
Abstract
Introduction
Computer tomography (CT) based navigation is considered by some authors as an advance in total hip arthroplasty (THA). A meta-analysis was conducted to compare CT based versus conventional THA in terms of surgical duration of the procedure, leg length difference, acetabular cup position, and rate of dislocation.
Material and methods
The present study was conducted according to the PRISMA 2020. In December 2022, the following databases were accessed: PubMed, Web of Science, Google Scholar, Embase with no time constrain. All the clinical studies comparing CT based navigation versus the conventional THA were accessed.
Results
Data from 1801 procedures were collected. The mean age of the patients was 61.6 ± 5.3 years, and the mean BMI was 26.9 ± 2.3 kg/m2. There was between studies comparability at baseline in terms of age, BMI, pain score, Harris hip score, leg length discrepancy (P > 0.1). The navigated group demonstrated lower leg length discrepancy (P = 0.02), and lower degrees of cup anteversion (P = 0.002). Similarity was found in cup inclination (P = 0.98), surgical duration (P = 0.3), and the rate of dislocation (P = 0.6).
Conclusion
CT guided THA may have the potential to increase the accuracy of acetabular positioning and reduce the leg length discrepancy. Current evidence is very limited and heterogeneous, and no recommendations can be inferred. Further investigations are required to definitely clarify the role of CT based THA in current practice.
Similar content being viewed by others


Introduction
Total hip arthroplasty (THA) restores joint function and patient quality of life [1, 2]. Proper implant positioning is necessary to achieve long term THA survivorship. Dislocation, impingement, pelvic osteolysis, acetabular migration, and inlay erosion are common following acetabular components malposition [3, 4]. A 45° ± 10° of cup inclination and a 15° ± 10° of cup anteversion are recommended [5,6,7]. In patients with leg length discrepancy, back pain, gait impairment, greater rate of aseptic loosening, and dissatisfaction are common [8,9,10,11].
Computer tomography (CT) based THA uses algorithms and tracking systems to detect anatomical features, limb axes, and joint orientation to assist surgeons [12, 13]. Several studies compared CT based THA versus the conventional freehand procedure [13,14,15,16,17,18]. Comparative studies were however not conclusive, and the application of CT based THA is still controversial [19,20,21,22,23]. Recently published evidence which has not yet been included in a systematic review evidenced that the CT based THA is a valuable option to perform total hip arthroplasty, presenting some advantages over the classical freehand technique [24]. A meta-analysis was conducted to compare surgical duration, leg length discrepancy, cup anteversion and inclination, and rate of dislocation between these two different modalities.
Material and methods
Eligibility criteria
All the clinical investigation comparing CT based navigation versus the conventional freehand THA were accessed. Level I to III of evidence, according to Oxford Centre of Evidence-Based Medicine [25], were eligible. Animals, in vitro, biomechanics, computational, and cadaveric studies were not eligible. Given the authors language capabilities, articles in English, German, Italian, French and Spanish were eligible. Reviews, opinions, letters, editorials were not considered. Only studies published in peer reviewed journals were considered. Studies which used innovative implants, materials, or experimental rehabilitation programs were not considered. Only studies which report the outcomes of CT based navigation and quantitative data under the outcomes of interest were suitable. Other types of navigation methods (e.g. imageless) were not eligible.
Search strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement [26]. The PICO algorithm was stated:
-
P (Population): end stage hip osteoarthritis;
-
I (Intervention): CT-based navigation THA;
-
C (Comparison): conventional freehand THA;
-
O (Outcomes): radiological parameters, surgical duration, dislocations.
In December 2022, the following databases were accessed: PubMed, Web of Science, Google Scholar, Embase with no time constrains. The keywords used for the search were: hip, total hip arthroplasty, replacement, prosthesis, osteoarthritis, anteversion, inclination, lower limb, leg discrepancy, radiological, complications, dislocation.
Selection and data collection
The literature search was conducted by two authors (**;**) independently. Titles and abstract of interest were screened and the full-text of the articles of interest were accessed. If the full-text was not accessible, the article was excluded from the present investigation. The bibliography of the full-text articles were also screened for inclusion. Disagreements were debated, and the final decision was taken by a third author (**).
Data items
Two authors (**;**) independently performed data extraction. The following data were extracted: author and year, journal, study design, number of procedures, sex of the patients, mean age at operation, type of intervention and surgical approach, type of navigation system. The following data were retrieved at last follow-up: mean cup inclination and anteversion, surgical duration, leg length discrepancy, rate of dislocations.
Methodological quality assessment
The methodological quality assessment was performed using the Review Manager software version 5.3 (The Nordic Cochrane Collaboration, Copenhagen). Two authors (**;**) evaluated the risk of bias of each included study using the Cochrane risk of bias tool. The following biases were evaluated: selection, detection, attrition, reporting, other source of biases. Disagreements were debated, and the final decision was taken by a third author (**). To assess the overall risk of publication bias, the funnel plot was evaluated. Asymmetries of the plot indicate higher risk of bias.
Synthesis methods
The statistical analyses were performed by the main author (**). For descriptive statistics, the IBM SPSS version 25 was used. The Shapiro–Wilk test has been performed to investigate data distribution. For parametric data, mean and standard deviation were evaluated. For non-parametric data, median and interquartile were evaluated. Mean difference (MD) effect measure was adopted to assess baseline comparability. Student T-test and Mann–Whitney U-test were performed for parametric and non-parametric data, with P values > 0.1 considered satisfactory. For the meta-analyses, the Review Manager 5.3 software (The Nordic Cochrane Collaboration, Copenhagen) was used. For continuous data, the inverse variance with MD effect measure was adopted, while the Mantel–Haenszel method with odd ratio (OR) effect measure was used for dichotomic data. Heterogeneity was investigated using the Higgins I2 and \(\chi\) 2 tests. If \(\chi\) 2 < 0.05 and I2 > 75%, high heterogeneity was found. A fixed method effect model was used as default; if high heterogeneity was found, a random effect model was used. The confidence interval (CI) was set at 95% in all comparisons. Overall P values of < 0.05 were considered statistically significant.
Results
Study selection
The literature search identified 2226 articles related to navigated arthroplasty. Of them, 501 were duplicates. Further 1702 articles were excluded: did not focused on CT based (N = 1395), not focused on hip (N = 177), study type (N = 103), other (27). Further 23 studies were excluded as did not report quantitative data under the outcomes of interest. This left 9 articles for inclusion: 3 randomized clinical trials (RCTs), 2 prospective, and 4 retrospective clinical studies (Fig. 1).

Flow chart of the literature search
Methodological quality assessment
Given the high ratio of non randomised studies (6 of 9 studies), the risk of selection bias was moderate to high. Moreover, 67% (4 of 6) of the included studies had a retrospective design, which further increase the risk of selection bias by allocation concealment. Given the lack of blinding in most studies, the risk of detection bias was moderate-high. Attrition bias and reporting biases were both moderate-low, and the risk of other biases was moderate. Concluding, the methodological assessment demonstrated a moderate risk of bias (Fig. 2).

Methodological quality assessment
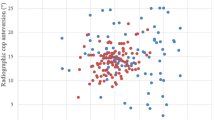
Risk of publication bias
The funnel plot of the most reported outcome (cup anteversion) has been performed to evaluate the risk of publication bias. The plot demonstrated high symmetry, indicating a very low risk of publication bias (Fig. 3).

Funnel plot
Study characteristics and results of individual studies
Data from 1801 procedures were collected, 58% in women. The mean age was 61.6 ± 5.3 years. The mean BMI was 26.9 ± 2.3 kg/m2.There was between group comparability at baseline in terms of age, BMI, VAS, Harris hip score, leg length discrepancy (P > 0.1). Generalities and patient baseline characteristics of the included studies is shown in greater detail in Table 1.
Results of syntheses
Two studies investigated surgical duration [17, 27]. The overall effect resulted statistically not significant (P = 0.3), evidencing similarity between the groups (Fig. 4).

Meta-analysis of the comparison: surgical duration
Two studies investigated leg length discrepancy [18, 27]. The navigated group demonstrated lower leg length discrepancy (MD -2.60; 95% CI − 4.75 to − 0.75; P = 0.02; Fig. 5).

Meta-analysis of the comparison: leg length discrepancy
Four studies compared cup anteversion [18, 24, 29, 31]. The navigated group demonstrated lower degrees of cup anteversion (MD − 5.62; 95% CI − 9.20 to − 1.05; P = 0.002; Fig. 6).

Meta-analysis of the comparison: cup anteversion
Four studies compared cup inclination [18, 24, 29, 31]. The overall effect resulted statistically not significant (P = 0.98), evidencing similarity between the groups (Fig. 7).

Meta-analysis of the comparison: cup inclination
Two studies compared the rate of dislocation [17, 31]. The overall effect resulted statistically not significant (P = 0.6), evidencing similarity between the groups (Fig. 8).

Meta-analysis of the comparison: rate of dislocation
Discussion
According to the main findings of the present study, the current evidence demonstrated that CT based THA may promote more accurate cup anteversion and lower leg length discrepancy compared to the conventional procedure. No difference was found in cup inclination, duration of surgery, and rate of dislocation between the two techniques.
CT based THA navigation resulted in similar inclination compared to the conventional procedure. However, navigated THA demonstrated a more accurate cup anteversion compared to the conventional procedure. Domb et al. [18] reported that cups in navigated THA were placed in the safe zone [32] in 100% of patients, compared to 80% in the freehand THA [18]. Kalteis et al. [24] found that 14 of 30 cups were placed in the safe zone following freehand THA, and 25 of 30 of the navigated were optimally placed. On the contrary, Lin et al. [29] evidenced similar positioning between freehand and CT based THA groups: inclination was optimal in 23 of 25 freehand THA and 25 of 25 CT navigated THA; cup anteversion was optimal in 19 of 25 conventional THA and 21 of 22 CT based THA [29]. The authors reported CT navigated THA is associated to more precise placement of the acetabular component, with low rates of malposition [29]. Verdier et al. [31] found that patients who target the optimal anteversion range was reached in 28 of 39 patients in the navigated THA, and in 17/39 of patients who underwent the freehand technique [31]. CT guided demonstrated lower leg length discrepancy compared to the conventional procedure [18, 27]. Confalonieri et al. [27] evidenced no difference between the two groups in pre-operative leg length discrepancy. Postoperatively, there were 0.4 cm of discrepancy in CT guided THA group and 0.8 cm in THA freehand group [27]. No post-operative leg length discrepancy greater than 1 cm was reported in any patient of the CT guided group [27]. Domb et at. [18] found a leg length discrepancy greater than 1 cm in 3% of 708 patients who had undergone conventional THA, and none of the navigated group (N = 43) demonstrated a discrepancy greater than 1 cm. Surgical duration was similar between the two procedures. Two studies investigated the surgical duration [17, 27]. Confalonieri et al. [27], in a population of 44 patients, showed a statistically longer surgical time with a mean time of 102.6 min in the navigated group compared to 87.7 min of free hand group. Murphy et al. [17], using specific instruments for CT based THA, reported similarity between the procedures: 177 min in the navigated group compared to the 178 min in the conventional group. This study demonstrated that the rate of dislocation between the two techniques was similar. Murphy et al. [17] found no dislocation in 185 patients treated with CT based THA, and two dislocations on 189 patients were reported in the cohort of freehand THA. Verdier et al. [31] found one dislocation in the freehand group (in a female patient with excessive anteversion) and none in the navigated group [31]. The present study indicated that CT guided THA may have the potential to increase the accuracy of acetabular positioning and reduce leg length discrepancy. To better identify the advantages of CT guided THA, high quality studies involving large cohort of patients. The current evidence is very limited and heterogeneous; therefore, no strong recommendations can be inferred. Further investigations are required to clarify the role of CT based THA.
The present study has several limitations. The limited number of clinical studies and procedures included for analysis represent the most important limitations, together with, the retrospective design of most studies. Given the limited data available in the current literature, surgical approach and/or the type of implant used were not analyzed. The description of the surgical technique was adequate in most studies. The eligibility criteria were barely reported, and often biased. Given the limited data available, perioperative data (e.g. mean blood loss, transfusion units), joint function, and patients quality of life was not possible to compare. Finally, most analyses were conducted using a random effect model, as the level of between studies heterogeneity was high. Given these limitations, results from the present study must be interpreted with caution.
Conclusion
CT guided THA may have the potential to increase the accuracy of acetabular positioning and reduce the leg length discrepancy. The current evidence is very limited and heterogeneous; therefore, no strong recommendations can be inferred. Further investigations are required to definitely clarify the role of CT based THA in current practice, as it is unclear whether these reported differences, though of statistical significance translate in clinical relevance in terms of better function and/ or greater longevity of the implants used for THA.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available throughout the manuscript.
Abbreviations
- THA:
-
Total hip arthroplasty
- CT:
-
Computer tomography
- MD:
-
Mean difference
- OR:
-
Odd ratio
- CI:
-
Confidence interval
- RCTs:
-
Randomized clinical trials
References
Reininga IH, Zijlstra W, Wagenmakers R, Boerboom AL, Huijbers BP, Groothoff JW, Bulstra SK, Stevens M. Minimally invasive and computer-navigated total hip arthroplasty: a qualitative and systematic review of the literature. BMC Musculoskelet Disord. 2010;11:92. https://doi.org/10.1186/1471-2474-11-92.
Wang Z, Hou JZ, Wu CH, Zhou YJ, Gu XM, Wang HH, Feng W, Cheng YX, Sheng X, Bao HW. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res. 2018;13(1):229. https://doi.org/10.1186/s13018-018-0929-4.
Williamson, J.A. and F.W. Reckling, Limb length discrepancy and related problems following total hip joint replacement. Clin Orthop Relat Res, 1978(134): p. 135-8.
Kennedy JG, Rogers WB, Soffe KE, Sullivan RJ, Griffen DG, Sheehan LJ. Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J Arthroplasty. 1998;13(5):530–4. https://doi.org/10.1016/s0883-5403(98)90052-3.
Cassidy KA, Noticewala MS, Macaulay W, Lee JH, Geller JA. Effect of femoral offset on pain and function after total hip arthroplasty. J Arthroplasty. 2012;27(10):1863–9. https://doi.org/10.1016/j.arth.2012.05.001.
Banaszkiewicz PA. Dislocations after total hip-replacement arthroplasties. Classic Papers Orthopaed. 2014. https://doi.org/10.1007/978-1-4471-5451-8_27.
Najarian BC, Kilgore JE, Markel DC. Evaluation of component positioning in primary total hip arthroplasty using an imageless navigation device compared with traditional methods. J Arthroplasty. 2009;24(1):15–21. https://doi.org/10.1016/j.arth.2008.01.004.
Friberg, O., Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine (Phila Pa 1976), 1983. 8(6): p. 643-51.
Harrison MH. Robert Jones, Gathorne Girdlestone and excision arthroplasty of the hip. J Bone Joint Surg Br. 2005;87(9):1306. https://doi.org/10.1302/0301-620X.16753.
Tanaka R, Shigematsu M, Motooka T, Mawatari M, Hotokebuchi T. Factors influencing the improvement of gait ability after total hip arthroplasty. J Arthroplasty. 2010;25(6):982–5. https://doi.org/10.1016/j.arth.2009.06.009.
Amstutz, H.C., et al., Revision of aseptic loose total hip arthroplasties. Clin Orthop Relat Res, 1982(170): p. 21-33.
Jia J, Zhao Q, Lu P, Fan G, Chen H, Liu C, Liu J, Chen S, Jin Z. Clinical efficacy of orthopilot navigation system versus conventional manual of total hip arthroplasty: a systematic review and meta-analysis. Medicine. 2019;98(20): e15471. https://doi.org/10.1097/MD.0000000000015471.
Masumoto Y, Fukunishi S, Fukui T, Yoshiya S, Nishio S, Fujihara Y, Okahisa S, Okada T, Kanto M, Goshi A, Morio F, Takeda Y. New combined anteversion technique in hybrid THA: cup-first procedure with CT-based navigation. Eur J Orthop Surg Traumatol. 2020;30(3):465–72. https://doi.org/10.1007/s00590-019-02589-y.
Ogawa H, Kurosaka K, Sato A, Hirasawa N, Matsubara M, Tsukada S. Does an augmented reality-based portable navigation system improve the accuracy of acetabular component orientation during THA? a randomized controlled trial. Clin Orthop Relat Res. 2020;478(5):935–43. https://doi.org/10.1097/CORR.0000000000001083.
Licini DJ, Burnikel DJ, Meneghini RM, Ochsner JL. Comparison of limb-length discrepancy after THA: with and without computer navigation. Orthopedics. 2013;36(5):e543-547. https://doi.org/10.3928/01477447-20130426-13.
Haaker RG, Tiedjen K, Ottersbach A, Rubenthaler F, Stockheim M, Stiehl JB. Comparison of conventional versus computer-navigated acetabular component insertion. J Arthroplasty. 2007;22(2):151–9. https://doi.org/10.1016/j.arth.2005.10.018.
Murphy SB, Ecker TM, Tannast M. THA performed using conventional and navigated tissue-preserving techniques. Clin Orthop Relat Res. 2006;453:160–7. https://doi.org/10.1097/01.blo.0000246539.57198.29.
Domb BG, Redmond JM, Louis SS, Alden KJ, Daley RJ, LaReau JM, Petrakos AE, Gui C, Suarez-Ahedo C. Accuracy of component positioning in 1980 total hip arthroplasties: a comparative analysis by surgical technique and mode of guidance. J Arthroplasty. 2015;30(12):2208–18. https://doi.org/10.1016/j.arth.2015.06.059.
Shah SM, Deep K, Siramanakul C, Mahajan V, Picard F, Allen DJ. Computer navigation helps reduce the incidence of noise after ceramic-on-ceramic total hip arthroplasty. J Arthroplasty. 2017;32(9):2783–7. https://doi.org/10.1016/j.arth.2017.04.019.
Ellapparadja P, Mahajan V, Atiya S, Sankar B, Deep K. Leg length discrepancy in computer navigated total hip arthroplasty-how accurate are we? Hip Int. 2016;26(5):438–43. https://doi.org/10.5301/hipint.5000368.
Oh KJ, Kim BK, Jo MI, Ahn BM. Which one is more affected by navigation-assisted cup positioning in total hip arthroplasty: anteversion or inclination? A retrospective matched-pair cohort study in Asian physique. J Orthop Surg. 2018;26(2):2309499018780755. https://doi.org/10.1177/2309499018780755.
Renkawitz T, Weber M, Springorum HR, Sendtner E, Woerner M, Ulm K, Weber T, Grifka J. Impingement-free range of movement, acetabular component cover and early clinical results comparing “femur-first” navigation and “conventional” minimally invasive total hip arthroplasty: a randomised controlled trial. Bone Joint J. 2015;97-B(7):890–8. https://doi.org/10.1302/0301-620X.97B7.34729.
Parratte S, Ollivier M, Lunebourg A, Flecher X, Argenson JN. No benefit after THA performed with computer-assisted cup placement: 10-year results of a randomized controlled study. Clin Orthop Relat Res. 2016;474(10):2085–93. https://doi.org/10.1007/s11999-016-4863-7.
Kalteis T, Handel M, Bathis H, Perlick L, Tingart M, Grifka J. Imageless navigation for insertion of the acetabular component in total hip arthroplasty: is it as accurate as CT-based navigation? J Bone Joint Surg Br. 2006;88(2):163–7. https://doi.org/10.1302/0301-620X.88B2.17163.
Howick J CI, Glasziou P, Greenhalgh T, Carl Heneghan, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine https://www.cebmnet/indexaspx?o=5653
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71. https://doi.org/10.1136/bmj.n71.
Confalonieri N, Manzotti A, Montironi F, Pullen C. Leg length discrepancy, dislocation rate, and offset in total hip replacement using a short modular stem: navigation vs conventional freehand. Orthopedics. 2008;31(10 Suppl 1):35.
Leenders T, Vandevelde D, Mahieu G, Nuyts R. Reduction in variability of acetabular cup abduction using computer assisted surgery: a prospective and randomized study. Comput Aided Surg. 2002;7(2):99–106. https://doi.org/10.1002/igs.10033.
Lin F, Lim D, Wixson RL, Milos S, Hendrix RW, Makhsous M. Limitations of imageless computer-assisted navigation for total hip arthroplasty. J Arthroplasty. 2011;26(4):596–605. https://doi.org/10.1016/j.arth.2010.05.027.
Sugano N. Computer-assisted orthopaedic surgery and robotic surgery in total hip arthroplasty. Clin Orthop Surg. 2013;5(1):1–9. https://doi.org/10.4055/cios.2013.5.1.1.
Verdier N, Billaud A, Masquefa T, Pallaro J, Fabre T, Tournier C. EOS-based cup navigation: randomised controlled trial in 78 total hip arthroplasties. Orthop Traumatol Surg Res. 2016;102(4):417–21. https://doi.org/10.1016/j.otsr.2016.02.006.
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217–20.
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
FM conception and design, interpretation of the data, drafting, final approval; NM: supervision, revision, final approval; ET: supervision, final approval; FO: supervision, final approval; FH: supervision, final approval; FC: drafting, final approval. All authors have agreed to the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This study complies with ethical standards.
Consent to publications
Not applicable.
Competing interests
The authors declare that they have any competing interests for this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Migliorini, F., Cuozzo, F., Oliva, F. et al. CT-based navigation for total hip arthroplasty: a meta-analysis. Eur J Med Res 28, 443 (2023). https://doi.org/10.1186/s40001-023-01437-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01437-4