
Abstract
Background and objectives
Substance use in women is associated with unique psycho-social and physical vulnerabilities and poses complex challenges during pregnancy and motherhood. Gender-sensitive drug policy which considers the needs of women and their children could address these concerns. The objectives of this study were: (1) to systematically explore national-level drug policies’ sensitivity and responsiveness to women, pregnant women, and children; and (2) to examine the adherence of drug policies with international guidelines for gender sensitivity in drug policy.
Methods
The research team was diverse professional backgrounds and nine countries. A summative content analysis of national drug policy documents, action plans, and strategies was performed. Specific documents focusing on women, pregnancy, and children were analysed. Specific themes and how frequently they appeared in the documents were identified. This quantification was an attempt to explore usage indicating the relative focus of the policies. A thematic map was developed to understand how national-level drug policies conceive and address specific concerns related to women who use drugs. We adapted the UNODC checklist for gender mainstreaming to assess policies’ adherence to international guidelines.
Results
Twenty published documents from nine countries were reviewed. The common themes that emerged for women, pregnancy, and children were needs assessment, prevention, treatment, training, supply reduction, and collaboration and coordination. Custody of children was a unique theme for pregnant women. Specific psycho-social concerns and social reintegration were special themes for women, whereas legislation, harm reduction, research, and resource allocation were children-specific additional themes. For women-specific content analysis, special issues/concerns in women with drug misuse, need assessment, and prevention were the three most frequent themes; for the children-specific policies, prevention, training, and treatment comprised the three most occurring themes. For pregnant women/pregnancy, prevention, treatment, and child custody were the highest occurring themes. According to ratings of the countries’ policies, there is limited adherence to international guidelines which ensure activities are in sync with the specific needs of women, pregnant women and their children.
Conclusion
Our analysis should help policymakers revise, update and adapt national policies to ensure they are gender-responsive and address the needs of women, pregnant women and their children.
Similar content being viewed by others

Background
Women comprise one-third of people who use drugs globally and account for one-fifth of the estimated global number of people who inject drugs [1]. Women comprised one-third of overdose deaths in the US and about one in four in Canada in 2017–18. The rate of fatal overdoses among women has increased by 260–500% in the last two decades [2]. Women also suffer serious long-term social and health consequences of incarceration related to drug use and drug-related offenses which are different to those suffered by men [3,4,5]. The latest European report on Women and Drugs estimated one in four people with serious drug problems and one in five entrants to treatment programs were women. Despite the disease burden, the report lamented limited availability of integrated and coordinated national-level gender-specific services and gender-mainstreaming responses of drug use-related problems [6].
Women face particular challenges related to drugs including gender, effects of drug use during pregnancy (e.g., neonatal abstinence syndrome, low birth weight, and premature birth), motherhood, gender-based violence, higher involvement in sex work, higher prevalence of (sexual) trauma, double stigma (being discriminated against for being a woman and persons who use drugs) with serious psychosocial consequences [7]. These challenges require gender-specific policy responses. Drug policy should be well-aligned with the objectives of sustainable development goals (SDG-2030), which envisage gender equality and empowerment [8]. Therefore, it is important to assess whether women who use drugs currently receive attention in drug policies and programs and in what ways. Assessing gender-specific elements of national drug policies may help to address the particular challenges faced by women who use drugs and improve access to rights- and evidence-based harm reduction, treatment, rehabilitation, and social reintegration programs adapted to the needs of women. Treatment services often are less accessible and do not align with the needs of women with substance use disorders, as they are designed to respond to the needs of the majority in treatment, namely men. Women who use drugs are typically stigmatized for their drug-use, marginalizing them from mainstream society. This can cause fear of legal sanctions and loss of child custody making them less likely to seek treatment. Women report social stigma in private and professional contexts as a barrier to seeking and accessing treatment [9].
Even though for most drug use remains lower among women than men, there are substances where these differences are less evident. For instance, the prevalence of non-medical use of tranquilizers and opioids remains comparable to that of men, if not higher in women [5, 10]. Underlying reasons for substance use may also differ, for example, self-medication after experiencing childhood adversity events and internalized behaviours. Women also tend to progress more rapidly than men from initiating substance use to developing substance use disorders known as telescoping [11]. Women who inject drugs have a higher risk for drug-related infectious diseases than men since they are likely to share injecting equipment with more people, and/or to trade sex for drugs or money while at the same time having difficulties negotiating condom use with sexual partners [12, 13].
Identifying and understanding gender differences in drug use and disorders is a starting point. It can help shape gender-sensitive policies and practices that respond to the needs of women and mothers who use drugs. A further issue which has a significant effect on women who use drugs and their children is policy and interventions which punish rather than support these women [12, 14,15,16]. The stigma and fear associated with loss of child custody and/or punitive legal measures often deter women from seeking treatment. Of particular concern is quasi-compulsory treatment delivered through child-protection services, practiced in several countries which lacks adequate scientific evidence [17].
Although gender in drug policies was first discussed at the 1984 Ministerial Conference of the Pompidou Group, the pioneer in Europe regarding the integration of the gender dimension into drug policies [10], in recent decades there has been a growing awareness of the importance of incorporating gender perspectives into national and international drug policies and practices. This has resulted in numerous publications and documents on drug policies and national and international drug strategies that give an increasingly significant place to gender perspectives.
The latest publications of the Pompidou Group related to the gender perspective in drug policy put gender sensitivity in drug responses into the focus of policymakers and practitioners, with an emphasis on integrating specific gender needs when providing services, as well as protecting the rights of children in families affected by substance use [7, 18].
The UNODC and WHO developed international standards for treating drug use disorders that will benefit policymakers, managers of health and social services, and practitioners working with people with drug use disorders. The standards aim to help achieve health target 3.5 of the United Nations 2030 Agenda for Sustainable Development by “strengthening prevention and treatment of substance abuse” and universal health coverage for people with drug use disorders. The standards will also support the evaluation and ongoing improvement of services and the development of new policies and treatment systems. Some of these quality standards are related to the fact that treatment services should be gender-sensitive and oriented toward the needs of the populations they serve. Services for women, pregnant women and women with children who use drugs should be non-discriminatory and comprehensive, and tailored to their needs. This is relevant for all aspects of intervention design and delivery, including location, staffing, program development, child-friendliness, and content [6, 19]. Maintaining or improving relationships with children may play a central role in women’s drug use and recovery [6]. Limited availability of evidence-based recommendations for identifying and managing substance use and substance use disorders in pregnancy, for managing neonatal abstinence syndrome, and care for children of parents who use drugs places women and their children at further risk of harm [20]. Therefore, we felt an urgent need to do an in-depth analysis of the drug policies’ sensitivity towards women, pregnancy, and motherhood.
This study aims to analyze nine countries’ national policies and programs from the perspectives of their sensitivity towards women, pregnancy, and motherhood. The two broad objectives were: (1) to systematically explore national-level drug policies/strategies/action plans’ sensitivity and responsiveness to women, pregnancy, and children; and (2) to examine the adherence of drug policies/strategies/action plans with international guidelines for gender sensitivity in drug policy. Our predominant focus is on illegal drugs. The countries were chosen according to the authors’ country of origin. We believe the authors’ familiarity of the content and language would allow an in-depth analysis of the national policies.
Methods
Research team
The research team was put together by the Intercontinental Perspectives on Global Addictions and Drug Markets (Inter-GLAM) project. Inter-GLAM is a European project, co-funded by the European Union’s DG Justice Programme “Drugs Policy Initiatives—Supporting initiatives in the field of drugs policy” (JUST-2019-AG-DRUGS) from July 2021 to end of June 2023. The mandate of the research team was to work on recognizing global diversity in public health responses.
The team comprised nine researchers, clinicians, and academics from diverse professional backgrounds. Three were addiction psychiatrists, two were drug policy experts, and there was one each from medicine, public health, psychology, social pedagogy, and social anthropology. The members were affiliated with public healthcare sectors (n = 3), academic institutions (n = 3), and research bodies (n = 3). The common denominator was their expertise in the public health concerns associated with drug and alcohol use and drug policy. The team members were from the European (n = 5), Eastern Mediterranean (n = 2), Asian (n = 1), and African (n = 1) regions. Each member contributed to collecting, organizing, and reviewing drug policy documents of their country of work.
Study design
A summative content analysis was performed of the published national drug policy documents/action plans/strategies. A quantitative description of the frequencies of the identified themes was presented.
Theoretical framework
The content analysis was not theory-driven, but it was data-driven. Preconceived coding categories were not used—codes and names for codes were allowed to emerge from the data. Researchers immersed themselves in the data to form new insights through the codes.
Sampling and sample size
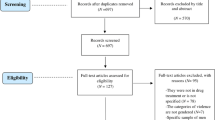
Twenty published national drug policies and related documents from nine countries (Botswana, Croatia, Egypt, India, North Macedonia, Netherlands, Poland, Portugal, and Spain) were reviewed.
Search strategy
The authors provided the drug policy documents for their respective countries of origin. We included policy documents related to supply, demand, and harm reduction, published in any language and any year of publication. We included any revised policy documents. We excluded documents exclusively on legal substances (e.g., alcohol and tobacco); however, if any country had a common policy document for all substances, these were included. Moreover, for countries that did not have a national-level drug policy (e.g., Botswana), we included alcohol and tobacco policy reports and national health/public health policies.
Method of approach
To search the relevant text matters within the policy documents, the following keywords were used “women,” “gender,” “children,” “minors,” “underaged, “pregnancy,” and “motherhood.” The authors of the respective countries also reviewed the full report to identify missing relevant text matter. For searching non-English documents, keywords were translated into the language of the concerned policy document. Non-English language texts were translated into English by the concerned author. Text was extracted into a Google Spreadsheet. Content analysis was performed on these texts/excerpts.
Analysis
After thoroughly reading the text and data immersion, DJ and AG independently generated codes to indicate specific concerns for women, pregnant women/pregnancy, and women with children. Codes were also generated for the strategies discussed to address these concerns. The words, phrases, sentences, and paragraphs of text extracts were double coded. Coding categories were derived directly and inductively from the raw data using the constant comparative method. The coders checked the coding consistency across documents. An explicit or manifest coding approach was used to minimize the effects of subjective judgments on analysis [21]. Coded words and phrases were sought and the analysis did not go into the message behind the text. Frequently mentioned and similar codes were combined to generate themes. Coding discrepancies between DJ and AG were reflected upon and resolved by discussion. A repeat summative analysis by counting the occurrence of a particular theme in the reviewed policy documents was performed. This quantification was an attempt not to infer meaning but to explore usage. The quantitative information indicated the relative focus of the policies on specific themes across the areas of interest. Microsoft Excel was used for the analysis.
A thematic map was developed to integrate various codes and themes, understand how national-level drug policies are conceived, and further address the specific concerns for women, pregnancy, and motherhood.
An adapted version of the UNODC checklist for gender mainstreaming in projects/programs was used to assess the national-level policies/strategies/action plans adherence to international guidelines [22]. The checklist was developed in 2021, envisioning the UN requirement of a global strategy for promoting gender equality in any planned action, including legislation, policies, or programs. The original checklist has 14 items which rates adherence as “yes” or “no.” The items are classified into three groups: situation analysis (n = 5), plan description (n = 3), and plan management (n = 2). Situation analysis asks about the magnitude of drug problems among women, pregnant women, and women with children, and seeks to understand whether the differential impact of national strategies and international best practices are considered and how the policy aims to reach and empower women with drug misuse. Plan description includes the locus of care, provision of gender-sensitive care, and gender-responsive indicators. Plan management comprises logistics and financial support, and implementation measures. The checklist was adapted to include only 10 items. Three unrelated items were removed (i.e. staffing, resource mobilization, counterpart capacity) and two items were combined. The items were rated on a seven-point Likert scale (“strongly disagree” to “strongly agree”) because adherence should lie in a continuum. DJ made the initial adaptation and shared the checklist with AG, who reviewed and commented on the adaptation. The agreed version was shared with the research team for their comments and suggestions, and the checklist was finalized. The final checklist was shared with the research team for rating the adherence of their national policies to each of the items.
Results
Brief description of the studied documents
Twenty documents from nine countries were reviewed; Botswana, Croatia, Egypt, India, The Netherlands, North Macedonia, Poland, Portugal and Spain. Two national-level drug policy/program/action plan documents were retrieved from the following countries: Croatia, Portugal and Spain. The highest number (n = 5) of documents reviewed was from Poland. Three relevant drug policy documents were found from The Netherlands and one from North Macedonia. No drug policy-specific document was found for Botswana; however, a member of the research team reviewed the country's alcohol and health policies. Except for The Netherlands, all countries mention women, pregnancy, and motherhood-related concerns in a common drug policy document or national strategies. Only the Netherlands has a specific document directed towards pregnant women, a factsheet produced by the Dutch Association for Obstetrics and Gynaecology, “Vulnerable pregnant women and protection of the unborn child” which is part of a series about (domestic) violence, abuse, neglect, exploitation and other types of harm that may be inflicted onto someone in a power-imbalanced relationship [23].
Original publication of all these documents was in the last decade, except for “Counteracting drug addiction,” a drug demand reduction policy report from Poland, published in 2005 [24], and the Dutch policy, published in 1995 [25]. Five of the nine countries (Egypt, India, Croatia, Spain, and Poland) updated/ revised their drug policy in recent years [26,27,28,29,30,31]. North Macedonia brought out its latest drug policy in 2021 [32]. Two countries (Portugal and Botswana) have not updated their policies in the last ten years [33,34,35]. In most countries (n = 5), the Ministry of Health was responsible for publication of drug policy reports. However, different ministries in India, Poland, and Botswana have issued drug/alcohol policy documents, namely the Ministry of Social Justice and Empowerment, the Ministry of Finance/Trade, and the Ministry of Education. Spain has specific Ministerial involvement for drug policy measures and implementation, the Government Delegation for the National Drug Plan [36]. All nine countries intend to use the state budget to implement drug programs.
Table 1 provides further details.
Content analysis of the national policy/programs/strategies
We describe the results of the conventional content analysis as per “women,” “pregnancy,” and “children” sensitive/responsive texts in the reports.
-
a. Women-sensitive policy
We identified 19 unique codes from the content analysis. The recurrent and similar codes were combined to generate 11 major themes. The excerpts from the policy documents were quoted and presented in Table 2.
-
1. Special concerns in women
Several policy documents discussed the need to recognize and address special issues in women with drug use. Vulnerability, shame, blame, stigma, gender role, and gender violence were specifically mentioned.
-
2. Needs assessment
Needs assessment refers to a practice for estimating the nature and magnitude of a health or social problem in a community/state/country where there is the intent to ameliorate or otherwise respond to that problem. The drug policy documents we reviewed described the need to conduct surveys among women and at-risk populations, not only to understand the problem but also to design acceptable and effective strategies to address it. Spain’s policy, in addition to the importance of conducting drug surveys, discusses a gender-responsive analytical framework to understand and integrate the needs of women with drug misuse.
-
3. Prevention
The prevention strategies discussed in the documents included both universal actions, such as raising awareness in the general population, and the need for selective and indicated prevention programs and interventions targeting women.
-
4. Treatment
Drug policy measures from various countries emphasize the role of gender-sensitive treatment. India’s National Action Plan for Drug Demand Reduction (2018–2025) talks about the provision of treatment in closed custodial settings and combined women with other vulnerable populations [26].
-
5. Social reintegration
Policy measures are needed to develop and promote interventions and strategies to address housing, education, vocational training and employment. These interventions can be grouped as strategies for social reintegration. North Macedonia’s national health policy talks about providing social and economic opportunities [32].
-
6. Supply reduction
Supply reduction means using strategies to disrupt the production and supply of illicit drugs. Interrupting drug trafficking along the shipping, air, and road transport routes is one supply reduction measure. The relationship between women and the drug trade is complex. Women’s participation in the drug supply chain can be attributed to vulnerability and oppression, where they are forced to be involved out of fear or exploitation. Another narrative explains the involvement in the drug trade as their own decision. Women may be involved in trafficking to sustain their drug consumption or be victims of in-person trafficking [4].
-
7. Training
The national policies recognized the need for workforce training and capacity building in gender-responsive prevention and treatment. The training need extends to non professional voluntary workers and peer groups.
-
8. Collaboration and coordination
Several national policies mentioned the need for inter-ministerial, inter-sectoral, and international collaborations to achieve the objectives of the policy documents. The Spanish National Strategy on Addictions states as a strategic objective, “Guarantee quality integrated care” which includes the coordination of resources for women who suffer gender-based violence and their children [31].
-
9. Monitoring and evaluation
Periodic surveillance is required to inform policymakers about existing drug policies’ effectiveness and limitations. Only a few of the countries’ policies reiterated the importance of gender-sensitive indicators for monitoring the implementation and outcome of the policy measures.
-
10. Policy
Policies are guiding principles chosen by a government and dictate the strategies and action plans to address a particular issue, e.g. control and regulation of psychoactive drugs.
-
11. Resource allocation
Resource allocation refers to assigning available resources to various uses.
-
b. “Pregnant women” sensitive policy
We discovered five major themes from nine different codes from the content analysis of the policy text concerning pregnant women. Four of the five themes have already been discussed while discussing women-sensitive policy. The only new theme that emerged in this section is the custody of children of women with drug misuse. Please see Table 3 for the excerpts from the policy documents, codes and themes.
-
1. Prevention
Universal prevention, such as education/awareness generation of pregnant women and their partners regarding the harmful effects of drugs on fetal development. Some policy texts broadened the scope of prevention by incorporating prevention of exposure to psychoactive substances during pregnancy, further preventing the fetal neurobehavioral and developmental consequences. As mentioned earlier, Spanish policy promotes screening, early identification, and brief interventions for alcohol in “…sexual and reproductive care services, family planning, pre-pregnancy visits, and obstetrics, as well as sexually transmitted infection units” [31].
-
2. Treatment
This was largely discussed in the context of gender-sensitive treatment, in the context of women and pregnant women together, or with an exclusive focus on pregnant women. The Portuguese policy also aspires to deliver a seamless and integrated model at all levels of care.
-
3. Custody issues
Child custody refers to a child's care, control, and maintenance through a legal mandate. The court aims to look after a child's best interest in deciding custody rights. Penalties for substance use in pregnancy can include loss of custody, compulsory treatment, and fines. [23, 40]. Fear of loss of custody can lead to some women avoiding seeking treatment [20].
-
4. Training
Training of human resources was discussed with the need for specialized gender, and youth sensitive training on the prevention and treatment of drug misuse. For example, the Indian drug demand reduction policy stated, “Specialized training for those who work with vulnerable groups, such as patients with psychiatric co-morbidities, children and women, including pregnant women.” [27].
-
5. Collaboration and coordination
A few national drug policies expressed the need for coordination between various levels of service delivery systems: prevention, treatment, and harm reduction and also collaboration between services for women, pregnant women, and their children [27, 32, 33].
-
c. Children-sensitive policy
The content analysis of policy documents that pertained to children revealed 20 unique codes and 10 major themes. Most themes (n = 7) were similar to those captured and already described under the women/gender-sensitive policy matters, such as needs assessment, prevention, treatment, supply reduction, training, collaboration and coordination, and policy. Additional themes discovered were legislation (to protect children), resource allocation, research, and harm reduction. Below we discussed only those themes exclusive to “children”/“children with a parent who uses drugs.” The excerpts supporting the codes and additional themes were presented in Table 3.
-
1. Legislation
Legislation signifies creating and implementing laws to prevent the production/manufacture/cultivating, possessing, selling, purchasing, transporting, storing, and/or consume any psychoactive substances. It aims to reduce the supply/access to drugs to those who use drugs.
-
2. Research
Research is an integral component of drug policy. Preventive intervention research is important in this particular context of drug policies on children. Prevention may target the at-risk population, which is known as selective prevention. Portuguese policy alludes to the commitment to conducting risk-factor research.
-
3. Harm reduction
Harm reduction refers to policies, programs, and practices that minimize drug use’s negative health, social and legal impacts. Harm reduction was cited in the Spanish national strategy, not for children, but for adults in order to protect the children in the family i.e., to minimize harm to others.
Summative quantitative analysis
Figure 1 depicts the number of times a particular theme occurred during the content analysis. Because the themes were different for three categories (e.g., women, pregnant women, children) and we wanted to check the relative frequency of occurrence of a particular theme in a specific category, we presented the “theme count” category-wise.

Summative analysis of the category-wise theme frequency (occurrence of a particular theme in the policy documents)
For women-specific content analysis, special issues/concerns in women with drug misuse, need assessment, and prevention were the three most frequent themes; for the children-specific policies, prevention, training, and treatment comprised the three most occurring themes. For pregnant women's sensitive policy texts, prevention, treatment, and child custody were the highest-occurring themes.
Thematic map
Figure 2 illustrates the thematic map to visualize the cross-connections between common and unique themes (specific to the target population) discovered during the content analysis. All policies/programs are envisioned to prevent and treat drug misuse among women, pregnant women, and children. They emphasized the importance of needs assessment to understand the magnitude and patterns of the problem. The prevention can be universal (that is desirable for everybody in the eligible population, e.g., raising awareness and education at the population level), selective (identifying and addressing concerns of the vulnerable population), and indicated (early detection of risk factors and condition, and providing intervention to prevent future development of SUD). However, some policies reported the need for supply reduction and legislation to protect children and women (and the unborn children of pregnant women) as preventive measures. The policies talked about training and capacity building of human resources to deliver gender-sensitive care. Special psychosocial concerns in women with drug misuse, such as the stigma, blame, gender-based violence, and typical gender-role, must be examined and addressed in a gender-sensitive prevention and treatment program. Following treatment, national drug policies envisage providing socio-economic opportunities for the social reintegration of women with drug misuse. Drug policies deliberated on the child custody issues for pregnant women with drug misuse and linked this with the treatment. Implementing the policy measures will require inter-ministerial and international collaboration and coordination.

Thematic map for visualizing inter-relationships between concepts and among main themes and subthemes. Green colored boxes are themes common to women, pregnant women, and children. Orange colored boxes are themes unique to women. Pink colored boxes contain unique theme for pregnant women. Blue colored boxes are children-specific themes
The performance of policies must be periodically monitored by gender-sensitive indicators and adapted to the changing needs and demands.
Adherence of the national policy/programs/strategies to the adapted checklist for gender-sensitive policy
Each author rated their own country’s policy reports. According to the ratings of the country’s gender-sensitive policy, there is limited adherence to international guidelines and lessons learned on gender equality and women’s empowerment, and engendering results chain which ensures outcome, output, and activities are in sync with the specific need in women and for pregnancy, and motherhood. Five and six out of nine members responded with different grades of disagreements (regarding their country’s policy adherence) on the likert scale for these two items, respectively.
Very little agreement was reached regarding the provision of gender-responsive indicators (agreement = 2/9) and targets and adequate and sustainable financial resources to implement the components of the policy (agreement = 1/9). The adherence is relatively better for the background situation and context analysis (agreement = 6/9), consideration of differential impact and strategies (agreement = 7/9), targeted approach to reach out to this special population (agreement = 7/9), envisioning equality and women empowerment (agreement = 7/9), improving access and participation in interventions (agreement = 6/9), and monitoring and evaluation of the implementation of the policy measures (agreement = 7/9). The agreement includes those who at least “somewhat agreed” to the checklist items. See Fig. 3 for finer details.

Adherence of national policies with the adapted check-list for gender-sensitive policy
Discussion
Gender differences in drug use patterns, characteristics, and intervention needs represent an important policy issue addressed to various extents in different countries [42]. Our first objective was to systematically explore national-level drug policies/strategies/action plans’ sensitivity and responsiveness to women, pregnancy, and motherhood.
The content analysis showed common and unique themes for all three included categories. For women, pregnant women, and children among the most frequently mentioned themes were prevention and treatment. This can be seen as a continuum of drug demand reduction responses relevant for people with substance-use disorders and their families that most of the included countries recognized as relevant [43]. Special concerns and needs assessment were among the most frequent themes for women. Women who use drugs have high rates of mental health problems and histories of childhood abuse, and greater vulnerability to drug-related harms [40, 44]. Our analysis shows that these issues have been addressed in the context of gender-sensitive drug policy responses in some (but not all) countries. Needs assessment was recognized as an important factor in providing adequate care. This aligns with research showing that combining integrated services based on the needs assessment can result in positive outcomes for individuals, families, and society [12, 43, 45].
The importance of child custody for children of mothers with drug-related disorders was considered a unique issue and the most frequent theme for pregnant women. Child custody has a long-term effect on children throughout their adulthood. Faherty et al. [14] emphasize that penalties for substance use in pregnancy can include loss of custody, which can have repercussions on children’s development and produce additional expenses for society [14]. Pregnant women with substance use disorders should get the care and support they need, not only in the context of treatment but also through supporting their motherhood [6, 12, 15, 16]. However, this theme also reflects the gendered differences in the perception of substance use and its conflict with the traditional gender role, where mothers are expected to care for and raise children, not fathers [46].
Among the most frequent themes for the children-specific category was training. Most countries recognize the importance of trained professionals when delivering interventions, which aligns with the guidelines for delivering effective interventions [47], and is supported and recognized by relevant international bodies [7]. While the themes found generally align with research evidence, it is unclear how much this has influenced the country’s policies.
The policy documents used stigmatizing language to depict persons who use drugs. Words and phrases such as “addicts,” “Addicted mother,” “drug users,” and “addicted women” were used in various policy documents. Although language did not typically fall under the purview of our work, we decided to code and generate additional themes because of the harmful effect of stigmatizing language in propagating public stigma. The use of inappropriate language in the policy documents might contribute to the public stigma against persons who use drugs. We recommend using neutral and person-centered language in all public and scientific documents on substance use [48]. This is more significant in women who use drugs because of the gendered perception of drug use.
Our second objective was to examine the adherence of drug policies/strategies/action plans with the international guidelines for gender sensitivity in drug policy. Findings showed that areas that need additional focus in national policies include budget, gender-sensitive indicators, engendering results chain, and synergies with other policies. It seems that a minority of the analyzed policies ensure adequate financial resources specifically for the activities for women, pregnancy, and motherhood. Likewise, gender-sensitive indicators and outcomes, outputs, and activities are not designed to a large extent to meet the different needs and priorities of included categories. Finally, the lack of synergies with other policies was recognized as an important area that can be improved by accepting the coherent approach to substance-use policies [49].
Although our analysis was limited to nine countries, our results showed some general drug policy lacunae that might apply to other countries. Gendered perception of drug use, a wide policy-practice gap resulting from inadequate resources and limited availability of gender-sensitive data, lack of synergy with other health policies, and potentially harmful and stigmatizing language use came up as significant concerns which need to be addressed.
Limitations
This study has several limitations that need to be acknowledged. Firstly, included countries came mostly from Europe and are high- or middle-income countries, which decrease the generalizability of the findings. There are differences among included countries regarding the infrastructure and responses to drug use. In addition, the chosen topic does not present an equal political priority in all included countries. In terms of policy, there is a lack of documents and national guidelines dedicated specifically to women using drugs, and also no civil society official documents were considered which means that we might be lacking a view that could complement state policies (or the lacking of gender specific approaches). Findings related to our first objective are based on content analysis, which has a component of subjectivity. Furthermore, group members came from different backgrounds and were not policy analysts by profession. Our second objective was to examine the adherence of the analyzed documents with the international guidelines for gender sensitivity in drug policy. This approach also has several limitations. First of all, the adapted Checklist focuses on women, pregnancy, and motherhood, but the situation might not necessarily be the same for the three issues. For instance, in some policy documents, there is almost no reference to pregnancy, so it is possible that an assessment was not made for all three target groups/terms in the included countries. Another area for improvement is that in the adapted Checklist, there was no option to not respond to a question, even though some questions perhaps required more information and knowledge than our group members had. Finally, each member analyzed their national policy, which might have resulted in bias and a degree of subjective interpretation. Adding a second rater could have improved the robustness; however, because of the unfamiliarity with the language of the documents and country context/situation, we had to rely on a single rater.
Conclusion
In sum, our research evinced the components in the national drug policies/documents that address special concerns in women, pregnancy, and motherhood. We identified areas that are either neglected or inadequately addressed and require further strengthening. We believe our analysis would stimulate discussion, critical review of national policies, and inclusion of gender sensitivity as a conscious and deliberate decision to meet the goals of United Nations SDG 2030 (Goal 5: Achieve gender equality and empower all women and girls).
Availability of data and materials
The URLs of the documents analyzed for the report are added to the references. Coding, thematic analysis, and adherence rating data supporting this study’s findings are available from the corresponding author, [DJ], upon reasonable request.
Abbreviations
- CSO:
-
Civil Society Organisations
- EMCDDA:
-
European Monitoring Centre for Drugs and Drug Addiction
- EU:
-
European Union
- FASD:
-
Fetal alcohol spectrum disorders
- Inter-GLAM:
-
Intercontinental Perspectives on Global Addictions and Drug Markets
- JUST-2019-AG-DRUGS:
-
European Union’s DG Justice Programme “Drugs Policy Initiatives—Supporting initiatives in the field of drugs policy”
- Misuse:
-
Harmful/hazardous use, use disorder, dependence
- PHI:
-
Public Health Institute
- SICAD:
-
General Directorate for Intervention on Addictive Behaviours and Dependencies
- EARNM:
-
Employment Agency of Republic of North Macedonia
- SUD:
-
Substance Use Disorders
- TAIEX:
-
Technical Assistance Instrument and Information Exchange Instrument of the European Commission
- UN:
-
United Nations
- UNODC:
-
United Nations Office on Drugs and Crime
- WHO:
-
World Health Organisation
References
UNODC. World drug report 2021. Vienna: U. Nations; 2021. https://www.unodc.org/unodc/en/data-and-analysis/wdr2021.html. Accessed on 12 March 2023.
Collins AB, et al. Gender and the overdose crisis in North America: moving past gender-neutral approaches in the public health response. Int J Drug Policy. 2019;69:43–5.
EMCDDA. Prisons and drugs in Europe. Current and future challenges. Luxembourg; 2022. https://www.emcdda.europa.eu/system/files/publications/13904/TDXD21001ENN.pdf. Accessed on 12 March 2023.
UNODC. Women and drugs, in world drug report 2018. Vienna: United Nations; 2018.
UNODC. World drug report 2022. Vienna: U. Nations; 2022. https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2022.html. Accessed on 12 March 2023.
EMCDDA. Women and drugs: health and social responses; 2022. https://www.emcdda.europa.eu/publications/mini-guides/women-and-drugs-health-and-social-responses_en. Accessed on 12 March 2023.
Mutatayi C et al. Implementing a gender approach in drug policies: prevention, treatment and criminal justice. A handbook for practitioners and decision makers. Strasbourg: Council of Europe; 2022. https://rm.coe.int/2022-ppg-implementing-a-gender-approach-in-drug-policies-a-pg-handbook/1680a66835. Accessed on 12 March 2023.
UN General Assembly. Transforming our world: the 2030 agenda for sustainable development 2015: U. Nations. https://sdgs.un.org/2030agenda. Accessed on 12 March 2023.
UNOV/UNODC. Strategy for gender equality and the empowerment of women (2022–2026). Vienna: United Nations; 2022. https://www.unodc.org/documents/evaluation/HumanRights-GenderEquality/Strategy_for_Gender_Equality_and_the_Empowerment_of_Women_2022-2026.pdf. Accessed on 12 March 2023.
Clark M et al. The gender dimension of non medical use of prescription drugs in Europe and the Mediterranean region. Strasbourg; 2015. https://rm.coe.int/the-gender-dimension-of-non-medical-use-of-prescription-drugs-in-europ/168075bac0. Accessed on 12 March 2023.
Keyes KM, et al. Telescoping and gender differences in alcohol dependence: new evidence from two national surveys. Am J Psychiatry. 2010;167(8):969–76.
EMCDDA. Health and social responses to drug problems: a European guide. Luxembourg; 2021. https://www.emcdda.europa.eu/publications/health-and-social-responses-a-european-guide_en. Accessed on 12 March 2023.
Larney S, et al. A gender lens is needed in hepatitis C elimination research. Int J Drug Policy. 2022;103: 103654.
Faherty LJ, Stein BD, Terplan M. Consensus guidelines and state policies: the gap between principle and practice at the intersection of substance use and pregnancy. Am J Obstet Gynecol MFM. 2020;2(3): 100137.
Goler NC, et al. Substance abuse treatment linked with prenatal visits improves perinatal outcomes: a new standard. J Perinatol. 2008;28(9):597–603.
Volkov N. Pregnant people with substance use disorders need treatment, not criminalization. Blog: National Institutes of Health National Institute on Drug Abuse. National Institutes of Health; 2023. https://nida.nih.gov/about-nida/noras-blog/2023/02/pregnant-people-substance-use-disorders-need-treatment-not-criminalization. Accessed on 12 March 2023.
Urbanoski K, Merrigan S, Milligan K. Gendered harms: The lack of evidence on treatment that is mandated by child protection services. Int J Drug Policy. 2022;99: 103481.
Giacomello C. Children whose parents use drugs. Council of Europe; 2022.
WHO & UNODC. International standards for the treatment of drug use disorders: revised edition incorporating results of field-testing. World Health Organization; 2020. https://apps.who.int/iris/handle/10665/331635. Accessed on 12 March 2023.
WHO, Guidelines for the identification and management of substance use and substance use disorders in pregnancy. Geneva: World Health Organization; 2014. https://www.who.int/publications/i/item/9789241548731. Accessed on 12 March 2023.
Wicks D. The coding manual for qualitative researchers. Qual Res Org Manag Int J. 2017;12(2):169–70.
UNOV/UNODC, Checklist for gender mainstreaming in project/programmes. Vienna; 2021. https://www.unodc.org/documents/Gender/Gender_Mainstreaming_Checklist_2021.pdf. Accessed on 12 March 2023.
Dutch Association for Obstetrics and Gynaecology. Vulnerable pregnant women and protection of the unborn child; 2020. https://www.huiselijkgeweld.nl/publicaties/factsheets/2018/11/15-september-2020/vulnerable-pregnant-women. Accessed on 12 March 2023.
Polish Journal of Laws. Act of 29 July 2005 on counteracting drug addiction. Republic of Poland; 2005. https://www.cinn.gov.pl/portal?id=216853. Accessed on 12 March 2023.
House of Representatives of the States General the Netherlands. Dutch drug policy: continuity and change (English version); 1995. https://www.emcdda.europa.eu/drugs-library/dutch-drug-policy-continuity-and-change-english_en. Accessed on 12 March 2023.
Abd El Wahab D. Egypt drug situation and policy. Council of Europe; 2014. https://rm.coe.int/drug-situation-and-policy-by-dr-dalal-abd-el-wahab-general-secretary-o/168075f0e5. Accessed on 12 March 2023.
Indian Ministry of Social Justice and Empowerment. National action plan for drug demand reduction (2018–2025). 2021 (updated): Government of India.
Croatian Ministry of Health and Croatian Public Health Institute. Proposal for the national strategy of actions in the field of addiction for the period until 2030. Government of the Republic of Croatia; 2023. https://narodne-novine.nn.hr/clanci/sluzbeni/2023_02_18_307.html. Accessed on 12 March 2023.
Croatian Office for Combating Narcotic Drug Abuse. National strategy on combating drug abuse in the Republic of Croatia for the period 2012–2017. Government of the Republic of Croatia; 2012. https://www.emcdda.europa.eu/system/files/media/country_overview/documents/2573/HR_National%20strategy_en.pdf. Accessed on 12 March 2023.
Polish SEJM. Public health act of 11 September 2015. Republic of Poland; 2015. https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20150001916/U/D20151916Lj.pdf. Accessed on 12 March 2023.
Ministry of Health & Government Delegation for the National Drug Plan. National strategy on addictions 2017–2024. Government of Spain; 2018. https://pnsd.sanidad.gob.es/pnsd/estrategiaNacional/docs/180209_ESTRATEGIA_N.ADICCIONES_2017-2024__aprobada_CM.pdf. Accessed on 12 March 2023.
North Macedonia Ministry of Health. National drugs strategy of the Republic of North Macedonia 2021–2025 with action plan 2021–2023. Republic of North Macedonia; 2021. https://hops.org.mk/wp-content/uploads/2022/05/Strategija-za-drogi_eng-final-version-1.pdf. Accessed on 12 March 2023.
SICAD Portugal. National plan for the reduction of addictive behaviours and dependencies 2013–2020. P.G.D.f.I.o.A.B.a. dependencies; 2013. https://www.sicad.pt/BK/Publicacoes/Lists/SICAD_PUBLICACOES/Attachments/61/SICAD_Plano_Nacional_Reducao_CAD_2013-2020.pdf. Accessed on 12 March 2023.
SICAD Portugal. Action plan for reduction of addictive behaviours and dependencies 2013–2016. P.G.D.f.I.o.A.B.a. dependencies; 2013. http://dge.mec.pt/sites/default/files/ficheiros/plano_acao_2013_2016.pdf. Accessed on 12 March 2023.
Botswana Ministry of Trade and Industry. National alcohol policy for Botswana. Republic of Botswana; 2010. https://saapa.africa/download/botswana-national-alcohol-policy/?wpdmdl=33770&refresh=63dccd72563381675414898. Accessed on 12 March 2023.
Government Delegation for the National Drug Plan. National drug plan. Government of Spain; 2000. https://pnsd.sanidad.gob.es/en/pnsd/Introduccion/home.htm. Accessed on 12 March 2023.
Spanish Ministry of Justice. Organic Law 3/2007, of March 22, for the equality of women and men. Government of Spain; 2007. https://www.boe.es/buscar/pdf/2007/BOE-A-2007-6115-consolidado.pdf. Accessed on 12 March 2023.
Polish SEJM. Regulation of the council of ministers of March 30, 2021 on the National Health Program for 2021–2025. Republic of Poland; 2021. https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20210000642. (in Polish). Accessed on 12 March 2023.
Botswana Ministry of Health. National Health Policy. Republic of Botswana; 2011. https://www.moh.gov.bw/Publications/policies/revised_National_Health_Policy.pdf. Accessed on 12 March 2023.
EMCDDA. Pregnancy, childcare and family: key issues for Europe’s response to drugs. Luxembourg; 2012. https://www.emcdda.europa.eu/publications/selected-issues/children_en. Accessed on 12 March 2023.
Egyptian National Council for Women. National strategy for the empowerment of egyptian women 2030. Government of Egypt; 2017. http://ncw.gov.eg/wp-content/uploads/2018/02/final-version-national-strategy-for-the-empowerment-of-egyptian-women-2030.pdf. Accessed on 12 March 2023.
Thomas N, Bull M. Representations of women and drug use in policy: a critical policy analysis. Int J Drug Policy. 2018;56:30–9.
Council of the European Union. European drug strategy 2021–2025; 2020. https://www.consilium.europa.eu/media/49194/eu-drugs-strategy-booklet.pdf. Accessed on 12 March 2023.
Trost LBJ, Njie F, Chandra G, Njie F, Berry J, Harvey A, Goodman DA. Pregnancy-related deaths: data from maternal mortality review committees in 36 US States, 2017–2019; 2022. https://www.cdc.gov/reproductivehealth/maternal-mortality/docs/pdf/pregnancy-related-deaths-data-mmrcs-2017-2019-h.pdf. Accessed on 12 March 2023.
Sword W, et al. Integrated programs for women with substance use issues and their children: a qualitative meta-synthesis of processes and outcomes. Harm Reduct J. 2009;6:32.
Campbell N. Using women: gender, drug policy, and social justice. Psychology Press; 2000.
Nation M, et al. What works in prevention. Principles of effective prevention programs. Am Psychol. 2003;58(6):449–56.
Volkow ND, Gordon JA, Koob GF. Choosing appropriate language to reduce the stigma around mental illness and substance use disorders. Neuropsychopharmacology. 2021;46(13):2230–2. https://doi.org/10.1038/s41386-021-01069-4.
Muscat R, Pike B, Members of the Coherent Policy Expert Group. Coherence policy markers for psychoactive substances. Strasbourg: Council of Europe. Strasbourg; 2014. https://rm.coe.int/coherence-policy-markers-for-psychoactive-substances/168075acb8.
Acknowledgements
Thanks to the following members of the InterGLAM Work Group 4: Recognising global diversity in public health responses; putting evidence into practice in different cultures and settings: Hossein Hassanian-Moghaddam, Johan Jongbloet, Julie Schamp, Irena Molnar, Kali Sedgemore, Senad Hasanagic, Gelareh Mostashari.
Funding
This work is supported by the Inter·GLAM project, co-funded by Grant No. 957776 under the European Union’s DG Justice Programme “Drugs Policy Initiatives—Supporting initiatives in the field of drugs policy” (JUST-2019-AG-DRUGS), running from 01/7/2021 to 30/6/2023.
Views expressed in this paper and any supplementary materials do not necessarily reflect the views of the European Commission.
Author information
Authors and Affiliations
Contributions
Conceptualisation, data collection, writing—reviewing and editing: AG, DJ, LAI, CB, DII, KOK, JMM, TFM, AN, JC, RC, Writing—original draft preparation: AG, DJ, LAI, Methodology, analysis: AG, DJ, Proofreading and editing: RG. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors delcare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ghosh, A., Jerkovic, D., Ignjatova, L.A. et al. Drug policies’ sensitivity towards women, pregnancy, and motherhood: a content analysis of national policy and programs from nine countries and their adherence to international guidelines. Addict Sci Clin Pract 18, 53 (2023). https://doi.org/10.1186/s13722-023-00410-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13722-023-00410-0