
Abstract
Women account for one in every three people who use drugs worldwide and tend to progress to drug use disorders in a shorter time than men. There is limited understanding of the situation of women who use drugs in the Middle East and North Africa. A multi-stakeholder rapid situation assessment (RSA) was conducted which aimed to investigate gendered and contextual vulnerabilities and service level responsiveness to the needs of women who use drugs (WWUD) in Egypt. An updated profile of female service user characteristics was sought via mapping of addiction and harm reduction services in the National Drug Observatory system. In-depth interviews were conducted with a purposive sample of representatives of UN agencies and health professionals providing treatment/harm reduction (government, private, community) (n = 21). Focus groups were facilitated with a convenience sample of women in treatment, accessing HIV services and community harm reduction services (n = 75). Thematic analysis and triangulation across data sources occurred. Eight themes emerged: profile of women who use drugs; access to drugs and settings for female drug use; dimensions of stigma; trauma and drivers of female drug use; networks and intimate partner relationships; high-risk behaviours and harms; barriers to help-seeking and accessing services; and enhancing gender-responsive and gender-transformative evidence-based services. This RSA yields a contemporary insight into the vulnerabilities, traumas, discrimination and stigma-related challenges experienced by WWUD in Egypt. Recommendations are made to enhance harm reduction awareness and uptake and to integrate gender-responsive care within existing maternal, addiction and harm reduction service structures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Women account for one in every three people who use drugs worldwide (UNODC, 2022a). Women tend to progress more rapidly to drug use disorders and are more likely to be diagnosed with a psychiatric illness and less likely to enter treatment (Agterberg et al., 2020; EMCDDA, 2017, 2023; Greenfield et al., 2007; Harrop & Marlatt, 2010; Valencia et al., 2020). There are identified sub-groups of vulnerable women who use drugs (WWUD): women affected by violence and trauma and co-morbidity, are pregnant and/or parenting, members of ethnic minorities, sex workers or living in prisons (CoE, 2022; El-Bassel & Strathdee, 2015; EMCDDA, 2017, 2023; Strathdee et al., 2015; Tripodi & Pettus-Davis, 2013). Many WWUD face numerous barriers in accessing drug treatment services, due to the fear of possible legal sanctions and social stigma relating to their drug use, lack of childcare or the fear of losing custody of children whilst in treatment (CoE, 2022; El-Bassel & Strathdee, 2015; INCB, 2016).
WWUD face a range of negative health consequences. The convergence of risky injecting practices (e.g. using contaminated injecting equipment, using the needle after her partner) and high-risk sexual activity (transactional sex) creates a substantial risk for human immune deficiency virus (HIV), sexually transmitted infections (STI) and viral hepatitis transmission (Dugan et al., 2021; El-Bassel & Strathdee, 2015; Iversen et al., 2015; UNODC, 2017, 2022). In particular, women who inject drugs and who engage in sex work and women living in prison are more likely than other women to be living with HIV (UNODC/UN Women/WHO/INPUD, 2014; UNAIDS, 2019a, 2021). Many WWUD have a male sexual partner who also injects drugs, which hampers efforts to seek help (El-Bassel et al., 2014).
In many contexts, WWUD remain a particularly hard-to-reach population, even where harm reduction programmes are in place (El-Bassel & Strathdee, 2015). For example, there is limited understanding of the situation of WWUD in the Middle East and North Africa (MENA). This is due to cultural stigma; low engagement of women in treatment and harm reduction services; and access difficulties for research purposes. In order to respond to this gap in the MENA, we report here from Egypt.
Egypt: Drug Profile and Related Health Consequences
Whilst Egypt is classed as a transit country for drugs, it continues to experience an increasing drug problem creating significant social and health problems. Common drugs include cannabis (or hashish), pharmaceutical opioids (mostly tramadol), amphetamine-type stimulants (ATS), heroin and various synthetic cannabinoids (‘Voodoo’, ‘Strox’) (El-Kouny, 2015; El-Masry & Abdelkader, 2021; Hussien et al., 2021; MENAHRA, 2021; UNODC, 2005). Recreational substance use among male youth and university students is common (Khafagy et al., 2021; Naguib et al., 2021; Rabie et al., 2020; Shaheen et al., 2021). Levels of drug use disorder, particularly of tramadol, heroin and cannabis, have risen steeply in recent years in Egypt (Balha et al., 2021; Mneimneh, 2018). The latest size estimate of people who inject drugs is 90,809 (71,485–119,633) (Mahmud et al., 2020).
Of significant concern is that Egypt has the fastest-growing HIV epidemic in the Middle East and North Africa, with evidence of a growing HIV and hepatitis C rates among people who inject drugs (Mumtaz et al., 2014; UNODC, 2015). In 2020, the Ministry of Health and Population (MOHP) ministerial decree was issued to adopt the use of opioid agonist treatment (OAT) as one of the harm reduction interventions and addiction treatment approaches in Egypt (UNODC, 2022b). Harm reduction is explicitly referred to in the Egypt National HIV Strategic Plan 2021–2025, with people who inject drugs identified as a target group for HIV prevention. Several non-governmental organizations (NGO) are providing condom promotion; HIV voluntary testing and counselling (HIV-VCT); and needle and syringe programmes (NSP) in large cities (MENAHRA, 2021; MOHP, 2015). Latest UNAIDS data from 2015 estimates use of sterile injecting equipment at last injection was 31.5% (UNAIDS, 2019b).
WWUD in Egypt
The National Drug Observatory documented 282 women were in treatment in 2021 (NDO, 2021). A prevalence rate of 68.44% was documented for heroin as the most popular substance, followed by tramadol (30.85%) and cannabis (28.72%) (NDO, 2021). A minority used Strox (4%) and pregabalin (5%). In terms of fully understanding their needs, few studies explicitly focus on women. Bio-behavioural surveillance and research studies on injecting drug use in Egypt have excluded women due to their small numbers, or have restricted recruitment to street girls and female sex workers due to difficulties in reaching WWUD (Anwar et al., 2022; MOHP, 2010). WWUD in Egypt are especially vulnerable to acquisition of HIV, hepatitis C and STIs via sexual transmission with partners who are engaged in high-risk sexual activity and to a lesser extent injection drug use (Khattab, 2007, 2010; Khattab & El–Geneidy, 2014; Oraby, 2013; Oraby & Abdel-Tawab, 2016). Several clinical studies have reported on the strong association between female substance use, adverse childhood experiences, mental health issues and exposure to violence (El-Sawy et al., 2010; Yousef et al., 2022).
There have been some efforts to identify, document and respond to the needs of WWUD in Egypt. MENAHRA (2013) reported on their hidden nature, particularly those who inject and the substantial traumas, stigma and challenges experienced by WWUD in Egyptian society. The 15-year evaluation of MedNET network of the Council of Europe Pompidou Group noted the lack of willingness among Egyptian women to declare their drug problem and access treatment, the lack of specialized addiction services for them, the restriction of community based services to males and the lack of in-depth research on these women (Van Hout, 2021). In response, MedNET assessed the need for gender-responsive services for women in Egypt (Sabry, 2016) and, in cooperation with government, supported the development of several specialized addiction clinics for women (including pregnant women) (Van Hout, 2021).
We conducted a recent multi-stakeholder rapid situation assessment (RSA) which aimed to investigate gendered and contextual vulnerabilities and service level responsiveness to the needs of women who use drugs (WWUD) in Egypt. The ultimate aim of the RSA was to respond to the gap in the evidence base and to develop a more comprehensive picture of WWUD in Egypt in order to refine a gender-responsive national strategy for WWUD and inform the further development of gender-responsive and gender-transformative evidence-based harm reduction and treatment services.
Methods
Research Design
RSA are useful in producing ‘real time’ accurate, contextually rich evaluations and identifying actionable information in short timeframes, especially pertinent when assessing organizational aspects of public health and healthcare in development or humanitarian contexts (Annett & Rifkin, 1995; Chambers, 1994; Cifuentes et al., 2006; Green et al., 2015; Holdsworth et al., 2020; McMullen et al., 2011; Palinkas & Zatzick, 2019; Phillips et al., 2014).
The RSA adopted a multi-level approach by scrutinizing three levels of determinants potentially impacting on future policy and service development and coverage for WWUD: the individual women and their drug using networks; their surroundings comprising family members, addiction treatment and harm reduction staff, police etc.); and the policy and service level environments. The assessment design adhered to the core features of RSA in terms of using mixed methods to assess the situation of WWUD in Egypt; operating under a strict rapid timeline of 6 weeks; and using a multi-pronged team approach of government officials, UN agencies and academics to collect and analyse multiple sources of data in an iterative cycle, with participation of active and former WWUD (McMullen et al., 2011; McNall & Foster-Fishman, 2007). Specific objectives included retrieval of current information on WWUD in terms of female drug use trends; levels of awareness around risks and harms; settings and motives for use; addiction treatment and harm reduction service uptake; level of gender responsiveness in government and community service provision; and impact of HIV and other health harms.
Context
Several governates of Egypt were reached, representing North Egypt (Delta), South Egypt (Upper Egypt), Coast governates and Cairo (the Capital and largest city). Whilst the data collection focused largely on urban areas, the RSA included attention on rural aspects of drug use (including injecting) and accessing of services by women and, where possible, probed into the experiences of WWUD who had been in prison (El Kanater) (see Tables 1 and 2).
Ethics
Ethical approval was granted by the National AIDS Programme and the General Secretariat of Mental Health and Addiction Treatment, Egypt. Written and verbal informed consent was obtained from each participant. All were assured of anonymity and confidentiality and participated voluntarily with the ability to withdraw at any stage.
Procedures
A mixed method approach consisted of the National Drug Observatory data, interviews with professional key informants and focus groups with WWUD in various clinical and community harm reduction settings across Egypt. Qualitative guides were based on an in-depth review of literature and multi-disciplinary team consultation. The RSA was conducted in the period April to June 2022 and consisted of three complimentary phases:
2022 National Drug Observatory Profile: Female Treatment Characteristics
An updated profile of female service user characteristics reflecting the first two quarters of 2022 was sought via mapping of addiction services in the National Drug Observatory system (in-/out-patient government clinics, private hospital and clinic settings and non-governmental organizations providing harm reduction) at the General Secretariat of Mental Health and Addiction Treatment (NDO-GSMHAT). The routine NDO reporting sheet was circulated to all in-/out-patient government clinics, private hospitals and harm reduction NGO.
Multi-stakeholder Professional Key Informant Interviews
In-depth interviews were conducted during site visits with a purposive sample of professionals involved in drug use disorder treatment, community harm reduction NGO or representing UN agencies (n = 21) (hereafter ‘key informant’). Six females and seven males were interviewed in the government cohort, consisting of experienced nursing specialists, psychiatrists and addiction counsellors. Two addiction counsellors were former users. Six women and two males were interviewed representing UN agencies and community harm reduction NGO (see Table 1).
Interviews explored the specific needs of WWUD relating to drug use; mental health and co-morbidities; WWUD awareness of harm reduction and addiction support services; factors motivating help-seeking and female-specific barriers to intake, retention and engagement in treatment; harm reduction and rehabilitation; and the identified needs of WWUD for enhanced gender-sensitive services in Egypt, spanning hospital and community settings, where possible prison settings were included.
Focus Group Discussions with WWUD
Small focus groups of 3–7 women were conducted with a convenience sample of WWUD in treatment, or accessing HIV-VCT and community harm reduction NGO (n = 75) (see Table 2).
Focus group discussions explored contextual aspects of female vulnerability to drug use; their drug use trajectories and pathways toward high-risk use and drug use disorder; experiences of trauma, mental health and co-morbidities; WWUD awareness and factors motivating help-seeking; and gendered barriers to treatment and specific gaps to inform development of future gender-responsive and gender-transformative evidence-based services.
Data Analysis and Triangulation
Data collection, analysis and triangulation across methods and sources were conducted concurrently. Interview and focus group transcripts were translated into English using back translation for consistency. Qualitative data was then coded using QSR NUD*IST 4 software. Thematic analysis was conducted and adhered to six steps to ensure scientific rigor (Braun et al., 2019): (1) familiarization with the data by reading and re-reading the text, individually (author one) and in pairs (authors two and three), to share and identify early ideas; (2) generating initial codes by development of coding schemes and the systematic coding of data; (3) generating themes using an iterative process to organize codes into groups in developing themes and subthemes; (4) reviewing potential themes via team refinement (all authors) and review of generated themes as a collective and with examination of coherence of patterns across themes; (5) defining and naming themes finalization and naming of themes; and (6) writing up by organizing the final order of themes (see Byrne, 2022).
Eight themes emerged: profile of WWUD; access to drugs and settings for female drug use; dimensions of stigma; trauma and drivers of female drug use; networks and intimate partner relationships; high-risk behaviours and harms; barriers to help-seeking and accessing services; and enhancing gender-responsive and gender-transformative evidence-based services. Each theme is presented with illustrative participant quotes.
Results
Profile of WWUD
Key informants employed in government services observed that women accessing treatment in Egypt are generally from urban areas and are of lower socio-economic status, often middle aged, unmarried/divorced with children. Representatives of UN agencies and community harm reduction NGOs observed similar patterns. This trend was also reflected in the women participating in the focus groups.
According to the NDO-GSMHAT during the first half of 2022, 142 women were in treatment, representing 2% of the treatment population. The most significant proportion was aged 26–30 years (25.40%), followed by 21–25 years (19.7%) and 36–40 years (16.20%). Very few were aged over 46 years. Injection drug use was reported by 9.9%, with no NDO reported cases of needle sharing. Prevalence of heroin (54.9%), hashish (18.3%) and tramadol (14.8%) use by women had all reduced compared to the 2021 NDO report. The use of Strox remained relatively stable at 4.2% (see Table 3).
Similar trends were reported by key informants and WWUD themselves who reported that most common drugs used by women in Egypt are heroin, tramadol, hash, cannabis, synthetic cannabis and cocaine. There were some reports by WWUD of progression toward iatrogenic dependence on opioids for menstruation pain management, with subsequent displacement to injection of heroin.
Key informants across government treatment and community harm reduction sectors all observed drug consumption by women to occur primarily through inhalation and swallowing of tablets/powders. They observed that the proportion of women injecting drugs was low compared to women using tablets or inhaling drugs for recreational purposes. There was one report by an NGO key informant about tropicamide (Mydrapid) injecting. Most reported that WWUD in Egypt do not reach the drug dependence levels attained by men.
Access to Drugs and Settings for Female Drug Use
Women in focus groups described various settings for the use of drugs generally in the home, particularly regarding injection of drugs with husbands, partners including sex work clients, friends and siblings (often brothers), and also on the street. All key informants observed similar settings, and that use of drugs by women was rarely alone. For example, an NGO key informant in Alexandria said: ‘They use drugs when their partner or someone in the family is using drugs or when working as sex worker’. In Upper Egypt, an NGO key informant illustrated the varied contextual pathways toward drug use among women: ‘The conditions of drug abuse differ among women, some went to drugs due to problems, some engaged in sex work and the clients made them use drugs. They inject drugs with clients or friends’.
At an NGO in Upper Egypt, several women in focus groups reported that close family relatives introduced them to drugs in order to relieve emotional distress and trauma due to domestic violence and aborted pregnancies. One woman accessing an NGO in Upper Egypt commented: ‘My stepfather was molesting me and made me take drugs with him and then my mother saw us together in an unpleasant situation and she kicked me out’. Access to drugs was viewed as easy via peers and user networks. Several women in Greater Cairo and in Upper Egypt (respectively) said: ‘I had the drugs delivered to my doorstep’ and ‘Someone taught me to use drugs since it was free, although I knew it was wrong’.
Dimensions of Stigma
Cultural norms and values in the conservative Egyptian society were described by the majority of key informants as heightening stigma of drug use among women and subsequent experiences of discrimination, isolation and marginalization. Government-level key informants also repeatedly mentioned the lack of awareness of families around the harms of drug use and where to seek treatment, for example: ‘The culture of the society is stigmatizing addiction in females. Lack of awareness in their families is hindering their access to treatment’. Perceptions of individual, familial and community stigma and gender discrimination were also pervasive in the narratives of many women consulted across hospital, HIV-VCT and NGO settings, who said:
Nobody in my family wants to deal with me. (HIV-VCT Centre: Delta)
People always stigmatize me. (HIV-VCT Centre: Suez Canal)
For women, being divorced in our community is stigmatizing just like using drugs. (Psychiatric hospital: Cairo)
The community is unfair and racist as it differentiates between men and women in everything, so in terms of drug abuse, it might be accepted for men to use cannabis - while it’s not acceptable for women, even if the reasons for the use are the same. (Psychiatric hospital: Cairo)
All key informants described how substantial levels of self-perceived, familial and community-level stigma of WWUD result in discriminatory experiences, feelings of hopelessness and poor mental health and hinder their attempts to enter treatment and receive support. A government treatment professional said: ‘Sometimes these feelings are motivating them [to use drugs], and sometimes they feel hopeless, and no one can help so they don’t seek treatment or support’. This was also especially evident in the narratives from professionals working in NGOs who said:
They always have shame, blame, depression, self-stigma and this is what keeps them from seeking help. (NGO: Alexandria)
The stigma and discrimination from society towards women who use drugs prevents them from requesting health services and health support. (NGO: Upper Egypt)
Various dimensions of stigma were observed relevant to the WWUD. For example, stigma is particularly exacerbated, if the woman is living with HIV, injecting drugs and engaging in commercial sex work. A UN agency key informant said: ‘Triple stigma (Women who inject drugs/ living with HIV /sex worker)’. In Greater Cairo, a woman accessing an NGO described drug user network level stigma regarding type of drug used: ‘Stigma between users themselves according to the type of drug the woman is using’. Government staff also felt the stigma of those working in the field of female addiction; for example, one key informant commented: ‘As service providers in the field of addiction treatment in general and the field of WWUD in particular, we are facing a stigma that is never less than the stigma of patients themselves’.
Trauma and Drivers of Female Drug Use
A broad range of motives for the use of drugs were illustrated by the women consulted. This included self-medication for physical and menstrual pain; the self-medication of symptoms of psychological stress (anxiety, depression and insomnia) due to marital stress, inter-familial addiction and bereavement (including of children); and for recreational intoxication purposes, due to boredom and for the enhancement of sexual activity. For example, two women described their experiences and said:
I faced a great shock when I lost my son. He was 22 years old and died, my husband was taking drugs and I tried with him to pass my mental suffering (NGO: Alexandria)
I was depressed and sad since my husband got prisoned for 5 years. When he got out, he left me. (HIV- VCT Centre: Upper Egypt)
Many women across the hospital, HIV-VCT and NGO settings experienced substantial trauma and discrimination and voiced their fears about being a poor role model and fears around loss of custody of their children. Several WWUD in Cairo illustrated their experiences and said:
My son used to see me smoking hash, he is 13 years old and now he has started smoking hash with his friends, I do not want him to be an addict. I am blaming myself for being a bad role model for my son. (Psychiatric hospital)
The community and my neighbours stigmatized me, and they began to curse my children… so I wanted to stop using drugs for them (NGO)
Very few women reported contact with the criminal justice system. At a HIV-VCT centre in Suez Canal, several women described their awareness of how WWUD are humiliated in prisons.
Networks and Intimate Partner Relationships
Key informants all observed that intimate partner relationships; membership of an existing network of people who use drugs; and clients of sex work support continued drug use by women and hinder their efforts to seek help. This was especially the case where husbands had introduced wives to drug use, injecting of drugs and co-dependencies had developed over time, as observed by NGO’s in Cairo and government-level professionals who said:
Their sexual partners prevent them from seeking help or seeking harm reduction tools. (NGO: Cairo)
Most cases I witnessed started using with the husband, which makes it difficult for them to seek treatment or even maintain their abstinence unless the husband is also seeking treatment. (Government)
Several women at psychiatric hospitals and NGOs in both Cairo and Upper Egypt reported using and injecting drugs with and often under coercion from their husband (generally heroin). Many reported marital difficulties, use of drugs during sexual relations and exposure to intimate partner violence. A woman accessing a HIV-VCT centre in Upper Egypt reflected: ‘My fiancé made me try it a couple of times, then I became addicted’.
High-Risk Behaviours and Harms
The hidden nature of female drug use was observed by all key informants to exacerbate high-risk activity. High-risk experiences included unwanted sexual relationships, multiple sex partners, commercial and transactional sex work, exploitation, kidnapping, unwanted pregnancies and unsafe injecting practices. Additional risks included crimes of poverty (for example, stealing, drug dealing). Two women illustrated their experiences of coercion and said:
My family always forces me to do things I don’t want to. That’s why I started taking drugs. (NGO: Greater Cairo)
My partner negotiates with me to have sexual relations in return for drugs or money for drugs. (HIV- VCT Centre: Delta)
Elevated risk behaviours such as sharing of injecting equipment and having unprotected sex were observed to hamper efforts to seek help and enter treatment. NGO key informants working in the community observed:
If she still practices those risky behaviours, she wouldn’t seek treatment. (NGO: Cairo)
Dangerous practices and unprotected sex affect women’s exposure to transmitted diseases, and when becoming an infected person, things get complicated and put women in a state of refusal of services. (NGO: Upper Egypt)
A minority of women reported experience of injecting drugs in focus groups at a HIV-VCT centre and NGO in Upper Egypt, generally to save money. Several reported using the same needle twice, particularly when pharmacies did not provide clean syringes. A woman accessing an NGO in Upper Egypt said: ‘When I can’t get a clean one from the pharmacy and I can’t wait to get a clean syringe’. At a HIV-VCT centre in Delta, one woman described how she used to share with her sister but then her sister was diagnosed with HIV (via sexual transmission by her husband), and so she stopped sharing. She then shared with her husband and became infected with HIV. One woman at an NGO in Cairo described sharing needles in prison. A woman accessing an NGO in Upper Egypt said: ‘I am afraid to go back to jail I got infected with HIV’.
Across the sample of women consulted, there was some awareness and experience of overdose, both personally and that of peers and husbands (in Cairo and in Upper Egypt). A woman accessing a HIV-VCT centre in Upper Egypt said: ‘A couple of times I overdosed and was rushed to the hospital, and they saved me’. There were some reports of thoughts to overdose intentionally. Many women described their fears; for example, one woman accessing an NGO in Upper Egypt said: ‘I could get into jail again. I could die alone, my dealer may take advantage of me, my family could reach me and kill me’.
Harm reduction principles and practices were observed to be not widely known in drug using networks, due to cultural sensitivities. Low-level awareness of harm reduction services was reported by the women, with most not knowing anything about harm reduction. A woman in the psychiatric hospital in Cairo said: ‘These strategies won’t be applicable in our society’. However, many women reported attempts to reduce harm and more serious forms of drug use, by tapering, replacing with over the counter medications and switching from injection to insufflation. Several said:
I tried quitting drugs using analgesics and it worked. (HIV- VCT Centre: Upper Egypt)
I tried powder inhalation [sniffing] with my first husband and tried injections with my friend after marital problems, but I got really sick so I went back to inhalations. (HIV- VCT Centre: Upper Egypt)
To reduce the harm of using, I can change the way I use heroin, to be sniffing instead of injection. (Psychiatric hospital: Upper Egypt)
Displacement between heroin, tramadol and hash was described by several women. A woman in the psychiatric hospital in Cairo said: ‘Harm reduction as I know it is gradually reducing my intake dose. I am reducing harm by using hash instead of Tramadol’.
Barriers to Help-Seeking and Accessing Support Services
All key informants reported that government and community harm reduction services are provided using a ‘gender neutral’ approach. Having mixed services for men and women and the location of centres was seen as discouraging to women seeking help. Geographic coverage across the country was observed to be inadequate, where centres were not available in all governates. For example, a key informant from an NGO in Upper Egypt said: ‘We have an increasing number of injecting drug users, but there are difficulties in reaching them, especially in Upper Egypt’. NGO key informants observed referral to treatment to occur mainly via the ‘inner circle’ of partners, family and friends. Self-referral and via outreach were also described. NGOs in particular were deemed to be a vital and trusted lifeline for engaging with WWUD and encouraging help-seeking. Various comments included:
The most important point is getting help from people around her and the community, either from family or work. The role of civil society and the AIDS program is also very important (UN Agency)
Secrecy, Trust, Safety. What influences the women is the services provided by the NGO without any stigma or discrimination. (NGO: Greater Cairo)
Barriers to engaging with services and reluctance to seek help centred on fears of losing custody of children and exposure to gender-based violence (including intimate partner violence) in the home. Some NGO key informants mentioned fears of WWUD around loss of confidentiality and how parental consent for HIV testing in minors represented a specific barrier to service uptake. Various triggers to initiate help-seeking and enter treatment were described by the women consulted. They included pregnancy, mental health conditions including drug-related psychosis, fear of contracting blood-borne viruses, fear of divorce, losing child custody and death:
I am so afraid of death, and I don’t want to do anything wrong or bad. (HIV- VCT Centre: Upper Egypt)
Don’t want to continue my life as a bad person anymore. (Psychiatric hospital: Cairo)
I want to get clean for my children. (HIV-VCT Centre: Delta)
Some women engaging with harm reduction NGOs were afraid to enter treatment and change their behaviours. For example, a woman accessing an NGO in Alexandria illustrated her fears: ‘I don’t want to go to rehabilitation centre or to be treated, I don’t want to face my real life’. In contrast, many women receiving treatment voiced that they were tired of addiction. A woman in Upper Egypt commented: ‘…. feeling like I am not a whole human being but just broken pieces’.
All women consulted described their experiences in seeking help for their drug use, with pathways toward treatment hampered by a lack of awareness about available drug detoxification and treatment modalities, a lack of awareness of harm reduction practices and services, a lack of specialized clinics for women and a lack of services for them in some governorates outside of Cairo (for example Asiut, Port Saied). Examples included:
Most of my user friends were not aware of available services for the treatment of addiction for women. (Psychiatric hospital: Cairo)
I come to the hospital with my brother who is mentally ill, and I used this opportunity to try treatment for my addiction problem. (Psychiatric hospital: Upper Egypt)
There was little awareness of the provision of treatment in prison. Two women reported denial of drug use disorder treatment in prison.
Enhancing Gender-Responsive, -Transformative and Evidence-Based Services
Key informants all observed the existing concentration of services in the Cairo and Delta governorates, mainly in big cities. Government-level key informants observed the need to address the lack of centres in some governates (mainly the Upper Egypt governorates (Assiut, Aswan, Qena) and some Delta governorates (Sharqeya, Gharbia)), the lack of trained staff, the lack of specialist centres for women and the lack of social integration initiatives for women within rehabilitation and aftercare. A UN agency key informant outlined this: ‘They do not have to be for women, but they should be separated from the places of service for men but combined with other female health services’.
Many women consulted remarked on the need for treatment services to adopt a more accepting approach for those seeking help. For example, a woman accessing an NGO in Cairo said: ‘Be more flexible in accepting people. I got rejected from treatment facility since my ID was expired from 1 month only’. They voiced concerns about privacy and confidentiality of treatment and highlighted their wishes to undergo treatment and individual counselling in preference to group therapy. Examples included:
I am afraid of my husband’s reaction if he finds out about my addiction problem. (Psychiatric hospital: Upper Egypt)
I am afraid of the idea of group therapy. As our society is small, it may happen that a neighbour of my husband’s family is attending the group session or a relative of one of my husband’s colleagues at work. (Psychiatric hospital: Upper Egypt)
I find it difficult to talk about what concerns me in a group, I prefer individual sessions (Psychiatric hospital: Upper Egypt)
All women with caregiving responsibilities voiced the importance of care of children whilst in treatment and recovering. A woman in treatment in Upper Egypt said: ‘We need home care of young children and day care for children of women in the treatment programme’. Most women were concerned around the general attitudes of healthcare providers toward them. At an NGO in Greater Cairo, two women illustrated discriminatory experiences by medical professionals:
My doctor didn’t want to operate on me and even though I couldn’t stop using alcohol.
Doctor refused to deliver me while I was using drugs at the same time.
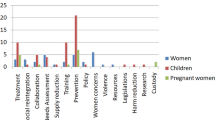
A range of suggestions to achieve an enhanced, appropriate and credible response to the needs of WWUD were documented. Many participants recommended to scale up and intensify efforts to sensitize and reduce stigma and discrimination against WWUD. Others recommended investment in more government places for free services, the location of services in women’s health units and primary care to reduce stigma, and creating more specialized units for women and for minors. Offering a distinct service for women inclusive of HIV-VCT and STI screening, separated from male facilities and integrated into existing women’s health services was advised. An NGO key informant in Cairo suggested: ‘Women only services at least for the first period since they may have been subjected to rape or violence from men so they may not be encouraged to deal with men at this time’. Components of this ‘wrap around’ support were advised to include special trainings for WWUD on safe injection, refusal skills and combating violence, counselling for trauma and gender-based violence, legal supports and community packages (day care/transportation fees for low-income level women, childcare), family support and sustainable livelihoods for when in aftercare.
All recognized the value of trusted NGOs operating in the community, and many indicated that a more strengthened and visible role by NGOs could support female outreach and raise awareness of available drug treatment and harm reduction services and practices, harm reduction uptake and retention and progression toward treatment. All observed the need for staff capacity building and the presence of specialized female staff for operating gender-sensitive and trauma-informed treatment to support a confidential and professional approach. An NGO key informant in Alexandria said: ‘I think that women who use drugs need special services directed toward them, such as “fieldwork teams made up of women”’.
Discussion
The RSA contributes to the small evidence base on WWUD in the MENA. Strengths of the RSA centre on its geographic coverage and sample size inclusive of the voices of those providing and receiving drug treatment and harm reduction services in Egypt. Limitations centre on its rapid nature, with data collection confined to a short timeframe in 2022, with not all governates reached.
It is however encouraging to see that the RSA illustrates progress in responding to the needs of WWUD achieved to date by the Egyptian government and the network of NGOs serving the community. Findings from diverse multi-stakeholder perspectives across Egypt underscore the need to continue to prioritize women in harm reduction and treatment service configurations and geographic coverage, with a particular emphasis on stigma reduction, specialist gender-responsive care and integration of evidence-based drug use disorder treatment for women into primary care and sexual and reproductive health units. The profile of WWUD consulted aligns with the current evidence base (MENAHRA, 2021) and NDO-GSMHAT reporting, which indicates that whilst WWUD are a very small population of people who use drugs, most women in treatment are aged between 25 and 40 years. Notably, many women consulted in this RSA had completed university-level education. Female drugs of choice reflect general trends in Egypt (heroin, tramadol, hashish, synthetic cannabinoids) (Balha et al., 2021; El-Masry & Abdelkader, 2021; Hussien et al., 2021; NDO, 2021).
Low levels of harm reduction awareness and overdose reports, both personal and that of peers, are of concern. Narratives of the WWUD revealed low levels of needle sharing but with some reusing of needles (including in prisons), with reports of self-tapering or switching to self-perceived less harmful forms of drug use. Pharmacies do not provide sufficient clean needles when requested. This occurs even though people who use drugs are identified as a target group for HIV. Whilst most recent UNAIDS (2019b) data on Egypt estimates the use of sterile injecting equipment at last injection at 31.5%, it is recommended to achieve more current surveillance on this public health issue, particularly in hidden groups of WWUD and in prisons. It is encouraging that the National AIDS Programme will conduct the Population Size Estimate and Integrated Bio-Behavioural Surveillance Surveys in mid-2023.
Substantial stigma and discrimination is experienced by WWUD, fuelling hidden and harmful forms of drug use. The disproportionate effects of stigma, discrimination, drug-related health issues (including psychiatric co-morbidities and blood-borne virus acquisition) and negative familial and social impacts of drug use (bereavement, incarceration, loss of child custody, divorce), which are navigated by WWUD in Egypt, are evident. Low help-seeking and uptake of women’s treatment services is likely due to the significant cultural stigma of female addiction in Egypt (Balha et al., 2021; Mohamed et al., 2021). The triple stigmas of being a woman, using drugs and engaging in transactional and coerced sexual activity were observed, compounding their health, fuelling harmful drug use and hindering help-seeking. The association of adverse and traumatic experiences including sexual exploitation and coercion to take drugs by partners, husbands and sex work clients; exposure to inter-personal violence; mental health issues; and poverty is also observed in other Egyptian studies (El-Sawy et al., 2010; Khattab, 2007, 2010; Khattab & El-Geneidy, 2014; Oraby, 2013; Yousef et al., 2022).
Evidence and recommendations generated here are intended to build on progress to date (MENAHRA, 2013; Sabry, 2016; UNODC, 2022) and support the further development of a culturally sensitive scaled-up and sustainable gender-responsive approach to drug use disorder treatment and harm reduction coverage in Egypt. A trauma-informed and trauma-responsive approach provided by specialized female staff is also an imperative given the vulnerabilities and prior exposure to many forms of violence of WWUD in Egypt. Findings are likely to be useful to other MENA countries. Table 4 illustrates a series of guiding principles for multi-stakeholder consideration and action planning.
Conclusion
The RSA contributes to the limited evidence based on WWUD in the MENA region. Further development and scale-up of gender-responsive, gender-transformative and evidence-based drug treatment and rehabilitation services in Egypt which address their unique needs and challenges are warranted. Key components for the Egyptian government to incorporate in future activities centre on boosting service level coverage and providing non-judgemental supportive and safe environments cognizant of healthy connections with children, family and the community (CoE, 2022). Capacity building within organizations (government and NGO) and working groups is crucial to support gender mainstreaming (WHO, 2011).
With regard to women in conflict with the law, access to evidence-based drug disorder treatment in the community is important as part of non-custodial sentencing (UNODC/WHO, 2020). Detention facilities are advised to acknowledge the gender-sensitive needs of women and uphold the rights of WWUD to access non-discriminatory equivalence of care (UN General Assembly, 2010, 2016).
Finally, gender-oriented programmes or services require sufficient monitoring and evaluation. It is recommended to routinely use the UNODC checklist to assess the implementation of gender mainstreaming within programming to assess and plan progress and to review existing strategy or policy documents (UNODC, 2021). Continued bio-behavioural research to support public health surveillance in Egypt and guide implementation of evidence-based interventions to respond in a culturally sensitive and effective manner to gender-based violence, trauma, drug use disorders and co-morbidities on the health and human rights of WWUD is warranted (UNODC, 2017).
References
Agterberg, S., Schubert, N., Overington, L., & Corace, K. (2020). Treatment barriers among individuals with co-occurring substance use and mental health problems: Examining gender differences. Journal of Substance Abuse Treatment, 112, 29–35.
Annett, H., & Rifkin, S.N. (1995). Guidelines for rapid participatory appraisals to assess community health needs. World Health Organization (WHO): Geneva. Available at: http://apps.who.int/iris/bitstRAP/handle/10665/59366/WHO_SHS_DHS_95.8.pdf?sequence=1&isAllowed=y (Accessed 21 May 2023).
Anwar, S., El Kharrat, E., Bakhoum, A., El-Sadr, W. M., & Harris, T. G. (2022). Association of sociodemographic factors with needle sharing and number of sex partners among people who inject drugs in Egypt. Global Public Health, 17(8), 1689–1698.
Balha, S. M., Abo-Baker, O., & Mahmoud, S. (2021). Assessment of psychological symptoms and cravings among patients with substance related disorders. Egyptian Journal of Health Care, 2(3), 751–763.
Braun, V., Clarke, V., Hayfield, N., & Terry, G. (2019). Thematic analysis. In, Liampiuttong, P (eds) Handbook of research methods in health social sciences. 843–860.
Byrne, D. (2022). A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Quality and Quantity, 56, 1391–1412.
Chambers, R. (1994). The origins and practice of participatory rural appraisal. World Development, 22, 953–969.
Cifuentes, E., Alamo, U., Kendall, T., Brunkard, J., & Scrimshaw, S. (2006). Rapid assessment procedures in environmental sanitation research: A case study from the norther border of Mexico. Canadian Journal of Public Health, 97(1), 24–28.
CoE (2022). Implementing a gender approach in different drug policy areas: From prevention, care and treatment services to law enforcement & the criminal justice system. Council of Europe (CoE) Pompidou Group: Strasbourg. Available at: https://rm.coe.int/2022-ppg-implementing-a-gender-approach-in-drug-policies-a-pg-handbook/1680a66835 (Accessed 19 May 2023).
Dugan, E., Blach, S., Biondi, M., Cai, Z., DePaola, M., Estes, C., Feld, J., Gamkrelidze, I., Kottilil, S., Ma, S., Mathur, P., Montoya, S., Razavi-Shearer, D., Razavi-Shearer, K., Robbins-Scott, S., Schmelzer, J., & Razavi, H. (2021). Global prevalence of hepatitis C virus in women of childbearing age in 2019: A modelling study. Lancet Gastroenterology & Hepatology, 6(3), 169–184.
El-Bassel, N., Shaw, S. A., Dasgupta, A., & Strathdee, S. A. (2014). People who inject drugs in intimate relationships: It takes two to combat HIV. Current HIV/AIDS Reports, 11(1), 45–51.
El-Bassel N., & Strathdee SA. (2015). Women who use or inject drugs: An action agenda for women-specific, multilevel, and combination HIV prevention and research. Journal of Acquired Immune Deficiency Syndromes 69 Suppl 2(Suppl 2):S182–90.
El-Kouny, N. (2015). Outcast: Egypt’s growing addiction problem. Ahramonline. Available at: https://english.ahram.org.eg/NewsContent/1/151/133715/Egypt/Features/Outcast-Egypts-growing-addiction-problem-.aspx. (Accessed 19 May 2023).
El-Masry, M., & Abdelkader, S. I. (2021). Clinical profile of designer drug “Strox” intoxicated cases presented to Poison control center Ain Shams University, Egypt from first of January 2017 to end of January 2018. Ain Shams Journal of Forensic Medicine and Clinical Toxicology, 36, 98–105.
El-Sawy, H., Hay, M. A., & Badawy, A. (2010). Gender differences in risks and pattern of drug abuse in Egypt. Egyptian Journal of Neurology, Psychiatry and Neurosurgery, 47(3), 413–418.
EMCDDA. (2017). Women who use drugs: Issues, needs, responses, challenges and implications for policy and practice. Background paper commissioned by the EMCDDA for Health and social responses to drug problems: A European guide. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA):Lisbon. Available at: www.emcdda.europa.eu/document-library/women-who-use-drugs-issues-needs-responses-challenges-and-implications-policy-and-practice_en (Accessed 19 May 2023).
EMCDDA. (2023). Women and drugs: Health and social responses. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA):Lisbon. Available at: www.emcdda.europa.eu/publications/mini-guides/women-and-drugs-health-and-social-responses_en (Accessed 19 May 2023)
Green, C. A., Duan, N., Gibbons, R. D., Hoagwood, K. E., Palinkas, L. A., & Wisdom, J. P. (2015). Approaches to mixed methods dissemination and implementation research: Methods, strengths, caveats, and opportunities. Administration and Policy in Mental Health and Mental Health Services, 42, 508–523.
Greenfield, S. F., Brooks, A. J., Gordon, S. M., Green, C. A., Kropp, F., McHugh, R. K., Lincoln, M., Hien, D., & Miele, G. M. (2007). Substance abuse treatment entry, retention, and outcome in women: A review of the literature. Drug & Alcohol Dependence, 86(1), 1–21.
Harrop, E. N., & Marlatt, G. A. (2010). The comorbidity of substance use disorders and eating disorders in women: Prevalence, etiology, and treatment. Addictive Behaviors, 35(5), 392–398.
Holdsworth, L. M., Safaeinili, N., Winget, M., Lorenz, K. A., Lough, M., Asch, S., & Malcolm, E. (2020). Adapting rapid assessment procedures for implementation research using a team-based approach to analysis: A case example of patient quality and safety interventions in the ICU. Implementation Science, 15(1), 12.
Hussien, R., El-Setouhy, M., Shinawi, M. E., El-Hariri, H. M., & Hirshon, J. M. (2021). Acute Toxic Effects of the New Psychoactive Substance “Voodoo” among Patients presented to the Poison Control Center of Ain Shams University Hospitals (PCC-ASUH), Egypt, during 2017. Substance Abuse Treatment, Prevention, and Policy, 16(1), 71.
INCB (2016). Report of the International Narcotics Control Board for 2016. International Narcotics Control Board (INCB): Vienna. (E/INCB/2016/1). Available at: www.drugsandalcohol.ie/26947/1/International_Narcotics_Control_Board%20-2016.pdf (Accessed 9 Sept 2023).
Iversen, J., Page, K., Madden, A., & Maher, L. (2015). HIV, HCV and health-related harms among women who inject drugs: Implications for prevention and treatment. Journal of Acquired Immune Deficiency Syndrome (1999), 69(0 1), S176–S181.
Khafagy, M., Gomaa, Z., & Elwasify, M. (2021). Substance use patterns among university students in Egypt. Middle East Current Psychiatry, 28, 59.
Khattab, H. (2007). All alone: The stories of Egyptian women living with HIV, stigma and isolation. Cairo, Egypt: Egyptian Society for Population Studies and Reproductive Health (ESPSRH).
Khattab, H. (2010). The agony of AIDS: A qualitative study of the experience of AIDS in Egypt. Cairo, Egypt: Egyptian Society for Population Studies and Reproductive Health (ESPSRH).
Khattab, H., & El–Geneidy, M. (2014). Living with AIDS: Suffering and courage. Cairo, Egypt: Egyptian Society for Population Studies and Reproductive Health (ESPSRH).
Mahmud, S., Mumtaz, G. R., Chemaitelly, H., Al Kanaani, Z., Kouyoumjian, S. P., Hermez, J. G., & Abu-Raddad, L. J. (2020). The status of hepatitis C virus infection among people who inject drugs in the Middle East and North Africa. Addiction, 115(7), 1244–1262.
McMullen, C. K., Ash, J. S., Sittig, D. F., Bunce, A., Guappone, K., Dykstra, R., Carpenter, J., Richardson, J., & Wright, A. (2011). Rapid assessment of clinical information systems in healthcare setting: An efficient method for time-pressed evaluation. Methods of Information in Medicine, 50(4), 299–307.
McNall, M., & Foster-Fishman, P. G. (2007). Methods of rapid evaluation, assessment, and appraisal. American Journal of Evaluation, 28, 151–168.
MENAHRA. (2013). Women injecting drug users in the MENA. Middle East and North Africa Harm Reduction Association (MENAHRA): Beirut. Available at: www.menahra.org/images/pdf/MENAHRA_OR_Women_Injecting_Drug_Users_2013_.pdf (Accessed 19 May 2023).
MENAHRA. (2021). Assessment of situation and response of drug use and its harms in the Middle East and North Africa 2021. Middle East and North Africa Harm Reduction Association (MENAHRA). Lebanon: Beirut. Available at: 2021 Assessment of Situation (menahra.org) (Accessed 19 May 2023).
Mneimneh, R. (2018).Ten percent of Egypt’s population is addicted to drugs. Available at: https://stepfeed.com/ten-percent-of-egypt-s-population-is-addicted-to-drugs-8667. (Accessed 19 May 2023)
Mohamed, S. F., Mourad, G. M, & El Hamid Zaki, R. A. (2021). Effect of educational program for reducing self stigma and shame among substance abuser women. Ilkogretim Online 20 (5):2278–2288. 11p.
MOHP. (2010). HIV/AIDS Biological & Behavioral Surveillance Survey: Round Two Summary Report, Cairo, Egypt 2010. Ministry of Health and Population, Cairo: Egypt.
MOHP (2015). Egypt Demographic and Health Survey 2014. Cairo and Rockville, MD: Ministry of Health and Population and ICF International. Ministry of Health and Population, Cairo.
Mumtaz, G. R., Weiss, H. A., Thomas, S. L., Riome, S., Setayesh, H., Riedner, G., Semini, I., Tawil, O., Akala, F. A., Wilson, D., & Abu-Raddad, L. J. (2014). HIV among people who inject drugs in the Middle East and North Africa: Systematic review and data synthesis. Plos Medicine, 11(6), e1001663.
Naguib, Y. M., Sherif, H. A., Elbalshy, A. T., Edrees, E. A., Sabry, A. E., Sharif, A. F., Aloshari, S. H. A., & Kasemy, Z. A. (2021). Prevalence and associated risk factors of cannabinoid abuse among Egyptian university students: A cross-sectional study. Environmental Science and Pollution Research, 28(48), 68706–68716.
National Drug Observatory Annual Report (2021). National Drug Observatory Egypt. Cairo: Egypt.
Oraby, D. (2013). Harm reduction approach in Egypt: The insight of injecting drug users. Harm Reduction Journal, 10, 17.
Oraby, D., & Abdel-Tawab, N. (2016). Understanding married women’s vulnerability to HIV infection in Egypt: An exploratory study. Cairo: Population Council.
Palinkas, L. A., & Zatzick, D. (2019). Rapid assessment procedure informed clinical ethnography (RAPICE) in pragmatic clinical trials of mental health services implementation: Methods and applied case study. Administration and Policy in Mental Health and Mental Health Services, 46, 255–270.
Phillips, C. B., Dwan, K., Hepworth, J., Pearce, C., & Hall, S. (2014). Using qualitative mixed methods to study small health care organizations while maximizing trustworthiness and authenticity. BMC Health Services Research, 14, 559.
Rabie, M., Shaker, N. M., Gaber, E., El-Habiby, M., Ismail, D., El-Gaafary, M., Lotfy, A., Sabry, N., Khafagy, W., & Muscat, R. (2020). Prevalence updates of substance use among Egyptian adolescents. Middle East Current Psychiatry, 27, 4.
Sabry, N (2016). Gender Responsive Services for Women with Substance Abuse Disorders in Egypt Council of Europe Pompidou Group, Strasbourg: France. Available at P-PG/Med (2016) 24 (coe.int) (Accessed 9 Sept 2023).
Shaheen, H. M., Amin, S., & Abou Elsoud, S. M. (2021). Substance use disorder and risk behaviors among secondary school adolescents in a rural area in Egypt. Menoufia Medical Journal, 34, 544–549.
Strathdee, S. A., West, B. S., Reed, E., Moazan, B., Azim, T., & Dolan, K. (2015). Substance use and HIV among female sex workers and female prisoners: Risk environments and implications for prevention, treatment and policies. Journal of Acquired Immune Deficiency Syndrome (1999), 69 Suppl 2(0 1), S110-7.
Tripodi, S. J., & Pettus-Davis, C. (2013). Histories of childhood victimization and subsequent mental health problems, substance use, and sexual victimization for a sample of incarcerated women in the US. International Journal of Law and Psychiatry, 36(1), 30–40.
UN General Assembly (2010). United Nations Rules for the Treatment of Women Prisoners and Non-Custodial measures for women offenders (the Bangkok Rules) : note / by the Secretariat, 6 October 2010, A/C.3/65/L.5. Available at: https://www.refworld.org/docid/4dcbb0ae2.html (Accessed 9 Sept 2023).
UN General Assembly (2016). United Nations Standard Minimum Rules for the Treatment of Prisoners (the Nelson Mandela Rules) : resolution / adopted by the General Assembly, 8 January 2016, A/RES/70/175. Available at: https://www.refworld.org/docid/5698a3a44.html (Accessed 9 Sept 2023).
UNAIDS (2019a) Women who inject drugs more likely to be living with HIV. Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva. Available at: www.unaids.org/en/resources/presscentre/featurestories/2019/june/20190611_women-who-inject-drugs. (Accessed 19 May 2023).
UNAIDS. (2019b). UNAIDS Data 2019b. Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva. Available from: https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf (Accessed 19 May 2023).
UNAIDS (2021). Update on HIV in prisons and other closed settings. Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva. Available at: www.unaids.org/sites/default/files/media_asset/PCB49_HIV_Prisons_Closed_Settings_rev1__EN.pdf (Accessed 19 May 2023).
UNODC. (2022b). Terms of Reference. Rapid Situation Assessment (RSA) on women who use and inject drugs in Egypt. Cairo: UNODC Regional Office of the Middle East and North Africa (ROMENA).
UNODC. (2005). Egypt Country Profile. UNODC Regional Office of the Middle East and North Africa (ROMENA): Cairo. Available at: http://www.unodc.org/pdf/egypt/egypt_country_profile.pdf. (Accessed 19 May 2023).
UNODC. (2015). Feasibility study opioid substitution treatment in Egypt. UNODC Regional Office of the Middle East and North Africa (ROMENA): Cairo. Available at: www.unodc.org/documents/middleeastandnorthafrica/drug-prevention-health-publications/OST_Feasibility_Study_in_Egypt.pdf. (Accessed 19 May 2023)
UNODC. (2017). Guidelines on drug prevention and treatment for girls and women. United Nations Office on Drugs and Crime, Vienna. Available at: www.unodc.org/documents/drug-prevention-and-treatment/unodc_2016_drug_prevention_and_treatment_for_girls_and_women_E.pdf (Accessed 21 May 2023).
UNODC (2021). Gender mainstreaming in the work of UNODC. Guidance note for UNODC staff”, United Nations Office on Drugs and Crime, Vienna. Available at: www.unodc.org/documents/Gender/20-04944_Gender_Note_final_ebook_cb.pdf (Accessed 21 May 2023).
UNODC. (2022a). World Drug Report 2022a. United Nations Office on Drugs and Crime (UNODC): Vienna. Available at: www.unodc.org/unodc/en/data-and-analysis/wdr2022.html (Accessed 19 May 2023).
UNODC/UN Women/WHO/INPUD. (2014). Women who inject drugs and HIV: Addressing specific needs. Policy Brief. UNODC/UNW/WHO/INPUD. Available at: www.unodc.org/documents/hiv-aids/publications/WOMEN_POLICY_BRIEF2014.pdf (Accessed 19 May 2023).
UNODC/WHO (2020). International standards for the treatment of drug use disorders. Revised edition incorporating results of field testing. World Health Organization and the United Nations Office on Drugs and Crime. Available at: International standards for the treatment of drug use disorders: revised edition incorporating results of field-testing (who.int) (Accessed 21 May 2023).
Valencia, J., Alvaro-Meca, A., Troya, J., Guerrez, J., Ramon, C., Rodrıguez, A., Vazquez-Moron, S., Resino, S., Moreno, S., & Ryan, P. (2020). Gender-based vulnerability in women who inject drugs in a harm reduction setting. PLoS ONE, 15(3), e0230886-e230889.
Van Hout, M. C. (2021). Evaluation Report of the Impact of 15 years of MedNET. Mediterranean cooperation network on drugs and addictions of the Pompidou Group. Council of Europe, Pompidou Group, Strasbourg: France.
WHO. (2011). Gender mainstreaming for health managers: A practical approach. Facilitators’ guide. World Health Organization, Geneva. Available at: www.who.int/publications/i/item/9789241501057 (Accessed 21 May 2023).
Yousef, A. M., Mohamed, A. E., Eldeeb, S. M., & Mady, R. S. (2022). Prevalence and clinical implication of adverse childhood experiences and their association with substance use disorder among patients with schizophrenia. Egypt Journal of Neurology Psychiatry Neurosurgery, 58, 4.
Funding
The RSA was funded by the UK acting as donor to the United Nations Office on Drugs and Crime Regional Office for the Middle East and North Africa.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics
Ethical approval was granted by the National AIDS Programme and the General Secretariat of Mental Health and Addiction Treatment, Egypt.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Van Hout, MC., Elsayed, H., Elgamil, R. et al. ‘Secrecy, Trust, Safety’: a Multi-stakeholder Situation Assessment of Gendered and Contextual Vulnerabilities and Service Level Responsiveness to the Needs of Women Who Use Drugs in Egypt. Int J Ment Health Addiction (2023). https://doi.org/10.1007/s11469-023-01143-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-023-01143-6