
Abstract
Background
As an emerging technology in robot-assisted (RA) surgery, the potential benefits of its application in transforaminal lumbar interbody fusion (TLIF) lack substantial support from current evidence.
Objective
We aimed to investigate whether the RA TLIF is superior to FG TLIF in the treatment of lumbar degenerative disease.
Methods
We systematically reviewed studies comparing RA versus FG TLIF for lumbar degenerative diseases through July 2022 by searching PubMed, Embase, Web of Science, CINAHL (EBSCO), Chinese National Knowledge Infrastructure (CNKI), WanFang, VIP, and the Cochrane Library, as well as the references of published review articles. Both cohort studies (CSs) and randomized controlled trials (RCTs) were included. Evaluation criteria included the accuracy of percutaneous pedicle screw placement, proximal facet joint violation (FJV), radiation exposure, duration of surgery, estimated blood loss (EBL), and surgical revision. Methodological quality was assessed using the Cochrane risk of bias and ROBINS-I Tool. Random-effects models were used, and the standardized mean difference (SMD) was employed as the effect measure. We conducted subgroup analyses based on surgical type, the specific robot system used, and the study design. Two investigators independently screened abstracts and full-text articles, and the certainty of evidence was graded using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach.
Results
Our search identified 539 articles, of which 21 met the inclusion criteria for quantitative analysis. Meta-analysis revealed that RA had 1.03-folds higher “clinically acceptable” accuracy than FG (RR: 1.0382, 95% CI: 1.0273–1.0493). And RA had 1.12-folds higher “perfect” accuracy than FG group (RR: 1.1167, 95% CI: 1.0726–1.1626). In the case of proximal FJV, our results indicate a 74% reduction in occurrences for patients undergoing RA pedicle screw placement compared to those in the FG group (RR: 0.2606, 95%CI: 0.2063- 0.3293). Seventeen CSs and two RCTs reported the duration of time. The results of CSs suggest that there is no significant difference between RA and FG group (SMD: 0.1111, 95%CI: -0.391–0.6131), but the results of RCTs suggest that the patients who underwent RA-TLIF need more surgery time than FG (SMD: 3.7213, 95%CI: 3.0756–4.3669). Sixteen CSs and two RCTs reported the EBL. The results suggest that the patients who underwent RA pedicle screw placement had fewer EBL than FG group (CSs: SMD: -1.9151, 95%CI: -3.1265–0.7036, RCTs: SMD: -5.9010, 95%CI: -8.7238–3.0782). For radiation exposure, the results of CSs suggest that there is no significant difference in radiation time between RA and FG group (SMD: -0.5256, 95%CI: -1.4357–0.3845), but the patients who underwent RA pedicle screw placement had fewer radiation dose than FG group (SMD: -2.2682, 95%CI: -3.1953–1.3411). And four CSs and one RCT reported the number of revision case. The results of CSs suggest that there is no significant difference in the number of revision case between RA and FG group (RR: 0.4087,95% CI 0.1592–1.0495). Our findings are limited by the residual heterogeneity of the included studies, which may limit the interpretation of the results.
Conclusion
In TLIF, RA technology exhibits enhanced precision in pedicle screw placement when compared to FG methods. This accuracy contributes to advantages such as the protection of adjacent facet joints and reductions in intraoperative radiation dosage and blood loss. However, the longer preoperative preparation time associated with RA procedures results in comparable surgical duration and radiation time to FG techniques. Presently, FG screw placement remains the predominant approach, with clinical surgeons possessing greater proficiency in its application. Consequently, the integration of RA into TLIF surgery may not be considered the optimal choice.
Systematic review registration
PROSPERO CRD42023441600.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Since the first report of transforaminal lumbar interbody fusion (TLIF) for the treatment of lumbar spondylolisthesis by Harms and Rolinger et al. [1] in 1982, TLIF has progressively evolved into a standard surgical procedure for addressing lumbar degenerative diseases [2]. Subsequently, Foley et al. [3] further advanced TLIF by introducing the minimally invasive technique (Wiltse technique). This breakthrough facilitated the initial adoption of minimally invasive surgery (MIS) in TLIF, leading to decreased surgical trauma, accelerated recovery, and an overall alleviation of the patient's daily life burden. Nevertheless, TLIF is not without its drawbacks, including prolonged surgical time and a steep learning curve. The duration of the surgery frequently hinges on the surgeon's proficiency in mastering technical skills [4, 5]. The restricted operating field frequently results in imprecise screw placement, often requiring additional corrective surgeries. To guarantee optimal accuracy in screw placement, real-time fluoroscopic examination is typically considered essential throughout the procedure. Consequently, the potential for excessive radiation exposure during MIS-TLIF remains a significant concern [6, 7]. Undoubtedly, whether it is fluoroscopy-guided (FG) TLIF or MIS-TLIF, the most critical aspect of the surgical procedure is the swift and accurate placement of pedicle screws. This objective is paramount in reducing surgical time, minimizing intraoperative bleeding, enhancing surgical outcomes, lowering the rate of revision surgeries, and mitigating radiation exposure. Therefore, achieving expedient and precise placement of pedicle screws remains an urgent concern in TLIF.
The integration of robotic technology into spine surgery has offered a solution for achieving accurate and efficient pedicle screw placement. Robotics can assist surgeons in precise navigation and access to critical anatomical structures during spinal surgery, leveraging 3D imaging. Furthermore, the employment of surgical robots for pedicle screw placement ensures both safety and accuracy, while also minimizing the surgeon's exposure to intraoperative radiation. However, at present, FG techniques persist as the predominant method for screw insertion in TLIF, with surgeons exhibiting greater proficiency in its application. As a nascent robot-assisted (RA) technology, the potential superiority of its application in TLIF surgery has not yet been substantiated by relevant evidence. Furthermore, opting for RA procedures in TLIF imposes a heightened financial burden on patients compared to traditional FG-TLIF. Consequently, the suitability of integrating RA technology into TLIF surgery remains uncertain [8, 9]. In order to examine the potential advantages of RA in terms of screw placement accuracy and its ability to address the limitations of FG in TLIF, we conducted a systematic review and meta-analysis.
Methods
This systematic review and meta-analysis are performed based on the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA, Text 1) and Cochrane Handbook for Systematic Reviews of Interventions [10, 11]. No ethical approval and patient consent are required because all analyses are based on previous published studies. The full protocol for this study is available in the supplementary material (Text 2). Literature search, data extraction, data synthesis, and quality assessment were conducted by at least two professional reviewers. The review protocols were retrospective registered on PROSPERO (International Prospective Register of Systematic Reviews, No. CRD42023441600). Our study was conducted retrospectively on July 12, 2022. The retrospective registration in no way compromises the quality, validity, or integrity of the research findings presented in this manuscript. All research procedures, data collection, and data analysis were carried out systematically and well-documented, ensuring the reliability and reproducibility of our results.
Search strategy and selection criteria
We systematically searched several databases, including PubMed, Excerpta Medical database (Embase), Web of Science, CINAHL (EBSCO), China National Knowledge Infrastructure (CNKI), WanFang Database (WanFang), China Science and Technology Journal Database (VIP), and the Cochrane Library, from inception to July 2022 using the following keywords combined with MeSH terms: 'robot-assisted,' 'fluoroscopy-assisted,' 'lumbar surgery,' 'spinal surgery,' 'transforaminal lumbar interbody fusion,' and 'minimally invasive surgery,' 'TLIF,' 'MIS-TLIF,' 'RA,' 'FG,' and 'lumbar degenerative diseases.' Search terms were combined using the Boolean operators 'AND' or 'OR.' Furthermore, the reference lists of manuscripts were also hand-searched to ensure that some studies, which were not identified by our original search, were also included in the present study. The complete search strategies were shown in Supplementary material 1.
We incorporated all types of relevant studies, encompassing randomized controlled trials (RCTs) as well as prospective and retrospective cohort studies (CSs). The study population comprised patients diagnosed with degenerative lumbar spinal diseases, such as spondylolisthesis and lumbar spinal stenosis, who underwent treatment via TLIF. In the included studies, the intervention group must be RA TLIF, and the control group is FG TLIF (Table 1). The following exclusion criteria were used: (1) studies with insufficient data; (2) cadaveric and animal studies; (3) sample size per arm < 10 participants; and (4) patients with other treatment. Moreover, there were no language restrictions.
Data extraction and synthesis
The two reviewers (JB.G and NN.F) extracted data independently using a standardized form. The following factors were recorded when the information in the reviewed articles was available: first author, year, participants and surgery, type of surgery, type of robot system, sample size, age, sex, study design, intra-pedicular accuracy, proximal facet joint violation (FJV), duration of surgery, estimated blood loss (EBL), radiation time and dose, and revision case. Any disagreements between the reviewers (JB.G and NN.F) were resolved through discussion. In case of insolvable discrepancies, a third reviewer (KT.Y) acted as an arbitrator.
The primary outcomes include the accuracy of percutaneous pedicle screw placement and the occurrence of proximal facet joint violation (FJV). For intra-pedicular accuracy, the positions of pedicle screws were classified using the Gertzbein and Robbins criteria [12]. Grade A represents an intra-pedicular screw without breaching the cortical layer of the pedicle. Grade B refers to a screw that breaches the cortical layer of the pedicle but does not exceed it laterally by more than 2 mm. Grades C and D indicate penetration of less than 4 mm and 6 mm, respectively (indicated by arrows). Grade E is assigned to screws (indicated by arrows) that either do not pass through the pedicle or, at any point in their intended intra-pedicular course, breach the cortical layer of the pedicle in any direction by more than 6 mm. Proximal FJV was assessed according to the violation grade proposed by Babu et al. [13]. The grading system for violations was as follows: Grade 0 represented pedicle screws that did not encroach on the facet joint. Grade 1 defined pedicle screws that violated the facet joint surface by ≤ 1 mm. Grade 2 represented pedicle screws that clearly violated the facet joint. The secondary outcomes include radiation time and dose (duration of radiation exposure and amount of radiation administered during the surgery), duration of surgery (total time required for the surgical procedure), estimated blood loss (EBL, an estimation of the amount of blood lost during surgery), and surgical revision (instances where revision surgery was required due to complications or issues with the initial pedicle screw placement).
The minimally important difference (MID) is the smallest amount of improvement in a treatment outcome that patients would recognize as important. For Proximal FJV, a lower grade is better, and the MID is Grade A. Regarding intra-pedicular accuracy, the MID of Grade 0 represents perfect intra-pedicular localization with no cortical breach. Any deviation from perfect intra-pedicular localization (i.e., any grade higher than 0) would be considered clinically meaningful. As for all secondary outcomes, there are no articles discussing the MID for them, but lower values are considered better.
Two investigators independently selected articles based on the criteria described above. The full text was scanned to determine whether the articles met the inclusion criteria. Disagreements were resolved through discussion until a consensus was reached. If no consensus was reached, a third investigator was consulted.
In this study, our primary objectives included assessing the accuracy of percutaneous pedicle screw placement, proximal FJV, radiation exposure, duration of surgery, EBL, and the necessity for surgical revision. We selected these outcomes based on their clinical relevance to spinal surgery and their alignment with the specific research questions we aimed to address. However, we must acknowledge that the manuscript does not include several outcomes that were initially planned in the study protocol, such as the length of hospital stay, VAS for leg pain and back pain, and the Oswestry Disability Index. The decision to exclude these outcomes was made after careful consideration of data availability and their alignment with the primary research objectives. The omission of these outcomes does not compromise the validity of our findings concerning the primary objectives mentioned above. We believe that focusing on these specific outcomes provided a more focused and in-depth analysis of the key aspects of our study.
Risk of bias and quality of evidence
The methodological quality of the included studies was evaluated using the Cochrane Risk of Bias Tool for randomized controlled trials (RCTs) and the Risk of Bias in Non-Randomized Studies—of Interventions (ROBINS-I) Tool for non-RCTs. Two researchers conducted the assessments independently. In instances of disagreement, a third researcher made the final decision. The ROBINS-I tool encompasses an evaluation of bias risks related to confounding factors (such as insufficient information on the number of operation levels, baseline health status, surgeon experience, patient selection criteria, or center-specific factors), participant selection, intervention classification, deviations from the intended intervention, missing data, outcome measurement, and the selection of reported results [14].
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool was used to assess the overall quality and strength of available evidence. With the use of this approach, evidence is classified as “very low,” “low,” “moderate,” or “high” quality. Evidence from RCTs receives a default grade of “high” quality but may be downgraded based on prespecified criteria. Reasons for downgrading include risk of bias (assessed through the Cochrane Risk of Bias tool and ROBIN-I tool), inconsistency (substantial unexplained interstudy heterogeneity; I2 ≥ 50%, P < 0.10), indirectness (presence of factors that limited the generalizability of the results), imprecision (the 95% CI for effect estimates were wide or crossed a minimally important difference for benefit or harm), and publication bias (significant evidence of small-study effects).
Subgroup analysis
We conducted subgroup analyses if there were 2 or more studies in a given subgroup and performed tests of interaction to establish whether the subgroups differed significantly from one another. We assessed the credibility of significant subgroup effects (P < 0.05) using previously suggested criteria. Subgroup analyses was performed for type of surgery, type of robot system and study design.
Statistical analysis
We assess standard mean difference (SMD) with 95% confidence interval (CI) for continuous outcomes and risk ratio (RR) with 95% CI for dichotomous outcomes. Random models were used for all analyses and not to rely on (arbitrary) cut of values for heterogeneity. The rationale for this is that studies on these patient populations cannot be assumed to have one true mean estimate. Statistical heterogeneity was assessed with the Q-test and the I2 statistic. I2 values of 25%, 50%, and 75% were considered to indicate low, moderate, and high heterogeneity, respectively [15]. If more than 10 studies were available for a particular comparison, we used funnel plots to determine publication bias. Sensitivity analysis using the trim and fill method is employed to assess the stability of the meta-analysis results [16]. If there is little difference in the funnel plot before and after the trim and fill method, it indicates that the results are stable and highly reliable. And missing values were handled, and imputation methods (mean SD from similar studies) was used.
Data were analyzed with the open-source, meta-analysis software OpenMeta-Analyst, which uses R as the underlying statistical engine [17]. All figures were generated using RStudio.
Results
Search results and trial characteristics
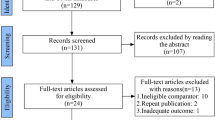
Title and abstract literature review yielded 539 articles, of which 72 met the inclusion criteria for full text review (Fig. 1). References of 7 systematic reviews found through our online search were also reviewed for relevant articles. A final 21 articles met the inclusion criteria for quantitative analysis. Among them, there were 2 randomized controlled trials (RCTs) [18, 19] and 19 CSs [8, 20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. Among the twenty-one studies, six of included studies used Renaissance™ system [20, 21, 26, 27, 30, 32], eleven of included studies used TiRobot system [18, 19, 22,23,24,25, 28, 34,35,36,37], three of included studies used ROSA™ system [8, 31, 33] and one of included studies used Mazor X Robot system [29]. In terms of surgical type, five of included studies applied the robot system in TLIF surgery [20, 22,23,24, 30] and sixteen of included studies used the robot system in MIS-TLIF surgery [8, 18, 19, 21, 25,26,27,28,29, 31,32,33,34,35,36,37]. Characteristics of included studies are summarized in Table 2.

Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow chart of the selection process. (The PRISMA 2020 statement: an updated guideline for reporting systematic reviews) [38]
Primary outcome
The accuracy of pedicle screw placement
The comparison of the accuracy of pedicle screw placement between RA-and FG-TLIF according to Gertzbein and Robbins criteria in fourteen CSs. If any portion of the screw was ≤ 3 mm outside the pedicle (Grade A + B), we categorized them as “clinically acceptable” accuracy. And the portion of the screw was not deviation (Grade A), we categorized them as “perfect” accuracy.
The “clinically acceptable” accuracy
Low-quality evidence from fourteen CSs [20,21,22,23,24,25,26, 28, 31, 32, 34,35,36,37] (Table 3), reported a significant difference in “clinically acceptable” accuracy between RA- and FG-TLIF, and RA had 1.03-folds higher “clinically acceptable” accuracy than FG (RR: 1.0382, 95% CI: 1.0273–1.0493, z = 6.96, I2 = 9%, p < 0.0001, Fig. 2). The funnel plot demonstrates a mostly symmetrical distribution, and minimal changes are observed after applying the trim-and-fill method. This indicates a high level of confidence in the result (Fig. 3).

Pooled Analysis of Pedicle Screw Insertion “clinically acceptable” Accuracy. a Subgroup of surgical type. b Subgroup of robotic type

Funnel plot of CSs comparing the “clinically acceptable” accuracy of pedicle screw placement between RA and FG TLIF (left). And the shape of funnel plot after trim-and-fill method (right). No funnel plot of RCTs has been included as there were fewer than 10 RCTs
Subgroup analysis based on surgical type showed that RA had higher “clinically acceptable” accuracy than FG both in TLIF (RR: 1.04, 95% CI: 1.02–1.06, I2 = 0%, p < 0.05, Fig. 2a) and MIS-TLIF (RR: 1.03, 95% CI: 1.02–1.04, I2 = 32%, p < 0.05, Fig. 2a).
Subgroup analysis based on robotic type showed that Renaissance™ system, TiRobot and ROSA ™ system assisted TLIF have higher “clinically acceptable” accuracy than FG-TLIF (Fig. 2b).
The “perfect” accuracy
Low-quality evidence from fourteen CSs [20,21,22,23,24,25,26, 28, 31, 32, 34,35,36,37] (Table 3), reported a significant difference in “perfect” accuracy between RA and FG TLIF. RA exhibited 1.12-folds higher “perfect” accuracy than FG group, with high evidence of heterogeneity (RR: 1.1167, 95% CI: 1.0726–1.1626, z = 5.37, I2 = 75%, p < 0.0001, Fig. 4). The funnel plot demonstrates a mostly symmetrical distribution, and minimal changes are observed after applying the trim-and-fill method. This indicates a high level of confidence in the result (Fig. 5).

Pooled Analysis of Pedicle Screw Insertion “perfect” Accuracy. a Subgroup of surgical type. b Subgroup of robotic type

Funnel plot of CSs comparing the “perfect” accuracy of pedicle screw placement between RA and FG TLIF (top). And the shape of funnel plot after trim-and-fill method (bottom)
Subgroup analysis based on surgical type showed that RA had higher “perfect acceptable” accuracy than FG in both TLIF (RR: 1.08, 95% CI: 1.04–1.12, I2 = 0%, p < 0.05, Fig. 3a) and MIS-TLIF (RR: 1.13, 95% CI: 1.07–1.19, I2 = 82%, p < 0.05, Fig. 3a). Subgroup analysis based on robotic type indicated that Renaissance™ system, TiRobot and ROSA ™ system assisted TLIF have higher “perfect acceptable” accuracy than FG-TLIF (Fig. 3b).
A RCT reported the accuracy of pedicle screw placement with the following result [28]. Among the 92 pedicle screws in the RA group, 87 were Grade A, and 5 were Grade B. Among the 100 pedicle screws in the FG group, 85 were Grade A, and 15 were Grade B. The superiority of Grade A screws was observed in the robot-assisted MIS-TLIF group.
Proximal facet joint violation
Low-quality evidence from five CSs [21,22,23, 35, 36], reported proximal FJV assessed through CT scans. The results suggest that the patients who underwent RA pedicle screw placement had 74% fewer proximal FJV than the FG group (RR: 0.2606, 95%CI: 0.2063- 0.3293, z = -11.27, I2 = 3%, p < 0.0001) (Fig. 6).

Pooled Analysis of Proximal Facet Joint Violation
Secondary outcome
Duration of surgery
Very low-quality evidence from seventeen CSs [8, 20, 22,23,24,25,26,27,28,29,30, 32,33,34,35,36,37] and two RCTs [18, 19] (Table 3), reported the duration of time, as shown in Fig. 7. The results of CSs suggest that there is no significant difference between RA and FG group, with high evidence of heterogeneity (SMD: 0.1111, 95%CI: -0.391–0.6131, z = 0.43, I2 = 93%, p = 0.6646). The funnel plot demonstrates a symmetrical distribution, and the funnel plot shows minimal changes after trim-and-fill method, indicating this result with a high level of confidence (Fig. 8).

Pooled Analysis of Duration of Surgery. a Subgroup of surgical type (Cohort study). b Subgroup of robotic type (Cohort study). c Pooled Analysis of RCT

Funnel plot of CSs comparing the duration of surgery between RA-and FG-TLIF (top). And the shape of funnel plot after trim-and-fill method (bottom). No funnel plot of RCTs has been included as there were fewer than 10 RCTs
Subgroup analysis of surgical type showed that the patients who underwent RA pedicle screw placement need more surgery time than FG group in TLIF surgery (Fig. 7a). However, the duration of surgery did not show a difference between RA and FG group in MIS-TILF surgery (Fig. 7a).
According to subgroup analysis of robotic types, no robotic system outperforms the FG-TLIF in terms of duration of surgery (Fig. 7b).
And the subgroup analysis of study types [18, 19] showed that the patients who underwent RA pedicle screw placement need more surgery time (3.72 × SD minutes) than FG group (SMD: 3.7213, 95%CI: 3.0756–4.3669, z = 11.30, I2 = 0%, p < 0.0001, Fig. 7c).
Estimated blood loss
Low-quality evidence from sixteen CSs [8, 20, 22,23,24,25,26, 28,29,30, 32,33,34,35,36,37] and two RCTs [18, 19] (Table 3), reported the estimated blood loss, as shown in Fig. 9. The results of CSs suggest that the patients who underwent RA pedicle screw placement had fewer estimated blood loss than FG group, with high evidence of heterogeneity (SMD: -1.9151, 95%CI: -3.1265–0.7036, z = -3.10, I2 = 98%, p = 0.0019). The funnel plot demonstrates a symmetrical distribution, and the funnel plot shows minimal changes after trim-and-fill method, indicating this result is reliable (Fig. 10).

Pooled Analysis of Estimated Blood Loss. a Subgroup of surgical type. b Subgroup of robotic type. c Pooled Analysis of RCT

Funnel plot of CSs comparing the estimated blood loss between RA-and FG-TLIF (top). And the shape of funnel plot after trim-and-fill method (bottom). No funnel plot of RCTs has been included as there were fewer than 10 RCTs
Subgroup analysis of surgical type showed that the patients who underwent RA pedicle screw placement with fewer EBL than FG group both in TLIF and MIS-TLIF surgery (Fig. 9a). And Subgroup analysis of robotic type showed that the patients who underwent Renaissance™ system and TiRobot assisted pedicle screw placement with fewer EBL both in TLIF and MIS-TLIF surgery, however, the Mazor X Robot and ROSA™ do not demonstrate this advantage (Fig. 9b).
And the results of RCTs [18, 19] suggest that the patients who underwent RA pedicle screw placement had fewer estimated blood loss than FG group, with high evidence of heterogeneity (SMD: -5.9010, 95%CI: -8.7238–3.0782, z = -4.10, I2 = 88%, p < 0.0001, Fig. 9c).
Radiation exposure
Radiation time
Very low-quality evidence from seven CSs [22,23,24, 28, 32, 34, 37] (Table 3), reported the radiation time, as shown in Fig. 11. The results of CSs suggest that there is no significant difference in radiation time between RA and FG group, with high evidence of heterogeneity (SMD: -0.5256, 95%CI: -1.4357–0.3845, z = -1.13, I2 = 98%, p = 0.2576).

Pooled Analysis of Radiation Time
Subgroup analysis of surgical type showed that the patients who underwent RA pedicle screw placement with fewer radiation exposure time in TLIF surgery, however, RA pedicle screw placement does not demonstrate this advantage when compared to FG pedicle screw placement in MIS-TLIF surgery (Fig. 11).
Radiation dose
Very low-Grade quality evidence from seven CSs [22,23,24, 29, 32, 34, 37] (Table 3), reported the radiation dose, as shown in Fig. 12. The results of CSs suggest that the patients who underwent RA pedicle screw placement had fewer radiation dose than FG group, with high evidence of heterogeneity (SMD: -2.2682, 95%CI: -3.1953–1.3411, z = -4.79, I2 = 94%, p < 0.0001).

Pooled Analysis of Radiation Dose
Subgroup analysis of surgical type and robotic type showed that the patients who underwent RA pedicle screw placement with fewer radiation exposure dose both in TLIF and MIS-TLIF surgery.
Surgical revision
Low-quality evidence from four CSs [8, 22, 30, 32] and one RCT [18] (Table 3), reported the number of surgical revisions, as shown in Fig. 13. The results of CSs suggest that there is no significant difference in the number of surgical revisions between RA and FG group (RR: 0.4087, 95% CI 0.1592–1.0495, z = -1.86, I2 = 0%, p = 0.0629). However, the RCT [18] reported that the number of surgical revisions of RA pedicle screw placement is lower than FG pedicle screw placement.

Pooled Analysis of Surgical Revision
Risk of bias
The Cochrane risk of bias tool was adopted evaluate the mythological quality of two RCTs, and the results were presented in Table 4. The quality of two RCTs was limited predominantly by lack of blinding, given the nature of clinical study. Regarding the random sequence generation and allocation concealment, two studies [18, 19] were low risk. In terms of blinding of outcome assessment, no information was reported to affect the outcomes because of the deviations [19]. With respect to the incomplete outcome data, two studies [18, 19] were not mentioned, thus these two studies were at unclear risks. As for selective reporting, all the RCTs were at low risk, because there is complete data and results reported with no selection. Other bias was not mentioned in these two RCTs, thus the risk of bias was unclear risks.
The ROBINS-I was used to assess the risk of bias for four prospective cohort studies [23, 24, 26, 35] and fifteen retrospective cohort studies [8, 20,21,22, 25, 27,28,29,30,31,32,33,34, 36, 37] (Table 5), and detail of reasons for bias are documented in Supplemental 2.
Discussion
Main findings and interpretation of the results
Lumbar degenerative diseases, such as spinal stenosis, disc herniation and spondylolisthesis, represent the primary causes of low back and leg pain in elderly patients [39]. When conservative treatments prove ineffective, surgical intervention becomes an inevitable option, and the choice of surgical methods varies significantly based on individual patient characteristics and their specific symptoms [40]. The conventional PLIF necessitates extensive soft tissue dissection, such as paraspinal muscles, resulting in surgical trauma and an increased risk of recurring postoperative pain [41]. This significantly impairs the postoperative quality of life for patients [42]. With the widespread promotion and application of minimally invasive techniques, there has been an increasing number of surgical options for lumbar degenerative diseases. TLIF, a technique that combines interbody fusion with pedicle screw fixation, has addressed several issues encountered in the traditional PLIF. TLIF utilizes a tube to access the intervertebral space through the intervertebral foramen, gradually expanding the muscle interval to avoid extensive soft tissue dissection. This technique effectively reduces damage to the paraspinal muscles and significantly lowers the risk of neurological and vascular injuries [43, 44]. However, the placement of channels for screw insertion and percutaneous pedicle screw fixation in TLIF requires fluoroscopic guidance, leading to extended surgical duration and increased radiation exposure compared to PLIF. In recent years, remarkable progress has been made in the clinical utilization of intelligent and digital technologies in the field of orthopedic surgery. Robot-assisted spinal surgery offers the benefits of minimally invasive procedures, enhanced precision, and reduced trauma. Through meticulous planning of optimal entry points, angles, and depths, the safety, accuracy, and precision of surgical procedures, including screw placement, have undergone significant enhancements [45, 46]. However, RA-TLIF has a steep learning curve compared to traditional FG-TLIF, requiring additional time and money. Hence, clinicians should thoroughly contemplate whether utilizing RA technology for TLIF is a more fitting choice.
The evaluation of RA pedicle screw placement primarily focuses on the accuracy of screw insertion, followed by factors such as radiation exposure, surgical duration, and blood loss. While most studies have demonstrated positive results for the RA screw placement compared to the free-hand or FG screw placement [47], there are still varying opinions in some studies. Some studies have indicated that in scenarios where anatomical structures are adequately visualized, RA screw placement may not necessarily provide a substantial accuracy advantage over traditional FG screw placement [20, 48]. Additionally, some studies indicating that RA may decrease accuracy of screw placement [49]. The debate of RA screw placement may stem from factors such as preoperative planning, image quality, and intraoperative manipulation. The automatic calculations for robot parameters still require surgeon verification, fine-tuning, or manual planning. The efficiency and accuracy of planning are closely related to image calibration and image mode selection. Currently, the automatic combination of 2D and 3D multimodal images is possible but may require more time-consuming. The design of screw placement still relies primarily on manual assessment, lacking self-planning and validation that incorporate motion and individual patient conditions. Therefore, whether RA-TLIF offers advantages in terms of accuracy, surgical time, and intraoperative blood loss over traditional FG-TLIF remains inconclusive until evidence from systematic reviews and meta-analyses becomes available.
Screw placement accuracy
For the assessment of screw placement accuracy, the Gertzbein and Robbins criteria are commonly used [12]. Based on previous literature categorizing the accuracy of screw placement, this study considers the combination of Grade A + Grade B as "clinically acceptable" accuracy of pedicle screw placement, while Grade A is categorized as "perfect" accuracy of pedicle screw placement. We conducted a meta-analysis with pooled data from fourteen CSs [20,21,22,23,24,25,26, 28, 31, 32, 34,35,36,37] that included 1432 patients and 5466 cranial pedicle screws to explore whether RA-TLIF is superior to FG-TLIF in terms of “clinically acceptable” and “perfect” accuracy of pedicle screw placement. We believe that this study is the first meta-analysis to systematically compare the accuracy of pedicle screw placement between RA and FG pedicle screw placement in TLIF; however, the quality of evidence is low. The meta-analysis demonstrated that RA insertion was associated with substantially higher accuracy of pedicle screw placement than conventional FG screw insertion in TLIF. Furthermore, the pooled results of subgroup analysis suggest that RA pedicle screw placement demonstrated greater accuracy than FG in both TLIF and MIS-TLIF. In terms of robotic type, the Renaissance™ system, TiRobot, and ROSA™ system assisted TLIF have higher accuracy than FG-TLIF.
A previous study conducted by Molliqaj et al. [50] retrospectively analyzed the comparison between RA and FG screw placement in thoracolumbar fractures. The study found that RA screw placement had a higher accuracy rate compared to FG screw placement. Macke et al. [51] demonstrated the application of RA screw placement in the treatment of idiopathic scoliosis, and found a screw placement accuracy rate of 99.04% for RA placement, superior to FG placement (90.74%). Serval studies also indicate that in spinal surgeries, RA screw placement achieves significantly higher accuracy rates than FG screw placement [46, 52, 53]. However, currently, there is still a lack of evidence to suggest that RA has a superiority over traditional FG in terms of screw placement accuracy in TLIF. Generally speaking, due to the specific anatomical characteristics of each patient, RA surgery requires preoperative detailed 3D planning. Through above, the surgeon gains a comprehensive understanding of the surgical anatomical structures and reduces the likelihood of intraoperative complications. Preoperative planning also allows for optimization of implant size and trajectory based on the specific pedicle anatomy of patients. The robot system can simulate ideal screw trajectories based on individual anatomical differences and accurately reproducing these simulations during surgery. This is the primary reason why RA-TLIF.
Proximal facet joint violation
This meta-analysis revealed that RA screw placement in TLIF can indeed reduce proximal FJV compared to FG-PLIF [21,22,23, 35, 36] (RR: 0.2606, 95%CI: 0.2063- 0.3293). The quality of evidence for proximal facet joint violation is low.
The accuracy of screw placement is also related to the proximal FJV [54], which has been regarded as an independent risk factor for ASD after spinal fusion [55, 56]. Sakaura et al. [57] conducted a comparative study, comparing cortical bone trajectory and traditional trajectory insertion techniques. They reported that the use of cortical bone trajectory may potentially decrease the occurrence of radiographic and systemic spinal degeneration by preserving the proximal facet joints. Levin et al. [58] pointed out that the FJV was associated with increased reoperation rates and reduced improvement in quality of life. Hyun et al. [59] conducted a prospective RCT and found no significant difference in the incidence of FJV between RA and FG insertion methods (0.00% vs. 0.71%). Similarly, Archavlis et al. [60] revealed that the occurrence of FJV in the RA group was similar to that in the FG group (5% vs. 6%). FG pedicle screw placement remains the most used technique for lumbar fusion. Meanwhile, RA screw placement has emerged as a novel minimally invasive technique, which has gradually gained acceptance for reducing screw misplacement rates and enhancing insertion safety. However, contradictory results exist regarding the incidence of FJV between FG-and RA-TLIF. We believe that the use of RA enables precise positioning, ensuring optimal screw placement within the target area of each pedicle. This minimizes the disturbance caused by pedicle screws to the adjacent proximal segment structures, reduces stress on the adjacent vertebrae, improves the biomechanical environment of the segmental structure, and ultimately decreases the probability of pseudoarthrosis and ASD.
Perioperative indicators
According to GRADE assessment of included studies, the quality of evidence for surgery duration is very low. Surgical duration and intraoperative blood loss are perioperative indicators directly related to screw placement accuracy. Currently, there is no evidence suggesting that RA-TLIF can reduce surgical time and intraoperative blood loss. The results of this meta-analysis revealed that there was no significant difference in surgical time between the two groups [8, 20, 22,23,24,25,26,27,28,29,30, 32,33,34,35,36,37], and the funnel plot remained unchanged after applying the trim-and-fill method, indicating result stability. However, results of RCTs [18, 19] showed that RA had a longer surgical time compared to the FG group. Although RCTs have higher methodological quality and evidence levels than CSs, we feel that this analysis contained a greater number of moderate-quality CSs, while the number of included RCTs was limited and lacked blinding. As a result, we have greater confidence in the CS results, which show that there is no significant difference in surgical time between RA-TLIF and FG-TLIF. This may be attributed to the higher proficiency level in manual percutaneous screw placement in MIS surgery. It is speculated that as proficiency in robot usage increases, this time difference may become more prominent. Furthermore, the pooled results of subgroup analysis show that RA has a benefit over FG only in open TLIF surgery in terms of shorting surgical time, but not in MIS-TLIF surgery (SMD: 0.57, 95%CI: 0.15–1). This could be because the field of view in open TLIF surgery is greater and the operation of the surgical robot is easier, resulting in a shorter operation time than in FG-MISTLIF.
Regarding EBL, the quality of evidence for surgery duration is low. The pooled results of this study indicated that both CSs [8, 20, 22,23,24,25,26, 28,29,30, 32,33,34,35,36,37] and RCTs [18, 19] showed lower EBL with the application of RA in TLIF compared to FG. Furthermore, the surgical type and robotic type subgroups all revealed that RA screw placement accuracy can lower EBL when compared to FG screw placement accuracy. This is primarily attributed to the more accurate screw placement in RA surgeries, where the planned screw trajectory may reduce tension on the pedicle screw insertion, thus decreasing stress on the pedicle and potentially reducing tension and damage to surrounding soft tissues, such as muscles and skin.
Intraoperative radiation exposure caused by fluoroscopy is another concern to consider in TLIF [61, 62]. This study found no significant difference in radiation exposure time between the RA-TLIF and FG-TLIF [22,23,24, 28, 32, 34, 37], and the evidence for them are low quality. Subgroup analysis showed that RA pedicle screw placement is associated with a reduction in radiation exposure time compared to FG techniques. This suggests that the use of robotics is particularly effective in decreasing radiation exposure in open TLIF procedures. In MIS-TLIF, there is no significant difference in radiation exposure time between RA and FG techniques. This implies that, in the context of MIS-TLIF, both RA and FG may result in similar levels of radiation exposure. However, the intraoperative radiation dose in the RA group was significantly lower than in the FG group [8, 18, 19, 22, 30, 32]. And subgroup analysis has the same results.
Most studies suggest that one of the advantages of surgical robots is their ability to minimize intraoperative radiation exposure. Roser et al. [63] compared the radiation doses between RA and FG techniques and found that RA has lower doses compared to the FG group. However, Ringel et al. [49] reported no significant difference in intraoperative radiation doses between RA an FG. Schizas et al. [64] reported similar radiation times between the two groups. Based on our results of RA surgeries, there is contradictory in reducing radiation time, and the analysis indicates that the experience of the surgeon is important factors in determining radiation exposure. We believe that while RA can reduce radiation exposure in the operating room, patients often require preoperative CT scans for surgical planning, and these studies may have included the radiation time from preoperative CT scans. FG techniques rely on repeated intraoperative fluoroscopy, while RA techniques rely on the patient's preoperative 3D CT scans and preoperative planning. This is the main reason for the lack of significant difference in radiation exposure time between the two techniques.
Surgical revision
It is important to note that the absence of a significant difference in the number of surgical revisions due to misplacement between the RA and FG screw placement in the study suggests that both techniques, when properly performed, have a similar rate of accuracy in pedicle screw placement [8, 18, 22, 30, 32]. However, the quality of evidence for surgical revision outcomes in the study is low, which affect the confidence in the results related to surgical revisions.
Surgical revision is necessary in cases of severe screw misplacement or persistent radicular pain following the initial surgery. This is because FG techniques, being the gold standard for implantation, are performed by experienced clinicians who can effectively avoid severe misplacements and postoperative complications, similar to the RA-TLIF. Nevertheless, we believe that with the advancement of modern spine surgery, the increasing complexity of spinal disorders poses higher demands on minimally invasive techniques. Robotic assistance, combined with artificial intelligence, can alleviate factors such as insufficient clinical experience, enabling more precise and accurate operations. Considering the diverse and complex clinical conditions and the need for different indications, the development of robotic technology is expected to become more refined and systematic, providing better service in the clinic.
Limitations
Several limitations should be interpreted in this meta-analysis. The main limitation of this study is that there were too few relevant RCTs devoted to the evaluation of the difference of RA-TLIF and FG-TLIF. Thus, we did not perform the assessment of publication bias in some outcome, such as proximal facet joint violation, radiation exposure and surgical revision. Another limitation is that our study included only two RCTs, four prospective CSs and fifteen retrospective CSs. A meta-analysis of such data will lead to less powerful results compared to study obtained purely from RCTs. This difficulty primarily arises from the challenges associated with executing double-blind, randomized selection of surgical techniques in a clinical setting. Next, a limitation of this systematic review is that the general quality of the available RCTs was not high. Because studies could not blind the participants because they had the right to know about the surgery interventions., blinding of personnel and participants was impossible in practice. Investigators in most of the included studies did not describe clearly whether the outcome assessments were blinded. Moreover, our findings are limited by the heterogeneity of the included studies, therefore, the reliability of the results may be insufficient. Then, an important limitation of this study is that not all initially planned outcomes were investigated. While the primary objectives were rigorously addressed, the decision to omit certain planned outcomes introduces a potential source of bias and limits the overall comprehensiveness of our analysis. Finally, while we took rigorous measures to ensure the systematic and well-documented execution of all research procedures, data collection, and data analysis, we acknowledge that the retrospective nature of protocol registration is a serious limitation. We want to emphasize that this retrospective registration does not compromise the quality, validity, or integrity of the research findings presented in this manuscript. However, we recognize its potential impact on the perception of study transparency and pre-specification.
Implications for future research
The results of this systematic review suggest that RA-TLIF may have certain advantages over traditional FG-TLIF. However, additional RCTs and CSs are needed to confirm these findings and provide a more comprehensive understanding of the benefits and drawbacks of each approach. Furthermore, large-scale, multicenter studies could provide more robust evidence by increasing the sample size and diversity of patient populations. Collaborative efforts can help validate the findings and enhance the generalizability of the results.
Further research in this field should focus on the following aspects. Future trials should pay attention to this area, expand the sample size, and adopt more rigorous RCT designs including the assessment of adverse effects, to incorporate additional studies in the meta-analysis. Furthermore, a critical aspect of future research should involve a comprehensive cost-effectiveness analysis comparing RA-TLIF with FG-TLIF. This would provide healthcare decision-makers with valuable information regarding the economic implications of adopting robotic technology. Last, Investigating the learning curve for surgeons adopting RA-TLIF is important. Future research should assess how surgeon experience and training impact patient outcomes to ensure safe and effective implementation of this technology.
Conclusion
In TLIF, RA technology demonstrates more accurate placement of pedicle screws compared to FG, offering advantages in protecting adjacent facet joints and reducing intraoperative radiation dosage and blood loss. However, due to longer preoperative preparation time, the surgical duration and radiation time of RA is comparable to FG techniques. Currently, FG screw placement continues to be the predominant technique, and surgeons have greater proficiency in its application. Thus, the integration of RA into TLIF surgery may not be an optimal choice.
Availability of data and materials
All data generated or analyzed during this study are included in this published article or are available from the corresponding author on reasonable request.
References
Harms J, Rolinger H. A one-stager procedure in operative treatment of spondylolistheses: dorsal traction-reposition and anterior fusion (author’s transl) [J]. Z Orthop Ihre Grenzgeb. 1982;120(3):343–7.
Heemskerk JL, Oluwadara AO, Clifton W, et al. Long-term clinical outcome of minimally invasive versus open single-level transforaminal lumbar interbody fusion for degenerative lumbar diseases: a meta-analysis[J]. Spine J. 2021;21(12):2049–65.
Foley KT, Lefkowitz MA. Advances in minimally invasive spine surgery[J]. Clin Neurosurg. 2002;49:499–517.
Lee JC, Jang HD, Shin BJ. Learning curve and clinical outcomes of minimally invasive transforaminal lumbar interbody fusion: our experience in 86 consecutive cases[J]. Spine (Phila Pa 1976). 2012;37(18):1548–57.
Sharif S, Afsar A. Learning curve and minimally invasive spine surgery[J]. World Neurosurg. 2018;119:472–8.
Rampersaud YR, Foley KT, Shen AC, et al. Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion[J]. Spine (Phila Pa 1976). 2000;25(20):2637–45.
Kouyoumdjian P, Gras-Combe G, Grelat M, et al. Surgeon’s and patient’s radiation exposure during percutaneous thoraco-lumbar pedicle screw fixation: A prospective multicenter study of 100 cases[J]. Orthop Traumatol Surg Res. 2018;104(5):597–602.
Passias PG, Brown AE, Alas H, et al. A cost benefit analysis of increasing surgical technology in lumbar spine fusion[J]. Spine J. 2021;21(2):193–201.
Garcia D, Akinduro OO, De Biase G, et al. Robotic-assisted vs nonrobotic-assisted minimally invasive transforaminal lumbar interbody fusion: A cost-utility analysis[J]. Neurosurgery. 2022;90(2):192–8.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement[J]. PLoS Med. 2009;6(7):e1000097.
Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: Cochrane Handbook for Systematic Reviews of Interventions[J]. Cochrane Database Syst Rev. 2019;10(10):D142.
Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo[J]. Spine (Phila Pa 1976). 1990;15(1):11–4.
Babu R, Park JG, Mehta AI, et al. Comparison of superior-level facet joint violations during open and percutaneous pedicle screw placement[J]. Neurosurgery. 2012;71(5):962–70.
Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions[J]. BMJ. 2016;355(12): i4919.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses[J]. BMJ. 2003;327(7414):557–60.
Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis[J]. Biometrics. 2000;56(2):455–63.
Wallace BC, Dahabreh IJ, Trikalinos TA, et al. Closing the gap between methodologists and end-users: R as a computational back end[J]. J Stat Softw. 2012;49:1–15.
Cui GY, Han XG, Wei Y, et al. Robot-assisted minimally invasive transforaminal lumbar interbody fusion in the treatment of lumbar spondylolisthesis[J]. Orthop Surg. 2021;13(7):1960–8.
Chang M, Wang L, Yuan S, et al. Percutaneous endoscopic robot-assisted transforaminal lumbar interbody fusion (pe ra-tlif) for lumbar spondylolisthesis: A technical note and two years clinical results[J]. Pain Physician. 2022;25(1):E73–86.
Schatlo B, Molliqaj G, Cuvinciuc V, et al. Safety and accuracy of robot-assisted versus fluoroscopy-guided pedicle screw insertion for degenerative diseases of the lumbar spine: A matched cohort comparison[J]. J Neurosurg Spine. 2014;20(6):636–43.
Yang JS, He B, Tian F, et al. Accuracy of Robot-assisted percutaneous pedicle screw placement for treatment of lumbar spondylolisthesis: A comparative cohort study[J]. Med Sci Monit. 2019;25:2479–87.
Zhang Q, Han XG, Xu YF, et al. Robot-assisted versus fluoroscopy-guided pedicle screw placement in transforaminal lumbar interbody fusion for lumbar degenerative disease[J]. World Neurosurg. 2019;125:e429–34.
Zhang Q, Xu YF, Tian W, et al. Comparison of superior-level facet joint violations between robot-assisted percutaneous pedicle screw placement and conventional open fluoroscopic-guided pedicle screw placement[J]. Orthop Surg. 2019;11(5):850–6.
Mao JP, Zhang Q, Fan MX, et al. Comparation between robot-assisted and free-hand technique in pedicle screw insertion in transforaminal lumbar interbody fusion surgery: A prospective cohort study[J]. Chinese Journal of Minimally Invasive Surgery. 2019;19(06):481–4.
Jiang SD, Guo H, Liang DH, et al. Primary outcomes of robot-assisted minimally invasive transforaminal lumbar interbody fusion for lumbar degenerative diseases[J]. Orthopedic Journal of China. 2020;28(07):586–91.
Zhao XF, Wang HQ, Gao ZY, et al. Robot assisted minimally invasive transforaminal lumbar interbody fusion for lumbar degenerative disease[J]. Journal of Chinese Practical Diagnosis and Therapy. 2020;34(02):144–7.
Wang TY, Mehta VA, Sankey EW, et al. Operative time and learning curve between fluoroscopy-based instrument tracking and robot-assisted instrumentation for patients undergoing minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF)[J]. Clin Neurol Neurosurg. 2021;206: 106698.
Chen X, Song Q, Wang K, et al. Robot-assisted minimally invasive transforaminal lumbar interbody fusion versus open transforaminal lumbar interbody fusion: a retrospective matched-control analysis for clinical and quality-of-life outcomes[J]. J Comp Eff Res. 2021;10(10):845–56.
De Biase G, Gassie K, Garcia D, et al. Perioperative comparison of robotic-assisted versus fluoroscopically guided minimally invasive transforaminal lumbar interbody fusion[J]. World Neurosurg. 2021;149:e570–5.
Lai YP, Lin YH, Wu YC, et al. Robot-assisted pedicle screw placement led to lower screw loosening rate than fluoroscopy-guided technique in transforaminal lumbar interbody fusion for lumbar degenerative disease: A single-center retrospective study[J]. J Clin Med, 2022,11(17).
Shafi KA, Pompeu YA, Vaishnav AS, et al. Does robot-assisted navigation influence pedicle screw selection and accuracy in minimally invasive spine surgery?[J]. Neurosurg Focus. 2022;52(1):E4.
Hou HT, Shen X, Zhang x, et al. Comparative study between two methods of assisted pedicle screw fixation on minimally invasive surgery transforaminal lumbar interbody fusion[J]. Chinese Journal of Traditional Medical Traumatology & Orthopedics, 2022,30(11):38–43.
Lin MC, Liu HW, Su YK, et al. Robot-guided versus freehand fluoroscopy-guided minimally invasive transforaminal lumbar interbody fusion: a single-institution, observational, case-control study[J]. Neurosurg Focus. 2022;52(1):E9.
Li T, Liu XL, Wang F, et al. Robot-assisted minimally invasive transforaminal lumbar interbody fusion in the treatment of lumbar degenerative diseases: accuracy and safety of screw placement [J]. Chinese Journal of Tissue Engineering Research. 2022;26(36):5812–8.
Wang Z, Sun XG, Li C, et al. Comparison of robot-assisted minimally invasive and freehand open transforaminal lumbar interbody fusion for degenerative lumbar spinal disease: A 2-year follow-up[J]. Journal of Shandong University (Health Sciences). 2023;61(03):97–106.
Wang L, Li C, Wang Z, et al. Comparison of robot-assisted versus fluoroscopy-assisted minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar spinal diseases: 2-year follow-up[J]. J Robot Surg. 2023;17(2):473–85.
Li T, Liao WA, Zhong WJ, et al. Robot-assisted minimally invasive transforaminal lumbar interbody fusion in treatment of lumbar degenerative diseases [J]. Chinese Journal of Tissue Engineering Research. 2023;27(5):1–8.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews[J]. BMJ. 2021;372: n71.
Koc M, Bayar B, Bayar K. A comparison of back pain functional scale with roland morris disability questionnaire, oswestry disability index, and short form 36-health survey[J]. Spine (Phila Pa 1976), 2018,43(12):877–882.
Swanson BT, Creighton D. The degenerative lumbar disc: not a disease, but still an important consideration for OMPT practice: A review of the history and science of discogenic instability[J]. J Man Manip Ther. 2020;28(4):191–200.
Li Y, Dai Y, Wang B, et al. Full-endoscopic posterior lumbar interbody fusion via an interlaminar approach versus minimally invasive transforaminal lumbar interbody fusion: A preliminary retrospective study[J]. World Neurosurg. 2020;144:e475–82.
Derman PB, Albert TJ. Interbody fusion techniques in the surgical management of degenerative lumbar spondylolisthesis[J]. Curr Rev Musculoskelet Med. 2017;10(4):530–8.
Mobbs RJ, Phan K, Malham G, et al. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF[J]. J Spine Surg. 2015;1(1):2–18.
Haws BE, Khechen B, Narain AS, et al. Iliac crest bone graft for minimally invasive transforaminal lumbar interbody fusion: A prospective analysis of inpatient pain, narcotics consumption, and costs[J]. Spine (Phila Pa 1976), 2018,43(18):1307–1312.
McDonnell JM, Ahern DP, Doinn TÓ, et al. Surgeon proficiency in robot-assisted spine surgery[J]. Bone Joint J, 2020,102-B(5):568–572.
Fu W, Tong J, Liu G, et al. Robot-assisted technique vs conventional freehand technique in spine surgery: A meta-analysis[J]. Int J Clin Pract. 2021;75(5): e13964.
Joseph JR, Smith BW, Liu X, et al. Current applications of robotics in spine surgery: A systematic review of the literature[J]. Neurosurg Focus. 2017;42(5):E2.
Liu H, Chen W, Wang Z, et al. Comparison of the accuracy between robot-assisted and conventional freehand pedicle screw placement: A systematic review and meta-analysis[J]. Int J Comput Assist Radiol Surg. 2016;11(12):2273–81.
Ringel F, Stuer C, Reinke A, et al. Accuracy of robot-assisted placement of lumbar and sacral pedicle screws: A prospective randomized comparison to conventional freehand screw implantation[J]. Spine (Phila Pa 1976), 2012,37(8):E496-E501.
Molliqaj G, Schatlo B, Alaid A, et al. Accuracy of robot-guided versus freehand fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery[J]. Neurosurg Focus. 2017;42(5):E14.
Macke JJ, Woo R, Varich L. Accuracy of robot-assisted pedicle screw placement for adolescent idiopathic scoliosis in the pediatric population[J]. J Robot Surg. 2016;10(2):145–50.
Perdomo-Pantoja A, Ishida W, Zygourakis C, et al. Accuracy of current techniques for placement of pedicle screws in the spine: A comprehensive systematic review and meta-analysis of 51,161 screws[J]. World Neurosurg. 2019;126:664–78.
Li HM, Zhang RJ, Shen CL. Accuracy of pedicle screw placement and clinical outcomes of robot-assisted technique versus conventional freehand technique in spine surgery from nine randomized controlled trials: A meta-analysis[J]. Spine (Phila Pa 1976), 2020,45(2):E111-E119.
Zhou LP, Zhang RJ, Li HM, et al. Comparison of cranial facet joint violation rate and four other clinical indexes between robot-assisted and freehand pedicle screw placement in spine surgery: A meta-analysis[J]. Spine (Phila Pa 1976), 2020,45(22):E1532-E1540.
Bagheri SR, Alimohammadi E, Zamani FA, et al. Adjacent segment disease after posterior lumbar instrumentation surgery for degenerative disease: Incidence and risk factors[J]. J Orthop Surg (Hong Kong). 2019;27(2):615502666.
Teles AR, Paci M, Gutman G, et al. Anatomical and technical factors associated with superior facet joint violation in lumbar fusion[J]. J Neurosurg Spine. 2018;28(2):173–80.
Sakaura H, Ikegami D, Fujimori T, et al. Early cephalad adjacent segment degeneration after posterior lumbar interbody fusion: A comparative study between cortical bone trajectory screw fixation and traditional trajectory screw fixation[J]. J Neurosurg Spine. 2019;32(2):155–9.
Levin JM, Alentado VJ, Healy AT, et al. Superior segment facet joint violation during instrumented lumbar fusion is associated with higher reoperation rates and diminished improvement in quality of life[J]. Clin Spine Surg. 2018;31(1):E36–41.
Hyun SJ, Kim KJ, Jahng TA, et al. Minimally invasive robotic versus open fluoroscopic-guided spinal instrumented fusions: A randomized controlled trial[J]. Spine (Phila Pa 1976), 2017,42(6):353–358.
Archavlis E, Amr N, Kantelhardt SR, et al. Rates of upper facet joint violation in minimally invasive percutaneous and open instrumentation: A comparative cohort study of different insertion techniques[J]. J Neurol Surg A Cent Eur Neurosurg. 2018;79(1):1–8.
Grelat M, Zairi F, Quidet M, et al. Assessment of the surgeon radiation exposure during a minimally invasive TLIF: comparison between fluoroscopy and O-arm system[J]. Neurochirurgie. 2015;61(4):255–9.
Yu E, Khan SN. Does less invasive spine surgery result in increased radiation exposure? A systematic review[J]. Clin Orthop Relat Res. 2014;472(6):1738–48.
Roser F, Tatagiba M, Maier G. Spinal robotics: current applications and future perspectives[J]. Neurosurgery. 2013;72(Suppl 1):12–8.
Schizas C, Thein E, Kwiatkowski B, et al. Pedicle screw insertion: robotic assistance versus conventional C-arm fluoroscopy[J]. Acta Orthop Belg. 2012;78(2):240–5.
Acknowledgements
The authors would like to thank the database search support.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JBG and KTY designed the systematic review. JBG and NNF drafted the protocol and KTY revised the manuscript. GJB and NNF will independently screen the potential studies, extract data, assess the risk of bias and finish data synthesis. GJB and KTY will arbitrate any disagreements during the review. Xing Yu revised English language of the manuscript. All authors approved the publication of the protocol. JBG is the first author and KTY is corresponding author.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guan, J., Feng, N., Yu, X. et al. Comparison of robot-assisted versus fluoroscopy-guided transforaminal lumbar interbody fusion (TLIF) for lumbar degenerative diseases: a systematic review and meta-analysis of randomized controlled trails and cohort studies. Syst Rev 13, 170 (2024). https://doi.org/10.1186/s13643-024-02600-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02600-6