
Abstract
Background
Parental stress often arises when parenting demands exceed the expected and actual resources available for parents to succeed in the parenting role. Parental stress is an important contributor to parent-child relationships. This, in turn, affects opportunities to engage their children in stimulating activities which could improve their development outcomes. However, limited evidence exists from sub-Saharan Africa (SSA) on the association between parental stress, caregiving practices, and child developmental outcomes.
Methods
The findings reported in this paper were derived from data collected through previous longitudinal work on nurturing care evaluation studies in Kisumu and Nairobi Counties in Kenya, and Chisamba District in Zambia. A total of 341 caregivers and their children who participated in the three rounds of data collection were included in this study. The children’s mean age was 9.3 (SD = 8.2) months pre-intervention, 25.5 (SD = 8.6) months in mid-intervention, and 36 (SD = 10.0) months post-intervention. The Ages and Stages Questionnaire (ASQ), Parental Stress Scale (PSS), and caregiving tools were used to assess children’s developmental outcomes, parental stress, and stimulation practices, respectively. A Random Intercept Cross-Lagged Panel model (RI-CLPM) was used to determine the association between caregivers’ parenting stress, child stimulation practices, and child developmental outcomes.
Results
The findings showed that caregiver stimulation practices were positively associated with developmental outcomes. Findings on the associations between parental stress and caregivers’ stimulation practices and children’s developmental outcomes were not universally supported.
Conclusion
The findings show that improved caregiver stimulation practices are likely to improve children’s developmental outcomes. The policy implications of the findings from this study focus on improving parenting practices by addressing the predictors of parental stress. This includes subsidising childcare services to reduce costs.
Trial registration
Pan African Clinical Trials Registry (https://pactr.samrc.ac.za/) database (ID number: PACTR20180774832663 Date: 26/July/2018.
Similar content being viewed by others

Introduction
Parental stress, which often arises when parenting demands exceed the expected and actual resources available for parents to succeed in the parenting role [1], negatively affects parent-child relationships [2, 3]. Therefore, exposure to parental stress during pregnancy and the postnatal period can result in delayed developmental outcomes. Studies have also linked parental stress during pregnancy with an increased risk of premature birth, schizophrenia, and low IQ in the offspring [4, 5]. Similar associations have been reported in previous genomic studies. That is, adversities related to stress have been associated with epigenetic patterns in neonates [6]. Studies examining maternal stress in pregnant women have shown an association between parental stress and transfer (methylation) of the CpG site of the NR3C1 promoter in the cord blood of newborns [7]. Replicated studies have also reported increased NR3C1 DNA methylation in male infants among parents with depression symptoms [8]. NR3C1 is a glucocorticoid (GC) receptor gene, exposure to early-life stressors can alter/result in a life-long increase in GC secretion and may result in disruption of the homeostatic mechanisms regulating hypothalamic-pituitary-adrenal (HPA) axis [9]. Therefore, this predisposes children to the risk of developing stress-related diseases such as anxiety disorders, borderline personality disorder (BPD), mood and affective disorders, and posttraumatic stress disorder (PTSD) [9, 10]. Although there are numerous studies on DNA methylation in child development, questions about its reliability and validity remain, such as understanding stable markers and the period of their stability hinders the replicability of such studies [11].
Notably, parental stress during postnatal has been linked to behavioural problems in children and dysfunctional parenting behaviours [12, 13]. In addition, studies have associated parental stress with parental burnout (physical, mental, and emotional exhaustion) and sleep disorders (disturbed or shortened sleep) [14, 15]. Parental burnout has negative effects on parents’ mental health and overall quality of life which could potentially affect their interactions with their child. A secure parent-child attachment/relationship is a central characteristic of responsive caregiving and child stimulation activities [16]. This implies that caregivers with secure attachments are more sensitive and responsive to their children’s needs and frequently engage their children in stimulation activities. They can modify their instructions/interactions appropriately in reaction to their children’s behaviour. Through this, the caregiver intentionally interacts with the child by carrying out stimulation activities aimed at improving their children’s developmental outcomes.
Regular engagement of children in stimulating/play activities is reported to significantly promote children’s developmental outcomes including fewer behavioural problems, higher intelligence scores, and positive academic outcomes [17]. In addition, play and stimulation activities significantly improve children’s cognitive abilities [18]. This is often observed in a transactional approach where engagement in stimulating activities also increases a parent’s cognitive abilities in subsequent parenting [19]. That is, frequent engagement in play/stimulating activities improves caregiving knowledge and skills, leading them to practice positive parenting in the future.
It is estimated that 250 million children aged less than five years in low- and middle-income countries (LMICs) are at risk of delayed developmental milestones [20]. Over 66% live in sub-Saharan Africa (SSA) and are at risk due to factors such as poor nutrition, family poverty, high Human Immunodeficiency Virus (HIV) prevalence, and under-stimulation in the home environment [21, 22]. Noting that parental stress has been linked to poverty which is salient in SSA, the level of parental stress in low-resource settings in SSA might be higher [23,24,25,26,27]. Limited studies have been done on the contributions of parental stress on child stimulation in sub-Saharan Africa (SSA). Therefore, this study sought to understand the relationship between parental stress, parenting stimulation practices, and children’s developmental outcomes in disadvantaged settings in SSA, as shown in the conceptual framework in Fig. 1.

Conceptual framework on the relationship between parental stress, caregiving practices and developmental outcomes (source; own)
This study aimed to use a dataset from longitudinal nurturing care evaluation studies conducted in Kisumu County in Kenya and the Chisamba District in Zambia [28] to investigate the relationship between parental stress, parenting stimulation practices, and children’s developmental outcomes over time.
The hypotheses of this study were as follows: (a) low parental stress scores are associated with frequent child stimulation practices, (b) low parental stress scores are associated with higher child developmental outcome scores, (c) frequent child stimulation practices are associated with higher child developmental outcome scores, and b) there is a reciprocal association between parental stress, stimulation practices, and child developmental outcomes.
Methodology
Study design
The study reported in this paper was derived from data collected through earlier longitudinal nurturing care evaluation studies conducted in Kisumu County in Kenya and Chisamba District in Zambia [28]. In these two studies, caregiver-child dyads were assigned to either the intervention arm (to receive nurturing care intervention) or the control arm (to receive standard care provided by the Ministry of Health and Ministry of Education in the respective countries). The caregiver-child dyads were drawn from villages/clusters that were purposively selected to ensure a buffer zone between the intervention and the control arms. The intervention was implemented by the Episcopal Relief & Development (ERD) team, together with the Zambia Anglican Council Programmes (ZACOP) in Zambia and with ACK Development Services (ADS) Nyanza in Kenya. The nurturing care intervention program was designed to enhance children’s cognitive, language, motor, social, and emotional development, as well as promote positive discipline and parenting overall. The program was implemented through trained ECD promoters, who facilitated sessions on positive parenting through home visits and support and learning group meetings [29]. The program had an intensive 24-month parental participation timeframe (24 group meetings and 24 ECD home visits). In addition, the project utilised the rich church structure and its wide reach for ECD program delivery to community leaders during weekly Sunday services, faith leaders’ meetings, pastoral visits to households, and cell group meetings. The intervention targeted children aged below three years.
Study sites
This study was conducted in Kenya and Zambia. In Kenya, the research took place in Kisumu County, specifically in Awasi-Onjiko, a sub-location within one ward of the Nyando sub-county. Kisumu County has a population of 1,131,982 individuals, with a growth rate of 2.6%, and is divided into six administrative Sub counties [30]. The county has one provincial hospital, two sub-county hospitals, 16 public health centres, 27 public dispensaries and five private hospitals. There were also four nursing homes and five private dispensaries. The average distance to a health facility is approximately six kilometres, and 67% of the population can access one within five kilometres. However, there are disparities in distance to the nearest health facility. The doctor-to-population ratio is 1:44,634, and the nurse-to-population ratio is 1:2,383. Although antenatal care attendance was relatively high at 71%, most mothers (54%) delivered at home. The proportion of women using contraceptives is low, estimated at 27%, compared to the national average of 46% [30]. The Nyando sub-county comprises five wards, namely, Awasi/Onjiko, Ahero, Kabonyo/Kanyagwal, Kobura, and East Kano/Wawidhi, with a total population of 141,037. Of this population, females account for approximately 49% [30]. The Ministry of Health (MOH) Health Information System (HIS) identified Ayucha, Boda 1, and Wanga’ng’a in Onjiko/Awasi Ward as the most vulnerable areas in the entire Nyando sub-county and recommended implementing nurturing care interventions at these sites.
In Zambia, the study was conducted in the Mwantaya and Chamuka wards, situated in Chisamba District in Central Province. The population of Chisamba district in 2010 was 103,983, and it had a higher HIV prevalence rate than the national average in rural Zambia (13.4%) [31]. Moreover, malnutrition rates were also high, with 42.1% of children under the age of five exhibiting stunted growth. Only 46.5% of the mothers had skilled professionals attending their deliveries, and fewer than a quarter (14.4%) of the population lacked formal education. According to 2010 data, Chamuka Ward had a population of 21,210, with 10,685 males and 10,525 females living in 3833 households. Mwantaya Ward had very little infrastructure and only one health clinic, despite being sparsely populated [31].
Participants
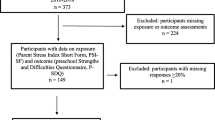
In rural Zambia, the survey design was a cluster-randomised controlled trial, in which the cluster was the community. The study team followed Hemming and Girling’s [32] study for sample size calculation by fixing the number of clusters to at least five in each arm. Hence, they assumed that the intervention could yield an effect size of 0.4 in terms of ECD parenting practices with an intracluster correlation (ICC) of = 0.03. The team also estimated a confidence interval of 95%, a margin of error of 5%, a power of 80%, and an attrition rate of 10%. Thus, the total sample size for each arm was 255 (510 primary caregivers in total). However, only 395 primary caregivers met the inclusion criteria; children aged below 18 months or who were pregnant and in their third trimester were identified and recruited from the households. Of the 395 caregivers recruited, 176 participated in the three rounds of data collection (pre-intervention, mid-intervention, and post-intervention).
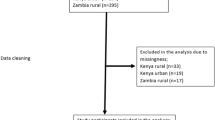
In rural Kenya, the survey was a cluster quasi-experiment, in which the cluster was a village nested in a ward. The study team followed Hemming and Girling’s [32] study for sample size calculation by fixing the number of clusters to at least five in each arm. There were two project implementation sites: three clusters at each site. Due to limited resources, with six clusters in each arm, the ICC was set at 0.02, the effect size at 0.43, and the dropout rate at 10%. With this information, the total number of caregivers in each arm was 129, and the cluster size was 21.5 caregivers. Due to rounding issues, the cluster size was 22 caregivers and the number of caregivers per arm was 132 caregivers, implying a total sample size of 264 for the two arms. Of the 264 caregivers recruited, 165 were included in the analysis. They participated in three rounds of data collection and were eligible for the collection of the outcome and predictor variables. The outcome variable was collected from children aged one month to 60 months; therefore, only children aged between 1 month and 36 months pre-intervention were included in this study. The total number of participants from the two study sites who were included in this study was 341 (Fig. 2).

The flow of study participants
Measures
Using questionnaires, information on caregivers’ socio-demographics, caregiving knowledge, attitudes and practices, and health-seeking behaviour was collected. The parental stress scale and the Ages and Stages Questionnaire (ASQ) were used to assess parental stress and child development, respectively. The predictors (PSS and stimulation practices) and outcomes (ASQ) were included in the primary caregiver questionnaire. The questionnaire was administered by trained field interviewers and the average duration of each interview was estimated to be one hour. Interviews and child assessments were conducted at caregivers’ homes. Quality control was ensured through spot checks, supervision, and weekly team debriefs.
Outcomes
The main outcome of this study was child development. These included gross and fine motor skills and language, socio-emotional, and cognitive development measured using the Ages and Stages Questionnaire– Third Edition (ASQ-3) [33]. This was done through a combination of primary caregiver self-reported questions and direct observations by trained field interviewers, similar to the procedures used in a study conducted in South Africa and Zambia [34]. Apart from self-reports, primary caregivers were requested to try each activity with their children to facilitate an accurate item assessment. Items were scored ‘yes’ (= 10 points) if the child was able to perform the activity, ‘sometimes’ (= 5 points) if the child tried and failed but the primary caregiver reported that the child could perform the activity sometimes, and ‘no’ (= 0 points) if the child was unable to perform the item. The responses to each domain’s six questions were summed to obtain a score for each area. The scores for each domain range from 0 to 60. Higher scores indicated outcomes that were more positive for children. To calculate the total ASQ score, the total score in each domain was summed, and the total score ranged from 0 to 300. The internal consistency of the ASQ tool was determined for the total score by using Cronbach’s alpha, and the result was 0.79.
Predictors
The first predictor was the caregiver’s parental stress level. The Parenting Stress Scale (PSS) has 18 questions that assess the level of parenting stress [35]. The PSS tool has been previously used in South Africa [36], and studies on its validity and reliability have indicated good internal consistency, construct validity, convergent validity, and test-retest reliability [35, 37,38,39,40,41]. In this study, the PSS tool was translated into the local languages of Dholuo in Kenya, Nyanja, and Tonga Zambia. These questions were asked before the intervention (pre-intervention), one year into the intervention (mid-intervention), and at the end of the intervention (the intervention period was two years). The PSS tool was used to obtain information from parents about their feelings and perceptions of their parenting experiences. In each dataset, the caregiver’s PSS responses were assigned scores (5-point Likert Scale; 1 = Strongly Disagree, 2 = Disagree, 3 = Not Sure, 4 = Agree, 5 = Strongly Agree). To compute the parental stress score, items 1, 2, 5, 6, 7, 8, 17, and 18 which were positively worded were reversed and scored as follows: (1 = 5) (2 = 4) (3 = 3) (4 = 2) (5 = 1). The item scores were then summed up. A low score signified a low level of stress, whereas a high score indicated a high level of stress. The overall possible scores on the scale ranged from 18 to 90.
Caregivers’ play and stimulation practices were the second predictors. A structured questionnaire was used to collect information on the caregivers’ parenting practices in each developmental domain. The questionnaire was adopted from nurturing care intervention program activities [29]. They were asked a set of questions to establish engagement in the child’s stimulation in the previous week in each developmental domain (cognitive, language, motor skills, social, and emotional development). Their practices were reported and scored as follows: Yes = 1 and No = 0. The total expected score (highest score) in each domain was cognitive = 6; language = 6; motor skills = 4; social = 5; and emotional development = 5. To calculate the total practice scores, the total score in each domain was summed, and the total score ranged from 0 to 26.
Statistical analysis
The data were cleaned and analysed using R software and R Studio [42]. Our analysis commenced with descriptive statistics of participants’ demographic characteristics. We also assessed the internal consistency of the ASQ, PSS, and stimulation practice questionnaire by using Cronbach’s alpha. Our findings revealed acceptable internal consistency for the total ASQ (0.79), total PSS (0.79), and total practice score (0.77) [43].
We then explored the association between parental stress, caregivers’ practices, and children’s developmental outcomes at the three-time points using an extension of a Random Intercept Cross-Lagged Panel Model (RI-CLPM) in R [44]. The RI-CLPM regression model was used to explore the association between two or more variables measured repeatedly over time. Using the RI-CLPM regression model, we were able to estimate within- and between-person effects as well as adjust for between-person covariates, such as demographic characteristics and intervention [45, 46]. The model allowed for the investigation of time-lagged associations between parenting stress, practices and child developmental outcomes. In addition, the model allowed us to explore reciprocity in the association between parental stress, stimulation practices, and child development at each time point. Further, we conducted a child developmental domain-specific model (personal social, problem-solving, communication, gross motor, and gross motor) as outcome variables and PSS and stimulation practices and predictors. This enabled us to check whether the association between PSS, stimulation practices, and child developmental outcomes was domain-specific. Our sensitivity analysis was performed using a multi-group model to assess whether there was a major difference between the results for participants in the intervention arm. The models were fitted using Lavaan.survey to account for the clustered structure of the data. The results showed no major differences between the two groups. Full analysis code is provided at OSF. To assess the model fit, we used the Comparative Fit Index (CFI), Tucker–Lewis’s index (TLI), Standardised Root Mean Square Residual (SRMR), and Root Mean Square Error of Approximation (RMSEA). Good fit was judged based on values greater than or equal to 0.95 for CFI and TLI, and less than or equal to 0.06 for SRMR and RMSEA [47].
Ethical considerations
Permission to use the current datasets was sought from the African Population and Health Research Centre (APHRC). Among the studies that collected the data, ethical approval was obtained from institutional review boards (IRBs) in Kenya and Zambia to conduct the research in their respective countries. Written informed consent was obtained from the study participants (parents/guardians) before data were collected. For respondents who could neither read nor write, a witnessed thumbprint was used to sign a consent form. Consent was obtained at every round of data collection. Consent documents and questionnaires were translated into Dholuo, the local dialect of the Kenyan rural study site, and Nyanja and Tonga, the local dialects of the Zambia rural study site. Confidentiality of the data and the participants’ privacy were observed during and after data collection. These rural studies were registered under the trial registration number PACTR20180774832663.
Results
Demographic characteristics
All participants in this study were female primary caregivers. That is biological mothers or those aged above 18 years whose primary responsibility was taking care of the child. Their demographic characteristics remained stable across the phases of this study, with a slight upward trajectory in the proportion of those who reported being married, ages ranging from 20 to 39 years, education above primary level, and with more than one child. Notably, there was a significant increase in the proportion of caregivers who reported earnings between USD 76 and USD 100 per month at both study sites. On the children’s demographic, slightly above the average were females (male; 48.4% and 51.6%), the children's mean age was 9 months at pre-intervention, 21 months at mid-intervention and 33 months at post-intervention as shown in Table 1).
Parental stress score, stimulation activities and children’s developmental scores
From the findings, the mean total ASQ score increased from pre-intervention to post-intervention for Zambia study sites (pre-intervention; 163.3 (SD = 106.5), mid-intervention; 240.0 (SD = 53.2) and post-intervention; 242.2 (SD = 51.1)). In Kenya, the mean total ASQ score increased from pre-intervention to mid-intervention and then decreased slightly from mid-intervention to post-intervention (pre-intervention: 174 (SD = 108.1), mid-intervention; 236.7 (SD = 55.6), and post-intervention; 221.0 (SD = 73.8)). However, the mean total ASQ score was higher for Zambia than for Kenya at two-time points (mid- and post-intervention), and the difference between the sites was larger post-intervention than pre-intervention. Regarding the stimulation practices, a similar trend was observed with an increase from pre-intervention to post-intervention in the Zambia study site (pre-intervention; 12.3 (SD = 8.0), mid-intervention; 20.8 (SD = 5.1), and post-intervention; 21.3 (SD = 5.8)) and a slight decrease from mid-intervention to post-intervention in the Kenya study site (pre-intervention; 12.7 (SD = 6.6), mid-intervention; 21.7 (SD = 3.2), and post-intervention; 21.3 (SD = 6.2)). This trend was also observed in PSS scores in Zambia (pre-intervention; 43.2 (SD = 9.2), mid-intervention; 37.0 (SD = 9.8) and post-intervention; 36.5 (SD = 9.1)) while in Kenya (pre-intervention; 39.1 (SD = 11.1), mid-intervention; 35.0 (SD = 10.1) and post-intervention; 37.5 (SD = 10.2)) as shown in Fig. 3A, B and C.

(A) ASQ scores by round compared by study sites. (B) Parental stress scores by round compared by study sites. (C) Stimulation practice scores by round compared by study sites
Association between parental stress, stimulation activities and child developmental outcomes
Combined study sites
When fitting the extended Random Intercept Cross-Lagged Panel Model (RI-CLPM) on the combined study site, the results showed a good fit, with CFI, TLI, RMSEA, and SRMR values of 1, 0.99, 0.016, and 0.008, respectively. Regarding the association between stimulation practices and child developmental outcomes, the findings showed that primary caregivers of children with better ASQ scores at T1 had higher stimulation practices at T0 (T1; β = 0.21, P =.02*). The findings from this study also indicated that primary caregivers of children with better ASQ scores had higher stimulation practices (reciprocal association) at all study points (TO: β = 0.64, P <.01***; T1: β = 0.27, P <.01***; and T2: β = 0.56, P <.01***). The findings on parental stress showed that primary caregivers with higher PSS reported reduced stimulating practices at T1 and T2 (T1: β = -0.19, P =.01** and T2; β = 0.30, P <.01***). In addition, primary caregivers of children with low ASQ scores reported higher PSS scores at T2 (β = -0.17, P =.01**). (Fig. 4A; Table 2).

(A) Random intercept cross-lagged panel model of parental stress, stimulation practices, and ASQ– Combined study sites. (B) Random intercept cross-lagged panel model of Parental stress, stimulation practices, and ASQ– Zambia rural study sites. (C) Random intercept cross-lagged panel model of parental stress, stimulation practices, and ASQ– Kenya rural study sites. Notes: T0 = pre-intervention, T1 = mid-intervention, T2 = post-intervention. The broken lines denote insignificant paths
Zambia rural study site
When fitting the RI-CLPM model to the Zambian rural site, the results showed a good fit, with CFI, TLI, RMSEA, and SRMR values of 1.0, 1.1, 0.00, and 0.05, respectively. Regarding the association between stimulation practices and child developmental outcomes, the findings showed that primary caregivers of children with better ASQ scores at T1 had higher stimulation practices at T0 (T1; β = 0.32, P =.06). The findings from this study also indicated that primary caregivers of children with better ASQ scores had higher stimulation practices (reciprocal association) at all study points (TO: β = 0.80, P <.01***; T1: β = 0.30, P =.01**; and T2: β = 0.35, P <.01***). Regarding parental stress, the findings showed that primary caregivers with higher PSS reported reduced stimulating practice at T2 (T2: β = -0.43, P <.01***). In addition, primary caregivers of children with higher ASQ scores at T1 reported higher PSS scores at T0 (T1; β = 0.24, P =.01**), as shown in Fig. 4B; Table 2.
Kenya rural study site
When the RI-CLPM model was fitted to the Kenyan rural site, the results showed acceptable CFI, TLI, RMSEA, and SRMR values of 0.99, 0.98, 0.024, and 0.022, respectively. The association between stimulation practices and child developmental outcomes, the findings show that primary caregivers of children with better ASQ scores at T1 had higher stimulation practices at T0 (T1; β = 0.22, P =.04*).
The findings from this study also indicated that primary caregivers of children with better ASQ scores had higher stimulation practices (reciprocal association) at all study points (TO: β = 0.50, P =.01**; T1: β = 0.24, P =.01**; and T2: β = 0.70, P <.01***). Regarding parental stress, primary caregivers with higher PSS reported low stimulating practice scores, and their children also reported low ASQ scores at T2 (Practices: β = 0.21, P =.03* and ASQ; β = 0.22, P =.03*), as shown in Fig. 4C; Table 2.
We conducted an exploratory analysis to determine whether the association between parental stress and stimulation practices and child developmental outcomes was domain-specific. Our findings revealed a similar trend of mixed findings on the association between PSS and overall stimulation practice and total ASQ scores. In addition, the positive association between parental stress T0 and child development outcome T1 in the Zambia study site was only observed in the communication, personal social, and problem-solving domains (personal social; β = 0.26, P =.05*, communication; β = 0.31, P =.01** and problem-solving; β = 0.24, P =.01**).
Discussion
This study aimed to establish the association between parental stress, stimulation practices, and child developmental outcomes using datasets from longitudinal studies in two different African regions (rural Kenya and rural Zambia). The main findings of this study suggest a significant association between caregivers’ stimulation practices and children’s development outcomes. The association between parental stress and stimulation practices was observed only at the Kenya study site. Even though an association between parental stress and child developmental outcomes was observed in both countries, the positive association reported in Zambia was surprising.
Results from this study, though inconsistent across the study sites, show that parental stress was negatively associated with stimulation activities and child developmental outcomes. We speculate that this difference between study sites could be attributed to the different study designs used and other country-specific socioeconomic factors. These findings on the association between PSS and stimulation activities mirror those of other studies that have shown parental stress to be an inhibitor of caregivers’ participation in child-stimulating activities. As pointed out in other studies, excessive parental stress can induce negative and problematic interactions between parents and children, leading to dysfunctional parenting behaviour [48,49,50]. In studies among parents of preschoolers, parental stress was associated with dysfunctional parent-child interactions [49, 50]. Therefore, this affects opportunities for interaction and engagement of their children in stimulating activities. Similar findings were also observed in a meta-analysis in which parental stress was identified as a predictor of harsh parenting practices [51]. The moderate association observed in this study also conforms to other studies on parental stress and satisfaction [52].
Noting that early years form a critical period for children’s growth and development, engagement in stimulating activities promotes optimal growth and development. Studies focusing on early deprivation and institutionalisation of children have also supported early stimulation for optimal development across all domains [53]. Due to the high brain plasticity at this age, positive early experiences, such as play and stimulation, have a major influence on a child’s future cognitive, psychomotor, social-emotional and language development. In addition, developmental delays in early childhood might lead to long-term issues such as low academic and educational achievement, increased risk of criminal behaviour, and low income in adulthood. Such findings were also evident in the current study, with positive associations between caregivers’ stimulation practices and children’s ASQ scores, indicating that frequent engagement in stimulating activities can improve developmental outcomes. Therefore, children who frequently engaged in stimulating activities were more likely to have improved developmental outcomes.
However, the positive association observed between PSS scores at T0 and ASQ T1 at the Zambia rural study site was surprising. This implies that despite their stress level, such parents might have a higher awareness of the importance of engaging their children in stimulating activities and adequate resources to care for their children. Despite this, the negative associations demonstrated in this study, although not statistically significant, indicate that it is essential to address parental stress which has been identified as a risk factor associated with reduced stimulation practices and child developmental outcomes.
Strategies geared towards improving parental stress levels could be focused on addressing the background factors underlying parental stress, including poverty and low caregiver education [54]. On the other hand, to improve parent-child interaction and maximise opportunities for stimulation activities, global studies have shown that targeted interventions enhance mother-child interactions and increase developmental outcomes [55]. This systematic review documented evidence of such interventions in Bangladesh, China, India, and South Africa which were implemented through home visits, individual parent counselling sessions delivered through health facilities, and combined home visits and health facilities. Such interventions can be replicated in the SSA context to improve stimulation practices.
Study limitations
Despite the longitudinal nature of our study, we could not confidently draw a conclusive link between parental stress, parenting practices, and child development based on these findings. The frequency of practice reported in this study was limited to one week. Noting that the data from this study came from two distinct trials with different study designs, it might be difficult to separate naturally occurring effects and effects related to the intervention. Another limitation of this study is that the data on parental stress and stimulation practices were self-reported, which could have introduced reporting biases, such as social desirability. In addition, although the study utilised datasets from two different settings, these findings may only be generalised to populations with similar characteristics. This, therefore, makes these findings indicative of such associations but does not prove that they are causal.
Future studies should focus on the frequencies of stimulation activities and real-time measurements of the effects of parental stress on stimulation activities and child developmental outcomes. The utilisation of Ecological Momentary Assessment (EMA) methods coupled with technology (wearable sensors such as actigraphy sensors) in the SSA setting could generate further evidence of the associations between PSS, child stimulation practices, and children’s developmental outcomes [56].
Conclusion and policy implications
This study examined the associations between parental stress, parental stimulation activities, and child developmental outcomes among caregivers in low-resource SSA settings. The findings consistently showed a significant positive association between stimulation practices and children’s developmental outcomes at all the study sites. However, the association between parental stress, stimulation practices, and child developmental outcomes was not universally supported across the two study sites. The findings of this study, therefore, contribute to the evidence of the associations between PSS, parenting/child stimulation practices, and child developmental outcomes. Due to the significance of early stimulation to the child’s optimal growth and development, these findings highlight the need for policies and interventions aimed at preventing or reducing parental stress and boosting or enhancing child stimulation practices. This can be achieved by addressing poverty, low parental education, and other factors that underlie parental stress.
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ASQ:
-
Ages and Stages Questionnaire
- ECD:
-
Early Childhood Development
- ESRC:
-
Ethics and Scientific Review Committee
- IRB:
-
Institutional Review Board
- PSS:
-
Parental Stress Score
- SSA:
-
Sub-Saharan Africa
References
Abidin R, Flens JR, Austin WG. The parenting stress index. Forensic uses of clinical assessment instruments. edn. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 2006. pp. 297–328.
Lo CKM, Chen MT, Chen QQ, Chan KL, Ip P. Social, Community, and Cultural Factors Associated with parental stress in fathers and mothers. Int J Env Res Pub He 2023, 20(2).
Schroder M, Seker S, D’Huart D, Izat Y, Bolten M, Schmeck K, Schmid M. The relationship of temperament and character, parental stress, and Mental Health problems with attachment disorders among children. Int J Env Res Pub He 2022, 19(23).
Malaspina D, Corcoran C, Kleinhaus KR, Perrin MC, Fennig S, Nahon D, Friedlander Y, Harlap S. Acute maternal stress in pregnancy and schizophrenia in offspring: a cohort prospective study. BMC Psychiatry 2008, 8.
Wadhwa PD, Entringer S, Buss C, Lu MC. The contribution of maternal stress to Preterm Birth: issues and considerations. Clin Perinatol. 2011;38(3):351–.
Gluckman PD, Hanson MA, Pinal C. The developmental origins of adult disease. Matern Child Nutr. 2005;1(3):130–41.
Hompes T, Izzi B, Gellens E, Morreels M, Fieuws S, Pexsters A, Schops G, Dom M, Van Bree R, Freson K, et al. Investigating the influence of maternal cortisol and emotional state during pregnancy on the DNA methylation status of the glucocorticoid receptor gene (NR3C1) promoter region in cord blood (vol 47, pg 880, 2013). J Psychiatr Res. 2014;56:165–7.
Braithwaite EC, Kundakovic M, Ramchandani PG, Murphy SE, Champagne FA. Maternal prenatal depressive symptoms predict infant NR3C1 1F and BDNF IV DNA methylation. Epigenetics-Us. 2015;10(5):408–17.
Bockmuhl Y, Patchev AV, Madejska A, Hoffmann A, Sousa JC, Sousa N, Holsboer F, Almeida OFX, Spengler D. Methylation at the CpG island shore region upregulates Nr3c1 promoter activity after early-life stress. Epigenetics-Us. 2015;10(3):247–57.
Heim C, Binder EB. Current research trends in early life stress and depression: review of human studies on sensitive periods, gene-environment interactions, and epigenetics. Exp Neurol. 2012;233(1):102–11.
Murgatroyd C, Spengler D. Epigenetics of early child development. Front Psychiatry 2011, 2.
Lovejoy MC, Graczyk PA, O’Hare E, Neuman G. Maternal depression and parenting behavior: a meta-analytic review. Clin Psychol Rev. 2000;20(5):561–92.
Fang Y, Luo J, Boele M, Windhorst D, van Grieken A, Raat H. Parent, child, and situational factors associated with parenting stress: a systematic review. Eur Child Adoles Psy 2022.
Merrill RM, Slavik KR. Relating parental stress with sleep disorders in parents and children. PLoS ONE. 2023;18(1):e0279476.
Ping YF, Wang W, Li YM, Li YX. Fathers’ parenting stress, parenting styles and children’s problem behavior: the mediating role of parental burnout. Curr Psychol 2022.
Dunst CJ, Kassow DZ. Caregiver sensitivity, contingent social responsiveness, and secure infant attachment. J Early Intensive Behav Intervention. 2008;5:40–56.
Nijhof SL, Vinkers CH, van Geelen SM, Duijff SN, Achterberg EJM, van der Net J, Veltkamp RC, Grootenhuis MA, van de Putte EM, Hillegers MHJ, et al. Healthy play, better coping: the importance of play for the development of children in health and disease. Neurosci Biobehav R. 2018;95:421–9.
Merz EC, Landry SH, Montroy JJ, Williams JM. Bidirectional associations between parental responsiveness and executive function during early childhood. Soc Dev. 2017;26(3):591–609.
Tucker-Drob EM, Harden KP. Early childhood cognitive development and parental cognitive stimulation: evidence for reciprocal gene-environment transactions. Dev Sci. 2012;15(2):250–9.
Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu CL, McCoy DC, Fink G, Shawar YR, Shiffman J, et al. Early childhood development coming of age: science through the life course. Lancet. 2017;389(10064):77–90.
Agrawal D, Chaudhary P, Pathak P. Promoting Nurturing Care for early Childhood Development through India’s Public Health System. Indian Pediatr. 2021;58(Suppl 1):23–S27.
Britto PR, Lye SJ, Proulx K, Yousafzai AK, Matthews SG, Vaivada T, Perez-Escamilla R, Rao N, Ip P, Fernald LCH, et al. Nurturing care: promoting early childhood development. Lancet. 2017;389(10064):91–102.
Okelo K, Onyango S, Murdock D, Cordingley K, Munsongo K, Nyamor G, Kitsao-Wekulo P. Parent and implementer attitudes on gender-equal caregiving in theory and practice: perspectives on the impact of a community-led parenting empowerment program in rural Kenya and Zambia. BMC Psychol. 2022;10(1):162.
Oyarzun-Farias MLA, Cova F, Bustos Navarrete C. Parental stress and satisfaction in parents with Preschool and School Age Children. Front Psychol. 2021;12:683117.
Parkes A, Sweeting H, Wight D. Parenting stress and parent support among mothers with High and Low Education. J Fam Psychol. 2015;29(6):907–18.
Qian GY, Mei J, Tian L, Dou G. Assessing Mothers’ Parenting Stress: Differences Between One- and Two-Child Families in China. Front Psychol 2021, 11.
Santiago CD, Kaltman S, Miranda J. Poverty and Mental Health: how do low-income adults and children fare in psychotherapy? J Clin Psychol. 2013;69(2):115–26.
Kitsao-Wekulo P, Okelo K, Murdock D, Donfouet HP, Onyango SO, Mwangi B, Illboudo P, Wanjohi MN, Nyamor G, Munsongo K, Kimani-Murage E. An evaluation of the effectiveness of a community-based parenting empowerment program to improve nurturing care of young children in Kenya and Zambia. The African Population and Health Research Center: Nairobi, Kenya. In.: African Population & Health Research Centre; 2021.
Murdock DE, Munsongo K, Nyamor G. Scaling the moments that Matter® early childhood development model: how communities’ monitoring for change contributes to sustainable impact. Front Public Health 2023, 11.
KNBS.: Kenya Population and Housing Census Volume I: Population by county and sub-county. In.; 2019.
(CSO) CSO. Zambia. Zambia Demographic and Health Survey 2013-14. Lusaka. In.; 2015.
Hemming K, Girling AJ, Sitch AJ, Marsh J, Lilford RJ. Sample size calculations for cluster randomised controlled trials with a fixed number of clusters (vol 11, 102, 2011). Bmc Med Res Methodol 2017, 17.
Ages. & Stages Questionnaires®, Third Edition (ASQ®-3): A Parent-Completed Child Monitoring System.
Hsiao C, Richter L, Makusha T, Matafwali B, van Heerden A, Mabaso M. Use of the ages and stages questionnaire adapted for South Africa and Zambia. Child Care Hlth Dev. 2017;43(1):59–66.
Berry JO, Jones WH. The parental stress scale - initial psychometric evidence. J Soc Pers Relat. 1995;12(3):463–72.
Massarwi AA, Cluver L, Meinck F, Doubt J, Green O. Pathways to parenting stress reduction among parents in South Africa. Child & Family Social Work. 2023;28(1):184–93.
Algarvio S, Leal I, Maroco J. Parental stress scale: validation study with a Portuguese population of parents of children from 3 to 10 years old. J Child Health Care. 2018;22(4):563–76.
Harding L, Murray K, Shakespeare-Finch J, Frey R. Understanding the parental stress scale with a Foster Carer Cohort. Fam Relat. 2020;69(4):865–79.
Leung C, Tsang SKM. The Chinese parental stress scale: psychometric evidence using rasch modeling on clinical and nonclinical samples. J Pers Assess. 2010;92(1):26–34.
Pontoppidan M, Nielsen T, Kristensen IH. Psychometric properties of the Danish parental stress scale: Rasch analysis in a sample of mothers with infants. PLoS ONE 2018, 13(11).
Zelman JJ, Ferro MA. The parental stress scale: Psychometric properties in families of children with Chronic Health conditions. Fam Relat. 2018;67(2):240–52.
Team RC. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. http://www.R-projectorg/ 2016.
Hornman J, Kerstjens JM, de Winter AF, Bos AF, Reijneveld SA. Validity and internal consistency of the ages and stages Questionnaire 60-month version and the effect of three scoring methods. Early Hum Dev. 2013;89(12):1011–5.
Mulder JD, Hamaker EL. Three extensions of the Random Intercept Cross-lagged Panel Model. Struct Equ Modeling. 2021;28(4):638–48.
Hamaker EL, Kuiper RM, Grasman RP. A critique of the cross-lagged panel model. Psychol Methods. 2015;20(1):102–16.
Lüdtke O, Robitzsch A. A Critique of the Random Intercept Cross-Lagged Panel Model. PsyArXiv 2021.
Pakpahan E, Hoffmann R, Kröger H. Statistical methods for causal analysis in life course research: an illustration of a cross-lagged structural equation model, a latent growth model, and an autoregressive latent trajectories model. Int J Social Res Methodology: Theory Pract. 2017;20:1–19.
Crnic KA, Gaze C, Hoffman C. Cumulative parenting stress across the preschool period: relations to maternal parenting and child behaviour at age 5. Infant Child Dev. 2005;14(2):117–32.
Chew Xing Jiun WMWJ, and Nor Mazlina Ghazali. The relationship between parenting stress and Perceived Children’s Social Problem Behavior among Chinese Working Mothers. Int J Social Sci Humanity. 2016;6(3):157–64.
Kwon JY. The relationship between parenting stress, parental intelligence and child behavior problems in a study of Korean preschool mothers. Early Child Development and Care. 2007;177(5):449–60.
Rueger SY, Katz RL, Risser HJ, Lovejoy MC. Relations between parental affect and parenting behaviors: a Meta-Analytic Review. Parenting. 2011;11(1):1–33.
Ribeiro MF, Porto CC, Vandenberghe L. [Parental stress in families of children with cerebral palsy: an integrative review]. Cien Saude Colet. 2013;18(6):1705–15.
Werchan DM, Ku S, Berry D, Blair C. Sensitive caregiving and reward responsivity: a novel mechanism linking parenting and executive functions development in early childhood. Dev Sci 2022.
Kenneth Odhiambo Okelo BA, Josiah K, et al. Sociodemographic predictors of parenting stress among caregivers in disadvantaged settings: evidence from Kenya and Zambia. Research Square; 2023.
Walker SP, Wachs TD, Grantham-McGregor S, Black MM, Nelson CA, Huffman SL, Baker-Henningham H, Chang SM, Hamadani JD, Lozoff B, et al. Inequality in early childhood: risk and protective factors for early child development. The Lancet. 2011;378(9799):1325–38.
Russell MA, Gajos JM. Annual Research Review: ecological momentary assessment studies in child psychology and psychiatry. J Child Psychol Psychiatry. 2020;61(3):376–94.
Acknowledgements
Bonnie Auyeung was supported by the European Union’s Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie grant agreement No.813546, the Baily Thomas Charitable Fund TRUST/VC/AC/SG/469207686, the Data-Driven Innovation and the UK Economic and Social Research Council (ES/W001519/1) during this work. We also gratefully acknowledge the contributions of the data collectors in Kenya and Zambia. Our work benefited from the input of many people, not least from the participation of survey respondents.
Funding
These studies were funded by the Episcopal Relief and Development funded this study with grants from the Conrad N. Hilton Foundation, Grand Challenges, Canada, and Other Donors.
Author information
Authors and Affiliations
Contributions
K.O. - Questionnaire development, data collection, manuscript concept, manuscript writing, statistical analysis, discussion, corresponding author. A.L.M. - Statistical analysis, theoretical framework, manuscript concept, manuscript writing. J.K. - Statistical analysis, manuscript concept, and manuscript writing. P.K.-W. - Project manager, data collection, questionnaire development, manuscript writing. S.O. - Questionnaire development data collection data recapitulation, manuscript writing. M.N. - Questionnaire development data collection data recapitulation, manuscript writing. B.A. - theoretical framework, manuscript concept, manuscript writing discussion, overall guidance. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Permission to use these datasets was granted by the African Population and Health Research Centre (APHRC). The APHRC obtained ethical approval from the Institutional Review Boards (IRBs) of Kenya and Zambia to conduct these studies. Written informed consent was obtained from the study participants before data were collected. For respondents who could neither read nor write, a thumbprint was used as a signature in the presence of a witness. Consent was obtained at every round of data collection. Consent documents and the questionnaire were translated into Dholuo (for the Kenyan rural study site) and Nyanja and Tonga (for the Zambia rural study site). Confidentiality of the data and the participants’ privacy were always observed during and after data collection. These studies were registered under the trial registration number PACTR20180774832663. In addition, all methods were carried out in accordance with the relevant guidelines and regulations of the Declaration of Helsinki. For example, respect for individuals, the right to make informed decisions, and the recognition of vulnerable groups.
Informed consent process
The data collectors sought informed consent from all study participants before they were interviewed. For those who were unable to read, the information sheet was read to them in their local language and they were asked to provide a thumbprint to signify their consent. Ethical research committees in both countries approved the use of a thumbprint or signature. The ethical research committees in both countries approved the use of a thumbprint or signature (Amref Health Africa’s Ethics and Scientific Review Committee in Kenya and the ERES Converge in Zambia).
Consent for publication
Not applicable.
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Okelo, K., Murray, A.L., King, J. et al. Parental stress and child stimulation practices: examining associations with child developmental outcomes over time in Kenya and Zambia. BMC Psychol 12, 50 (2024). https://doi.org/10.1186/s40359-024-01533-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-024-01533-y