
Abstract
Background
The acceptability and preference for clear aligner therapy (CAT) has been increasing among orthodontists, but there is still a lack of consensus regarding CAT best practices. Consequently, this study aimed to investigate CAT practices among orthodontists practicing in Canada.
Methods
The survey was conducted among orthodontists practicing in Canada using a modified previously published survey. Sixty orthodontists participated (6.1% response rate). It consisted of 11 sections with open and closed questions related to demographic information and particularities about using or not using CAT. The survey responses were exported from REDCap to a Microsoft Excel (Microsoft, Redmond, Wash) spreadsheet, then statistically analyzed using SPSS software (SPSS for Windows, version 21.0; IBM Inc., Armonk, NY, USA). The comments were categorized under themes and subthemes. Data were organized in descriptive statistics, expressing frequencies and percentages.
Results
Almost 30% of the orthodontist’s annual caseload was treated with CAT, most frequently prescribed to adult patients. Case complexity and patient cooperation were the factors that most influenced the decision to prescribe CAT. Almost half of orthodontists reported sometimes combining CAT with adjunctive fixed appliances.
Conclusions
Most orthodontists prescribe CAT, and its use is based on the malocclusion’s complexity. Orthodontists who do not prescribe CAT believe that fixed appliance therapy has superior treatment outcomes.
Similar content being viewed by others


Background
Clear Aligner Therapy (CAT) was popularized after the introduction of Invisalign® (Align Technology, Santa Clara, Calif.) [1]. Its growth was strongly supported by its aesthetic appearance and patient comfort, which directly impacts patients’ Oral Health-Related Quality of Life (OHRQoL) [2]. Its association with cutting-edge technology, such as CAD (computer-aided design) and CAM (computer-aided manufacturing), and extensive investment in merchandising further increased its popularity [3].
However, this technology has some limitations, mainly in treating complex malocclusions [1, 4]. So far, treatment success is reported to be mostly achieved in mild and moderate crowding cases [1, 4]. Frequently reported difficulties with CAT include patient adherence, finishing/detailing performance, closure of extraction spaces, specific tooth movements such as torque control, tooth rotations in rounded teeth, management of upper lateral incisors due to their size and morphology, and intrusion and extrusion movements [1, 5, 6].
This study aims to investigate CAT practices among orthodontists practicing in Canada, but more importantly, analyze the reasons for their use or not, as well as the malocclusion traits most frequently managed with CAT in this sample. Previous studies in the United States/Canada, United Kingdom, France, Australia, Republic of Ireland and New Zealand have reported increased acceptability and preference for CAT [1, 6,7,8,9,10,11]. However, orthodontists still lack consensus regarding the CAT best practices [1, 11].
Materials and methods
The University of Alberta Research Ethics Board approved this study (ID Pro00128404). The survey was conducted among orthodontists practicing in Canada using a modified previously published survey (adapted from Meade & Weir, 2022) [9]. It consisted of 11 sections with open and closed questions related to demographic information and particularities about using or not using CAT. Section A addressed demographic characteristics. Section B assessed if respondents incorporated CAT in practice and the frequency of their use. If respondents answered that they did not use CAT, they were directed to Section K. Section C included questions regarding specific CAT choices and the reasoning behind them. Section D addressed digital treatment planning (DTP) protocols. Sections E and F included questions regarding case selection and treatment protocols. Section G contained questions about interproximal enamel reduction (IPR). Section H sought information about refinements and finishing. Section I aimed to determine the frequency of patient-reported CAT-related issues reported by orthodontists. Section J addressed aspects of CAT compared to fixed appliances. Section K addressed the factors influencing the decision not to provide CAT. The electronic questionnaire was adapted to the REDCap (Research Electronic Data Capture) software platform hosted at the University of Alberta. Data were collected and managed using REDCap tools. A pilot test was conducted among local community orthodontic colleagues to check survey validity, reliability, and acceptability. After modifications based on this feedback, the survey would take approximately 15 min to be completed.
The respondents were all active orthodontists (retired and student members were not considered) registered with the Canadian Association of Orthodontists (CAO), which comprised 981 orthodontic specialists at the survey date. The CAO was contacted in April 2023 to send the survey link to all active Canadian Association of Orthodontists members through their monthly bulletin. The provincial boards and local boards for orthodontists were also contacted individually by email, and they forwarded the survey link to its affiliates through email. After two weeks, a reminder email was sent to the provincial boards. The survey was closed in October 2023.
The survey responses were exported from REDCap to a Microsoft Excel (Microsoft, Redmond, Wash) spreadsheet, then statistically analyzed using SPSS software (SPSS for Windows, version 21.0; IBM Inc., Armonk, NY, USA). The comments were categorized under themes and subthemes. Data were organized in descriptive statistics, expressing frequencies and percentages.
Results
Eighty-one active orthodontists accessed the email containing the link to the questionnaire. Among them, 60 agreed to participate in the study (overall response rate = 6.1%). Not all respondents answered all questions. Most responders were male (71.7%, n = 43) and obtained their specialist orthodontic qualification in Canada (60.0%, n = 36). A total of 95% (n = 57) of the respondents reported using CAT in clinical practice. Among them, the mean number of years in orthodontic practice was 19.0 (± 11.8), and 96.5% (n = 55) exclusively practiced in a private clinical setting.
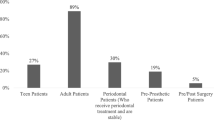
Respondents reported that, on average, 29.9% (± 24.1%) of their annual caseload were treated with CAT. Table 1 indicates that most responders managed more than 50 CAT per year. Table 2 outlines that the complexity of the case influenced the decision of most responders to prescribe CAT. Table 3 shows that CAT was most frequently prescribed to adult patients. Most responders utilized more than one CAT brand, with Invisalign® being the most used (77.2%, n = 44), followed by 3 M Clarity® (3 M, St. Paul, Minn) at 10.5% (n = 6).
The ease and quality of the DTP significantly influenced the choice of a particular aligner company/provider (Table 4). Only three (5.0%, n = 60) responders reported not changing the initially proposed DTP before acceptance. One to three sets of changes were made by 67.9% (n = 38), four to six sets of changes by 25.0% (n = 14), and more than six sets of changes were made by 1.8% (n = 1) before the digital plan was accepted. Table 5 shows that final movement protocols and tooth positions were the factors that mainly required changes from the initial DTP received from the CAT provider.
Regarding malocclusion traits, most responders reported feeling more comfortable treating spaced dentitions and mild crowding with CAT (Table 6). Table 7 shows that most respondents rarely or never used CAT in cases that required premolar extraction. Almost half (47.4%, n = 27) of orthodontists reported that they sometimes combined CAT with adjunctive fixed appliances, 40.4% (n = 23) rarely, and 8.8% (n = 5) never in the initial DTP.
Most responders (71.9%, n = 41) did not routinely use Dental Monitoring® (Dental Mind, Paris, France) or other remote monitoring systems compared with 3.5% (n = 2) who always do. Table 8 shows that weekly aligner changes are preferred. The frequency of progress checks of CAT by responders was mainly performed at eight weeks (35.1%, n = 20) and 12 weeks (35.1%, n = 20) (Table 9).
Half of the responders (n = 28) mainly prescribed IPR to address the relief of crowding or reduction of potential dentoalveolar expansion in the initial digital plan (Table 10). Table 11 shows that 50.9% (n = 29) of responders reported that the amount of IPR provided was routinely less than the initial plan. The tools orthodontists considered always or mainly to carry out IPR were the perforated strips and the solid strip tools (Table 12).
The mean percentage of the responder’s annual CAT caseloads requiring one or more refinements was 97.1% (± 4.5). The responders reported a mean of 2.2 (± 1.1) refinements per patient. At the same time, the mean percentage of cases that begin with CAT and are completed with fixed appliances was 5.9% (± 13.1).
Table 13 shows patient-reported CAT-related issues by responders. None of the individuals noted problems occurred with a meaningful frequency. Regarding responders’ opinions on CAT, 20.0% (n = 11) disagreed, and 25.5% (n = 14) strongly disagreed that CAT provides superior treatment outcomes than fixed appliance therapy (Table 14). According to respondents who did not use CAT (n = 3), they decided not to provide CAT because they believe fixed appliance therapy provides better treatment outcomes.
Discussion
In the present study, we investigated CAT practices among orthodontists in Canada. Most respondents reported using CAT in their clinical practice, prescribing it in more than 50 cases annually. These findings reflect a trend due to CAT’s increased popularity and acceptability as an orthodontic treatment modality [1, 6,7,8,9,10,11]. Of approximately 981 orthodontists registered to CAO, 8% accessed the survey, but only 6% completed it. Though our survey experienced a low response rate, the response rate is like related surveys applied in other countries - with higher or lower response rates [1, 6,7,8,9,10,11].
A recent systematic review concluded that, despite low certainty, CAT might be associated with better OHRQoL than fixed appliances [2]. One of the main draws that make patients request CAT is their aesthetic characteristics [2, 11]. In this sample, patient preferences were a significant reported factor influencing decisions to prescribe CAT.
As reported in previous studies, adults comprised most of the patients undergoing CAT [9, 12, 13]. Lately, there has been an apparent rise in the number of teenagers being treated with CAT, potentially attributed to the CAT aesthetic appeal [1, 12, 13].
In our sample, the complexity of the case influenced the decision of most respondents to prescribe CAT, with cases requiring premolar extraction rarely or never being treated with CAT, as reported in previous studies in Australia, the United Kingdom, the Republic of Ireland, the USA, and New Zealand [1, 6,7,8,9,10]. Evidence supports that prescribing CAT is an alternative to fixed appliances in patients with mild-to-moderate malocclusion but not in more severe malocclusion cases [1, 4]. This is possibly due to the perception that CAT is less efficient than fixed appliances in torque control, resulting in less optimal occlusal contacts and post-treatment retention issues [5, 14]. Nearly half of the responders reported occasionally combining CAT with fixed appliances. This suggests that a treatment plan incorporating both approaches can optimize their respective advantages in managing certain malocclusions [6, 9, 15]. Orthodontists’ reports of the need to refine and complete CAT cases with fixed appliances may suggest a limitation in the DTP software to estimate individual tooth movements and treatment outcomes precisely [9, 16].
Jaber et al. suggested that CAT and fixed appliances are equally effective in orthodontic extraction cases [17]. However, treatment duration was shorter with fixed appliances than with CAT, as they offered the advantage of achieving better buccolingual inclination and occlusal contacts in a shorter treatment time [5, 17].
In the present study, most responders use more than one brand, with Invisalign® being the most common. Similar findings were previously found in the United States, the United Kingdom, Australia, and New Zealand [1, 6, 9]. Moreover, brand advertising weakly influences orthodontists’ decision-making regarding CAT prescriptions, whereas the ease and quality of DTP have a moderate or significant impact [3, 9]. Most respondents indicated that they made one to three modifications to the DTP before its approval. A recent survey by Meade et al. (2023) revealed a similar finding in patients undergoing non-extraction treatment with the Invisalign® appliance [6]. Our respondents predominantly cited adjustments from the initial plan related to final movement protocols and tooth positions.
In our sample, orthodontists do not routinely use remote monitoring systems. Current evidence contradicts remote monitoring’s capability to reduce treatment duration and the number of in-person visits [18, 19]. However, remote monitoring is a business decision since its current costs may be a limiting factor [18].
In this survey, most orthodontists reported adopting a weekly aligner change protocol. A randomized clinical trial result indicated that a 7-day protocol appeared effective, as there was no notable clinical distinction compared to protocols lasting 10 or 14 days [20]. Notably, employing a 7-day protocol did lead to a significant reduction in the overall treatment duration. The authors also suggested that, especially in instances necessitating intricate adjustments of posterior teeth, a 14-day interval for changing aligners could prove advantageous [20].
During CAT, IPR is a frequently used technique for creating spaces to align teeth and improve long-term alignment stability [21]. According to the respondents in our sample, the amount of IPR finally provided was expected to be less than initially planned − a pattern consistent with findings from previous investigations [9, 21,22,23]. Overall, these studies have concluded that the in vivo removal of interproximal enamel was generally less than the initially planned IPR. This finding raises the possibility of shortcomings in the DTP, deviations from the initial DTP specifications during IPR implementation, and potential inadequacies in the clear aligners software systems [9]. It has also been suggested that creating interproximal spaces are needed while attempting to move teeth with CAT; the argument is that those spaces improve the grip of the aligner material around the teeth, improving the overall tooth movement efficiency. No references have been identified to support or refute this hypothesis.
In the present study, the belief that fixed appliances provide better outcomes than CAT may have influenced responders’ decision not to prescribe CAT. Nearly half of orthodontists who prescribed CAT disagreed or strongly disagreed that it offered superior results to fixed appliances. Therefore, the finding that orthodontists in the sample believe that CAT does not yield superior treatment outcomes may be because it is indicated based on the case’s complexity, making a “subjective” comparison between CAT and fixed appliance cases challenging.
The limitations included the relatively low response rate and recall bias, which were still higher than in other studies. Another issue we faced was orthodontists’ compliance in answering the lengthy questionnaire, leading to incomplete responses. A saturation of online research in the field may also explain the lack of interest among respondents [24].
In addition, orthodontists who do not prescribe CAT may have declined participation, as the survey explicitly focused on CAT prescription, as indicated in the survey title. Consequently, individuals using CAT might have shown a higher inclination to participate, introducing recruitment bias and potentially leading to overestimating CAT prevalence among respondents.
Conclusions
Within the limitations of this study, the assessment of CAT practices among orthodontists practicing in Canada showed that most of them prescribe CAT. CAT use is based on the malocclusion’s complexity. Furthermore, the ease and quality of the digital planning interface influence the option of a particular aligner company/provider, with one to three modifications to the DTP being more frequently reported before its approval. A mean of 2.2 refinements per patient was reported during treatment.
The amount of IPR performed was believed to be lower than initially planned by the DTP software. Orthodontists who do not prescribe CAT do not do so because they believe that fixed appliance therapy has superior treatment outcomes. The results in the present study broadly match those reported in several recent studies in Australia, the United Kingdom, the Republic of Ireland, the USA, and New Zealand, indicating a broadly similar landscape of CAT practice across all nations thus far surveyed.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CAD:
-
Computer-aided design
- CAM:
-
Computer-aided manufacturing
- CAO:
-
Canadian Association of Orthodontists
- CAT:
-
Clear aligner therapy
- DTP:
-
Digital treatment planning
- IPR:
-
Interproximal enamel reduction
- OHRQoL:
-
Oral health-related quality of life
- REDCap:
-
Research Electronic Data Capture
References
Abu-Arqub S, Ahmida A, Godoy LC, Kuo CL, Upadhyay M, Yadav S. Insight into clear aligner therapy protocols and preferences among members of the American Association of Orthodontists in the United States and Canada. Angle Orthod. 2023;93(4):417–26. https://doi.org/10.2319/101022-694.1.
Kaklamanos EG, Makrygiannakis MA, Athanasiou AE. Oral health-related quality of life throughout treatment with Clear aligners in comparison to conventional metal fixed Orthodontic Appliances: a systematic review. Int J Environ Res Public Health. 2023;20(4):3537. https://doi.org/10.3390/ijerph20043537.
Weir T. Clear aligners in orthodontic treatment. Aust Dent J. 2017;1:58–62. https://doi.org/10.1111/adj.12480.
Yassir YA, Nabbat SA, McIntyre GT, Bearn DR. Clinical effectiveness of clear aligner treatment compared to fixed appliance treatment: an overview of systematic reviews. Clin Oral Investig. 2022;26:2353–70. https://doi.org/10.1007/s00784-021-04361-1.
Upadhyay M, Abu-Arqub S. Biomechanics of clear aligners: hidden truths & first principles. J World Fed Orthod. 2022;11(1):12–21. https://doi.org/10.1016/j.ejwf.2021.11.002.
Meade MJ, Weir T, Seehra J, Fleming PS. Clear aligner therapy practice among orthodontists in the United Kingdom and the Republic of Ireland: a cross-sectional survey of the British Orthodontic Society membership. J Orthod. 2023;13:14653125231204889. https://doi.org/10.1177/14653125231204889.
Keim RG, Iii DSV, Vogels PB. 2020 JCO Study of Orthodontic Diagnosis and treatment procedures part 1: results and trends. J Clin Orthod. 2020;54(10):581–610.
Balteau M, Lefebvre F, Kanter D, Wagner D, Bolender Y. Diagnosis and treatment procedures in French Orthodontic practices. J Clin Orthod. 2021;55(2):83–100.
Meade MJ, Weir T. A survey of orthodontic clear aligner practices among orthodontists. Am J Orthod Dentofac Orthop. 2022;162(6):e302–31. https://doi.org/10.1016/j.ajodo.2022.08.018.
Meade MJ, Weir T. Clear aligner therapy procedures and protocols of orthodontists in New Zealand. Aust Orthod J. 2023;39(2):123–35. https://doi.org/10.2478/aoj-2023-0031.
Hussain SR, Jiang SS, Bosio JA. Generational perspectives of orthodontists in the US and Canada: a survey study. Am J Orthod Dentofac Orthop. 2022;162(6):824–38. https://doi.org/10.1016/j.ajodo.2021.07.020.
Abbate HM, Caria MP, Montanari P, Mannu C, Orrù G, Caprioglio A, et al. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J Orofac Orthop. 2015;76(3):240–50. https://doi.org/10.1007/s00056-015-0285-5.
d’Apuzzo F, Perillo L, Carrico CK, Castroflorio T, Grassia V, Lindauer SJ, et al. Clear aligner treatment: different perspectives between orthodontists and general dentists. Prog Orthod. 2019;20(1):10. https://doi.org/10.1186/s40510-019-0263-3.
Henick D, Dayan W, Dunford R, Warunek S, Al-Jewair T. Effects of Invisalign (G5) with virtual bite ramps for skeletal deep overbite malocclusion correction in adults. Angle Orthod. 2021;91(2):164–70. https://doi.org/10.2319/072220-646.1.
Kravitz ND, Dalloul B, Zaid YA, Shah C, Vaid NR. What percentage of patients switch from Invisalign to braces? A retrospective study evaluating the conversion rate, number of refinement scans, and length of treatment. Am J Orthod Dentofac Orthop. 2023;163(4):526–30. https://doi.org/10.1016/j.ajodo.2022.03.016.
Timm LH, Rößler R, Baxmann M. Comparison of Clear Aligner Treatment in First-Treatment and Re-treatment patients: a retrospective cohort study. Appl Sci. 2023;13(7):4303. https://doi.org/10.3390/app13074303.
Jaber ST, Hajeer MY, Sultan K. Treatment effectiveness of Clear aligners in correcting complicated and severe malocclusion cases compared to fixed Orthodontic Appliances: a systematic review. Cureus. 2023;15(4):e38311. https://doi.org/10.7759/cureus.38311.
Hansa I, Katyal V, Ferguson DJ, Vaid N. Outcomes of clear aligner treatment with and without Dental Monitoring: a retrospective cohort study. Am J Orthod Dentofac Orthop. 2021;159(4):453–59. https://doi.org/10.1016/j.ajodo.2020.02.010.
Lam J, Freer E, Miles P. Comparative assessment of treatment efficiency and patient experience between Dental Monitoring and conventional monitoring of clear aligner therapy: a single-center randomized controlled trial. Am J Orthod Dentofac Orthop. 2023;163(4):456–64. https://doi.org/10.1016/j.ajodo.2022.12.004.
Al-Nadawi M, Kravitz ND, Hansa I, Makki L, Ferguson DJ, Vaid NR. Effect of clear aligner wear protocol on the efficacy of tooth movement. Angle Orthod. 2021;91(2):157–63. https://doi.org/10.2319/071520-630.1.
De Felice ME, Nucci L, Fiori A, Flores-Mir C, Perillo L, Grassia V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog Orthod. 2020;21(1):28. https://doi.org/10.1186/s40510-020-00329-1.
Kalemaja Z, Levrini L. Quantitative evaluation of implemented interproximal enamel reduction during aligner therapy: a prospective observational study. Angle Orthod. 2021;91(1):61–6. https://doi.org/10.2319/040920-272.1.
Weir T, Shailendran A, Kerr, Brett K, Freer E. Quantitative assessment of interproximal tooth reduction performed as part of Invisalign treatment in 10 orthodontic practices. Aust Orthod J. 2021;37(2),176 – 86. https://doi.org/10.21307/aoj-2021-019.
Brosnan K, Kemperman A, Dolnicar S. Maximizing participation from online survey panel members. Int J Market Res. 2021;63(4):416–35. https://doi.org/10.1177/1470785319880704.
Acknowledgements
This study was partly supported by the Coordination for the Improvement of Higher Education Personnel (CAPES – finance code 001).
Funding
D.MP, L.F.MS. & M.C.T. received funding from Coordination for the Improvement of Higher Education Personnel (CAPES – finance code 001) - Government of Brazil.
Author information
Authors and Affiliations
Contributions
D.MP.: conceptualization, data acquisition, formal analysis, writing—original draft preparation; L.F.MS: formal analysis, writing—original draft preparation; M.C.T.: formal analysis, writing—original draft preparation; T.W.: supervision, conceptualization, data acquisition, formal analysis, writing—original draft preparation; M.M.: supervision, conceptualization, data acquisition, formal analysis, writing—original draft preparation; C.FM.: supervision, conceptualization, data acquisition, formal analysis, writing—original draft preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The University of Alberta Research Ethics Board approved this study (IDPro00128404). All participants agreed to participate through a consent form before answering the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Miranda e Paulo, D., Moreira-Santos, L.F., Tavares, M.C. et al. Clear aligner therapy practices among orthodontists practicing in Canada. Prog Orthod. 25, 27 (2024). https://doi.org/10.1186/s40510-024-00525-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40510-024-00525-3