
Abstract
Background
SuperAging is one of the current concepts related to elite, resilient or high-functioning cognitive aging. The main aim of our study was to find possible predictors of SuperAgers (SA).
Methods
Community-dwelling older persons (N = 96) aged 80–101 years in 2018 were repeatedly tested (year 2012 and 2018). SA were defined based on their performance in 2018 as persons of 80+ years of age who recalled ≥ 9 words in the delayed recall of the Philadelphia Verbal Learning Test, and had a normal performance in non-memory tasks [the Boston Naming Test, the Trail Making Test Part B, and Category Fluency (“Animals”)], which was defined as a score within or above one standard deviation from the age and education appropriate average. Three composite scores (CS; immediate memory, processing speed, and executive functions) were created from the performance in 2012, and analysed as possible predictors of SA status in 2018.
Results
We identified 19 SA (15 females) and 77 nonSA (42 females), groups did not significantly differ in age, years of education, and sex. The logistic regression model (p = 0.028) revealed three predictors of SA from the baseline (year 2012), including processing speed (p = 0.006; CS-speed: the Prague Stroop Test—Dots and the Digit Symbol Substitution Test), sex (p = 0.015), and age (p = 0.045).
Conclusions
Thus, SA may be predicted based on the level of processing speed, which supports the hypothesis of the processing speed theory of healthy aging.
Similar content being viewed by others

Background
Longer life expectancy and global aging of societies promote research of the spectrum of cognitive aging, which directly affects self-sufficiency and indirectly economic and labour issues related to both formal and informal care [1,2,3].
After decades of research of pathological cognitive decline, an area of research of cognitive resilience, elite cognitive aging or SuperAging has emerged. Definitions of superior cognition in old age vary, but each has precise criteria [4]. Most studies of superior or resilient cognitive aging use individuals of 65 years or younger as reference groups, which from a biological point of view is a better design than using an age-appropriate reference group, since the decline of cognitive functions and the thinning of brain regions through aging is not linear but rather non-linear [4,5,6,7,8].
The term SuperAging was coined by the Northwestern Mesulam Center for Cognitive Neurology and Alzheimer’s Disease. SuperAgers (SA) were defined as individuals over the age of 80 with episodic memory performance at least as good as normative values for 50–65-year-olds, while their non-memory performance is on the mean level of their peers [9, 10]. In other words, we might say that SA are younger in memory age by at least 15 years.
The prevalence of SA in general population is, to our knowledge, unknown. However, several studies, including the one by our team, found about 12–35% of healthy aging old- and oldest-old adults to be SA [11,12,13]. Previous research of SA focused especially on the investigation of anatomic, genetic, and histopathologic markers. SA have youthful brain regions in the major paralimbic and limbic nodes of the default mode and salience networks that support attentional, executive, and mnemonic processes subserving memory function [9, 10, 14,15,16,17,18,19]. Also, preserved greater neural differentiation and reinstatement helps SA with superior memory performance [17]. However, non-memory cognitive performance and other associated phenomena of SA has not been of much focus [10, 15, 16, 19]. Despite it, there is a study [16] suggesting, that SA in comparison to their peers have better performance in other cognitive domains a few years earlier, such as working memory or processing speed. They pointed out that despite the better performance in these domains, it declines in the same rate as in normal older adults (i.e. the cognitive maintenance does not differ). Thus, it seems that SA are somehow protected from the decline of episodic memory, but not from the decline in other cognitive domains.
Processing speed is one of the cognitive functions that declines with the age and it describes how fast a person executes mental operations in order to complete a task [20]. It is considered as one of the strongest predictors of performance in different cognitive tasks in older adults [20,21,22]. Its decline begins from midlife and linearly continues with increasing age [23,24,25,26]. Significant slowing in processing speed is associated with the overall cognitive decline and subsequently with the need for help with the activities of daily living [22, 27, 28], clinical disorders of cognition, mobility and mood [29], or even with mortality [30, 31]. On the other hand, there are factors related to a robust and stable processing speed in older age, such as greater self-reported physical activity [23], that has also been reported in SA [32]. Or despite the same amount of physical activities, it seems that SA perceive it as less demanding compared to nonSA [33].
As described above, SA are identified based on their superior memory performance and age appropriate non-memory cognitive performance (naming ability and executive functions) at a certain point beyond the age of 80. Previous studies on aging showed that faster processing speed is associated with better performance in other cognitive domains (i.e. memory). These studies used data from one time point using different samples (cross-sectional [19]) or longitudinal data for the evaluation of trajectory [16, 34, 35]. In contrast, we decided to use longitudinal approach not to analyse the trajectory but in order to seek the best predicting model of SA. Data from a time point (year 2012) were used to predict SA status determined at a later time point (year 2018). Therefore, the former time point (year 2012) rendered the baseline performance and predictors, and the performance at the latter time point (year 2018) was the dependent variable for determining of SA. We hypothesized that processing speed is the best predictor of SA status in comparison to other cognitive domains such as executive functions and short-term memory. To our knowledge this is the first study that aims to find the best predictor of future status of SA.
Method
Study design and sample
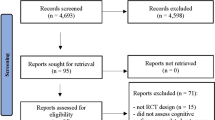
The current study uses the data from the project Cognitive SuperAging (CoSA) realized in 2018–2020, and from the first wave of the National Normative Study of Cognitive Determinants of Healthy Aging (NANOK), which was its predecessor, realized in 2012–2015 [36], and approved by the Ethics Committee of the Prague Psychiatric Centre under the reference number 64/11. Only participants of the NANOK were invited to the CoSA. The inclusion criteria for the NANOK were an age of ≥ 60 years, Czech as first language, willingness to participate in the 4-years study, and a medical history free of cognitively critical issues (such as a diagnosis/treatment for a serious neurological disorder, stroke, traumatic brain injury, acute phase of a serious mental disorder, hospitalization for a substance abuse, or chemotherapeutic treatment). There were 568 persons enrolled in wave 1 (the year 2012), aged 60–98 years, who met the inclusion criteria. The assessment and recruitment (through advertising in the local media, doctor's waiting rooms, post offices, senior institutions, or on the web), took place in 12 regions of the Czech Republic to increase representativeness, with the help of 25 trained psychometrists. Then, in the CoSA (the year 2018), there were 113 persons enrolled from the NANOK who met the inclusion criteria (age ≥ 80) and provided their informed consent. For this study, five participants were excluded due to Mini-Mental State Examination (MMSE) < 23 suggestive of an imminent cognitive disorder; four persons were excluded due to the age limit—the persons declared to be 80 during recruitment when actually they were not yet 80 at the assessment date; one participant was excluded because of their inability to finish the protocol; seven participants were excluded because they did not finish Trail Making Test (part B), a test included in the definition of SA. Therefore, the final dataset for analysis included 96 participants aged from 80 to 101 years (mean age 86.32, SD = 5.06), 40.6% were male, and the sample had an average of 13.58 years (SD = 3.92) of education. Demographic data are in Table 1.
Protocol approval and consents
The study was approved by the Ethics Committee of the National Institute of Mental Health, Klecany, Czech Republic (reference number 115/17) and all participants signed an informed consent form.
Transparency and openness
We describe all manipulations and measures that were collected. Data that met our a priori exclusion criteria (described above) were excluded. Analyses were performed using IBM SPSS 23 and JASP 0.14.1. Deidentified data are available at the project’s Open Science Framework page at osf.io/wbcer/. This study’s design and its analysis were not pre-registered.
Procedure and instruments
The assessment protocol consisted of a battery of neuropsychological tests [30]. For this study, we analysed measures used in both the CoSA and NANOK. Performance in the baseline (cognitive measures without those used in SA definition) was used as the predictor of the SA status, and measures in the follow-up were used for the identification of SA, and description of the present state.
Baseline performance (2012): predictors of SA
-
Short-term memory (Composite score-memory (CS-memory)): the Wechsler Memory Scale-Revised subtest of Logical Memory IA (immediate recall) [37, 38], and the Digit Span Forward (number of correctly recalled sequences) [39].
-
Processing speed (CS-speed): the Digit Symbol Substitution Test (number of correctly drawn symbols in 120 s [39]) and the Prague Stroop Test (PST) subtest Dots (completion time in s [40]).
-
Executive functions (CS-executive): the Prague Stroop Test subtest Colors (completion time in s [40]), and the Digit Span Backward (number of correctly recalled reversed sequences [39]).
Follow-up measures (2018): general and SA status
-
General screening: the Mini-Mental State Examination (MMSE; [41, 42]).
-
Identification of SA: We identified SA in year 2018 according to the following procedure. The mean delayed recall score of the Philadelphia Verbal Learning Test (PVLT-DR) was 9 words for the age group 60–64 years [43]. The score of 9 words is equal to the score used in the previous SuperAging studies, where it represented the average normative value of the delayed verbal recall score of the Rey Auditory Verbal Learning Test (another word list test) for individuals in their 60 s [10, 14, 16, 19]. Furthermore, additional criteria for SA in accord with the previous SuperAging studies were applied: that is, performance on non-memory tasks such as the Boston Naming Test (30-item) (BNT-30; [44, 45]), the Trail Making Test—part B (TMT-B; [46, 47]), and Category (Animals) Fluency (CF-Animals; [48]) to be equal or better than minus one standard deviation for their age band [9, 10, 14, 15, 19, 45]. The performance in the SA criterion tasks is in Table 1.
Statistical analysis
We created 3 composite scores (CS) of the immediate memory, processing speed, and executive functions by standardizing performance on each task, and averaging the z-scores. Z-scores for specific test were calculated using the mean and standard deviation (taking into account age, sex, and education) computed from normative data of older adults [36]. We chose to use this larger group as the z-score reference cohort instead of the study cohort for increased accuracy of the mean and variance estimates [16]. Additionally, interference score of the PST was calculated using ratio of two subtests: Colors/Dots. Two ratio interference scores were calculated, first using raw scores, and second using standardized scores.
The group comparison of cognitive performance and demographic variables in 2012 was performed using independent sample t-tests. In addition to effect sizes, we also report Bayes factors (BF10) calculated in accordance with recommendations by Wetzels and Wagenmakers [49]. We report probability of our data fitting under the null vs. the alternative hypothesis. Note that values larger than one are in favour of the alternative hypothesis and the values smaller than one are in favour of the null [49].
Series of binomial logistic regression analyses (method: Enter) were performed to find predictors of the SA status in 2018 based on the baseline neuropsychological data (year 2012). Age, number of years of education, sex, and composite scores (each CS separately) were used as predictors in the regression model (method Enter); SA status in 2018 was the dependent variable.
Then, all significant CS predictors (p < 0.05) plus age, number of years of education, and sex were inserted in the binomial logistic regression (method: Stepwise) to identify the best model for predicting SA.
Moreover, analysis of associations between significant predictor (2012) and PVLT delayed recall in 2018 (Pearson’s correlation) and status of SA in 2018 (Rank Biserial correlation) were performed.
The level of significance was for all analyses set at 0.05.
Results
Factors associated with SuperAging (2018)
We identified 19 SA (18%) out of 96 persons. SA did not significantly differ in the number of years of education nor in the age (all p > 0.05; Table 1) from nonSA. We did not find a significant association between sex and status of SA (p > 0.05), 15 females and 4 males were in the SA group. Groups significantly differed in the MMSE (Χ2 = 3.76; p = 0.005), the mean score of SA was ca. 2 points higher than the mean of nonSA (Table 1).
Baseline performance (2012)
SA compared to nonSA, as identified in the follow-up (year 2018), had significantly better performance at the baseline (year 2012) only in the CS-speed (p = 0.012) with medium effect size and substantial evidence in favour of the effect (BF10 = 4.06) (Table 2). Groups did not significantly differ in CS-memory nor in CS-executive (p > 0.05; Table 2) with substantial evidence in favour of null hypothesis (i.e. no difference between the groups; BF10 = 0.26). Despite non-significant difference between the groups in CS-executive, there was a medium effect size and anecdotal evidence in favour of the effect (BF10 = 1.17).
Moreover, groups did not significantly differ in PST interference scores (raw score: t(94) = 0.898, p = 0.371, d = 0.23, BF10 = 0.37; standardized score: t(94) = − 0.393, p = 0.696, d = − 0.10, BF10 = 0.28) and there was anecdotal respectively substantial evidence in favour of the null hypothesis (i.e. no difference).
Predictors of SuperAging
Logistic regression analysis was performed to identify significant predictors of SA. Firstly, we performed a series of separate logistic regression analyses (method: Enter), that were controlled for sex, age, and years of education. Based on these analyses, two measures were identified as significant predictors: CS-speed (p = 0.006) and CS-executive (p = 0.028). CS-memory was not identified as significant predictor (p > 0.05). Age was significant predictor when combined with all three CSs (CS-speed, CS-memory, and CS-executive), and in case of sex only in combination with CS-speed. There was no significant effect of the number of years of education. All results are presented in Table 3.
Then, we performed logistic regression analysis (method: Stepwise) to identify the best model for predicting SA. All significant measures from the previous analysis (CS-speed, CS-executive; see Table 3), number of years of education, sex, and age were entered in the stepwise logistic regression analysis. Compared to other significant models, model no. 3 (Table 4), which included the following measures: CS-speed (p = 0.006), sex (p = 0.015), and age (p = 0.045) was the best prediction model of SA (BIC = 96, AIC = 86, p = 0.028). Table 4 shows only the models that reached statistical significance. CS-executive did not reach it, therefore it is not included.
The results showed that CS-speed (OR = 3.74, 95% CI 1.47, 9.52) was an important predictor of the future status of SA, along with sex (OR = 5.39, 95% CI 1.40, 20.82), and age (OR = 0.87, 95% CI 0.75, 1.00). Moreover, CS-speed was not significantly associated with PVLT delayed recall in year 2012 (r = − 0.04, p = 0.728) nor in year 2018 (r = 0.10, p = 0.338). However, significant association between CS-speed and SA status (rb = 0.26, p = 0.012) was revealed, which is in line with results of Binomial logistic regression analysis.
In closer look, each second faster in PST-D (while maintaining other variables on the same level) meant a 0.6 times (OR = 0.60, 95% CI 0.41, 0.89) higher chance of being SA. As for DSST-120, the chance of SA status increased by 1.13 times (OR = 1.13, 95% CI 1.03, 1.24) with every point. Also, women had higher chance of being SA compared to men. As well, with younger age increased the chance of being SA.
Discussion
The current study aimed to identify the role of processing speed in the predicting of the status of SuperAger (SA). For this purpose, the longitudinal approach was chosen. Predictors were identified from the baseline data (2012) and data from the follow-up (2018) were used as the dependent variable to determine the status of SA. We found that processing speed measures (CS-speed) in combination with sex and age, predicted SA status.
The definition postulates that SA are superior in episodic memory compared to their peers [9, 10, 16], namely in delayed recall of a word list test such as Rey Auditory Verbal Learning Test (RAVLT) or PVLT. Despite it, SA did not significantly differ in other short-term memory measure (CS-memory) from nonSA. These results are not in accord with previous studies suggesting that SA had a better baseline episodic memory performance (measured with composite score) compared to their peers [16, 34]. The reason of this discrepancy could be that our CS-memory was composed from Logical memory test—Immediate Recall and Digit span (forward), which both test only immediate recall of the material without refreshing opportunities, or short-term memory, and do not support developing of a learning strategy unlike the word list tests or Logical Memory Delayed Recall that were used by Dang et al. [34] or Harrison et al. [16].
Our study revealed that SA significantly differed at baseline from nonSA in the non-memory measure: CS-speed, and the difference in CS-executive was with medium effect size but it did not reach significance. After controlling for age, sex, and education, CS-speed and CS-executive turned out to be predictors of future SA status (see Table 3). This is in accordance with previous studies [16, 35], but not with Dang et al. [34], who reported a better baseline performance of SA in executive functions but not in processing speed measures. Based on previous research, these two cognitive abilities (processing speed and executive functions) to some extent overlap, and tests measuring processing speed usually involve executive processes (e.g. DSST involves inhibition, shifting, and updating) [50]. In our case, we found that processing speed (CS-speed) is a best predictor of the future status of SA (see Table 4). Although, CS-executive seemed to also predict the future status of SA, but in the further regression analysis was not predictor strong enough in comparison with CS-speed. Also, both CSs (CS-speed and CS-executive) are significantly strongly associated (r = 0.60; p < 0.001), so possibly these measures may share mutual variance [50, 51]. Additionally, PST ratio interference scores were calculated (both using raw scores or standardized scores). There was non-significant difference between SA and nonSA in these measures. So, based on our results, it seems that processing speed and less executively demanding measures (DSST and PST-D) are stronger in predicting future SA status, as suggested also by Baudouin et al. [51].
Faster processing of information may have facilitated overall performance of SA, as it is suggested in our study. Processing speed is important for our everyday activities because it supports performance in other cognitive domains [20, 21]. Its slowing is associated with a decline in cognition, mobility, and mood [29, 52]. On the other hand, in our case, we see that a faster processing speed predicts future SA status, but not superior memory performance. This was supported also by additional analysis revealing significant association between CS-speed and SA status, but not between CS-speed and PVLT delayed recall (2018). Based on our data, 36 persons originally fulfilled the delayed memory criteria, however all criteria for the status of SA were fulfilled by 19 persons out of those 36. Therefore, it seems that the SA is not just about youthful memory processes, but retaining normal non-memory performance seems to play an important role either.
Our results did not show an important role of the number of years of education in the prediction of SA, but sex or age, along with processing speed measures (CS-speed), seem to be important in the prediction of SA. As suggested in other SA studies [10, 16, 18, 53], females have higher chance of being SA. Our results support this finding. It may be due to the greater cortical thickness in females compared to males [54]. Also, persons with greater cortical thickness are better able to compensate for cortical thinning [55]. According to our results, younger age was also predictor of SA [56]. It seems that with increasing age the chance of being SA decreases.
Limitations
The present study has several limitations that need to be acknowledged. We used the PVLT memory test instead of the RAVLT, which was used in the studies performed at the Northwestern Mesulam Center for Cognitive Neurology and Alzheimer’s Disease. Both RAVLT and PVLT are word list tests. The PVLT test is shorter (a 12-word list) than the RAVLT (a 15-word list), and ranks among the categorical word-list tests, such as the CVLT—California Verbal Learning Test [57], which it was modelled after. We found no direct comparisons of RAVLT and PVLT in healthy adults. Nevertheless, CVLT, a test similar to PVLT, was used instead of RAVLT in other SuperAging studies [16, 19] with similar results as in those studies where RAVLT was used [14]. The PVLT is a validated episodic memory test [58] with normative data for older Czech adults [43]. We used a PVLT normative equivalent (with the mean in the age group 60–64 years) that was, coincidentally, the same as for RAVLT in the original studies [9, 10]. The other tests used were the same as in the previous SuperAging studies. Also, our study included quite a small sample because this study was a follow-up to the NANOK, which was not originally designed for this purpose. Despite the fact that there are studies with a larger sample size [34], which is rather an exception in the field of SA studies, our sample size is comparable or even larger compared to most SuperAging studies [14,15,16, 19]. However, future studies with a larger sample size would be beneficial and could reveal more factors associated with SA status (such as lifestyle characteristics). According to previous study [12], the prevalence of SA is about 10%, therefore future studies should reflect it while planning the sample size.
Conclusions
The concept of memory SuperAging is a relatively new one. Nevertheless, it has been confirmed by independent research centres. The SA is an ideal status and we tried to understand the role of processing speed in predicting status of SA. The main finding of our study is that SA may be predicted based on their faster processing speed. Thus, it gives support and relevance to the speed of processing concept in aging and show the importance of its monitoring in the older age. Therefore, it seems that monitoring speed of processing may bring us an information not only about decline in cognitive performance, but also it may reflect a future SA status in old-old adults. In future studies, it would be interesting to find modifiable factors for cognitive SuperAging.
Availability of data and materials
The dataset supporting the conclusions of this article is available in the Open Science Framework page, https://osf.io/wbcer/.
References
Diem SJ, Lui LY, Langsetmo L, Taylor B, Cawthon PM, Cauley JA, et al. Effects of mobility and cognition on maintenance of independence and survival among women in late life. J Gerontol Ser A. 2018;73(9):1251–7.
Guralnik JM, Alecxih L, Branch LG, Wiener JM. Medical and long-term care costs when older persons become more dependent. Am J Public Health. 2002;92(8):1244–5.
Lowry KA, Vallejo AN, Studenski SA. Successful aging as a continuum of functional independence: lessons from physical disability models of aging. Aging Dis. 2012;3(1):5–15.
Nyberg L, Boraxbekk CJ, Sörman DE, Hansson P, Herlitz A, Kauppi K, et al. Biological and environmental predictors of heterogeneity in neurocognitive ageing. Ageing Res Rev. 2020;64:101184.
Fjell AM, Westlye LT, Grydeland H, Amlien I, Espeseth T, Reinvang I, et al. Critical ages in the life course of the adult brain: nonlinear subcortical aging. Neurobiol Aging. 2013;34(10):2239–47.
Nyberg L, Lövdén M, Riklund K, Lindenberger U, Bäckman L. Memory aging and brain maintenance. Trends Cogn Sci. 2012;16(5):292–305.
Rogalski EJ. Don’t forget: age is a relevant variable in defining SuperAgers. Alzheimers Dement Diagn Assess Dis Monit. 2019;11(1):560–1.
Verhaeghen P, Salthouse TA. Meta-analyses of age–cognition relations in adulthood: estimates of linear and nonlinear age effects and structural models. Psychol Bull. 1997;122(3):231–49.
Harrison TM, Weintraub S, Mesulam MM, Rogalski EJ. Superior memory and higher cortical volumes in unusually successful cognitive aging. J Int Neuropsychol Soc. 2012;18(06):1081–5.
Rogalski EJ, Gefen T, Shi J, Samimi M, Bigio E, Weintraub S, et al. Youthful memory capacity in old brains: anatomic and genetic clues from the Northwestern SuperAging Project. J Cogn Neurosci. 2013;25(1):29–36.
Calandri IL, Crivelli L, Martin ME, Egido N, Guimet NM, Allegri RF. Environmental factors between normal and superagers in an Argentine cohort. Dement Neuropsychol. 2020;14(4):345–9.
Červenková M, Heissler R, Kopeček M. Stability of memory SuperAgers over 3 years. PsyCh J. 2020;9(1):147–9.
Saint Martin M, Sforza E, Barthélémy JC, Roche F, Lefèvre P, Liénard G, et al. Long-lasting active lifestyle and successful cognitive aging in a healthy elderly population: the PROOF cohort. Rev Neurol. 2017;173(10):637–44.
Cook AH, Sridhar J, Ohm D, Rademaker A, Mesulam MM, Weintraub S, et al. Rates of cortical atrophy in adults 80 years and older with superior vs average episodic memory. JAMA. 2017;317(13):1373.
Gefen T, Peterson M, Papastefan ST, Martersteck A, Whitney K, Rademaker A, et al. Morphometric and histologic substrates of cingulate integrity in elders with exceptional memory capacity. J Neurosci. 2015;35(4):1781–91.
Harrison TM, Maass A, Baker SL, Jagust WJ. Brain morphology, cognition, and β-amyloid in older adults with superior memory performance. Neurobiol Aging. 2018;67:162–70.
Katsumi Y, Andreano JM, Barrett LF, Dickerson BC, Touroutoglou A. Greater neural differentiation in the ventral visual cortex is associated with youthful memory in superaging. Cereb Cortex. 2021;31(11):5275–87.
Katsumi Y, Wong B, Cavallari M, Fong TG, Alsop DC, Andreano JM, et al. Structural integrity of the anterior mid-cingulate cortex contributes to resilience to delirium in superaging. Brain Commun. 2022;4(4):fcac163.
Sun FW, Stepanovic MR, Andreano J, Barrett LF, Touroutoglou A, Dickerson BC. youthful brains in older adults: preserved neuroanatomy in the default mode and salience networks contributes to youthful memory in superaging. J Neurosci. 2016;36(37):9659–68.
Salthouse TA. Aging and measures of processing speed. Biol Psychol. 2000;54(1–3):35–54.
Rast P. Verbal knowledge, working memory, and processing speed as predictors of verbal learning in older adults. Dev Psychol. 2011;47(5):1490–8.
Salthouse TA, Ferrer-Caja E. What needs to be explained to account for age-related effects on multiple cognitive variables? Psychol Aging. 2003;18(1):91–110.
Bott NT, Bettcher BM, Yokoyama JS, Frazier DT, Wynn M, Karydas A, et al. Youthful Processing speed in older adults: genetic, biological, and behavioral predictors of cognitive processing speed trajectories in aging. Front Aging Neurosci. 2017. https://doi.org/10.3389/fnagi.2017.00055/full.
Salthouse TA. When does age-related cognitive decline begin? Neurobiol Aging. 2009;30(4):507–14.
Salthouse TA. Trajectories of normal cognitive aging. Psychol Aging. 2019;34(1):17–24.
Tucker-Drob EM, Johnson KE, Jones RN. The cognitive reserve hypothesis: a longitudinal examination of age-associated declines in reasoning and processing speed. Dev Psychol. 2009;45(2):431–46.
Bezdicek O, Stepankova H, Martinec Novakova L, Kopecek M. Toward the processing speed theory of activities of daily living in healthy aging: normative data of the functional activities questionnaire. Aging Clin Exp Res. 2016;28(2):239–47.
Finkel D, Reynolds CA, McArdle JJ, Pedersen NL. Age changes in processing speed as a leading indicator of cognitive aging. Psychol Aging. 2007;22(3):558–68.
Rosano C, Perera S, Inzitari M, Newman AB, Longstreth WT, Studenski S. Digit symbol substitution test and future clinical and subclinical disorders of cognition, mobility and mood in older adults. Age Ageing. 2016;45(5):687–94.
Smits CHM, Deeg DJH, Kriegsman DMW, Schmand B. Cognitive functioning and health as determinants of mortality in an older population. Am J Epidemiol. 1999;150(9):978–86.
Swindell WR, Cummings SR, Sanders JL, Caserotti P, Rosano C, Satterfield S, et al. Data mining identifies digit symbol substitution test score and serum cystatin C as dominant predictors of mortality in older men and women. Rejuvenation Res. 2012;15(4):405–13.
Kim BR, Kwon H, Chun MY, Park KD, Lim SM, Jeong JH, et al. White matter integrity is associated with the amount of physical activity in older adults with super-aging. Front Aging Neurosci. 2020;12:549983.
Heissler R, Georgi H, Kopeček M. Leisure activities of SuperAgers. In: Ageing 2021: Proceedings of the 5th Gerontological Interdisciplinary Conference [Internet]. Prague College of Psychosocial Studies; 2021. p. 77–86. Available from: http://www.konferencestarnuti.cz/files/Starnuti_2021_sbornik.pdf.
Dang C, Harrington KD, Lim YY, Ames D, Hassenstab J, Laws SM, et al. Superior memory reduces 8-year risk of mild cognitive impairment and dementia but not amyloid β-associated cognitive decline in older adults. Arch Clin Neuropsychol. 2019;34(5):585–98.
Dekhtyar M, Papp KV, Buckley R, Jacobs HIL, Schultz AP, Johnson KA, et al. Neuroimaging markers associated with maintenance of optimal memory performance in late-life. Neuropsychologia. 2017;100:164–70.
Štěpánková H, Bezdíček O, Nikolai T, Horáková K, Lukavský J, Kopeček M. Zpráva o projektu Národní normativní studie kognitivních determinant zdravého stárnutí. E-Psychol. 2015;9(1):43–64.
Jenčová A, Černochová D. WMS–IIIa:Wechslerova zkrácená paměťová škála. Vol. 1. Praha: Hogrefe—Testcentrum; 2011.
Wechsler D. Wechsler memory scale. 3rd ed. USA: The Psychological Corporation; 2002. p. 195.
Wechsler D. Wechsler adult intelligence scale. 3rd ed. San Antonio: The Psychological Corporation; 1997.
Bezdicek O, Lukavsky J, Stepankova H, Nikolai T, Axelrod BN, Michalec J, et al. The prague stroop test: normative standards in older Czech adults and discriminative validity for mild cognitive impairment in Parkinson’s disease. J Clin Exp Neuropsychol. 2015;37(8):794–807.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–98.
Štěpánková H, Nikolai T, Lukavský J, Bezdíček O, Vrajová M, Kopeček M. Mini-mental state examination: česká normativní studie. Čes Slov Neurol Neurochir. 2015;78/111(1):57–63.
Bezdicek O, Libon DJ, Stepankova H, Panenkova E, Lukavsky J, Garrett KD, et al. Development, validity, and normative data study for the 12-word Philadelphia verbal learning test [czP(r)VLT-12] among older and very old Czech adults. Clin Neuropsychol. 2014;28(7):1162–81.
Kaplan E, Goodglass H, Weintraub S. The Boston naming test. 2nd ed. Lea & Febiger; 1983.
Nikolai T, Stepankova H, Kopecek M, Sulc Z, Vyhnalek M, Bezdicek O. The uniform data set, Czech Version: normative data in older adults from an international perspective. J Alzheimers Dis. 2018;61(3):1233–40.
Bezdicek O, Stepankova H, Axelrod BN, Nikolai T, Sulc Z, Jech R, et al. Clinimetric validity of the trail making test Czech version in parkinson’s disease and normative data for older adults. Clin Neuropsychol. 2017;31(S1):42–60.
Reitan RM. Validity of the trail making test as an indicator of organic brain damage. Percept Mot Skills. 1958;8(3):271–6.
Nikolai T, Štěpánková H, Michalec J, Bezdíček O, Horáková K, Marková H, et al. Tests of verbal fluency, czech normative study in older patients. Čes Slov Neurol Neurochir. 2015;78/111(3):292–9.
Wetzels R, Wagenmakers EJ. A default Bayesian hypothesis test for correlations and partial correlations. Psychon Bull Rev. 2012;19(6):1057–64.
Albinet CT, Boucard G, Bouquet CA, Audiffren M. Processing speed and executive functions in cognitive aging: how to disentangle their mutual relationship? Brain Cogn. 2012;79(1):1–11.
Baudouin A, Clarys D, Vanneste S, Isingrini M. Executive functioning and processing speed in age-related differences in memory: contribution of a coding task. Brain Cogn. 2009;71(3):240–5.
Jaeger J. Digit symbol substitution test: the case for sensitivity over specificity in neuropsychological testing. J Clin Psychopharmacol. 2018;38(5):513–9.
Maccora J, Peters R, Anstey KJ. Gender differences in superior-memory superagers and associated factors in an Australian cohort. J Appl Gerontol. 2021;40(4):433–42.
Ritchie SJ, Cox SR, Shen X, Lombardo MV, Reus LM, Alloza C, et al. Sex differences in the adult human brain: evidence from 5216 UK biobank participants. Cereb Cortex. 2018;28(8):2959–75.
Subotic A, McCreary CR, Saad F, Nguyen A, Alvarez-Veronesi A, Zwiers AM, et al. Cortical thickness and its association with clinical cognitive and neuroimaging markers in cerebral amyloid angiopathy. J Alzheimers Dis. 2021;81(4):1663–71.
Pettigrew C, Soldan A. Defining cognitive reserve and implications for cognitive aging. Curr Neurol Neurosci Rep. 2019;19(1):1.
Delis DC, Kramer JH, Kaplan E, Ober BA. CVLT, California verbal learning test: adult version: manual. San Antonio: Psychological Corporation; 1987.
Libon DJ, Mattson RE, Glosser G, Kaplan E, Malamut BL, Sands LP, et al. A nine—word dementia version of the California verbal learning test. Clin Neuropsychol. 1996;10(3):237–44.
Acknowledgements
We thank Tamara Anne Wheeler for the language editing.
Funding
We gratefully acknowledge funding from the Czech Science Foundation to the National Institute of Mental Health (under Grant Number GA 18-06199S; Cognitive SuperAging) and to Prague College of Psychosocial Studies (under Grant Number GA 22-24846S; Cognitive SuperAging in physically active women).
Author information
Authors and Affiliations
Contributions
Obtaining funding: MK, HG. Study design: ZT, HG, BS. Data collection: HG, RH. Data analysis: ZT, BS. Data interpretation: ZT, HG, BS, MK. Drafting manuscript: ZT. Critical revision of manuscript: all authors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the National Institute of Mental Health, Klecany, Czech Republic (Reference Number 115/17) and all participants signed an informed consent form. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ticha, Z., Georgi, H., Schmand, B. et al. Processing speed predicts SuperAging years later. BMC Psychol 11, 34 (2023). https://doi.org/10.1186/s40359-023-01069-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-023-01069-7