
Abstract
Background
Systematic evaluation of the successful heartbeat recovery rate (HRR) in patients during the platinum ten minutes after cardiac arrest.
Methods
The databases of CNKI (January 1979–March 2019), Chongqing VIP (January 1989–March 2019), Wanfang (January 1990–March 2019) and Web of Science (1900-May 2020) were searched. To collect the clinical data of patients with cardiac arrest before hospitalization and analyze the cardiopulmonary resuscitation (CPR) at different times. Literature selection and data extraction were carried out by two researchers independently, and the meta package of R software (version 3. 61) was used for analysis.
Results
A total of 116 papers met the inclusion criteria, including 37,181 patients. Of these patients, 3367 had their heartbeats successfully restored. The results showed a high degree of heterogeneity (χ2 = 6999.21, P < 0.01, I2 = 97.6%). The meta-analysis was conducted using a random-effects model. The combined effect size was 0.199 (0.157–0.250). (1) According to the five CPR groups (International Cardiopulmonary Resuscitation Guide 2000, 2005, 2010, 2015 and other versions), the HRR of other versions [0.264 (0.176–0.375)] was higher than the International Cardiopulmonary Resuscitation 2005 edition [0.121 (0.092–0.158)]. (2) The rescue time was divided into the 0 to ≤5 min group, the 5 to ≤10 min group, the 10 to ≤15 min group, and the > 15 min group. The HRR were 0.417 (0.341–0.496), 0.143 (0.104–0.193), 0.049 (0.034–0.069), and 0.022 (0.009–0.051), respectively. The HRR was higher in the 0 to ≤5 min group than in the 5 to ≤10 min group, the 10 to ≤15 min group and the > 15 min group. There was no difference between the 10 to ≤15 min group and the > 15 min group. (3) When the groups were stratified with the cutoff of 10 min, the ≤10 min group HRR [0.250 (0.202–0.306)] was higher than the > 10 min group rate [0.041 (0.029–0.057)]. (4) The HRR of the telephone guidance group was [0.273 (0.227–0.325)] lower than that of the 0 to ≤5 min group [0.429 (0.347–0.516)] but higher than that of the 5 to ≤10 min group, the 10 to ≤15 min group, and the > 15 min group. (5) The HRR of the witness group [0.325 (0.216–0.458)] was not different from that of the 0 to ≤5 min group, but it was higher than those of the 5 to ≤10 min group, the 10 to ≤15 min group and the > 15 min group. (6) There was no significant difference HRR between the witnessed group, the telephone guidance group and the ≤10 min group.
Conclusions
(1) The HRR is time-sensitive, and early rescue can improve it. (2) CPR performed within the platinum ten minutes must be executed by the public, and other forces are auxiliary. (3) The concept of peri-cardiac arrest period (PCAP) should be established and improved to guide CPR.
Similar content being viewed by others


Background
Cardiopulmonary resuscitation (CPR) is an important measure used to restore a heartbeat in patients with cardiopulmonary arrest. It is very useful for gaining treatment time and saving patients’ lives. The number of cardiac arrests in the world is as high as 800–900 million per year [1], and approximately 70% of patients experience cardiac arrest before arriving at a hospital. The number of sudden deaths in China is 1 million per year [2], but the rate of prehospital heartbeat recovery in out-of-hospital cardiac arrest patients is only 17.1% [3], which is lower than in developed countries. Thus, the author proposes the concepts of “peri-sudden death period (PSDP)” and “peri-cardiac arrest period (PCAP)” to guide the public in preventing and responding to cardiopulmonary arrest [4]. In first-aid, the platinum 10 min refers to the time-saving principle and first-aid theory of treatment after accidental injury; in the first 10 min, the professionals cannot reach the patient, but it is the most critical time to receive treatment. This stage is the key link with the “120″ emergency system, and it includes CPR, remove airway foreign body, defibrillation, and stopping bleeding. It is necessary to propagate the first-aid knowledge and skills such as airway asphyxia from the start of the witness. The PSDP is the most important part of the study. The National Self-help and Rescue Volunteer Service Alliance conducts a meta-analysis of the success rate of heartbeat recovery in patients with prehospital cardiac arrest in China every 5 years to assess and improve the status of prehospital or public CPR.
Methods
Inclusion and exclusion criteria
CPR patients rescued by different international versions of guidelines. Study type: Retrospective case summary and analysis; Language limit: Chinese; Study object: CPR patients with cardiac arrest caused by various diseases before hospital; patients with CPR have definite time in different stages and CPR recovery. The results showed that the patients had spontaneous rhythm and pulse recovery. Exclusion criteria: Literature exclusion of patients without event occurrence time, repetition, unreported data and number of patients ≤10.
Retrieval strategy
The computer searches the CNKI (January 1979–March 2019), Wanfang database (January 1990–March 2019), Chongqing VIP database (January 1989–March 2019), and Web of Science (1900-May 2020). The search terms are title, title or theme, including “心跳骤停+院前+中国(cardiac arrest + out of hospital + China)”, and“心肺复苏+院前+中国 (CPR +out of hospital+ 中国)”.
Paper screening, data extraction, and quality evaluation
Select the documents according to the pre-determined inclusion and exclusion labels. Two researchers read the titles and abstracts of the obtained documents independently. After excluding the documents that clearly do not meet the inclusion criteria, further read the full text of the documents that may meet the inclusion criteria to determine whether they meet the inclusion criteria. In case of any disagreement, it shall be discussed or submitted to a third party for adjudication. The contents of the literature must include: (1) general information: title, author, date of publication and source of the literature; (2) research features: whether there is CPR rescue time and rescue has a clear number of people and deaths; (3) clinical outcome indicators include one of the following indicators: Patients have pulse recovery, spontaneous breathing recovery, consciousness recovery and discharge data.
Statistical analyses
Analyses were conducted using R Meta package software (version 3.61). The χ2 test was used to test the heterogeneity of the data. P > 0.05 denoted no significant heterogeneity in the dependent variables. A meta-analysis was conducted using a fixed-effects model. P < 0.05 denoted heterogeneity in the dependent variables. A random-effects model can be used when heterogeneity remains after controlling for it and the combined data continue to have clinical significance [5]. The I2 statistic was used to reflect the magnitude of the heterogeneity of the combined effect. Larger I2 values denote greater heterogeneity. If I2 < 25%, then mild heterogeneity exists across the studies. If 25% < I2 < 75%, then moderate heterogeneity exists across the studies. If I2 > 75%, then a high degree of heterogeneity exists across the studies. A funnel plot was used to estimate the publication bias. A two-sided test was used when a need existed to test the above statistical analyses. The significance level was set at 0.05.
Results
Literature retrieval
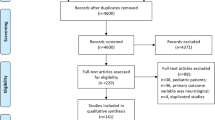
A total of 699 relevant papers were initially retrieved. After screening the papers, 116 papers were included in the final analysis [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121]. A total of 37,181 patients were included in these 116 papers. Figure 1 shows a flow chart of the literature screening process.

Flowchart of literature screening process
General information of the papers
In total, 116 papers met the inclusion criteria, containing 37,181 patients. Of these patients, the heartbeats of 3367 patients were restored. The results of the heterogeneity test (χ2 = 6999.21, P < 0.01, I2 = 97.6%) indicated a high degree of heterogeneity. A meta-analysis was conducted using a random-effects model. The combined effect size was 0.199 (0.157–0.250; Fig. 2). The publication bias test was performed with the Egger test (t = 1.3718, p = 0.1728). The results showed that the articles did not have publication bias (Fig. 3).

CPR success rates

Funnel plot of the publication bias
CPR was performed using the methods provided by different guidelines
The different rescue programs used in the included studies were the International Cardiopulmonary Resuscitation Guide 2000、2005、2010、2015 Edition and other guidelines. Among these, The International Cardiopulmonary Resuscitation 2000 edition was used in 9 articles, 2005 edition was used in 20 articles, 2010 edition was used in 26 articles, 2015 edition was used in 8 articles, and other guidelines were used in 53 articles. The results show that HRR [0.121 (0.092–0.158)] when the 2005 guidelines were used was significantly different from that when other versions of the guidelines were used [0.264 (0.176–0.375)]. There was no significant difference with other CPR versions (as shown in Fig. 4). Since the literatures included in other editions have reported more successful heartbeat recovery results, the results of the 2005 edition included in the publication bias were less, resulting in differences in the HRR. There may not be a difference. The HRR is not related to the version of the guidelines used for CPR. Timeliness is the key to the success rate. The results are shown in Table 1.

Comparisons of the HRR using the methods provided in the different guidelines
Time-dependent conditions of CPR
Patients were divided into the 0 to ≤5 min group, 5 to ≤10 min group, 10 to ≤15 min group, and > 15 min group according to different CPR initiation times. According to the times recorded in the studies, 58 were included in the 0 to ≤5 min group, 66 in the 5 to ≤10 min group, 49 in the 10 to ≤15 min group, and 16 in the > 15 min group. Results: The 0 to ≤5 min group HRR [0.417 (0.341–0.496)] was higher than those of the 5 to ≤10 min group [0.143 (0.104–0.193)], the 10 to ≤15 min group [0.049 (0.034–0.069)] and the > 15 min group [0.022 (0.009–0.051)]. The 5 to ≤10 min group HRR [0.143 (0.104–0.193)] was higher than those of the 10 to ≤15 min group [0.049 (0.034–0.069)] and the > 15 min group [0.022 (0.009–0.051)]. There was no different in the HRR between the 10 to ≤15 min group and the > 15 min group. The results show that with the prolongation of the duration before the initiation of CPR, the survival rate decreases. The results are shown in Fig. 5 and Table 2.

Comparison of the CPR success rates at different times
According to the different CPR initiation times, the two groups were the ≤10 min group and the > 10 min group. According to the recorded times in the studies, 124 articles were included in the ≤10 min group, and 65 articles were in the > 10 min group. The ≤10 min group HRR [0.250 (0.202–0.306)] was higher than the > 10 min group HRR [0.041 (0.029–0.057)]. The results are shown in Fig. 6 and Table 3.

The HRR for the ≤10 min and > 10 min groups
According to whether telephone guidance for first aid was provided, the groups in the comparative analysis were the telephone instruction group, 0 to ≤5 min group, 5 to ≤10 min group, 10 to ≤15 min group and > 15 min group. Telephone guidance was provided in 5 articles, while there were 53 in the 0 to ≤5 min group, 66 in the 5 to ≤10 min group, 49 in the 10 to ≤15 min group, and 16 in the > 15 min group. The HRR of the telephone guidance group was [0.273 (0.227–0.325)] less than that of the 0 to ≤5 min group [0.429 (0.347–0.516)] but higher than those of the 5 to ≤10 min group [0.143 (0.104–0.193)], the 10 to ≤15 min group [0.049 (0.034–0.069)] and the > 15 min group [0.022 (0.009–0.051)]. The results are shown in Table 4 and Fig. 7.

The HRR of the telephone guidance group and the other groups at different times
According to the presence or absence of witnesses, the patients were divided into the witness + public group, the 0 to ≤5 min group, the 5 to ≤10 min group, the 10 to ≤15 min group, and the > 15 min group for a comparative analysis. There were 11 articles included in the witness + public group, 47 in the 0 to ≤5 min group, 66 in the 5 to ≤10 min group, 49 in the 10 to ≤15 min group, and 16 in the > 15 min group. Results: The HRR of the witness + public group [0.325 (0.216–0.458)] was not different from that of the 0 to ≤5 min group [0.439 (0.351–0.533)], but it was higher than those in the 5 to ≤10 min group [0.143 (0.104–0.193)], the 10 to ≤15 min group [0.049 (0.034–0.069)] and the > 15 min group [0.022 (0.009–0.051)]. The results are shown in Table 5 and Fig. 8.

The HRR of the witness + public group and other groups at different times
The witness + public group, telephone guidance group and ≤ 10 min group were compared. In total, 11 articles were included in the witness + public group, 5 in the telephone guidance group, and 108 in the ≤10 min group. The results show that the HRR of the witness + public group was 0.325 (0.216–0.458), and the HRR of the telephone guidance group was 0.273 (0.227–0.325), while the ≤10 min group HRR was 0.240 (0.188–0.302). There were no significant differences among the three groups, as shown in Table 6 and Fig. 9.

The HRR of the witness +public group, telephone guidance group and ≤ 10 min group
Discussion
Cardiac arrest is the most critical condition in the clinic, and patients can obtain a better recovery if they receive effective CPR immediately. The overall prognosis of patients with cardiac arrest outside the hospital is currently poor. According to the American Heart Association, there were approximately 360,000 out-of-hospital cardiac arrest patients in the United States in 2016, and the discharge rate was only 10.6% [122]. The out-of-hospital survival rate of out-of-hospital cardiac arrest in the Asia-Pacific region ranges from 0.8 to 9.0% [123]. Due to the limitations of the studies in this analysis and the analysis of other aspects of CPR, we used concept of the platinum ten minutes to investigate CPR in China. Extracting the single clinical index of the earliest recovered heartbeat during CPR to analyze early CPR can reflect the state of CPR in China to some extent. There were 116 articles that met the inclusion criteria, with a total of 37,181 patients, and the number of patients with recovered heartbeats was 3367, with a heartbeat recovery success rate of 19.9%.
The limitations of this study are as follows: (1) This study included 116 articles, all of which were retrospective observational studies. The quality of the clinical data varied substantially, and it was impossible to evaluate the comprehensive cardiopulmonary cerebral resuscitation of the heartbeat, respiration, brain function and vital status. (2) The numbers of papers in the telephone guidance and the witness + public groups were small, and more studies need to be performed. (3) When fewer than 10 patients were discussed in an article, that article was excluded from this analysis. Despite these limitations, this study can still provide us with useful guidance.
Version comparison: In articles using the five different versions of the CPR guidelines (The International Cardiopulmonary Resuscitation Guide 2000, 2005, 2010, 2015 and other guidelines), the HRR rates were 20.2, 12.1, 16.9, 20.4, and 26.4%, respectively. Among the different guidelines used, the HRR was different when the 2005 edition was used than when other editions were used. Studies using editions other than the 2005 guidelines reported more success in terms of heartbeat recovery, with publication biases, while the articles using the 2005 edition showed less publication bias, resulting in differences in the HRR. The HRR has nothing to do with the guideline version of CPR, and timeliness is the key to its success rate.
Timeliness analysis
The CPR initiation time was divided into 0 to ≤5 min, 5 to ≤10 min, 10 to ≤15, and > 15 min. The HRR were 41.7, 14.3, 4.9 and 2.2%, respectively. The 0 to ≤5 min group had a higher success rate than the other 3 groups, and the 5 to ≤10 min group had a higher success rate than the last 2 groups, while the 10 to ≤15 min group and the > 15 min group were not different from each other, indicating that the rescue survival rate decreased with the prolongation of the time to the initiation of CPR. The conclusion is the sooner CPR is started, the better [124]. For every minute CPR and defibrillation are delayed, the success rate is reduced by 7–10%. Therefore, they do not have the best aging platform, and there is no such rule of prime time [125].
Artificial differences
The HRR of the telephone guidance group and the witness + public group were 27.3 and 32.5%, respectively, and the rate in the telephone guidance group was less than that in the 0 to ≤5 min group. There was no difference between the HRR between the witness + public group and the 0 to ≤5 min group, but both had rates that were higher than those in the last three time strata, indicating that they were superior. This is contrary to our expectations. To further support this conclusion, we need more detailed, accurate research.
Rescuer and time-effectiveness analysis
The HRR were different among the witness group (32.5%), telephone guidance group (27.3%) and ≤ 10 min group (24.0%). This order of success rates matches our expectation, although they are not significantly different. It is possible that the numbers of studies included in the telephone guidance group and the witness group were small, and more studies with larger sample sizes should be conducted in the future. There is a significant difference in the HRR between the ≤10 min group (25.0%) and the > 10 min group (4.1%), suggesting that CPR should be performed within 10 min and that every minute counts in terms of improving the HRR; effective treatment greatly enhances the possibility of survival [126].
Public cardiopulmonary resuscitation(P-CPR) and telephone-guided CPR within the platinum ten minutes is the key to first aid. For the case of sudden cardiac arrest, it is difficult for emergency medical personnel to reach the emergency site in a short time. The best first aid can be provided by the injured person and any eyewitnesses. Timely self-help and rescue by witnesses can be valuable [127]. It may be that the number of articles included is small. We hope that the HRR of the telephone guidance group and the witness group will meet or exceed the HRR of the 0 to ≤5 min group.
In the article we published 5 years ago, the exclusion criteria were patients with repeated, unreported data and studies with fewer than 20 patients [3], while in this study, the exclusion criteria were duplicate patients, patients with unreported data and studies with fewer than 10 patients. The number of articles included in the study increased by 59, and the successful HRR increased from 17.1 to 19.9% [3], but the real-world HRR is still low. In the analysis of the different versions of the CPR guidelines, 8 articles used the 2015 edition, and the HRR was not significantly different from those in the articles using the other versions of the guidelines. Because the ≤1 min group would have had fewer articles and the time boundary was difficult to define, it was included in the 0 to ≤5 min group. Compared with the studies available 5 years ago, the number of studies in the witness + public and telephone guidance groups increased by 4 and 2, respectively, and CPR was shown to be time-sensitive. We should increase public awareness and make first aid technology available to the public. Only self-help and action on the part of witnesses can lead to a higher rescue success rate.
In previous studies, we found that in order to improve the success rate of cardiac arrest, we must change the node awareness of cardiac arrest to the process of understanding, and define the beginning and outcome of cardiac arrest as PCAP [4]. We can divide the clinical process of PCAP into three periods: pre-PCAP, mid-PCAP, and late-PCAP. When the patient has critical symptoms such as hypothermia, altered consciousness, abnormal breathing, abnormal heart rhythm, unstable blood pressure, oliguria or anuria, a hemoglobin level < 5 g, critical electrolyte values, or severe acidosis or when the patient shows further deterioration of the aforementioned conditions/symptoms and signs and is on the verge of respiratory and cardiac arrest, then the CPR process must be initiated. CPR measures must be taken until they are deemed ineffective and abandoned or stable circulation returns.
Conclusions
Therefore, we believe the following: (1) The successful HRR depends on the timeliness of the administration of treatment. When administered as soon as possible, CPR can improve the successful HRR. (2) The platinum ten minutes after cardiac arrest means it must be performed by the P-CPR, and other forces are auxiliary. (3) The concept of the heartbeat should be established to guide CPR. (4) Making CPR equipment more readily accessible to the public and improving the public’s awareness of the tools and techniques can improve the successful HRR because rescue strategies will be more likely to be initiated within the platinum ten minutes.
Availability of data and materials
Not applicable.
Abbreviations
- CPR:
-
Cardiopulmonary resuscitation
- HRR:
-
Heartbeat recovery rate
- P-CPR:
-
Public cardiopulmonary resuscitation
- PCAP:
-
Peri-cardiac arrest period
References
Zhang ZQ, Luo FT, Chen B, Chen F, GongBao CD, Huang L, et al. Epidemiological investigation and analysis of pre-hospital emergency in our eight large and medium-sized cities. Chin J Emerg Med. 2010;19(11):1130–6.
Mehra R. Global public health problem of sudden cardiac death. J Electrocardiol. 2007;40(6 suppl):S118–22.
Gu XM, Li ZH, He ZJ, Zhao ZW, Liu SQ. A meta-analysis of the success rates of heartbeat restoration within the platinum 10 min among outpatients suffering from sudden cardiac arrest in China. Mil Med Res. 2016;3(6):1–15.
He ZJ, Zhao ZW. The definition, staging and coping strategies of "public encirclement and death". Chin J Hygiene Rescue. 2018;4(6):75–8.
Zintzaras E, Ioannidis JPA. Hegesma: genome search meta-analysis and heterogeneity testing. Bioinformatics. 2005;21(18):3672–3.
Liu WM. The effect of pre-hospital cardiopulmonary rescue. In: Compilation of abstracts of the Third National Emergency Medicine Conference; 1990. p. 1.
Xu J, Gong XJ. Clinical analysis of cardiopulmonary resuscitation in 79 patients with pre-hospital cardiac arrest. J Clin Med Pract. 2016;20(24):15–9.
Li ZL, Yang JJ, Qu YH. Retrospective analysis of 96 cases of outpatient emergency cardiopulmonary resuscitation. Gansu Med J. 2015;34(8):590–2.
Zhao W. Pre-hospital first aid analysis of 113 patients with cardiac arrest. Chin J Trau Disabil Med. 2016;24(5):8–9.
Huang MH. 120 telephone guidance on the impact of the first witnesses on the scene of cardiopulmonary resuscitation on pre-hospital emergency cardiopulmonary resuscitation and patient prognosis. Health People. 2018;12(2):11–2.
Wang M. The role of nursing staff in pre-hospital emergency cardiopulmonary resuscitation. World Latest Med Inform. 2016;16(12):264–5.
Wang F, Yong YY, Xiang Y. Epidemiological study on pre-hospital rescue of 1696 patients with cardiac arrest in Utstein mode. Med Inform. 2015;28(52):126.
Ke D. Analysis of the effect of portable ventilator in pre-hospital emergency. Modern Diagn Treat. 2015;6:1409–10.
Su G, Ke D, Chen YM. Application and influence of different ventilation methods in patients with pre-hospital cardiac arrest. Chin J Modern Drug Appl. 2015;9(11):82–3.
Yao XL, Jin PY, Weng WF. Comparison of the effects of intubation type laryngeal mask and conventional resuscitation mask in pre-hospital first aid. J Nurs Rehabil. 2015;14(10):953–4.
Zhao HL. Successful rescue experience of 13 cases of cardiopulmonary resuscitation. Hebei Med. 2002;7(22):39–40.
Ye MZ, Qiu MF. Clinical analysis of prehospital cardiopulmonary resuscitation in 62 patients with sudden death. Clin Med. 2016;26:84.
Lu YB, Wei YF. Prehospital resuscitation of 38 patients with cardiac arrest caused by electric shock. J Youjiang Med Univ Natl. 2012;7:304.
Chen WZ. Clinical analysis of 50 prehospital cardiopulmonary resuscitation. Chin Pract Med. 2012;7(16):111–2.
Dong BY, Yang LL. Analysis of pre-hospital emergency cardiopulmonary resuscitation in 52 patients with sudden death. Modern Med J China. 2011;5(23):39–40.
Li XL, Zhang S. Retrospective analysis of prehospital cardiopulmonary resuscitation in 102 patients. Sichuan Med J. 2014;9(35):1219–20.
Hu JC, Liu XM, Wang XD. Analysis of pre-hospital cardiopulmonary resuscitation in 106 patients with cardiac arrest. General Pract Med. 2007;5(8):688–9.
Liu C, Zhao ZG, Wu GF, Yuan HH. Clinical analysis of 188 prehospital cardiopulmonary resuscitation. Proc Clin Med. 2009;7(18):1831–3.
Xu J. Clinical analysis of 218 cases of cardiopulmonary arrest before cardiopulmonary resuscitation. Sichuan Med J. 2012;33(10):1750–2.
Mu LH, Xu B, Sun H, Shi LL. Clinical analysis and discussion of 266 prehospital cardiopulmonary resuscitation. Nurs Forum. 2010;17(3):171–2.
Zeng YH, Yin JZ, Pan M, Liang QL. Clinical analysis of 428 prehospital cardiopulmonary resuscitation. Intern Med Health Guid. 2008;14(12):67–8.
Chen GH. Telephone guidance for cardiopulmonary resuscitation in pre-hospital emergency. Shandong Med J. 2010;50(14):91.
Yang HF, Jia JH. Analysis of 58 cases of pre-hospital cardiopulmonary resuscitation with respiratory arrest. Gansu Med J. 2009;10(28):374–5.
Wu SC. Analysis of 27 cases of emergency cardiopulmonary resuscitation. Chin J Crit Care Med. 2002;7(22):395–6.
Li XQ. Analysis of influencing factors on the success rate of pre-hospital rescue in 47 patients with cardiopulmonary resuscitation. Clin Res. 2014;19:228.
Xu YY. Talking about the effect of pre-hospital ambulance on cardiopulmonary resuscitation in patients with cardiac arrest under different conditions. Road Health Mag. 2013;12(8):160.
Li SQ. Impact of eyewitness on-site rescue on the success rate of pre-hospital cardiopulmonary resuscitation. Chin Remedies Clin. 2010;10(6):699–700.
Liu P, Liu GL, Zu LJ. Clinical analysis of pre-treatment and emergency cardiopulmonary resuscitation in pediatric hospital. Chin J Coal Ind Med. 2009;12(4):575–6.
Ye NL. Rescue analysis of on-site cardiopulmonary resuscitation for patients with sudden death before hospitalization. Med Inform. 2013;26(12):487.
Lin LF. Influencing factors of pre-hospital first aid success rate in cardiopulmonary resuscitation. Today Nurse. 2008;8:71–2.
Xia LJ. Application of "120" telephone guidance for cardiopulmonary resuscitation in pre-hospital emergency. Chin J Pract Nurs. 2011;27:15.
Xu ZB, Chen YX. Analysis of factors related to the effect of pre-hospital emergency cardiopulmonary resuscitation. Jilin Med J. 2012;33(2):256–7.
Yuan QM, Li FM, Shi XQ. Analysis of factors related to the success or failure of pre-hospital cardiopulmonary resuscitation. Chin J Gen Med. 2011;9(12):1961–2.
Tang FR, Yang T, Huang W. First aid analysis of 65 cases of cardiopulmonary resuscitation before hospital. Chin Mod Med. 2010;17(19):228–9.
Hua HM. 72 cases of cardiopulmonary resuscitation and clinical analysis. Chin J Emerg Resusc Disaster Med. 2010;5(9):885–6.
Jin X, Deng YJ, Qu Z. Retrospective analysis of the success or failure of 103 patients with cardiopulmonary resuscitation. China Foreign Health Abstr. 2012;9(13):135–7.
Sun LP. Rescue experience of 61 cases of pre-hospital respiratory arrest. Proceed Clin Med. 2007;16(5):392–3.
Zhao LX, Li JH, Wang F. Analysis of 65 patients with sudden death cardiopulmonary resuscitation (CPR) before hospitalization[J]. J Front Med. 2011;1(14):44-5.
Zhang JY, He SJ. Analysis of 144 cases of pre-hospital emergency cardiopulmonary resusc. Mod Med Health. 2008;24(13):2015–6.
Zhang Y. Analysis of 9 cases of pre-hospital emergency cardiopulmonary resuscitation. Shanxi Med J. 2009;38(9):839.
Jing XM. Discussion on the success rate of pre-hospital emergency cardiopulmonary resuscitation and the importance of medical cooperation. Chin Med Innov. 2011;8(7):117–8.
Zhou BL. Analysis of the reasons for the success rate of pre-hospital emergency cardiopulmonary resuscitation. Pract J Cardiac Cereb Pneum Vascu Dis. 2010;18(8):1159–60.
Wang XD. Analysis of 105 cases of pre-hospital emergency cardiopulmonary resuscitation. Fujian Med J. 2006;28(5):53–5.
Wen CM. Retrospective analysis of 452 cases of pre-hospital emergency cardiopulmonary resuscitation. Med J Liaoning. 2007;21(5):309–11.
Hu JC, Liu XM, Yang C, Wang Z, Zhang WT, Zhang Q, et al. Effect of pre-hospital emergency cardiopulmonary resuscitation conditions on the efficacy of patients with cardiac arrest. J Anhui Health Vocat Tech College. 2013;12(1):27–8.
Liao WQ. Analysis of influencing factors of pre-hospital emergency cardiopulmonary resuscitation. Chin Foreign Med Res. 2011;9(19):40–1.
Jia YR, Wang PY. Pre-hospital emergency cardiopulmonary resuscitation. J Pract Med Tech. 2008;15(19):2546–7.
Luo QX. Analysis of 27 cases of prehospital cardiopulmonary resuscitation. J Pract Med. 2007;23(18):2911–2.
Wang GF. Analysis of 79 cases of prehospital cardiopulmonary resuscitation. Chin J Misdiag. 2008;8(16):3923–4.
Zhang Y, Xiao H. Clinical analysis of 100 cases of pre-hospital cardiopulmonary resuscitation. Mod Med J Chin. 2009;11(4):105–6.
Wu X, Lin SB. Analysis of 115 cases of pre-hospital cardiopulmonary resuscitation. Lingnan J Emerg Med. 2004;9(3):166–7.
Pan YY. Clinical analysis of 132 cases of pre-hospital cardiopulmonary resuscitation. Shandong Med J. 2009;49(28):57–8.
Diao PS. Correlation analysis of 382 cases of prehospital cardiopulmonary resuscitation. Mod J Integ Tradit Chin West Med. 2007;16(16):2234.
Zhang M, Hua HM, Gong X. Analysis of the success factors of 454 cases of pre-hospital cardiopulmonary resuscitation and intervention strategies. Chin Gene Pract. 2010;13(12):1322–3.
Chen X. Analysis of 504 patients with cardiac arrest and cardiopulmonary resuscitation. Chin Med Herald. 2009;6(7):42–3.
Meng H. Retrospective analysis of 605 pre-hospital cardiopulmonary resusc. Chin Tradit Chin Med Inf. 2010;2(10):127–9.
Ji YJ. Retrospective analysis of 796 pre-hospital cardiopulmonary resusc. Chin J Crit Care Med. 2007;27(9):854–6.
Zhao YT. Analysis of 36 cases of pre-hospital cardiopulmonary resuscitation. Henan J Diagn Ther. 2001;15(4):204–5.
Wu YL, Zhang YX, Wang CM. Discussion on the causes and failures of pre-hospital cardiopulmonary resuscitation. Proc Clin Med. 2007;16(8):793–4.
Liu WL, Li SZ, Liu SF. Discussion on the success factors of pre-hospital cardiopulmonary resuscitation. Am J Chin Clin Med. 2004;6(1):39–43.
Guo QX, Li Y. Discussion on methods of pre-hospital cardiopulmonary resuscitation. Chin Commun Phys. 2008;10(188):67–8.
Han XT. Discussion on related factors of pre-hospital cardiopulmonary resuscitation. Shandong Med J. 2002;42(17):54–5.
Song QQ, Zhou XH, Cheng J, Li CM, Wang HB. Rescue observation of patients with sudden death after standard cardiopulmonary resuscitation in pre-hospital emergency. Pract J Card Cereb Pneumal Vasc Dis. 2012;20(10):1624–5.
Liu WM. Analysis of 41 cases of pre-hospital cardiopulmonary resuscitation in Suzhou. Emerg Med. 1993;2(4):243–4.
Dong J, Lu F. Effect of (2010 AHA guide) on the success rate of pre-hospital cardiopulmonary resuscitation in Shanghai. Health People. 2013;7(7):1–3.
Zhao JH, Li M, Zhang JY. Analysis of 34 cases of pre-hospital cardiopulmonary resuscitation. Hebei Med. 2001;23(5):394.
Zhou X, Gao X. Application and nursing measures of defibrillation in pre-hospital emergency cardiopulmonary resuscitation. Chin Fore Med Treat. 2015;20:164–8.
Wang L. Zhang FQThe effect of the first witnesses on the site to implement CPR. Chin J Emerg Resusc Disaster Med. 2015;10(7):634–7.
Zhu J, Hong JR. Study on pre-hospital emergency methods for patients with electric shock. Chin Med Pharmacy. 2015;5(17):184–8.
Guo YB. Therapeutic effect of pre-hospital first aid in patients with cardiac arrest and respiratory arrest. Chin J cardio Rehabili Med. 2015;24(4):442–4.
Zhang J. Analysis of pre-hospital emergency treatment for malignant arrhythmia. Med Frontier. 2018;8(16):166–7.
Wei Y, Nong CL, Huang SX. Pre-hospital first aid experience in patients with cardiac arrest using cardiopulmonary resuscitation. J Guangxi Med Univer. 2015;32(5):812–4.
Liu HW, Wang YH, Sun W. Analysis of the status quo of survival chain of patients with pre-hospital cardiac arrest in Qinhuangdao area based on Utstein model. J Clini Emerg. 2018;19(3):172–5.
Lin HQ. Experience of first aid in 121 patients with sudden cardiac arrest [C]. Proceedings of the 3rd Annual Academic Exchange Conference ofShanghai Pre-hospital Emergency System. 2009;66-9.
Zhao L, Han WB. Analysis of 172 cases of emergency cardiopulmonary resuscitation. Clin Med. 2015;35(6):36–7.
Chen H, Zhang CY, Xu JY. Analysis of cardiopulmonary resuscitation in patients with cardiac arrest before and after emergency hospital. Hebei Med J. 2017;39(16):2475–7.
Cui G, Xu H. Analysis of cardiopulmonary resuscitation effect and related factors in elderly patients. Henan Med Res. 2016;27(13):11–5.
Li S, Chen CL, Wang XR, Kan T, Zhu SY, Wang YX. Etal. Analysis of prognostic factors in patients with successful cardiopulmonary resuscitation in Pudong new area. Nur J Chin PLA. 2018;35(21):1–4.
Gao DJ. Analysis of the reasons for the low success rate of pre-hospital CPR in 167 patients with CA and coping strategies. Public Med Forum Mag. 2015;19(15):2051–3.
Ma ZY, Zhang XL. Clinical study of pre-treatment and emergency cardiopulmonary resuscitation in pediatric hospital. Chin Pract Med. 2016;11(17):266–7.
Liao XB, Lian G. Discussion on related factors of successful cardiopulmonary resuscitation. Guide Chin Med. 2015;13(4):145–6.
Wu GY. Application of cardiopulmonary resuscitation in pre-hospital emergency. Psychologist. 2017;23(16):341–2.
Fang H, Xiang C, Bin LZ. Application analysis of cardiopulmonary resuscitation in pre-hospital emergency treatment[J]. Home Med. 2017;1:34-5.
Fang Y, Xu J, Ren Y, Chen JM. Comparative analysis of pre-hospital first aid in adult cardiac arrest (SCA) patients under the guidance of cardiopulmonary resuscitation guidelines. Psychologist. 2016;22(21):56–8.
Zhou WL, Ceng FJ, Qin WY, Tang SH, Peng X. Factors influencing the success of cardiopulmonary resuscitation in patients with cardiac arrest. Mili Med J South Chin. 2015;29(11):839–42.
Liu Y. Clinical study of pre-hospital first-aid therapy for patients with cardiac arrest using cardiopulmonary resuscitation. World Latest Med Infor. 2017;17(89):176.
Zhao YL. Exploring the related factors of CPR application and drug efficacy in pre-hospital emergency treatment of patients with cardiac arrest. Smart Healthcare. 2017:17–9.
Chen F, Luo J. Analysis of factors affecting the effect of cardiopulmonary resuscitation before and after emergency hospital. Mod Instrum Med. 2018;24(1):55–7.
Zhang YK, Cui XP, Zhuang DY, Sun D, Xiao Z, Huang RH. Etal. Multivariate analysis of the impact of cardiopulmonary resuscitation on cardiac arrest. Chin Med Innov. 2018;15(11):97–100.
Zhao SY. Study on related factors affecting the effect of pre-hospital emergency cardiopulmonary resuscitation. Guide Chin Med. 2015;13(14):67–8.
Liang YH, Huang WP. Analysis of some factors affecting the hospital discharge rate of pre-hospital heartbeat respiratory arrest. Lingnan J Emerg Med. 2018;23(2):163–4.
Tan ZL. Analysis of factors related to the success of cardiopulmonary resuscitation in patients with pre-hospital cardiac arrest. Med Rec. 2015;21(13):2457–8.
Zhang TS. Effect evaluation of pre-hospital first aid on heartbeat respiratory arrest caused by motor injury. Psychologist. 2017;23(1):139–40.
Peng DY. Analysis of clinical influencing factors of pre-hospital emergency cardiopulmonary resuscitation[J]. China Foreign Med Treat. 2016;35(2):51-2.
Li JF. Analysis of clinical influencing factors of pre-hospital emergency cardiopulmonary resuscitation. Clin Pract. 2017;21(23):3089–90.
Xie YX. Influential factors of pre-hospital emergency cardiopulmonary resuscitation. Clin J Med Office. 2016;29(18):130–1.
Ma J. Analysis of influencing factors of pre-hospital emergency cardiopulmonary resuscitation. Clin Res. 2016;14(21):90–1.
Luo L. Analysis of influencing factors of pre-hospital emergency cardiopulmonary resuscitation. Chin Mod Doctor. 2018;56(5):104–6.
Li GZ. Clinical investigation on the influencing factors of pre-hospital emergency cardiopulmonary resuscitation. World Latest Med Inform. 2018;18(67):47–9.
Li QP, Xiong XM. Study on influencing factors of pre-hospital emergency cardiopulmonary resuscitation. Clin Res. 2017;15(26):128–9.
Liu N. First-aid measures and nursing care for emergency cardiac arrest in pre-hospital patients. Chin Health Care Nutri. 2016;26:239–40.
Tang ZH, Gu YL, Guo J. Analysis of factors affecting pre-hospital cardiopulmonary resuscitation and countermeasures. Shanghai J Prevent Med. 2016;28(6):415–8.
Wang XG, Gao D. Clinical experience of 505 patients with cardiopulmonary resuscitation in prehospital cardiac arrest and analysis of its success factors. Chin J Clin. 2015;43(4):39–41.
Ye J. Discussion on the strategy of cardiopulmonary resuscitation in patients with pre-hospital cardiac arrest. Chin J Public Health Manag. 2018;10:286.
Yu ZZ, Ma ZL, Tian XL. Discussion on the role of comprehensive measures in improving the success rate of pre-hospital cardiopulmonary resuscitation in the old city. Clin Med. 2015;9:79–80.
Li Y. Application of defibrillator in pre-hospital emergency. Orien Diet-Therapy Heal Care. 2017;12:22–3.
Zhang H. Pre-hospital emergency analysis of 45 cases of acute myocardial infarction. Chin Pract Med. 2014;9(7):49–50.
Shan HL, Wu XE, Zhang L. Analysis of pre-hospital cardiopulmonary resuscitation nursing cooperation in patients with sudden cardiac arrest[C]. Research Association of Clinical Research on Emergency Medicine. 2016;267-8.
An J. Analysis of important factors affecting patients with cardiac arrest before hospitalization. J Clin Med Litera. 2018;5(22):77.
Wang ZF, Li XM, Liu RQ. Analysis of 50 cases of successful rescue of cardiac arrest before hospital. Chin J Misdiag. 2006;6(12):2362.
Chen MH. First-aid measures and nursing care for emergency cardiac arrest in pre-hospital patients. World Latest Med Inform. 2013;13(14):372–3.
Pai HB. Analysis of 15 cases of cardiopulmonary resuscitation before cardiac arrest. Chin Fore Health Abstract. 2008;5(3):70–1.
Liu XH. Clinical analysis of 16 cases of pre-hospital emergency cardiopulmonary resuscitation. Med Inform. 2011;24(4):85.
Hu HL, Li Y, Liu YS, Guo RC, Deng QW, Chen YL. Investigation and analysis of pre-hospital first aid in 472 patients with cardiac arrest. Lingnan J Emer Med. 2015;20(3):222–4.
Liu X, Pei YC, Zhang Q. Analysis of the reasons for the success rate of pre-hospital emergency cardiopulmonary resuscitation in Tianjin. Chin J Urban Rural Indust Hygi. 2007;1:34–6.
Wang SX. Preliminary study on 18 cases of pre-hospital cardiopulmonary resusc. Nei Mongol Jo Tradit Chin Med. 2002;21(5):37.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke satistics-2016 Updata: a report from the American Heart Association. Circulation. 2016;133(4):e38–360.
Wang LX, Meng QY, Yu T. China CPR consensus and US CPR guidelines. Chin Crit Care Med. 2017;29(10):865–70.
He ZJ, Ma JX, Wang YG. Establish a 10 minute concept of first aid platinum, improve the success rate of sudden death in the community. Med Philosophy. 2006;27(8):11–4.
He ZJ. Explore the prime time for cardiopulmonary resuscitation. Chin J Crit Care Med. 2017;3(2):75-8.
He ZJ, Ning B, Zhang ZC. Establishing the Chinese first aid day - first aid platinum 10 minutes self-help rescue day. Chin J Crit Care Med. 2014;34(10):I0001-2.
Yue MX, He ZJ. The definition and main development direction of health emergency medicine. Chin J Hygiene Rescue. 2018;4(1):14–20.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HZJ conceived of the study,reviewed and finalized the manuscript. YSB and WYG proposed research framework and reviewed manuscript. GXM and LZH collected the data and drafted the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gu, XM., Yao, SB., He, Zj. et al. Meta-analysis of the success rate of heartbeat recovery in patients with prehospital cardiac arrest in the past 40 years in China. Military Med Res 7, 34 (2020). https://doi.org/10.1186/s40779-020-00263-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40779-020-00263-7