
Abstract
Purpose
The objective of this study was to evaluate the effect of removal torque (reverse torque) of titanium implants in peri-implant bone.
Methods
The P1-M1 teeth were extracted bilaterally of 6 mini pigs (BR-1). Each animal received 6 titanium implants, three for each side of mandible. On the right side of mandible, 3 implants reminded 9 months (9M) under masticatory activity and on the left side, other 3 implants were placed and immediately removed (IR). All 36 implants were removed by removal torque, and the recorded values were statistically analyzed. Animals were euthanized right after the removal torque and recording. Each third (cervical, medium, and apical) of peri-implant bone was extracted and analyzed histological and immunohistochemically. Student’s t test was used to determine statistical differences in the values between the 9M and IR samples. Data were presented as means with standard deviations. The level of significance was set at 5% (P < 0.05).
Results
Removal torque was higher in 9M experimental situation than in IR. Histological characteristics of mature bone were presented in the 9M experimental condition, and immature bone characteristics were presented in the IR experimental condition. Removal torque caused small fractures and rounding in the bone grooving. Immunohistochemical analysis reinforced the histological results; Student’s t test provided statistically significant differences to osteocalcin expression in 9M samples and no statistically significant differences expression to collagen I in both experimental conditions (P < 0.05).
Conclusions
Removal torque caused microscopical fractures and smoothing in the peri-implant bone grooves, but it does not compromise the bone healing.
Similar content being viewed by others


Introduction
Since the discovery of osseointegration by Branemark in Sweden in 1960, where found that when titanium screws left undisturbed in bone, the osteocytes grow in close apposition to the titanium surfaces and provide firm anchorage. This discovery was successfully applied in dental and craniofacial reconstructive surgery in 1965 [1, 2]. Dental implants became a common procedure in the modern dental treatment with long-term success rates exceeding 90% reaching up to 100% [3, 4] due to the development of some implant systems [5]. However, the increased use of dental implants also improved the fails. The main causes of failure are incorrect position, fracture, peri-implantitis, chronic diseases, and smoking [6–9].
Several studies indicated that screw loosening appeared to be one of the most common complications in dental implants once osseointegration has occurred, especially in single-tooth implant restorations [8, 10, 11]. The incorrect position of implants can cause maxillary sinus membrane damage, pressure on the dental nerves, or difficulties in prosthetic procedure as well as inconvenient esthetical problems. Esthetical requirements of patients have increased, especially for anterior teeth [12, 13]. Even after successful osseointegration, the implant remotion may be necessary [1, 12, 14, 15].
To correct the wrong position or fractured implant is necessary to remove it. For this purpose, it may be used various surgical techniques such as the use of trephine, implant drills, ultrasound, and others. But the use of these techniques cause great loss of peri-implant bone, what limits or prevents a new immediate rehabilitation [16, 17]. Alternatives to removal implants without losing or expanding alveolar bone led Anitua and Orive [18] to use the counter torque. Studies comparing counter torque with trephine drills to remove implants indicated better performance for the first [18, 19].
The causes of implant failure are well known and described; however, what happened with the peri-implant bone that can influence on the success of a reimplantation needs to be better described, with the increase of implant removals to replacement for functional or aesthetic corrections and the need to reduce alveolar bone loss [20].
Many authors investigated bone reactions around dental implants [17–21]. What happens in the peri-implant bone implants removed is not reported in scientific articles. This study evaluated the peri-implant bone after his immediate removal and after 9 months of osseointegration. The aim of the present study was to evaluate the peri-implant bone after dental implant removal.
Materials and methods
Animals and preparation
This study was approved by the University Animal Ethics Committee-CEUA/UNICAMP-(Campinas, SP) (no.2730-1/12). Six adult male mini pigs (BR-1 mini pigs, São Paulo, Brazil) with ~36 months old and weighed ~55 kg were used in the experiment. The mini pigs were kept in the Experimental Center of the Veterinary Faculty (FESB-Bragança Paulista, SP) and were allowed to adapt to the environment 1 week prior to surgeries. At the beginning of the study, all animals underwent a physical examination by a veterinarian and were found to be healthy. During the study period, the mini pigs were weighed if abnormalities in food intake were observed [21]. The identification of the animals was enabled by marking earrings numbered. The mini pigs were kept separately in cemented stalls. Fresh water was available ad libitum. For 12 h, before surgery, the animals were fasting with water ad libitum. The animals were inspected after the first few postoperative days for signs of wound dehiscence or infection and weekly thereafter to assess general health.
The removal torque and the histological and immunohistochemical analysis of peri-implant bone were conducted in the mandible of the mini pigs.
The animals were premedicated to induce anesthesia with midazolam (0.2 mg/kg) (Medley, Sumaré, SP, Brasil) and chlorpromazina IM (0.1 mg/kg) (Cristália, Itapira, SP, Brasil). An endotracheal tube was used for intubation, and a mixture of isofluran (Baxter Healthcare Corporation, IL, USA) with oxygen in a ratio 1:1 (5–10 mL/kg/min) was used to maintain anesthesia during the experiment. Local anesthesia was performed with lidocaine 2% with epinephrine 12.5 μg/mL (Xylocain/Adrenalin®, Astra, Wedel, Germany). After surgery, veterinarian Pentabiotic Reinforced antibiotic 40.000 UI/kg (Eurofarma, Itapevi, SP) and anti-inflammatory dexamethasone 3 mg/pig (MSD, São Paulo, SP, Brasil) were administered IM application .
Surgical procedures and implant removal
The same operator performed all the surgeries and radiographic. The P1, P2, P3, and M1 teeth were extracted bilaterally of each animal. The tooth extractions were difficult in every case because the roots were divergent and usually curved distally. It was necessary to odontosection before extracting them [22]. After 4 months of healing, three external hexagon implants (EH) (Dentifix. Santa Rita do Passa Quatro, SP, Brasil) with the same diameter and length (ø4.1 × 10 mm) were placed with the STA surface on one side of the mandible (Figs. 1 and 2). The side was chosen by lot. Six months later, this implant group received a prosthetic (Fig. 3) to improve the bone tension [23]. Three months later, the 3 implants with prosthetic were removed, totalizing 9 months (9M) and opposite side of the mandible three new implants were placed and immediately removed (IR). Each miniature pig received 6 implants, 3 on each side of the mandible. Thus, a total number of 36 implants were placed. Pigs were anesthetized as described above; all dental implants were carefully removed by a counterclockwise force (removal torque) with a torque driver (Retriever Maximus - Belo Horizonte, MG, Brasil); and the level of torque required to remove the implant from the bone was recorded by mark-10 universal torque series sensor STW, and removal torque were read by a force/torque indicator model BGI (JLW Instruments, Chicago, IL, USA). Afterwards, anesthetized pigs were euthanized with pentobarbital; their mandibles were cut and the respective peri-implant bone was removed in small blocks (10×10×6 mm).

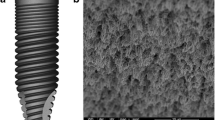
Type of implant and clinical picture of implants position in the mandible of mini pigs

Radiographs illustrating implants in the mandible of mini pigs. a Radiography of the mini pigs head with implants in both mandible sides. b Periapical radiograph of implants position

Prothesis fixed installed on the three implants
Histology and immunohistochemical analysis
The mandibles were sectioned into left and right segments, and each peri-implant bone was sectioned again to individualize them. Each peri-implant bone block was fixed in buffered formalin solution, pH 7.0, for 6 days, demineralized in 10% formic acid, and dehydrated through progressing alcohol concentrations and paraffin-embedded. Paraffin blocks were sectioned at 7-μm thick mounted on poly-l-lysine coated glass slides (Sigma–Aldrich, Gillingham, UK) and processed for hematoxylin-eosin staining and for immunohistochemical analysis. Each peri-implant bone paraffin block was longitudinal and colored with hematoxylin-eosin (H&E) to identify sites of new bone destruction or remodeling.
Immunohistochemical analysis was performed on duplicate tissue sections of peri-implant bone from each experimental specimen (9M and IR—randomly chosen). Sections were deparaffinized and rehydrated by rinsing with xylene for 10 min, industrial methylated spirit for 5 min, and more 5 min in tap water. In order put out endogenous peroxidase activity, sections were incubated at room temperature in 3% hydrogen peroxide for 10 min. Two proteins were evaluated due to their sequential expression during bone healing. Collagen type I because it is expressed early in the healing process [24]. Osteocalcin because it is a late marker of bone formation and is expressed during mineralization by osteoblastic cells [24]. To prevent nonspecific protein binding, serum-free blocking agent (DAKO, Hamburg, Germany) was used. The sample was allowed to react for 1 h at room temperature with a primary anti-collagen I antibody (Abcam, Cambridge, UK) and anti-osteocalcin antibody (Takara Biomedicals Europe, France). Immunohistochemical analysis was performed at different thirds of the peri-implant bone (cervical, medium, and apical). Each third was selected at least two times per sample and analyzed. Sample images were captured then observed by means of Leica DM 4000 light microscopy (Leica Cambridge Ltd, Cambridge, UK) incorporating a Leica DFC 320 camera (Leica Cambridge Ltd) for computerized images in histological and immunohistochemistry analysis with a ×40 magnification.
Image and statistical analysis
Hematoxylin-eosin-stained section images were digitized and analyzed in order to recognize the presence of native bone tissue by the presence of osteocyte lacunae-containing cells and the newly formed bone tissue recognized by the absence of lacunae. Also, the characteristics of peri-implant bone, presence or absence of bone fractures, and the shape and contour of bone grooving resultant of the trephine action were analyzed. Histological analysis was performed in images of the semi-serial slices of each peri-implant bone. They were captured by a digital camera (Samsung, South Korea) coupled to a light microscope (Zeiss, Germany) with original ×200 magnification and resolution of 600 dpi. Images around 116–80 cm were captured of each third of the peri-implant bone. Then, a digital framework of entire peri-implant bone was built by the combining three images.
Immunohistochemical analysis also was performed on three thirds on each sample with collagen I and osteocalcin. The same image capture and construction were made, but they were measured, and the value was defined by the positive-staining samples and was used to automatically analyze images of all samples that were stained under identical conditions for both proteins and implant removals.
In the analysis of both mandible sides, the images were acquired at ×200 magnification using a Nikon E600 microscope (Nikon Instruments Inc, Melville, USA). The integral optical density (IOD) of target protein was measured with Image-Pro Plus 5.0 (Media Cybernetics, Rockville, MD, USA). In the process of measurement, the values were defined firstly by determining the positive staining of control sections and were used to automatically analyze images of all samples that were under identical conditions (u/pixel) [25].
Statistical analyses were performed with SPSS software (SPSS, Chicago, Ill). Student’s t test was used to determine statistical differences in the values between the 9M and IR samples. Data were presented as means with standard deviations. The level of significance was set at 5% (P < 0.05).
Results
Clinical observation
No remarkable complications were found during the healing period. At sacrifice, all 18 implants fixed after 9 months were considered successfully integrated at the time of the removal and none showed any mobility or signal of infection at sacrifice. There was no difference in the healing between animals who had the implants immediately removed after installation, and animal whose implants were removed 9 months later of installation.
Removal torque
The mean and standard deviation of removal torque are illustrated in Tables 1 and 2 for both experimental specimens. The removal torque values increased after 9 months, with significant differences between IR and after 9M specimens.
Histological analysis
Each third of the peri-implant bone was evaluated and showed not representative difference in the bone conditions for each experimental specimen separately (9M and IR) (Figs. 4 and 5). Removal torque did not alter the characteristics of mature bone and the healing process; thereby, did not cause significant damage in the peri-implant bone. After surgical trauma, it was possible to notice inflammatory process, which blood cells in the alveolar bone of IR specimens. At the 9M specimens, mature bone was evident, as well as presence of fibrous connective tissue without evidence of inflammatory infiltrate. A vital bone with many osteocytic lacunae was observed on the grooving of the internal wall of peri-implant bone. Many capillaries were present, and a rim of osteoblasts was observed on the bone margins. Natural inflammatory and bloody cells were visible only in IR specimens. As well as only in the IR specimens were observed small fractures and rounding in the bone grooving caused by implant trephine and removal torque. At 9M experimental condition, bone grooving presented clear contours, without rounding or fractures. In both experimental specimens, there was no evidence of bone formation particularly at tissue around the peri-implant bone surface. Only in the last third (apical) was possible to identify some bone fragments, probably caused by implantation procedure.

Representative photomicrographs of each third of the peri-implant bone of 9M experimental condition (H&E, ×40). a First third (cervical third). b Intermediate third. c Apical third. Bone grooving with no altered contour

Representative photomicrographs of each third of the peri-implant bone of IR experimental condition (H&E, ×40). a First third (cervical third). b Intermediate third. c Apical third. Note the edges of bone grooving present rounded contour, mainly in the last third
Immunohistochemistry analysis
Duplicate sections of peri-impant bone were obtained from each implant sample to evaluate the percentage of stained areas in order to differentiate markers of collagen I and osteocalcin within both experimental conditions (Fig. 6). The highest collagen I expression values were observed at the IR experimental condition, and osteocalcin expression was higher at the 9M.

Immunohistochemical staining of osteocalcin (a) and collagen I (c) in sections from mini pigs mandible from 9M and IR osteocalcin (b) and collagen I (d). There were statistically significant differences to osteocalcin in 9M samples and no statistically significant differences to collagen I samples. Magnification: ×40 (a, b) and ×100 (c, d)
There was a statistically significant difference between the two experimental specimens (9M and IR) in immunohistochemical evaluation for osteocalcin expression (Tables 3 and 4). Immunohistochemical analyses allowed to identify manifestation of osteocalcin protein in all thirds of peri-implant bone in both models evaluated, with greatest expression to model which the healing time was higher (9M). Statistical difference presented was observed especially in the middle and lower thirds. The first third presented a difference, but it was not significant. The evaluation of collagen I expression did not show statistical differences. In all evaluated thirds, the presence of the protein was equivalent.
Discussion
Dental implant revolutionized oral rehabilitation, becoming the natural teeth replacement by a titanium implant, a successful alternative to treat total or partial edentulism [14, 26, 27]. Nowadays, dental implants are definitely a current procedure in many dental offices [3, 28, 29]. Despite the long-term success shown by different studies [14, 30], implant failure is inevitable [31–33]. Since, to correct early or later failure implants is necessary to remove them, any tool available is necessary. Five different techniques to remove failing implants provided to be successful; however, the counter torque technique, used in our study, is the highest predictability for the insertion of another implant [17, 18, 34–36].
Previous in vivo assessments of bone healing around implants presented histological observations such as bone-implant contact studies under monitored torque values [19, 22, 37]. This study adds an extended methodology of previous investigations, because it provides beyond histological analysis and immunohistochemical analysis to assess peri-implant bone behavior in a real clinical condition.
Histological analysis of early failed implants has indicated that bone overheating might be the most probable cause of failure [33, 37–39]. Bur-forceps, neo bur-elevator-forceps, trephine drill, and scalpel-forceps are safe implant removal techniques, however, require experience and training of the operator. Counter torque technique is an easy and practice tool because it is a heating control procedure; it does not require training and can be performed by a beginner operator, so we opted to test this tool.
The clinical observations of this study showed all 18 implants fixed after 9 months were considered successfully integrated at the time of the removal, and none showed any mobility [40] or signal of infection [21, 33, 41, 42] at sacrifice.
The results of this work showed higher values of removal torque in 9M than in IR specimens. It was expected since the longer healing time (9M) promotes better osseointegration than immediate implant removal. It was verified by the presence of mature bone in the peri-implant bone in the 9M specimens [4, 22, 43].
In order to better use a model which reproduce the natural conditions of dental implant in action, minipigs (BR-1) have been used in this study [44], the nonprimate animal model that is most appropriate for the study of human mastication [45] and commonly used in research because suine and human share important anatomic and physiologic characteristics [46, 47].
The osseointegration process is quite similar to the primary bone healing [1]. After surgical procedure, there is an inflammatory process with local circulatory alteration. Afterwards, regeneration happens than bone tissue beginning to be replaced [1, 48]. As well as other peri-implant response happen, as the presence of collagen layer between bones and implant surfaces. The connective tissue consists in parallel collagen fibers supported by blood elements, setting the anatomical organization of collagenous ligament [49, 50]. All histological events described above were clearly observed in all IR specimens evaluated on this study. To the 9M specimens, those events were less evident due to postsurgical time.
At the 9M specimens, mature alveolar bone was evident. There is a presence of a fibrous connective tissue with no evidence of inflammatory infiltrate. A vital bone with many osteocytic lacunae was present around the grooving implant surface. Many capillaries were present, and a rim of osteoblasts was observed on the bone margins. Natural inflammatory and bloody cells were visible only in IR experimental condition.
As all surgical procedures of our study were taken with a strict care, there was no fracture or heating in bone tissue, which could compromise the results of this study. Long-term studies indicated in histological analysis of early failed implants that bone overheating might be the most probable cause of failure [33, 37–39].
The histological analysis also presented small fractures and rounding in the bone grooving caused by implants only in the IR condition. Considering the time healing in both specimens (9M and IR), after surgical procedure, some fractures and fragments were produced and those aspects were not presented after 9 months due to healing time. Removal torque caused little fracture and smooth on the peri-implant bone grooves just after the installation procedure (IR); however, none considerable damage or alteration compromised the bone healing. As at 9M specimens, the bone grooving presented clear contours, without rounding or fractures, demonstrating that removal torque is not a factor of dental implant failure. Even though some bone fragments were presented in the last third (apical) just in the IR procedure, it also did not compromise the bone healing.
According to Christenson R.H. [24], the bone structure, metabolism, and regulation are reflected by markers of resorption, formation, and/or turnover. Among the markers of bone resorption is the type 1 collagen degradation and maker of bone formation: Osteocalcin. Bone formation markers derive from the osteoblastic activity, formed during the different stages of osteoblasts proliferation, differentiation, and osteoid synthesis [6, 51–53], namely the bone osteocalcin, alkaline phosphatase, and other makers. Osteocalcin is expressed during mineralization by osteoblastic cells. [24, 54–56]. Those evidences supported us to analyze the expression of bone extreme activities: resorption (collagen I) and formation (osteocalcin). Our immunohistochemistry results expressed the bone repair because it showed higher expression of osteocalcin at the 9M specimens. Since the titanium implants were fixed for 9 months, peri-implant bone was submitted to masticatory tension [23] and that causes bone activity, stimulating osteocalcin expression, because it occurs during mineralization. Notwithstanding, collagen I expression did not show statistical difference between both experimental conditions, in spite of all numerical values were higher to IR experiment. It can also be explained by the healing time evaluated. Immediate implant removal caused histological evidence but has no time enough to express changes in the expression of collagen type I. The healing time was not extended because immediate removal represents a clinical situation in titanium implant procedures, when failure is detected just after its installation. The higher numerical values of collagen I expression to IR experiment condition indicate more protein activity than 9M. It also represents no removal torque influence in the healing process leading to the understanding that this does not hinder the immediate installation of a new implant in the same socket.
Conclusion
Implant removal torque should be higher to remove implants with long-time installation than implants removed immediately after installation. Although, removal torque causes microscopical fractures and smooth on the peri-implant bone grooves, it does not compromised the bone healing.
References
Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent. 1983;50(3):399–410.
Chiapasco M, Gatti C. Immediate loading of dental implants placed in revascularized fibula free flaps: a clinical report on 2 consecutive patients. Int J Oral Maxillofac Implants. 2015;19(6):906–12.
Shemtov-Yona K, Rittel D. On the mechanical integrity of retrieved dental implants. J Mech Behav Biomed Mater [Internet]. Elsevier; 2015;49:290–9. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1751616115001812.
Paolantonio M, Dolci M, Scarano A, Archivio D, Placido G. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J Periodontol. 2001;72(11):1560-71.
Esposito M, Grusovin MG, Coulthard P, Thomsen P, Worthington HV. A 5-year follow-up comparative analysis of the efficacy of various osseointegrated dental implant systems: a systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants [Internet]. 2005;20(4):557–68. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16161740.
Chung H-J, Cho L, Shin J-S, Lee J, Ha I-H, Park HJ, et al. Effects of JSOG-6 on protection against bone loss in ovariectomized mice through regulation of osteoblast differentiation and osteoclast formation. BMC Complement Altern Med [Internet]. 2014;14:184. [cited 2015 Aug 11] Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4066836&tool=pmcentrez&rendertype=abstract.
Clementini M, Rossetti PHO, Penarrocha D, Micarelli C, Bonachela WC, Canullo L. Systemic risk factors for peri-implant bone loss: a systematic review and meta-analysis. Int J Oral Maxillofac Surg [Internet]. 2014;43(3):323–34. [cited 2015 Aug 11] Available from: http://www.sciencedirect.com/science/article/pii/S0901502713011922.
Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JYK. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90(2):121–32.
Klinge B, Hultin M, Berglundh T. Peri-implantitis. Dent Clin North Am. 2005;49(3 SPEC. ISS):661–76.
Jemt T, Pettersson P. A 3-year follow-up study on single implant treatment. J Dent. 1993;21(4):203–8.
Lenssen O, Barbier L, De Clercq C. Immediate functional loading of provisional implants in the reconstructed atrophic maxilla: preliminary results of a prospective study after 6 months of loading with a provisional bridge. Int J Oral Maxillofac Surg [Internet]. 2011;40(9):907–15. [cited 2015 Oct 5] Available from: http://www.sciencedirect.com/science/article/pii/S090150271100213X.
Glauser R, Sailer I, Wohlwend A, Studer S, Schibli M, Schärer P. Experimental zirconia abutments for implant-supported single-tooth restorations in esthetically demanding regions: 4-year results of a prospective clinical study. Int J Prosthodont [Internet]. 2004;17(3):285–90. [cited 2015 Oct 6] Available from: http://www.mendeley.com/catalog/experimental-zirconia-abutments-implantsupported-singletooth-restorations-esthetically-demanding-reg/.
Kohal R-J, Att W, Bächle M, Butz F. Ceramic abutments and ceramic oral implants. An update. Periodontol. 2000 [Internet]. 2008;47(1):224–43. [cited 2015 Oct 6] Available from: http://www.ncbi.nlm.nih.gov/pubmed/18412584.
Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10(6):387–416.
Lello GE. The Branemark Novum protocol for same-day teeth: a global perspective. Br J Oral Maxillofac Surg [Internet]. 2002;40(3):268–9. [cited 2015 Aug 5] Available from: http://www.sciencedirect.com/science/article/pii/S0266435601907776.
Kim Y-K, Kim B-S, Lee H-J, Hwang J-W, Yun P-Y. Surgical repositioning of an unrestorable implant using a trephine bur: a case report. Int J Periodontics Restorative Dent [Internet]. 2010;30(2):181–5. [cited 2015 Aug 13] Available from: http://www.ncbi.nlm.nih.gov/pubmed/20228977.
Li CH, Chou CT. Bone sparing implant removal without trephine via internal separation of the titanium body with a carbide bur. Int J Oral Maxillofac Surg. 2014;43(2):248–50.
Anitua E, Orive G. A new approach for atraumatic implant explantation and immediate implant installation. Oral Surg Oral Med Oral Pathol Oral Radiol [Internet]. Elsevier; 2012;113(3):e19–25. Available from: http://dx.doi.org/10.1016/j.tripleo.2011.06.035.
Anitua E, Murias-Freijo A, Alkhraisat MH. Conservative implant removal for the analysis of the cause, removal torque and surface treatments of failed nonmobile dental implants. J Oral Implantol [Internet]. 2014 Dec 1 [cited 2015 Aug 20]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/25436836.
Torsiglieri T, Raith S, Rau A, Deppe H, Hölzle F, Steiner T. Stability of edentulous, atrophic mandibles after insertion of different dental implants. A biomechanical study. J Cranio-Maxillofacial Surg [Internet]. 2015;43(5):616–23. [cited 2015 Oct 6] Available from: http://www.sciencedirect.com/science/article/pii/S1010518215000530.
Markwardt J, Sembdner P, Lesche R, Jung R, Spekl K, Mai R, et al. Experimental findings on customized mandibular implants in Göttingen minipigs—a pilot study. Int J Surg [Internet]. 2014;12(5):60–6. [cited 2016 Jan 16] Available from: http://www.sciencedirect.com/science/article/pii/S1743919113010868.
Assenza B, Scarano A, Perrotti V, Vozza I, Quaranta A, Quaranta M, et al. Peri-implant bone reactions around immediately loaded conical implants with different prosthetic suprastructures: Histological and histomorphometrical study on minipigs. Clin Oral Investig. 2010;14(3):285–90.
Sasaki H, Koyama S, Yokoyama M, Yamaguchi K, Itoh M SK. Bone metabolic activity around dental implants under loading observed using bone scintigraphy. J Prosthet Dent [Internet]. 2009;101(2):127. [cited 2015 Oct 5] Available from: http://www.sciencedirect.com/science/article/pii/S002239130960007X.
Christenson RH. Biochemical markers of bone metabolism: an overview. Clin Biochem. 1997;30(8):573–93.
Wei G, Hu Y, Zheng L, Huo J, Tang T, Deng F. Bone remodeling at microscrew interface near extraction site in the beagle dog mandible-histologic and immunohistochemical analyses. J Appl Oral Sci [Internet]. 2013;21(5):443–51. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3881839&tool=pmcentrez&rendertype=abstract.
Chrcanovic BR, Albrektsson T, Wennerberg A. Immediately loaded non-submerged versus delayed loaded submerged dental implants: a meta-analysis. Int J Oral Maxillofac Surg [Internet]. 2015;44(4):493–506. [cited 2015 Dec 3] Available from: http://www.sciencedirect.com/science/article/pii/S090150271400441X.
Wennerberg A, Albrektsson T. Current challenges in successful rehabilitation with oral implants. J Oral Rehabil. 2011;38(1):286–94.
Ayub EA, Shiratori FK, Bonfante G, do Valle AL, Abrão AM. Nobel Direct - Um novo conceito de implantes para ativação imediata - Relato de caso clínico^ipt. ImplantNews. 2007;4(1):70–5.
Nogueira-Filho G, Iacopino AM, Tenenbaum HC. Prognosis in implant dentistry: a system for classifying the degree of peri-implant mucosal inflammation. J Can Dent Assoc [Internet]. 2011;77:b8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21266099.
Lekholm U, Gunne J, Henry P, Higuchi K, Lindén U, Bergström C, et al. Survival of the Brånemark implant in partially edentulous jaws: a 10-year prospective multicenter study. Int J Oral Maxillofac Implants. 1999;14:639–45.
Pabst AM, Walter C, Ehbauer S, Zwiener I, Ziebart T, Al-Nawas B, et al. Analysis of implant-failure predictors in the posterior maxilla: a retrospective study of 1395 implants. J Craniomaxillofac Surg [Internet]. 2015;43(3):414–20. [cited 2016 Jan 13] Available from: http://www.sciencedirect.com/science/article/pii/S1010518215000141.
Chiapasco M, Zaniboni M. Failures in jaw reconstructive surgery with autogenous onlay bone grafts for pre-implant purposes: incidence, prevention and management of complications. Oral Maxillofac Surg Clin North Am [Internet]. 2011;23(1):1–15, v. [cited 2015 Aug 5] Available from: http://www.sciencedirect.com/science/article/pii/S1042369910001305.
Piattelli A, Scarano A, Piattelli M. Microscopical aspects of failure in osseointegrated dental implants: a report of five cases. Biomaterials [Internet]. 1996;17(12):1235–41. [cited 2015 Oct 5] Available from: http://www.sciencedirect.com/science/article/pii/0142961296849441.
Stajčić Z, Stojčev Stajčić LJ, Kalanović M, Đinić A, Divekar N, Rodić M, et al. Removal of dental implants: review of five different techniques. Int J Oral Maxillofac Surg [Internet]. 2015 Dec 10 [cited 2015 Dec 30];In press. Available from: http://www.sciencedirect.com/science/article/pii/S0901502715014162.
Albu S. The “double-barrel” approach to the removal of dental implants from the maxillary sinus. Int J Oral Maxillofac Surg [Internet]. 2013;42(12):1529–32. [cited 2015 Aug 4] Available from: http://www.ncbi.nlm.nih.gov/pubmed/23684814.
Smith LP, Rose T. Laser explantation of a failing endosseous dental implant. Aust Dent J [Internet]. 2010;55(2):219–22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20604768.
Piattelli A, Scarano A, Dalla Nora A, De Bona G, Favero GA. Microscopical features in retrieved human Branemark implants: a report of 19 cases. Biomaterials [Internet]. 1998;19(7-9):643–9. [cited 2015 Dec 30] Available from: http://www.sciencedirect.com/science/article/pii/S0142961297001580.
Piattelli A, Piattelli M, Mangano C, Scarano A. A histologic evaluation of eight cases of failed dental implants: is bone overheating the most probable cause? Biomaterials [Internet]. 1998;19(7-9):683–90. [cited 2015 Dec 30] Available from: http://www.sciencedirect.com/science/article/pii/S0142961297001725.
Piattelli A, Scarano A, Piattelli M. Histologie retrieved dental implants: 8 years’ experience ( 1989-1996 )*. J Periodontol. 1998;178–84.
Grandi T, Guazzi P, Samarani R, Grandi G. Clinical outcome and bone healing of implants placed with high insertion torque: 12-month results from a multicenter controlled cohort study. Int J Oral Maxillofac Surg [Internet]. 2013;42(4):516–20. [cited 2016 Jan 13] Available from: http://www.sciencedirect.com/science/article/pii/S0901502712004286.
Ata-Ali J, Ata-Ali F. Do antibiotics decrease implant failure and postoperative infections? A systematic review and meta-analysis. Int J Oral Maxillofac Surg [Internet]. 2014;43(1):68–74. [cited 2016 Jan 13] Available from: http://www.sciencedirect.com/science/article/pii/S0901502713002580.
Aloufi F, Bissada N, Ficara A, Faddoul F, Al-Zahrani MS. Clinical assessment of peri-implant tissues in patients with varying severity of chronic periodontitis. Clin Implant Dent Relat Res. 2009;11(1):37–40.
Aubin JE, Liu F, Malaval L, Gupta AK. Osteoblast and chondroblast differentiation. Bone [Internet]. 1995;17(2):S77–83. [cited 2015 Dec 30] Available from: http://www.sciencedirect.com/science/article/pii/875632829500183E.
Mariano M. Minisuíno (minipig) na pesquisa biomédica experimental. O Minipig br1. Acta Cirúrgica Bras. 2003;18(5):387–91.
Herring SW. How can animal models answer clinical questions? Futur Orthod. 1998;89–96.
Swindle MM, Smith AC, Laber-laird K, Dungan L. Farm Animals in Biomedical Research — Part One Swine in Biomedical Research: Management and Models. 1994;36(1):1–5.
Ruehe B, Niehues S, Heberer S, Nelson K. Miniature pigs as an animal model for implant research: bone regeneration in critical-size defects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod [Internet]. 2009;108(5):699–706. [cited 2015 Aug 5] Available from: http://www.sciencedirect.com/science/article/pii/S1079210409004363.
McKinney Jr RV, Steflick DE, Koth DLSB. The scientific basis for dental implant therapy. J Dent Educ. 1988;52(12):696–705.
McKinney Jr RV, Koth D. The single-crystal sapphire endosteal dental implant: material characteristics and 18-month experimental animal trials. J Prosthet Dent. 1982;47(1):69–84.
McKinney RV Jr, Steflik DE, Kolt D. Histological results from a comparative endosteal dental implant study. J Dent Res. 1987;66(186):34–41.
Aubin JE. Principles of Bone Biology [Internet]. Principles of Bone Biology. Elsevier; 2008 [cited 2015 Dec 30]. 85-107 p. Available from: http://www.sciencedirect.com/science/article/pii/B9780123738844000264.
Cremers S GP and SM. Biochemical markers of bone metabolism. Princ Bone Biol 3rd ed. 2008;Press:1857–81.
Seibel MJ. Molecular markers of bone turnover: biochemical, technical and analytical aspects. Osteoporos Int [Internet]. 2000;11 Suppl 6:S18–29. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11193236.
Verbicaro T, Giovanini AF, Zielak JC, Baratto Filho F, de Araujo MR, Deliberador TM. Osteocalcin immunohistochemical expression during repair of critical-sized bone defects treated with subcutaneous adipose tissue in rat and rabbit animal model. Braz Dent J [Internet]. 2013;24(6):559–64. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24474349.
Campos JM de, Prati AJ, Cirano FR, Pimentel SP, Pastore GP, Pecorari VG, et al. Smoking modulates gene expression of type-1 collagen, bone sialoprotein and osteocalcin in human alveolar bone. J Oral Maxillofac Surg [Internet]. 2015 Jun [cited 2015 Jun 29]; Available from: http://www.sciencedirect.com/science/article/pii/S0278239115009039.
Yun H-M, Ahn S-J, Park K-R, Kim M-J, Kim J-J, Jin G-Z, et al. Magnetic nanocomposite scaffolds combined with static magnetic field in the stimulation of osteoblastic differentiation and bone formation. Biomaterials [Internet]. 2016;85:88–98. [cited 2016 Feb 10] Available from: http://www.sciencedirect.com/science/article/pii/S0142961216000491.
Acknowledgements
We would like to thank Mario Perussi for supplying us with the customized system, implants, and prosthetic components, Dentifix®, FESB, veterinary professors Rafael Rodrigues and Alexander Correa Borghesan, and CAPES for the scholarship and financial support.
Authors’ contributions
ROS conceived the study, held surgical procedures, and drafted the manuscript. FP did the preparation and helped in reading the histological slides and immunohistochemistry. PHFC participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Competing interests
Ricardo de Oliveira Silva, Fabrício Passador, and Paulo Henrique Ferreira Caria declare that they have no competing interests.
Ethics approval
This study was approved by the University Animal Ethics Committee-CEUA/UNICAMP-(Campinas, SP) (no.2730-1/12).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Silva, R.d., Passador, F. & Caria, P.H.F. Twist removal of healed vs. nonhealed implants—a mechanical and histological study in mini pigs. Int J Implant Dent 2, 23 (2016). https://doi.org/10.1186/s40729-016-0059-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40729-016-0059-x