
Abstract
Background
We conducted a systematic review and meta-analysis to summarize the available literature and comprehensively appraise the renal profiles of sodium-glucose cotransporter 2 inhibitors (SGLT2i) in Japanese patients with type 2 diabetes mellitus (T2DM).
Methods
The electronic databases MEDLINE, Ichushi-web, and ClinicalTrials.gov were searched for studies without language restrictions from their inception until 20 July 2023 and CENTRAL until 21 September 2021. Studies were included if they were double-masked randomized controlled trials (RCTs) (1) including Japanese patients with T2DM aged > 18 years who received SGLT2i or a placebo, (2) reporting at least one renal outcome of serum creatinine or the estimated glomerular filtration rate (eGFR), and (3) with a follow-up of > 12 weeks. Cross-over and open label trials were excluded. The risk of bias based on the Cochrane risk-of-bias tool for randomized trials (RoB 2) was appraised. We computed the weighed mean difference with 95%CI for each renal outcome and used a random-effects model (inverse variance method).
Results
We ultimately retrieved 13 RCTs including 2687 individuals in our review. The durations of RCTs ranged between 12 and 104 weeks. Only one trial had a longer duration of more than one year. Ten out of 13 RCTs reported serum creatinine, while nine included eGFR. Serum creatinine and eGFR were slightly worse with SGLT2i than with a placebo [mean difference 0.01 (95%CI 0.00 to 0.02) mg/dL, p = 0.002, mean difference − 1.30 (95%CI -2.23 to -0.37) mL/min/1.73 m2, p = 0.006, respectively]. Merged results revealed insignificant heterogeneity (I2 < 30%).
Conclusion
These results suggest that SGLT2i slightly worsens serum creatinine and eGFR in Japanese patients with T2DM. However, since the durations of most RCTs were short, the effects of eGFR in particular may be transient. Further evidence is needed from rigorous studies that focus on renal outcomes with a longer duration to confirm the present results.
Similar content being viewed by others

Background
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) were developed as a glucose-lowering medication that inhibits glucose reabsorption in proximal tubules and increases urinary glucose excretion. Large trials demonstrated that SGLT2i, such as empagliflozin (EMPA), canagliflozin (CANA), and dapagliflozin (DAPA), exerted reno-protective effects in patients with type 2 diabetes mellitus (T2DM) [1,2,3].
In contrast, meta-analyses of patients with T2DM showed no significant differences in the estimated glomerular filtration rate (eGFR) between SGLT2i and a control or placebo [4,5,6]. However, these studies were consistently affected by statistical heterogeneity and had a broad population in terms of participants. Furthermore, the large trials described above had racial diversity, including > 50% Caucasians [1,2,3]. Additionally, a recent meta-analysis of 14 randomized controlled trials (RCTs) including Asian populations with T2DM showed that SGLT2i reduced eGFR and serum creatinine (SCr) [7]. One cohort study on SGLT2i users demonstrated that Black race was associated with an increased risk of eGFR dipping [8]. Based on these findings, it currently remains unclear whether renal profiles in patients with T2DM receiving SGLT2i are dependent on racial differences. Moreover, to the best of our knowledge, meta-analyses have not yet examined the renal effects of SGLT2i in a population restricted to Japanese patients with T2DM. Therefore, the aims of our systematic review and meta-analysis were to summarize the available literature and comprehensively appraise the renal profiles of SGLT2i in Japanese patients with T2DM.
Methods
The protocol was not prepared. We followed the PRISMA 2020 statement and submitted check lists [9] (Additional file 1).
Search strategies
We searched MEDLINE, Ichushi-web, and ClinicalTrial.gov from their inception to 20 July 2023 and Cochrane Central Register of Controlled Trials (CENTRAL) until 21 September 2021. We also collected information on six SGLT2i that have been approved in Japan: CANA, DAPA, EMPA, ipragliflozin (IPRA), luseogliflozin (LUSEO), and tofogliflozin (TOFO). Individual SGLT2i names, alternative names, and “SGLT2 inhibitors” were used as search terms (Additional file 2). Our search of these databases was restricted to “randomized controlled trials”. We did not use a language filter. We also used the advanced search mode of ClinicalTrial.gov in terms of an age older than 18 years using each SGLT2i name, type 2 diabetes, and Japan as the key words. At least two assessors (YS and JM or NO and JM in a team) independently undertook the literature search. Any discrepancies were settled through discussions between assessors. A reference search was also performed to identify more RCTs based on the studies retrieved where appropriate.
Data collection
Studies were included if they were double-masked RCTs (1) including Japanese patients with T2DM older than 18 years who received SGLT2i or a placebo, (2) reporting at least one renal outcome of our interest: SCr, eGFR, and the percentage of subjects showing a decline in eGFR from baseline as renal dysfunction [10], and (3) with a follow-up of > 12 weeks. Cross-over studies, open-label studies, RCTs without information on race/ethnicity, RCTs involving healthy participants, and trial registries with no results posted were excluded from our review. Data were also collected on concomitant medication, subtypes of SGLT2i, daily doses of SGLT2i, the number of participants, the dropout rate during the double-blind period, trial durations for the double-blind period, age, HbA1c, body mass index (BMI), eGFR at baseline, and the presence or absence of cardiac disease. We described insufficient information in RCTs as unclear. The first reviewer (JM) extracted data. The second reviewer (NO) then carefully rechecked the data.
Endpoint
eGFR was the primary endpoint and SCr was the secondary endpoint.
Assessment of the risk of bias
Two assessors (NO and JM) independently appraised the risk of bias based on the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) [11]. Any discrepancies were also resolved through discussions between assessors. Five domains for the risk of bias were as follows: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. Each domain was labeled as a “low risk of bias”, “some concerns”, or a “high risk of bias”.
Data synthesis
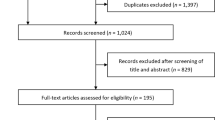
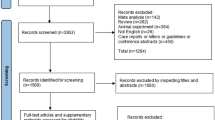
The first reviewer (JM) extracted changes from the baseline data of SCr and eGFR in both the intervention and placebo arms for the double-blind period using a spreadsheet; in instances where changes for the standard deviation were not reported directly (e.g., standard error of a mean or confidence interval (CI) for a mean), they were converted to the standard deviation for a mean using Review Manager 5.4.1 software (The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). If the least squares mean was used in each RCT, we considered the value to be a mean. A RCT with insufficient data for analysis was excluded; for example, the number of subjects analyzed was unclear or the change from baseline data was not reported directly (Fig. 1). Multiple SGLT2i arms in a single RCT were combined into a single arm [12]. The second reviewer (NO) then carefully rechecked the data. In the meta-analysis, we computed the weighed mean difference (MD) with 95%CI for each renal outcome. The heterogeneity of each outcome was evaluated using chi-squared and I-squared statistics. A value of 40% or more represented marked heterogeneity [12]. We used a random-effects model (inverse variance method) to provide a conservative estimate. We depicted a forest plot for each outcome. Three post-hoc subgroup analyses were performed by including patients with T2DM and renal impairment only, with T2DM and normal renal function only, and those treated with SGLT2i as monotherapy only. We drew a funnel plot and used Egger’s test to assess the publication bias for each renal outcome. All statistical analyses were performed with Review Manager 5.4.1 software and Stata/MP 17.0 version (Stata Corp, College Station, TX, USA). A P value < 0.05 was considered to be significant. The certainty of a body of evidence was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Evidence was rated as high, moderate, low, or very low.

PRISMA2020 flow diagram
Results
Among 1740 studies in the database search, 252 full texts and 58 trials registries were retrieved after the removal of duplicates and the screening of titles and abstracts. We ultimately included 13 RCTs in our systematic review. Figure 1 shows the process used to identify eligible RCTs [10, 13,14,15,16,17,18,19,20,21,22,23,24] following a PRISMA 2020 flow diagram [9]. Table 1 shows the characteristics of RCTs included in the review. Four types of SGLT2i were collected: CANA, IPRA, LUSEO, and TOFO. DAPA and EMPA studies were not retrieved in our review process because they did not meet our criteria. The durations of RCTs ranged between 12 and 104 weeks. Among 13 RCTs, three included patients with T2DM and renal impairment [10, 15, 16]. All trials were published in English.
Quality assessment of each RCT
We assessed the risk of bias of RCTs based on RoB 2 [11]. The majority of studies were judged as having a “high risk of bias”. A “low risk of bias” was the highest in the domain of the measurement of the outcome. “Some concerns” was the highest in the domain of the selection of the reported result. A “high risk of bias” was the highest in the domains of missing outcome data (Figs. 2 and 3).

Risk of bias assessment using Version 2 of the Cochrane risk-of-bias tool for randomized trials

Risk of bias in individual studies
SCr
Among 13 studies, 10 RCTs were included in the meta-analysis. No heterogeneity was observed among RCTs (I2 = 20%). SCr values were slightly worse with SGLT2i than with a placebo [MD 0.01 (95%CI 0.00 to 0.02) mg/dL, p < 0.002], whereas no significant differences were noted in a sub-group analysis of all subtypes of SGLT2i (Fig. 4).

Forest plot for SCr. Abbreviations: SCr, serum creatinine; CANA, canagliflozin; IPRA, ipragliflozin; LUSEO, luseogliflozin; TOFO, tofogliflozin; SGLT2, sodium-glucose cotransporter 2
eGFR
Among 13 studies, nine RCTs were included in the meta-analysis. No heterogeneity was observed among RCTs (I2 = 28%). eGFR values were slightly worse with SGLT2i than with a placebo [MD -1.30 (95%CI -2.23 to -0.37) mL/min/1.73 m2, p = 0.006], and TOFO and CANA were not significant in the sub-group analysis (Fig. 5).

Forest plot for eGFR. Abbreviations: eGFR, estimated glomerular filtration rate; CANA, canagliflozin; IPRA, ipragliflozin; LUSEO, luseogliflozin; TOFO, tofogliflozin; SGLT2, sodium-glucose cotransporter 2
Incidence of a decline in eGFR from baseline
We were unable to combine data because only one study reported the incidence of a decline in eGFR [10].
Publication bias
A publication bias was not observed for SCr or eGFR (Additional files 3–4).
Additional analyses
The sub-group analysis of patients with T2DM and renal impairment only showed inconsistent main outcomes. The effect size of SCr among patients with T2DM and renal impairment only was greater than those with T2DM and normal renal function only. The effect size of eGFR among patients with T2DM and renal impairment only was smaller than those with T2DM and normal renal function only, but was not significant. The sub-group analysis including patients receiving SGLT2i monotherapy only was consistent with the main results (Table 2).
Evaluation for GRADE
We rated the certainty of evidence for SCr as low. We downgraded the SCr outcome because six studies had a high risk of bias in terms of missing outcome data or deviations from the intended interventions, and 95%CI was near to zero for imprecision. We rated the certainty of evidence for eGFR as moderate. We downgraded the eGFR outcome because seven studies had a high risk of bias in terms of missing outcome data or deviations from the intended interventions (Fig. 3, Additional file 5).
Discussion
We conducted a systematic review and meta-analysis to summarize the available literature and comprehensively appraise the renal profiles of SGLT2i in Japanese patients with T2DM. eGFR and Scr were slightly worse with SGLT2i than with a placebo. Merged results revealed insignificant heterogeneity (I2 < 30%).
Our analysis showed that SCr was significantly higher with SGLT2i than with a placebo; the results obtained on the subtypes of SGLT2i were not significant, whereas merged results on subtypes of SGLT2i were significant [MD 0.01 (95%CI 0.00 to 0.02) mg/dL, p < 0.002] (Fig. 4). The LUSEO or IPRA group with a larger sample size may have caused this result in the forest plot. However, this undesirable effect of SGLT2i may be negligible. A previous meta-analysis that included more than 50% of Japanese patients with T2DM without renal impairment who received SGLT2i showed no significant differences in SCr between SGLT2i and a placebo [5]. Furthermore, Inagaki et al. reported that an increase in SCr due to SGLT2i did not explain the attenuation of renal function because the change was not progressive and UACR did not increase with higher SCr [20]. Two previous meta-analyses of T2DM showed that UACR was consistently lower with SGLT2i than with a placebo [4, 6].
The present results revealed a significantly larger reduction in eGFR in the SGLT2i group than in the placebo group; however, our trial duration ranged between 12 and 104 weeks. SGLT2i has been shown to transiently decrease eGFR within the initial four weeks and thereafter return it to the baseline level, which is often referred to as the eGFR dip [1, 3, 25]. A previous meta-analysis that merged two large RCTs including patients with T2DM and chronic kidney disease showed that the decline in the eGFR slope (rate of change in eGFR from week four to the last measurement within a double-blind period) was slower with SGLT2i than with a placebo [2, 26, 27]. However, we were unable to combine eGFR at the initial dip because only one RCT conducted by Kashiwagi et al. presented both the mean and standard deviation of eGFR at the initial dip; the value of eGFR at week two in their study was the lowest at any timepoint measured throughout the treatment period [16]. Besides the short duration of the RCTs we observed, the different assessment time points of eGFR may explain the opposite result of a large RCT showing that SGLT2i administered for one year or longer to patients with T2DM slowed the reduction in eGFR more than a placebo: one large-scale RCT showed that eGFR at baseline in the SGLT2i arm declined within the first four weeks and then gradually recovered after four weeks, while the level of eGFR on SGLT2i was roughly matched with that of the placebo arm at 52 weeks [1]. Similarly, in one matched cohort study using a Japanese database that included patients with T2DM and with a median observation period of 17 months, the reduction in eGFR was slower with SGLT2i than with other glucose-lowering medications [28]. Therefore, more domestic RCTs with longer durations that evaluate eGFR over time are needed to verify the different findings obtained from Japanese populations. One large-scale longitudinal study reported that the rate of the annual decline in eGFR among a general Japanese population was 0.36 mL/min/1.73 m2/year [29]. The impact of eGFR in the present analysis may have been transient and the annual decline in eGFR may also partially account for the results obtained. A pooled analysis consisting of four phase 3 studies that included Japanese individuals with a mean HbA1c of 7.8% also showed that an acute decline in eGFR after the initiation of SGLT2i was inversely associated with age, BMI, and eGFR at baseline [30]. Furthermore, a similar result for eGFR was observed in chronic kidney disease patients without diabetes [31]. Therefore, an acute change in eGFR among patients with these characteristics needs to be closely monitored in the early stage after initiating SGLT2i, and recovery from the eGFR dip needs to be confirmed.
Our sub-analysis suggested that the impact of SGLT2i on eGFR was weak among Japanese patients with T2DM and renal impairment [MD -1.00 (95%CI -3.04 to 1.03) mL/min/1.73 m2]. Consistently, this parameter may return to baseline values over time even in the presence of CKD [3, 32]. Furthermore, when the RCT with a longer follow-up period of 104 weeks was excluded [10], our results on the overall population revealed a more negative impact on eGFR: the eGFR value was worse with SGLT2i than with a placebo [MD -1.64 (95%CI -2.47 to -0.81) mL/min/1.73 m2]. The CANVAS study, which included approximately 80% Caucasians, showed that eGFR gradually recovered over several years irrespective of mean eGFR at baseline [33]. Additionally, the percentage of eGFR non-dippers receiving SGLT2i was similar between a Japanese population and EMPA-REG OUTCOME, including approximately 70% Caucasians; however, BMI was lower in the Japanese population than in the Caucasians [25, 30]. Therefore, race/ethnicity may not have an impact on changes in eGFR in a sufficient time window.
The present study has a number of strengths. To the best of our knowledge, this is the first systematic literature review and meta-analysis to summarize the available literature and comprehensively appraise the renal profiles of SGLT2i in Japanese patients with T2DM. Additionally, our merged outcomes consistently had acceptable heterogeneity (I2 < 30%). However, the present study also had several limitations. Therefore, the present results need to be interpreted with caution. There was a likelihood of a publication bias because we mostly identified published data. Another limitation is that not all of the RCTs collected set the outcomes of our interest as the primary outcome, and the majority of RCTs were judged as a “high risk of bias”, as described above. Furthermore, DAPA and EMPA, which exert reno-protective effects, were not included in the present analysis, which may have led to an under- or overestimation. Our study had limited information on dipeptidyl peptidase 4 inhibitors, which have the highest prescription rate as a first-line treatment for T2DM in Japan [34], or on renin–angiotensin system inhibitors, which exert reno-protective effects [35]. Moreover, an elderly population as one of the risk factors associated with chronic kidney disease was not included in our analysis [36]. This information is needed to verify the present results for their use in future studies. Another limitation was that neither SCr nor eGFR may have been accurate because we treated the least squares mean as the mean; however, we confirmed that similar results were obtained when these RCTs were excluded [10, 22,23,24]. Moreover, the present study may not truly reflect current clinical settings because the RCTs analyzed included highly selective populations that were rigorously controlled. Therefore, real-world evidence from diverse conditions is needed to confirm the present results.
Conclusion
The present study, which included Japanese patients with T2DM only, suggests that SCr and eGFR were slightly worse with SGLT2i than with a placebo. There was also no important heterogeneity. However, since the durations of the RCTs included were mostly short, the effects of eGFR in particular may be transient. Further evidence is needed from rigorous studies that focus on renal outcomes for a longer duration and involve subtypes, such as DAPA and EMPA, to confirm the present results.
Data Availability
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- CANA:
-
Canagliflozin
- LUSEO:
-
Luseogliflozin
- IPRA:
-
Ipragliflozin
- TOFO:
-
Tofogliflozin
- SGLT2i:
-
Sodium-glucose co-transporter 2 inhibitor
- eGFR:
-
Estimated glomerular filtration rate
- SCr:
-
Serum creatinine
- MD:
-
Weighted mean difference
- T2DM:
-
Type 2 diabetes mellitus
- RCTs:
-
Randomized controlled trials
- BMI:
-
Body mass index
- RoB 2:
-
The Revised Cochrane risk-of-bias tool for randomized trials
References
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, Johansen OE, Woerle HJ, Broedl UC, Zinman B. EMPA-REG OUTCOME investigators. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375:323–34. https://doi.org/10.1056/NEJMoa1515920.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR, CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377:644–57. https://doi.org/10.1056/NEJMoa1611925.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, Mann JFE, McMurray JJV, Lindberg M, Rossing P, Sjöström CD, Toto RD, Langkilde AM, Wheeler DC. DAPA-CKD trial committees and investigators. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383:1436–46. https://doi.org/10.1056/NEJMoa2024816.
Feng C, Wu M, Chen Z, Yu X, Nie Z, Zhao Y, Bao B. Effect of SGLT2 inhibitor on renal function in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Int Urol Nephrol. 2019;51:655–69. https://doi.org/10.1007/s11255-019-02112-6.
Seidu S, Kunutsor SK, Cos X, Gillani S, Khunti K, For, on behalf of Primary Care Diabetes Europe. SGLT2 inhibitors and renal outcomes in type 2 diabetes with or without renal impairment: a systematic review and meta-analysis. Prim Care Diabetes. 2018;12:265–83. https://doi.org/10.1016/j.pcd.2018.02.001.
Bae JH, Park EG, Kim S, Kim SG, Hahn S, Kim NH. Effects of Sodium-Glucose cotransporter 2 inhibitors on renal outcomes in patients with type 2 diabetes: a systematic review and Meta-analysis of Randomized controlled trials. Sci Rep. 2019;9:13009. https://doi.org/10.1038/s41598-019-49525-y.
Zhao SD, Zhou L, Tao YY, Yue Y, Wang JX, Shen L, Lu GY, Hang YF. Renal outcomes in asian patients with type 2 diabetes mellitus treated with SGLT2 inhibitors: a systematic review and meta-analysis of randomized controlled trials. Int J Diabetes Dev Ctries. 2022;42:178–90. https://doi.org/10.1007/s13410-021-00999-5.
Xie Y, Bowe B, Gibson AK, McGill JB, Maddukuri G, Al-Aly Z. Clinical implications of estimated glomerular filtration rate Dip following sodium-glucose Cotransporter-2 inhibitor initiation on Cardiovascular and kidney outcomes. J Am Heart Assoc. 2021;10:e020237. https://doi.org/10.1161/JAHA.120.020237.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Wada T, Mori-Anai K, Takahashi A, Matsui T, Inagaki M, Iida M, Maruyama K, Tsuda H. Effect of canagliflozin on the decline of estimated glomerular filtration rate in chronic kidney disease patients with type 2 diabetes mellitus: a multicenter, randomized, double-blind, placebo-controlled, parallel-group, phase III study in Japan. J Diabetes Investig. 2022;13:1981–9. https://doi.org/10.1111/jdi.13888.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook. Accessed 9 May 2023.
Kaku K, Kadowaki T, Seino Y, Okamoto T, Shirakawa M, Sato A, O’Neill EA, Engel SS, Kaufman KD. Efficacy and safety of ipragliflozin in japanese patients with type 2 diabetes and inadequate glycaemic control on sitagliptin. Diabetes Obes Metab. 2021;23:2099–108. https://doi.org/10.1111/dom.14448.
Seino Y, Sasaki T, Fukatsu A, Imazeki H, Ochiai H, Sakai S. Efficacy and safety of luseogliflozin added to insulin therapy in japanese patients with type 2 diabetes: a multicenter, 52-week, clinical study with a 16-week, double-blind period and a 36-week, open-label period. Curr Med Res Opin. 2018;34:981–94. https://doi.org/10.1080/03007995.2018.1441816.
Haneda M, Seino Y, Inagaki N, Kaku K, Sasaki T, Fukatsu A, Kakiuchi H, Sato Y, Sakai S, Samukawa Y. Influence of renal function on the 52-Week efficacy and safety of the Sodium glucose cotransporter 2 inhibitor luseogliflozin in japanese patients with type 2 diabetes Mellitus. Clin Ther. 2016;38:66–88e20. https://doi.org/10.1016/j.clinthera.2015.10.025.
Kashiwagi A, Takahashi H, Ishikawa H, Yoshida S, Kazuta K, Utsuno A, Ueyama E. A randomized, double-blind, placebo-controlled study on long-term efficacy and safety of ipragliflozin treatment in patients with type 2 diabetes mellitus and renal impairment: results of the long-term ASP1941 safety evaluation in patients with type 2 diabetes with renal impairment (LANTERN) study. Diabetes Obes Metab. 2015;17:152–60. https://doi.org/10.1111/dom.12403.
Kashiwagi A, Akiyama N, Shiga T, et al. Efficacy and safety of ipragliflozin as an add-on to a sulfonylurea in japanese patients with inadequately controlled type 2 diabetes: results of the randomized, placebo-controlled, double-blind, phase III EMIT study. Diabetol Int. 2015;6:125–38. https://doi.org/10.1007/s13340-014-0184-9.
Kashiwagi A, Shiga T, Akiyama N, et al. Efficacy and safety of ipragliflozin as an add-on to pioglitazone in japanese patients with inadequately controlled type 2 diabetes: a randomized, double-blind, placebo-controlled study (the SPOTLIGHT study). Diabetol Int. 2015;6:104–16. https://doi.org/10.1007/s13340-014-0182-y.
Kashiwagi A, Kazuta K, Takinami, et al. Ipragliflozin improves glycemic control in japanese patients with type 2 diabetes mellitus: the BRIGHTEN study. Diabetol Int. 2015;6:8–18. https://doi.org/10.1007/s13340-014-0164-0.
Inagaki N, Kondo K, Yoshinari T, Takahashi N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin monotherapy in japanese patients with type 2 diabetes inadequately controlled with diet and exercise: a 24-week, randomized, double-blind, placebo-controlled, phase III study. Expert Opin Pharmacother. 2014;15:1501–15. https://doi.org/10.1517/14656566.2014.935764.
Kaku K, Watada H, Iwamoto Y, Utsunomiya K, Terauchi Y, Tobe K, Tanizawa Y, Araki E, Ueda M, Suganami H, Watanabe D, Tofogliflozin 003 Study Group. Efficacy and safety of monotherapy with the novel sodium/glucose cotransporter-2 inhibitor tofogliflozin in japanese patients with type 2 diabetes mellitus: a combined phase 2 and 3 randomized, placebo-controlled, double-blind, parallel-group comparative study. Cardiovasc Diabetol. 2014;13:65. https://doi.org/10.1186/1475-2840-13-65.
Seino Y, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Dose-finding study of luseogliflozin in japanese patients with type 2 diabetes mellitus: a 12-week, randomized, double-blind, placebo-controlled, phase II study. Curr Med Res Opin. 2014;30:1231–44. https://doi.org/10.1185/03007995.2014.909390.
Seino Y, Sasaki T, Fukatsu A, Sakai S, Samukawa Y. Efficacy and safety of luseogliflozin monotherapy in japanese patients with type 2 diabetes mellitus: a 12-week, randomized, placebo-controlled, phase II study. Curr Med Res Opin. 2014;30:1219–30. https://doi.org/10.1185/03007995.2014.901943.
Seino Y, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Efficacy and safety of luseogliflozin as monotherapy in japanese patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled, phase 3 study. Curr Med Res Opin. 2014;30:1245–55. https://doi.org/10.1185/03007995.2014.912983.
Kraus BJ, Weir MR, Bakris GL, Mattheus M, Cherney DZI, Sattar N, Heerspink HJL, Ritter I, von Eynatten M, Zinman B, Inzucchi SE, Wanner C, Koitka-Weber A. Characterization and implications of the initial estimated glomerular filtration rate ‘dip’ upon sodium-glucose cotransporter-2 inhibition with empagliflozin in the EMPA-REG OUTCOME trial. Kidney Int. 2021;99:750–62. https://doi.org/10.1016/j.kint.2020.10.031.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE. EMPA-REG OUTCOME investigators. Empagliflozin, Cardiovascular Outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–28. https://doi.org/10.1056/NEJMoa1504720.
Toyama T, Neuen BL, Jun M, Ohkuma T, Neal B, Jardine MJ, Heerspink HL, Wong MG, Ninomiya T, Wada T, Perkovic V. Effect of SGLT2 inhibitors on cardiovascular, renal and safety outcomes in patients with type 2 diabetes mellitus and chronic kidney disease: a systematic review and meta-analysis. Diabetes Obes Metab. 2019;2:1237–50. https://doi.org/10.1111/dom.13648.
Takeuchi M, Ogura M, Minoura T, Inagaki N, Kawakami K. Comparative effectiveness of sodium-glucose Cotransporter-2 inhibitors Versus other classes of glucose-lowering medications on renal outcome in type 2 diabetes. Mayo Clin Proc. 2020;95:265–73. https://doi.org/10.1016/j.mayocp.2019.12.004.
Imai E, Horio M, Yamagata K, Iseki K, Hara S, Ura N, Kiyohara Y, Makino H, Hishida A, Matsuo S. Slower decline of glomerular filtration rate in the japanese general population: a longitudinal 10-year follow-up study. Hypertens Res. 2008;31:433–41. https://doi.org/10.1291/hypres.31.433.
Kohagura K, Yamasaki H, Takano H, Ohya Y, Seino Y. Luseogliflozin, a sodium-glucose cotransporter 2 inhibitor, preserves renal function irrespective of acute changes in the estimated glomerular filtration rate in japanese patients with type 2 diabetes. Hypertens Res. 2020;43:876–83. https://doi.org/10.1038/s41440-020-0426-0.
Shibata R, Taguchi K, Kaida Y, Fukami K. Effect of dapagliflozin on the initial estimated glomerular filtration rate dip in chronic kidney disease patients without diabetes mellitus. Clin Exp Nephrol. 2023;27:44–53. https://doi.org/10.1007/s10157-022-02277-y.
Yale JF, Bakris G, Cariou B, Yue D, David-Neto E, Xi L, Figueroa K, Wajs E, Usiskin K, Meininger G. Efficacy and safety of canagliflozin in subjects with type 2 diabetes and chronic kidney disease. Diabetes Obes Metab. 2013;15:463–73. https://doi.org/10.1111/dom.12090.
Perkovic V, de Zeeuw D, Mahaffey KW, Fulcher G, Erondu N, Shaw W, Barrett TD, Weidner-Wells M, Deng H, Matthews DR, Neal B. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS Program randomised clinical trials. Lancet Diabetes Endocrinol. 2018;6:691–704. https://doi.org/10.1016/S2213-8587(18)30141-4.
Bouchi R, Sugiyama T, Goto A, Imai K, Ihana-Sugiyama N, Ohsugi M, Yamauchi T, Kadowaki T, Ueki K. Retrospective nationwide study on the trends in first-line antidiabetic medication for patients with type 2 diabetes in Japan. J Diabetes Investig. 2022;13:280–91. https://doi.org/10.1111/jdi.13636.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S. RENAAL Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861–9. https://doi.org/10.1056/NEJMoa011161.
Imai E, Horio M, Iseki K, Yamagata K, Watanabe T, Hara S, Ura N, Kiyohara Y, Hirakata H, Moriyama T, Ando Y, Nitta K, Inaguma D, Narita I, Iso H, Wakai K, Yasuda Y, Tsukamoto Y, Ito S, Makino H, Hishida A, Matsuo S. Prevalence of chronic kidney disease (CKD) in the japanese general population predicted by the MDRD equation modified by a japanese coefficient. Clin Exp Nephrol. 2007;11:156–63. https://doi.org/10.1007/s10157-007-0463-x.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
Author contributions: JM had full access to all the data in the present study. JM conceived and designed the study. JM, NO, and YS performed the systematic review of the literature. JM and NO conducted the risk of bias assessment. JM and NO curated the data. JM analyzed and interpreted the data. JM wrote the manuscript. RK contributed to manuscript revisions for intellectual content. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mukai, J., Okamura, N., Saito, Y. et al. A systematic review of sodium-glucose cotransporter 2 inhibitors and renal profiles among Japanese patients with type 2 diabetes mellitus. J Pharm Health Care Sci 9, 36 (2023). https://doi.org/10.1186/s40780-023-00305-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40780-023-00305-x