrophic endometrium and myometrium. E Cervix with ulcerated endocervical mucosa, and seminal vesicles tissue
Furthermore, seminal vesicle tissue is noticeable on the wall. On one side of the uterus, the Fallopian tube tissue surrounded by fibrous-fatty tissues, including rete testis and efferent ductules were detectable. The histopathological examination overall confirmed the presence of both seminoma on the right side undescended testis and uterus, cervix, Fallopian tube (persistent Müllerian duct structures) (Fig. 5). The final diagnosis was a seminoma of the undescended testis with PMDS. Post-operation, the patient's condition remained stable with no evidence of recurrence. He was assigned to the cancer center and he responds well to chemotherapy, his clinical conditions are stable the patient is seen twice yearly.
Conclusions and discussion
PMDS was first described in a male with an inguinal hernia in 1939 by Nilson, presenting as hernia uteri inguinal. It may be caused by an absence of AMH released from Sertoli cells of the male fetus from the seventh week of gestation, it is responsible for the regression of the Müllerian duct. When AMH is not secreted, that may lead to the persistence of female reproductive organs in the males with PMDS [6, 7].
Two anatomic variants have been described: male and female. The male type is most common, and it is classified into two subcategories: hernia uteri inguinal and transverse testicular ectopia. The majority of cases present with unilateral cryptorchidism, and contralateral inguinal hernia [8]. In this case, we demonstrate a rare type of pseudo-hermaphroditism in males characterized by extra female genital organs present in a normal 46XY genotypical and phenotypical father. These organs represent MD structures (the uterus, Fallopian tubes, and upper two-thirds of the vagina). However, radiological findings only revealed the right Fallopian tube in this syndrome (Fig. 3) [9].
PMDS patients are rarely fertile and most of them usually suffer from infertility and inguinal hernia. Causes of infertility are various as testis hypoplasia, and ejaculatory duct obstruction due to compression by MD structures. In comparison, our patient was married and had a child [10].
The diagnosis of PMDS is often controversial, because there are no specific clinical symptoms, it is discovered incidentally either hernia repair or surgery for undescended testes. The risk of malignant transformation increases after puberty; therefore, early diagnosis should be recommended (Fig. 5) [11, 12].
Seminoma is the most common testicular germ-cell tumor. In PMDS, the incidence of malignant transformation in the undescended testis is similar to the incidence of testicular carcinoma in patients without PMDS. Moreover, Müllerian malignancies are more probable to develop than testicular cancer in PMDS [12, 13].
Usually, the undescended testis is detected in the inguinal channel or intra-abdominally, as in our case the right undescended testis was situated intra-abdominally and the left one was in the scrotum. When testicular malignant is suspected the appropriate surgical procedures of orchiectomy followed by removal of MD structures may be discussed [14].
As a long-term follow-up, the palpation of the testis and radiological examinations should be mandatory for any inconsistencies in patients with PMDS [12]. In stage T1b seminoma a single dose of the carboplatin area under the curve 7 (AUC7) was chosen to be the standard treatment for stage I seminoma rather than the adjuvant radiotherapy according to the results from MRC TE19/EORTC 30982 Study [15]. In our case, the patient consent was requested to perform the excision of the Mullerian remnants which were first being discovered during the laparoscopic procedure. This is considered a fundamental step due to the inconclusive guidelines of performing a surgical resection of the mass or just long-term monitoring [11, 12].
Of note the resection of the Mullerian remnants is not standardized as a treatment approach due to the high risk of malignancy; however, a recent outcome analysis showed the effectiveness of performing a laparoscopic approach to treat the patients with PMDS [16].
This publication aims to emphasize the importance of profound clinical examination that may help the diagnosis of PMDS associated with seminoma, even in males with typical appearance and secondary sexual characteristics. The correlation between these two diseases is still unclear. Further diagnostic procedures are required while dealing with an inguinal hernia and cryptorchidism patients to early detect PMDS and to prevent relevant complications.
Availability of data and materials
Not applicable. All data (of the patient) generated during this study are included in this published article and its supplementary information files.
Abbreviations
- PMDS:
-
Persistent Müllerian duct syndrome
- MD:
-
Müllerian ducts
- AMH:
-
Anti-Müllerian hormone
- RIF:
-
Right iliac fossa
- US:
-
Ultrasound
- CT:
-
Computed tomography
- (AUC7):
-
Area under the curve 7
References
Saleem M, Ather U, Mirza B, et al. Persistent mullerian duct syndrome: a 24-year experience. J PediatrSurg. 2016;51(10):1721–4.
Renu D, Rao G, Ranganath K, et al. Persistent mullerian duct syndrome. Indian J Radiol Imaging. 2010;20(1):72.
Josso N, Belville C, di Clemente N, et al. AMH and AMH receptor defects in persistent Müllerian duct syndrome. Hum Reprod Update. 2005;11(4):351–6.
Ferguson L, Agoulnik AI. Testicular cancer and cryptorchidism. Front Endocrinol (Lausanne). 2013. https://doi.org/10.3389/fendo.2013.00032.
Vala N, Bhatt N, Chamrajan S, et al. Persistent mullerian duct syndrome in a patient with bilateral cryptorchid testes with seminoma. J Hum ReprodSci. 2012;5(2):215.
Nilson O. Hernia uteri inguinalisbeim Manne. Acta Chir Scand. 1939;83:231.
Josso N, Lamarre I, Picard J, et al. Anti-Mullerian hormone in early human development. Early Hum Dev. 1993;33(2):91–9.
Dekker H, Jong I, Sanders J, et al. Persistent Mullerian duct syndrome. Radiographics. 2003;23:309–13.
Rey R, Picard J. Embryology and endocrinology of genital development. Balliere’s Clin Endocrinol and Metab. 1998;12:17–33.
Martin EL, Bennett AH, Cromie WJ. Persistent Mullerian duct syndrome with transverse testicular ectopia and spermato-genesis. J Urol. 1992;147:1615–7.
Nayak VJ, Kamath AS, Krishnappa MH, et al. Persistent mullerian duct syndrome: a case report and review of the literature. Int J Appl Basic Med Res. 2014;4(2):125–7.
Farikullah J, Ehtisham S, Nappo S, et al. Persistent Mullerian duct syndrome: lessons learned from managing a series of eight patients over a 10-year period and review of literature regarding malignant risk from the Mullerian Remnants. BJU Int. 2012;110:E1084–9.
Shalaby M, Kurkar A, Zarzour M, et al. The management of the persistent Müllerian duct syndrome. Arab J Urol. 2014;12:239–44.
Alp B, Demirer Z, Gürağaç A, et al. Persistent Mullerian duct syndrome with transverse testicular ectopia and seminoma. Int Urol Nephrol. 2014;46:1557–62.
Oliver RTD, Mead GM, Rustin GJS, et al. Randomized trial of carboplatin versus radiotherapy for stage I seminoma: mature results on relapse and contralateral testis cancer rates in MRC TE19/EORTC 30982 Study (ISRCTN27163214). J Clin Oncol. 2011;29:957–62.
Raicevic M, Saxena AK. Laparoscopic management of Müllerian duct remnants in the paediatric age: evidence and outcome analysis. J Minim Access Surg. 2018;14:95–8.
Acknowledgements
We are grateful to Dr. Mohammad Zakaria Al-Issa, Dr. ShaherYosif, and Khaled Al-Ali for their help in management this case, and contributing in the operation room.
Funding
No funding was required.
Author information
Authors and Affiliations
Contributions
MM: design of study, data collection, data interpretation and analysis, drafting, critical revision, approval of final manuscript. Data interpretation and analysis, critical revision, AF: drafting, approval of final manuscript. Data interpretation and analysis, critical revision, YO: drafting, approval of final manuscript. TA: The Supervisor, drafting, critical revision, approval of final manuscript. OK: The Supervisor, patient care, drafting, critical revision, approval of final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not required for this case report.
Consent for publication
Written informed consent was obtained from the patient for publishing this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Guarantor
Omar Kanjawi is the guarantor of this work.
Competing interests
Marah Mansour, Abdullah Fattal, Yassamine Ouerdane, Tamim Alsuliman, and Omar Kanjawi. All authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mansour, M., Fattal, A., Ouerdane, Y. et al. A 35-year-old father with persistent Mullerian duct syndrome and seminoma of the right undescended testis: a rare case report. surg case rep 7, 271 (2021). https://doi.org/10.1186/s40792-021-01354-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-021-01354-w