
Abstract
Background
New vertebral compression fractures (NVCFs) are common adverse events in percutaneous kyphoplasty (PKP). The present study aimed to investigate the risk factors for NVCFs in patients after PKP and to construct a nomogram for the prediction of the risk of re-fracture.
Methods
We retrospectively analyzed the medical records of patients after PKP surgery between January 2017 and December 2020. Patients were divided into an NVCF group (n = 225) and a control group (n = 94) based on the presence or absence of NVCFs, respectively, at follow-up within 2 years after surgery. Lasso regression was used to screen for risk factors for re-fracture. Based on the results, a Lasso-logistic regression model was developed, and its prediction performance was evaluated using receiver operating characteristic curves, calibration, and decision curve analysis. The model was visualized, and a nomogram was constructed.
Results
A total of eight potential predictors were obtained from Lasso screening. Advanced age, low body mass index, low bone mineral density, lack of anti-osteoporosis treatment, low preoperative vertebral body height, vertebral body height recovery ≥ 2, cement leakage, and shape D (lack of simultaneous contact of bone cement with the upper and lower plates) were included in the logistic regression model.
Conclusions
A nomogram for predicting postoperative NVCF in PKP was developed and validated. This model can be used for rational assessment of the magnitude of the risk of developing NVCFs after PKP, and can help orthopedic surgeons make clinical decisions aimed at reducing the occurrence of NVCFs.
Similar content being viewed by others


Background
Osteoporosis, the most common bone disease, is a systemic condition characterized by decreased bone mass which leads to deterioration of bone tissue microarchitecture and increased bone fragility. Approximately one-third of women experience osteoporosis-related fractures after the age of 50 compared to one-fifth of men [1]. Osteoporosis has an insidious onset and is potentially very harmful. Falls or injuries in older adults often result in osteoporotic fractures, with vertebral compression fractures (VCFs) being the most common [2]. Patients with VCFs experience severe chronic pain, kyphosis, decreased mobility, reduced pulmonary function [3], and increased mortality rates [4]. Since 1987, osteoporotic vertebral compression fractures (OVCFs) have been widely treated with percutaneous kyphoplasty (PKP), which is effective in relieving pain and restoring vertebral height with minimal trauma and rapid recovery time; therefore, PKP has become the treatment of choice for OVCFs [5, 6].
However, re-collapse of cemented vertebrae frequently occurs after percutaneous augmentation [7]. Many risk factors for re-fracture have been considered, and several relevant factors have been reviewed in the literature [7, 8]. Very few studies have developed visual models for risk factors of re-fracture after PKP, and none of these studies have included bone mineral density (BMD) in these models [9, 10]. Previous studies have suggested that BMD has major effects on OVCFs [11], with a low BMD predisposing patients to re-fracture after PKP [7]. A retrospective study of cases by Venmans et al. [12] found that the severity of osteoporosis was a risk factor for vertebral re-fracture after PKP surgery. Therefore, in the present study, we developed and validated a nomogram to predict the risk of NVCFs after PKP surgery.
Methods
Patients
A total of 466 patients with single-segment OVCFs treated with PKP at Zhejiang Provincial People’s Hospital between January 2017 and December 2020 were analyzed. The inclusion criteria were: 1. single-segment OVCFs caused by low-energy injuries (falls, bending) in older patients treated with PKP, 2. significant low back pain or restricted movement, and 3. indications on imaging examination (radiography or computed tomography showing vertebral fracture; magnetic resonance (MR) T2-weighted imaging showing significant edema of the fractured vertebrae). The exclusion criteria were: 1. OVCFs due to cancer, infection, or tuberculosis; 2. long-term glucocorticoid treatment; 3. inability to tolerate surgery; 4. spinal cord compression with significant neurological symptoms such as numbness or muscle weakness; 5. multiple segmental fractures of the spine; 6. endocrine disorders such as hyper- or hypothyroidism; and 7. loss to follow-up for other reasons or incomplete preoperative imaging data.
Based on the inclusion and exclusion criteria, 147 patients were excluded: 66 did not meet the indications for single-segment vertebral fractures, 45 lacked complete preoperative imaging data (imaging data from outside institutions), 22 had malignant cancer, one received glucocorticoid treatment, and 12 were lost to follow-up. A total of 319 patients were enrolled in the study, including 225 patients in the training cohort and 94 patients in the validation cohort.
Observation indicators
We reviewed previously published literature on the risk factors that may contribute to VCF after PKP, as well as the general characteristics and imaging parameters of patients. Age, sex, history of diabetes and hypertension, body mass index (BMI), BMD, vertebral segments fractured, mean volume of cement used, volume of cement leakage, volume of cement dispersion, distribution of cement (Fig. 1), contact between cement and endplate, anti-osteoporosis treatment, scoliosis status, preoperative Cobb angle, postoperative Cobb angle, preoperative anterior vertebral height (AVH), and postoperative AVH of the patients were recorded. Good bone cement dispersion was defined as bone cement crossing the midline of the vertebral body on spinal X-ray; otherwise, it was defined as poor bone cement dispersion. Anterior vertebral body height ratio (AVHR) was defined as the percentile of the height of the anterior margin of the compressed vertebral body relative to the mean height of the anterior margins of the adjacent upper and lower vertebral bodies. The anterior vertebral height recovery ratio (AVHRR) was defined as postoperative AVHR minus preoperative AVHR. The Cobb angle was defined as the angle formed by the superior and inferior endplates of the fractured vertebral body. The Cobb angle recovery was defined as the percentile of the preoperative Cobb angle over the postoperative Cobb angle.

Distribution of the type of bone cement. A Shape A: Bone cement is only in contact with the upper endplate. B Shape B: Bone cement is only in contact with the lower endplate. C Shape C: Bone cement is in contact with the upper and lower endplate. D Shape D: Bone cement is not in contact with the upper and lower vertebral plates
Surgical methods
The patient was placed in the prone position, frontal C-arm fluoroscopy was used to locate the bilateral projections of the pedicles of the injured vertebrae, and marker lines were drawn. The patient was routinely disinfected and draped, and 1% lidocaine was used for local anesthesia at the bilateral pedicle puncture sites. The left side was operated on first, and an incision approximately 1 cm in length was made at the projection of the left pedicle. The skin and subcutaneous tissues were incised, and the pedicle was punctured at the projection at the 10 o'clock position approximately, paying attention to the sagittal angle and the internal angle. Frontal and lateral C-arm fluoroscopy was used to confirm satisfactory puncture. The puncture needle was withdrawn, a guide needle was introduced, a working trocar was placed approximately 0.5 cm anterior to the posterior margin of the vertebral body, and the guide needle was withdrawn. A reamer was placed in the working trocar, the reamer was withdrawn, and the bone was removed and preserved for pathological examination. A compression rod was placed, the rod was withdrawn, contrast agent was injected, and then a balloon was placed and expanded to an appropriate pressure. The contrast agent was withdrawn, and the balloon was removed. The same procedure was then performed by puncturing the right side of the projection of the pedicle at approximately 2 o’clock position. A mesh bag was then placed in each working trocar bilaterally, and bone cement was injected. These operations were performed under C-arm monitoring, and cement injection was immediately discontinued if intraoperative cement leakage was detected.
Postoperative management
All patients received oral calcium supplements (600 mg/day) and active vitamin D (0.25 μg/dose, twice daily) as the foundation of treatment. Additionally, they were administered either intravenous infusion of zoledronic acid (5 mg/year) or subcutaneous injection of denosumab (60 mg/6 months). Patients wore a thoracolumbar brace for 4 months while out of bed and active. All patients underwent frontal and lateral spinal X-ray at 24 h after surgery. Follow-up was conducted at 1 month, 3 months, 6 months, 1 year, and 2 years after surgery. Telephonic follow-up was conducted for patients unable to visit for regular outpatient follow-up. Due to convenience and financial considerations, patients underwent frontal spine radiographs during follow-up. Spinal MR examination was used to support diagnosis of early NVCFs. All patients were followed up for 2 years with post-PKP re-fracture as the study endpoint.
Evaluation of re-fractures
The principal diagnostic criteria for re-fracture after PKP were as follows: 1. development of new low back pain and/or restricted lumbar motion after PKP; 2. spinal MR examination suggesting new spinal fracture with low signal in T1 phase and high signal in T2 phase; and 3. X-rays and MR examination suggesting that the fractured vertebrae were different from the previously operated vertebrae.
Statistical analysis
SPSS 26.0 and R (4.2.0) were used for statistical analysis of data. Continuous variables were expressed as mean ± standard deviation, and the independent samples t-test was used for comparison between groups. Categorical variables were expressed as percentages, and the chi-square test was used for comparison between groups. Lasso regression was used to screen for risk factors. Logistic regression was used to construct a prediction model based on the risk factors screened from Lasso regression. Risk factors were entered into a predictive nomogram prediction model using R software. Differences with p < 0.05 were considered statistically significant.
Results
Characteristics of patients
Patients were randomly divided into a training cohort and a validation cohort at a ratio of 7:3. The training cohort was used to construct the model and the validation cohort was used to test the model. In the training cohort, 32 of the 225 patients (14.2%) developed NVCFs, the control group had an average age of 74 ± 9 years and a T-score of -2.39 ± 1.23 kg/m2, and the NVCF group had an average age of 80 ± 7 years and a T-score of -3.00 ± 1.32 kg/m2. In the validation cohort, 11 of the 94 patients (11.7%) developed NVCFs, the control group had an average age of 74 ± 10 years and a T-score of 2.56 ± 1.37 kg/m2, and the NVCF group had an average age of 75 ± 10 years and a T-score of -3.55 ± 1.20 kg/m2. The clinical characteristics of the patients are shown in Table 1. No patients exhibited postoperative complications such as infection, nerve injury, vascular thrombosis, or bone cement reaction.
Construction of a Lasso-logistic regression-based prediction model
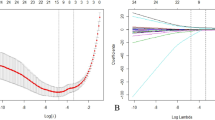
Variables were screened using Lasso regression. The changes in these variables and coefficients are shown in Fig. 2A. Iterative analysis was performed using the tenfold cross-validation method with λ = 0.043{Logλ =− 3.1} (Fig. 2) to obtain a model with good performance and the minimum number of variables. The screened variables included age, BMI, BMD, AVH, AVHRR, volume of bone cement leakage, anti-osteoporosis treatment status, and shape D (Fig. 1D, Table 2). A nomogram was created based on the screened variables (Fig. 3).

Filter variables based on lasso regression. A The variation characteristics of the variable coefficient. B The optimum value of λ in the lasso model is determined by ten-fold cross-validation

A nomogram is used to predict the risk of new vertebral compression fracture after PKP. BMI, body mass index; BMD, bone mineral density; PKP, percutaneous kyphoplasty; AVH, anterior vertebral height; AVHRR, anterior vertebral height recovery ratio
Model performance
The receiver operating characteristic curve of the model was plotted (Fig. 4) to validate its discriminative ability. The area under the curve (AUC) of the training cohort was 0.881 (CI: 0.822–0.940), and the AUC of the validation cohort was 0.929 (CI: 0.857–1.000), indicating that the model has good discriminative ability. The calibration curves of the training and validation cohorts demonstrated that the predicted results of the model were in good agreement with the actual results (Fig. 5). In the training cohort, the decision curve analysis (DCA) curve showed that the model predicted the risk of NVCF with a net benefit at a threshold probability of 2–85% (Fig. 6A). In the validation cohort, the DCA curve showed that the model predicted the risk of NVCFs with a net benefit at a threshold probability of 1–88% (Fig. 6B). Overall, the model was feasible and appropriate for prediction.

Receiver operating characteristic curves for the training A and validation B cohorts. ROC receiver operating characteristic, AUC area under the curve

Calibration plots of predicted NVCFs based on logistic regression modeling in the training A and validation B cohorts. NVCFs, new vertebral compression fractures

Decision curve analysis of nomogram prediction of NVCFs in the training A and validation B cohorts. NVCFs, new vertebral compression fractures
Discussion
OVCFs are common in patients with osteoporosis [13] and can be treated satisfactorily with minimally invasive surgery [14]. NVCFs are common and serious complications in patients with OVCFs that can lead to hospitalization. No studies have included BMD in prediction models; therefore, we developed and validated a nomogram in the present study to predict the risk of re-fracture after PKP surgery.
Osteoporosis is a systemic bone disorder characterized by low bone mass and destruction of bone tissue microarchitecture, leading to increased bone fragility and susceptibility to fracture [15]. The World Health Organization uses BMD and the T-score to define osteoporosis. The T-score is a standard deviation representing the difference between the patient and the mean BMD of healthy young adults. A T-score < − 2.5 is defined as osteoporosis, and a T-score between -1 and -2.5 is defined as osteopenia. The results of our multivariate analysis suggest that low BMD and age are independent risk factors for NVCF, and that BMD is negatively associated and age is positively associated with the development of NVCFs. In older women, increased bone remodeling in cancellous and cortical bone with negative remodeling balance leads to bone loss and destruction of bone microstructure. Cancellous bone exhibits trabecular thinning and trabecular loss, whereas cortical bone exhibits reduced cortical thickness and increased cortical porosity. In older men, osteoporosis is primarily associated with reduced bone formation and low bone turnover [16]. BMD decreases with age [17], and low BMD is a factor in surgical vertebral re-fracture that cannot be neglected [7]. An analysis of bone tissue and serum bone turnover markers in 206 patients by Qi et al. [18] showed that patients with low BMD had more necrotic bone tissue and lower bone turnover markers after fracture, indicating that patients with low BMD have poorer bone healing capacity. In addition, patients with osteoporosis have sparse trabeculae, significantly reduced vertebral body strength and compression resistance, and more severe vertebral body collapse under the same external force, making NVCFs more likely.
In our study, lack of anti-osteoporosis treatment is a major risk factor for development of NVCFs after PKP. Anti-osteoporosis treatment reduces the progression of osteoporosis and prevents the development of NVCFs [19]. In the training cohort, 98 control patients were given anti-osteoporosis treatment (51%), compared to seven NVCF patients (22%). Bisphosphonate and denosumab are first-line agents in the treatment of osteoporosis [20]. Bisphosphonate causes a progressive increase in BMD that plateaus after 3–4 years of treatment, whereas denosumab increases BMD more dramatically and persists for 10 years [20]. In a 3-year phase III clinical trial, denosumab reduced vertebral fractures by 68% [21]. Routine anti-osteoporosis treatment is recommended for post-PKP patients without contraindications.
Our study suggests that low BMI is a risk factor for NVCF. The effect of high BMI on vertebral fractures is controversial. In a study of osteoporotic fractures, high BMI was a protective factor for vertebral fracture due to the protective effect of higher adiposity [22]. Obese menopausal women tend to have higher estrogen levels, resulting in high BMD and low bone turnover and contributing to a lower risk of fracture [23]. However, it is hypothesized that obesity produces a pro-inflammatory/pro-oxidative state in bone, inhibiting bone formation and inducing bone resorption [24]. In addition, low BMI leads to NVCFs associated with low BMD [25]. Recent studies have suggested classifying Chinese adults with a BMI < 20 kg/m2 as malnourished [26]. Calcium and vitamin D are important nutritional factors in the management of osteoporosis. Calcium is an essential substance for bone mineralization and provides hardness and strength to bone [27]. Vitamin D regulates calcium homeostasis, and vitamin D deficiency also leads to osteomalacia. Studies have shown that malnutrition can promote the progression of osteoporosis [28].
In the present study, high AVHRR was considered an independent risk factor, consistent with previous findings [29,30,31]. In addition, we report for the first time that low AVH is also a risk factor. Patients with low preoperative vertebral body height tend to have higher vertebral body recovery rates. The relationship between high AVHRR and vertebral fracture has not been clearly explained. One hypothesis is that excessive vertebral body height recovery leads to increased tension of paravertebral soft tissues, which increases the mechanical load on the augmented vertebral body or the instability of the fractured segment [30]. Heo et al. [32] suggested that excessive vertebral body recovery may also increase the progression of osteonecrosis. PKP is not a procedure for correcting a deformity but rather a minimally invasive procedure used to reduce the pain experienced by patients with NVCFs. Therefore, moderate but not excessive expansion of the fractured vertebral body is recommended.
The simultaneous absence of contact between the bone cement and the upper and lower endplates, as well as the absence of cement leakage, were identified as independent risk factors for vertebral re-collapse. A retrospective study [33] found that NVCFs occurred 4.6 times more frequently in patients with bone cement leakage than in those without leakage. Other studies [34, 35] have confirmed that bone cement leaks through the ruptured endplates into the intervertebral disc, which results in altered peri-vertebral stresses and reduced disc cushioning. In addition, the distribution of bone cement in the treated vertebral body is considered a risk factor for vertebral re-fracture [36]. The results of a cohort study showed that adequate contact of bone cement with the upper and lower plates significantly reduced the risk of vertebral re-compression [37]. When bone cement contacted only the upper or the lower plate, the strength of the vertebral body was increased by only a factor of 2; however, when the cement contacted both the upper and lower plates, the strength was increased by a factor of 8–12, significantly improving stress transfer [38].
Lasso regression has the advantages of univariate analysis, as it can solve the problem of multicollinearity among variables. However, our study still has some limitations. First, the study was retrospective in nature and the effects of missing data and case selection bias were inevitable. Second, although the nomogram was validated in a validation cohort, the data were derived from the same hospital and were not validated through multiple centers in other regions and countries, which may limit the use of the model in some hospitals. Therefore, further validation in large-sample multi-center studies is needed in the future.
Conclusions
In conclusion, the present study found that advanced age, low BMI, low BMD, lack of anti-osteoporosis treatment, low preoperative vertebral height, AVHRR ≥ 2, cement leakage, and shape D (lack of simultaneous contact of bone cement with the upper and lower plates) were independent risk factors for the development of NVCFs after PKP surgery. The nomogram developed in the present study is a good predictor of the risk of NVCFs after PKP. Physicians should develop individualized follow-up strategies based on risk, utilize clinical resources rationally, and avoid overtreatment.
Abbreviations
- NVCFs:
-
New vertebral compression fractures
- PKP:
-
Percutaneous kyphoplasty
- VCFs:
-
Vertebral compression fractures
- OCVFs:
-
Osteoporotic vertebral compression fractures
- BMD:
-
Bone mineral density
- BMI:
-
Body mass index
- AVH:
-
Anterior vertebral height
- AVHR:
-
Anterior vertebral height ratio
- AVHRR:
-
Anterior vertebral height recovery ratio
- AUC:
-
The area under the curve
- DCA:
-
Decision curve analyses
References
Cummings SRE, et al. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761–1767. https://doi.org/10.1016/S0140-6736(02)08657-9.
Sambrook P, Cooper C. Osteoporosis. Lancet. 2006;367:2010–8. https://doi.org/10.1016/s0140-6736(06)68891-0.
Schlaich C, et al. Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int. 1998;8(3):261–7. https://doi.org/10.1007/s001980050063.
Ensrud KE, et al. Prevalent vertebral deformities predict mortality and hospitalization in older women with low bone mass. Fracture Intervention Trial Research Group. J Am Geriatr Soc. 2000;48:241–9. https://doi.org/10.1111/j.1532-5415.2000.tb02641.x.
Galibert P, Deramond H, Rosat P, Le Gars D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33:166–8.
Fehlings MG. The safety of percutaneous vertebroplasty and kyphoplasty. J Neurosurg Spine. 2009;11:605–6. https://doi.org/10.3171/2009.6.SPINE09359. (discussion 606).
Li YX, et al. Risk factor analysis for re-collapse of cemented vertebrae after percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP). Int Orthop. 2018;42:2131–9. https://doi.org/10.1007/s00264-018-3838-6.
An Z, et al. Logistic regression analysis on risk factors of augmented vertebra recompression after percutaneous vertebral augmentation. J Orthop Surg Res. 2021;16:374. https://doi.org/10.1186/s13018-021-02480-9.
Li Q, et al. Development and validation of a nomogram for predicting the probability of new vertebral compression fractures after vertebral augmentation of osteoporotic vertebral compression fractures. BMC Musculoskelet Disord. 2021;22:957. https://doi.org/10.1186/s12891-021-04845-x.
Bian F, et al. Risk factors for recollapse of new vertebral compression fractures after percutaneous kyphoplasty in geriatric patients: establishment of a nomogram. BMC Musculoskelet Disord. 2022;23:458. https://doi.org/10.1186/s12891-022-05409-3.
Cui L, et al. Vertebral fracture in postmenopausal Chinese women: a population-based study. Osteoporos Int. 2017;28:2583–90. https://doi.org/10.1007/s00198-017-4085-1.
Venmans A, et al. Percutaneous vertebroplasty and pulmonary cement embolism: results from VERTOS II. AJNR Am J Neuroradiol. 2010;31:1451–3. https://doi.org/10.3174/ajnr.A2127.
Lee JH, Lee DO, Lee JH, Lee HS. Comparison of radiological and clinical results of balloon kyphoplasty according to anterior height loss in the osteoporotic vertebral fracture. Spine J. 2014;14:2281–9. https://doi.org/10.1016/j.spinee.2014.01.028.
Chen L, Yang H, Tang T. Unilateral versus bilateral balloon kyphoplasty for multilevel osteoporotic vertebral compression fractures: a prospective study. Spine (Phila Pa 1976). 2011. https://doi.org/10.1097/BRS.0b013e3181f99d70.
Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 1993;94:646-650. https://doi.org/10.1016/0002-9343(93)90218-e.
Compston JE, McClung MR, Leslie WD. Osteoporosis. The Lancet. 2019;393:364–76. https://doi.org/10.1016/s0140-6736(18)32112-3.
Dai C, Liang G, Zhang Y, Dong Y, Zhou X. Risk factors of vertebral re-fracture after PVP or PKP for osteoporotic vertebral compression fractures, especially in Eastern Asia: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17:161. https://doi.org/10.1186/s13018-022-03038-z.
Qi H, Qi J, Gao J, Sun J, Wang G. The impact of bone mineral density on bone metabolism and the fracture healing process in elderly Chinese patients with osteoporotic vertebral compression fractures. J Clin Densitom. 2021;24:135–45. https://doi.org/10.1016/j.jocd.2020.11.003.
Cosman F. Anabolic therapy and optimal treatment sequences for patients with osteoporosis at high risk for fracture. Endocr Pract. 2020;26:777–86. https://doi.org/10.4158/ep-2019-0596.
Reid IR, Billington EO. Drug therapy for osteoporosis in older adults. Lancet. 2022;399:1080–92. https://doi.org/10.1016/S0140-6736(21)02646-5.
Cummings SR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361:756–65. https://doi.org/10.1056/NEJMoa0809493.
Nevitt MC, et al. Risk factors for a first-incident radiographic vertebral fracture in women > or = 65 years of age: the study of osteoporotic fractures. J Bone Miner Res. 2005;20:131–40. https://doi.org/10.1359/JBMR.041003.
Tanaka S, Kuroda T, Saito M, Shiraki M. Overweight/obesity and underweight are both risk factors for osteoporotic fractures at different sites in Japanese postmenopausal women. Osteoporos Int. 2013;24:69–76. https://doi.org/10.1007/s00198-012-2209-1.
Ronis MJ, Mercer K, Chen JR. Effects of nutrition and alcohol consumption on bone loss. Curr Osteoporos Rep. 2011;9:53–9. https://doi.org/10.1007/s11914-011-0049-0.
Reid IR. Fat and bone. Arch Biochem Biophys. 2010;503:20–7. https://doi.org/10.1016/j.abb.2010.06.027.
Wang Y, et al. Establishing a new body mass index cutoff value for malnutrition diagnosis using the Global Leadership Initiative on Malnutrition (GLIM) tool in Chinese older adults. J Parenter Enter Nutr. 2022;46:1071–9. https://doi.org/10.1002/jpen.2296.
Bonjour JP. Calcium and phosphate: a duet of ions playing for bone health. J Am Coll Nutr. 2011;30:438S-448S. https://doi.org/10.1080/07315724.2011.10719988.
Montalcini T, et al. Osteoporosis in chronic inflammatory disease: the role of malnutrition. Endocrine. 2013;43:59–64. https://doi.org/10.1007/s12020-012-9813-x.
Lin WC, et al. Refractures in cemented vertebrae after percutaneous vertebroplasty: a retrospective analysis. Eur Spine J. 2008;17:592–9. https://doi.org/10.1007/s00586-007-0564-y.
Yu W, Xu W, Jiang X, Liang D, Jian W. Risk factors for recollapse of the augmented vertebrae after percutaneous vertebral augmentation: a systematic review and meta-analysis. World Neurosurg. 2018;111:119–29. https://doi.org/10.1016/j.wneu.2017.12.019.
Zhu S, et al. Risk factors of cemented vertebral refracture after percutaneous vertebral augmentation: a systematic review and meta-analysis. Neuroradiology. 2020;62:1353–60. https://doi.org/10.1007/s00234-020-02495-9.
Heo DH, Chin DK, Yoon YS, Kuh SU. Recollapse of previous vertebral compression fracture after percutaneous vertebroplasty. Osteoporos Int. 2009;20:473–80. https://doi.org/10.1007/s00198-008-0682-3.
Yoo CM, et al. The analysis of patterns and risk factors of newly developed vertebral compression fractures after percutaneous vertebroplasty. J Korean Neurosurg Soc. 2012;52:339–45. https://doi.org/10.3340/jkns.2012.52.4.339.
Komemushi A, et al. Percutaneous vertebroplasty for osteoporotic compression fracture: multivariate study of predictors of new vertebral body fracture. Cardiovasc Intervent Radiol. 2006;29:580–5. https://doi.org/10.1007/s00270-005-0138-5.
Ahn Y, Lee JH, Lee HY, Lee SH, Keem SH. Predictive factors for subsequent vertebral fracture after percutaneous vertebroplasty. J Neurosurg Spine. 2008;9:129–36. https://doi.org/10.3171/SPI/2008/9/8/129.
Zhang L, et al. Bone cement distribution in the vertebral body affects chances of recompression after percutaneous vertebroplasty treatment in elderly patients with osteoporotic vertebral compression fractures. Clin Interv Aging. 2017;12:431–6. https://doi.org/10.2147/CIA.S113240.
Tan L, Wen B, Guo Z, Chen Z. The effect of bone cement distribution on the outcome of percutaneous Vertebroplasty: a case cohort study. BMC Musculoskelet Disord. 2020;21:541. https://doi.org/10.1186/s12891-020-03568-9.
Chevalier Y, et al. Cement distribution, volume, and compliance in vertebroplasty: some answers from an anatomy-based nonlinear finite element study. Spine. 2008;33:1722–30. https://doi.org/10.1097/BRS.0b013e31817c750b.
Funding
This research was supported by grant from the National Nature and Science Foundation of China(81873128).
Author information
Authors and Affiliations
Contributions
Conceptualization: AZ; methodology: AZ and YL; validation: AZ; formal analysis: YL; investigation: MK and WG; data curation: MK; writing—original draft preparation: AZ and YL; writing–review and editing: JC and JF supervision: JW; project administration: ZC. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Zhejiang Provincial People’s Hospital(QT2023051). This retrospective study was a retrospective analysis of anonymized data, so the institutional review board approved the waiver of informed consent. All experiments were approved by the medical ethics committee of the Zhejiang Provincial People's Hospital. The requirement for informed consent was waived due to the retrospective analysis of anonymous data.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, A., Lin, Y., Kong, M. et al. A nomogram for predicting the risk of new vertebral compression fracture after percutaneous kyphoplasty. Eur J Med Res 28, 280 (2023). https://doi.org/10.1186/s40001-023-01235-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01235-y