
Abstract
Background
Chronic ankle instability (CAI) is a common yet serious problem for elder patients. This meta-analysis aimed to evaluate the effects of balance training for CAI, to provide evidence for the clinical treatment, and care of CAI patients.
Methods
Two investigators searched PubMed, EMBASE, Science Direct, Web of Science, Cochrane Library, China National Knowledge Infrastructure, Wanfang, and Weipu Databases up to May 20, 2023, for randomized controlled trials (RCTs) on the effects of balance training for CAI. The mean difference (MD) with 95% confidence intervals (95%CIs) was calculated for each outcome with a fixed or random effect model. Review Manager 5.3 software was used for meta-analysis.
Results
Nine RCTs involving 341 patients were included. Meta-analysis results showed that compared with blank controls, balanced training treatment of CAI could significantly improve the score of CAI [MD = 3.95, 95% CI (3.26, 4.64), P < 0.00001], SEBT-PM [MD = 4.94, 95% CI (1.88, 8.00), P = 0.002], SEBT-PL [MD = 5.19, 95% CI (1.57, 8.81), P = 0.005], and FAAM Sports [MD = 17.74, 95% CI (14.36, 21.11), P < 0.00001]. Compared with strength training, balance training treatment of CAI improved the score of CAIT [MD = 2.36, 95% CI (0.29, 4.44), P = 0.03], FAAM-ADL [MD = 4.06, 95% CI (1.30, 6.83), P = 0.004].
Conclusion
The analysis outcomes indicate that balance training enhances daily activity capability, motor function, and dynamic balance to different extents. Additionally, when comparing the results of balance training and strength training, no significant difference was observed between the two methods in improving the dynamic stability of CAI patients. However, it is noteworthy that balance training exhibits a more pronounced impact on enhancing functional scale scores.
Similar content being viewed by others


Background
Ankle joint injury is an important medical care problem. Ankle sprains affect about 8% of the general population, and the recurrence rate is as high as 80% in patients engaging in high-risk sports [1, 2]. A previous study [3] has reported that 40%-55% of patients still have residual symptoms of ankle joint six months after the occurrence of ankle sprain. Lateral ankle instability refers to the injury of the lateral ligament caused by excessive supination of the ankle or varus of the hind foot and the continued development of residual symptoms [4]. Chronic ankle instability (CAI) refers to the instability of the lateral ankle joint caused by repeated ankle sprains. Patients with CAI may have obstacles in proprioception, neuromuscular control, strength, and posture control alone or simultaneously [5, 6].
For CAI patients, conservative treatment is the first choice. After active conservative treatment, if the symptoms still do not improve, surgical treatment can be attempted [7]. The surgical treatment is usually the repair or reconstruction of ankle ligaments, for the purpose of strengthening the stability of the ankle joint and avoiding sprain again [8]. Postoperative rehabilitation methods for CAI include physical therapy, strength training, joint range of motion training, balance training, proprioception training, gait training, etc. Previous studies [9, 10] have shown that early and standardized rehabilitation after CAI can avoid and improve ankle joint range of motion limitation, proprioception, muscle strength, balance ability decline, gait abnormalities, and other dysfunctions.
Balance training refers to rehabilitation training aimed at restoring or improving body balance ability. It includes static balance training, dynamic balance training, reactive balance training, sensory integration balance training, and functional activity balance training [11]. The Cumberland Ankle Instability Tool (CAIT), Foot and Ankle Ability Measure ADL (FAAM-ADL), Foot and Ankle Ability Measure Sports (FAAM Ports), and Star Deviation Balance Test (SEBT) are commonly used tools for the evaluation of the effects of balance training. Previous studies [12, 13] have shown the effectiveness of balance training for sensory-motor and functional activities of CAI patients in terms of function, stability, strength, joint range of motion, balance, and other aspects. However, some studies [14, 15] have shown that balance training is not superior to other conservative treatments in terms of self-reported function, ankle strength, balance ability, and range of motion of CAI patients. The effectiveness of balance training on functional recovery of CAI patients is still controversial among the findings of related studies, and the related reports focused on the role of balance training in CAI patients are few. Therefore, the purpose of this systematic review and meta-analysis is to comprehensively and quantitatively analyze the available evidence and compare the role of balance training in self-reported function and dynamic balance stability, to provide reliable evidence for the clinical treatment of CAI.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodological review framework was used in this systematic review and meta-analysis to ensure systematic data collection and analysis of literature [16].
Inclusion and exclusion criteria
The inclusion criteria were as follows: the study design was a randomized controlled trial (RCT). The study population was patients with chronic ankle instability (CAI), including functional ankle instability (FAI) and mechanical ankle instability (MAI). The experimental group used balance training as the intervention method. The balance training included static balance training, dynamic balance training, reactive balance training, sensory integration balance training, and functional activity balance training. The control group used unbalanced training as the intervention method, including no intervention and strength training. The outcome indicators shall at least include one of the CAIT, FAAM-ADL, FAAM Ports, and SEBT. This meta-analysis excluded the repetitively reported literature and the studies reported in languages other than Chinese and English.
Search strategy
Two investigators searched PubMed, EMBASE, Science Direct, Web of Science, Cochrane Library, China National Knowledge Infrastructure, Wanfang, and Weipu Databases. The two investigators accessed the databases simultaneously. The retrieval time limit was between the establishment of the database and May 20, 2023. The Medical Subject Headings (MeSH) terms used for the literature search were as follows: (“ankle instability” OR “recurrent ankle sprain” OR “chronic ankle instability” OR “chronic lateral ankle instability” OR “CAI” OR “CLAI” OR “functional ankle instability") AND (“balance”) AND (“rehabilitation” OR “physical therapy” OR “health management” OR “physiotherapy” OR “exercise” OR “training”). We adapted the search strategy in different databases to retrieve the relevant studies. The references in the reference lists of potentially included reports were screened to identify additional articles that might meet the inclusion criteria.
Literature screening and data extraction
According to the title and abstract of the literature, the two researchers independently completed the preliminary screening of the literature. After removing the duplicate literature, they searched and read the original text, and screened the literature that met the inclusion criteria for the second time. Any disagreements between reviewers during the screening process were submitted to a third reviewer and discussed collectively. The data extracted in this meta-analysis included the name of the first author, publication time, sample size, age, duration, frequency, and intensity of the intervention and the related outcomes such as CAIT, FAAM-ADL, FAAM Ports, and SEBT.
Quality evaluation
Two researchers independently evaluated the methodologic quality using the Physiotherapy Evidence Database (PEDro) scale [17]. If agreement in an RCT’s score was not achieved, the authors discussed and came to a consensus on a score. The choice of the PEDro scale over other bias assessment tools recommended for RCTs was deliberate. The PEDro scale is widely recognized and specifically designed for the quality evaluation of RCTs related to physiotherapy. We believed that the PEDro scale was more targeted and appropriate for our specific context.
Statistical analysis
We used Review Manager 5.3 (RevMan 5.3) [18] for meta-analysis. Continuity variables were expressed by mean difference (MD) and 95% confidence interval (CI). A chi-square test was used to judge the difference among the included RCTs. When the P > 0.05, I2 < 50%, there was homogeneity in the results. When P ≤ 0.05 and I2 ≥ 50% indicated that the results were heterogeneous. A fixed effect model was used for homogeneous data, and the random effect model was used for heterogeneous data. Publication bias was assessed by funnel plots and the Egger regression test in this meta-analysis. Funnel plot, a simple scatter plot of the intervention effect estimates from each study, was plotted against some measure of each study’s size or precision. Ten or more studies were required for the significant evidence of funnel plot. Further, we conducted sensitivity analyses to identify the influence of a single study on the whole synthesized results. P < 0.05 indicated that the difference was statistically significant.
Results
Study inclusion
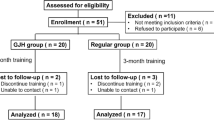
A total of 224 reports were obtained from the initial database searches. After the removal of duplicates, 192 reports were screened, and 175 reports were excluded after the first screening of the title and abstract, thus 17 reports were further included for full-text screening. According to the inclusion and exclusion criteria, nine RCTs [19,20,21,22,23,24,25,26,27] were finally included in this meta-analysis. The PRISMA flowchart of study selection is presented in Fig. 1.

PRISMA flow diagram of RCT inclusion
Characteristics and quality of included RCTs
The characteristics of the included studies are presented in Table 1. Of the included RCTs, 341 patients were involved, and 165 patients underwent balance training. There are eight groups of “balance training versus no intervention” trials and two groups of “balance training versus strength training” trials. The outcome indicators of the study included seven groups of CAIT, three groups of FAAM, and seven groups of SEBT.
The PEDro scores for the quality of the included studies are presented in Table 2. There were three RCTs with 7 points, five RCTs with 6 points, and one RCT with 5 points.
Five RCTs reported the CAIT after the intervention, including 202 patients. There was homogeneity (I2 = 0%, P = 0.76), and the fixed effect model was used. Meta-analysis results showed that compared with the blank control group (controls without interventions), the CAI score of the balance training group was significantly improved [MD = 3.95, 95% CI (3.26, 4.64), P < 0.001, Fig. 2a].

The forest plots for CAIT, FAAM-ADL, FAAM-Sports, and SEBT-A compared to black control
Two RCTs reported the FAAM-ADL after the intervention, including 70 patients. There was heterogeneity (I2 = 85%, P = 0.001), and the random effect model was used. Meta-analysis results showed that there was no significant difference in the FAAM-ADL score between the balance training group and the blank control group [MD = 8.28, 95% CI(− 3.49, 20.05), P = 0.17, Fig. 2b].
Two RCTs reported the FAAM-Sports after the intervention, including 70 patients. There was homogeneity (I2 = 48%, P = 0.16), and the fixed effect model was used. Meta-analysis results showed that compared with the blank control group, the FAAM- Sports score of the balance training group was significantly improved [MD = 17.74, 95% CI(14.36, 21.11), P < 0.001, Fig. 2c].
Five RCTs reported the SEBT-A after the intervention, including 195 patients. There was heterogeneity (I2 = 94%, P < 0.001), and the random effect model was used. Meta-analysis results showed that there was no significant difference in the SEBT-A score between the balance training group and the blank control group [MD = 4.05, 95% CI (− 1.64, 9.75), P = 0.16, Fig. 2d].
Three RCTs reported the SEBT-AM after the intervention, including 88 patients. There was heterogeneity (I2 = 51%, P < 0.001), and the random effect model was used. Meta-analysis results showed that there was no significant difference in the SEBT-AM score between the balance training group and the blank control group [MD = 1.05, 95% CI (− 1.73, 3.84), P = 0.46, Fig. 3a].

The forest plots for SEBT-AM, SEBT-M, SEBT-PL, and SEBT-PM compared to black control
Three RCTs reported the SEBT-M after the intervention, including 89 patients. There was heterogeneity (I2 = 84%, P = 0.002), and the random effect model was used. Meta-analysis results showed that there was no significant difference in the SEBT-M score between the balance training group and the blank control group [MD = 4.06, 95% CI(− 1.53, 9.64), P = 0.15, Fig. 3b].
Four RCTs reported the SEBT-PL after the intervention, including 173 patients. There was homogeneity (I2 = 81%, P = 0.001), and the random effect model was used. Meta-analysis results showed that compared with the blank control group, the SEBT-PL score of the balance training group was significantly improved [MD = 5.19, 95% CI (1.57, 8.81), P = 0.005, Fig. 3c].
Six RCTs reported the SEBT-PM after the intervention, including 229 patients. There was heterogeneity (I2 = 94%, P < 0.001), and the random effect model was used. Meta-analysis results showed that compared with the blank control group, the SEBT-PM score of the balance training group was significantly improved [MD = 4.94, 95% CI(1.88, 8.00), P = 0.002, Fig. 3d].
Two RCTs reported the CAIT after the intervention between the balance training group and the strength training group, including 61 patients. There was homogeneity (I2 = 0%, P = 0.55), and the fixed effect model was used. Meta-analysis results showed that compared with the strength training group, the CAI score of the balance training group was significantly improved [MD = 2.36, 95% CI (0.29, 4.44), P = 0.03, Fig. 4a].

The forest plots for CAIT, FAAM-ADL, FAAM-Sports, and SEBT-PM compared to strength training
Two RCTs reported the FAAM-ADL after the intervention between the balance training group and the strength training group, including 61 patients. There was homogeneity (I2 = 0%, P = 0.81), and the fixed effect model was used. Meta-analysis results showed that compared with the strength training group, the FAAM-ADL score of the balance training group was significantly improved. [MD = 4.06, 95% CI (1.30, 6.83), P = 0.004, Fig. 4b].
Two RCTs reported the FAAM-Sports after the intervention between balance the training group and the strength training group, including 61 patients. There was homogeneity (I2 = 0%, P = 0.73), and the fixed effect model was used. Meta-analysis results showed that there was no significant difference in the FAAM-Sports score between the balance training group and the strength training group [MD = 5.00, 95% CI (− 0.38, 10.39), P = 0.07, Fig. 4c].
Two RCTs reported the SEBT-PM after the intervention between the balance training group and the strength training group, including 61 patients. There was homogeneity (I2 = 0%, P = 0.95), and the fixed effect model was used. Meta-analysis results showed that there was no significant difference in the SEBT-PM score between the balance training group and the strength training group [MD = 0.03, 95% CI (− 0.02, 0.08), P = 0.24, Fig. 4d].
We conducted a subgroup analysis based on the duration and frequency and intensity of balance training to evaluate the homogeneity, the synthesized outcomes did not change statistically (all P > 0.05).
Publication bias
Limited by as number of included studies, we could not perform a funnel plot. Regression analyses on the synthesized outcomes indicated that there was no publication bias (all P > 0.05).
Sensitivity analysis
We systematically excluded RCTs for each individual result to assess whether the overall outcomes were affected. Our investigation revealed that the overall results remained unchanged regardless of excluding any specific RCT.
Discussions
Balance is the ability to maintain a stable state of the body by resisting forces that interfere with the body [28]. The performance of impaired postural control and decreased postural stability in CAI patients may be caused by proprioception loss or neuromuscular control deficiency [29,30,31]. Therefore, improving the balance function of CAI patients can improve the functional activity of the affected ankle and reduce the risk of sprain again [32, 33]. The results of this analysis have shown that balance training improves daily activity ability, motor function, and dynamic balance to varying degrees. At the same time, comparing the results of balance training and strength training shows that there is no significant difference between the two training methods in improving the dynamic stability of CAI patients, while balance training has a more significant effect in improving the score of the functional scale.
CAIT is a scale to evaluate the existence and severity of ankle instability [34, 35]. Our results have shown that the stability of self-perception of CAI patients is improved after balance training. There is no significant heterogeneity between the research results of the CAIT questionnaire, but due to the insufficient number of included studies, more high-quality studies are needed. Activities of daily living and motor function can effectively reflect the activity and participation ability of patients [36,37,38]. FAAM is a very widely used scale to evaluate the functional activity ability caused by ankle joint-related injuries of lower limbs, which includes two self-assessment scales for the activity function in daily life and during exercise [39, 40]. For these two indicators, this study included two reports. Our meta-analysis results have shown that, compared with the control group that does not receive any intervention, the FAAM-ADL scores of CAI patients in the balance training group do not show significant differences, but the ability of sports activities is significantly improved. This may be because the impact of CAI proprioception damage on daily life was less than that of sports activities. At the same time, the ceiling effect of FAAM-ADL may also be one of the reasons why this analysis failed to draw significant differences, and the insufficient number of included studies is also worth considering.
SEBT can quantitatively measure changes in dynamic posture control and balance stability and can be used as an effective tool to measure patients’ dynamic balance [41,42,43]. Dynamic balance refers to the ability of the center of gravity to maintain the stability and direction of the body and posture during physical activities [44]. In daily life and various sports activities, the human body must constantly change the support plane and constantly adjust the body posture to meet the needs of balance [45, 46]. In SEBT, there are 5 directions (A front lateral, AM front medial, M medial, PM rear medial, and PL rear lateral) for analysis and comparison [47]. For the star bias test, SEBT-A, SEBT-AM, and SEBT-M were included in 5, 3, and 3 studies respectively. The results showed that there was no significant difference in the improvement of the stability of dynamic shift balance in each direction of the front side of the CAI patients in the test group who used balance training as an intervention method. Considerable heterogeneity was observed among the studies, potentially stemming from inadequate sample sizes, inconsistent baselines, varying intervention methods, and other factors. The results also substantiated a significant enhancement in the effectiveness of balance training on these two sets of indicators in both groups.
The analysis results show that balance training has advantages over strength training in improving the CAI and FAAM-ADL scores of CAIT patients, while there is no significant difference in improving FAAM Ports. This may be because CAI patients cannot resume all physiological activities to perform difficult tasks such as sports, even though some studies have shown that balance training is better than strength training in this respect [48, 49]. In the eight directions of the star bias test SEBT, only PM was included in more than one report. The results have shown that there is no significant difference between balance training and strength training in improving the dynamic stability of patients, which may be associated with the inconsistent baseline level between studies.
Some limitations of this meta-analysis are worth considering. Firstly, the number of included RCTs is small, and the sample size of included experimental studies is small. Secondly, the patients’ baseline levels were inconsistent and the training methods and parameters were different. Finally, some studies have not clearly pointed out the specific method of random allocation, whether the allocation method is hidden, and the implementation of blind methods for study populations. The quality of research methods included in the literature is different, leading to greater heterogeneity between various studies, which ultimately leads to the reduction of the credibility of research results. Future studies should be designed with more specific types of balance or strength interventions to determine appropriate and personalized exercise types, long-term prognosis, and patient compliance. At the same time, a comparison of baseline levels among included patients and an expansion of sample size should be added to increase the reliability of research results.
Conclusions
In conclusion, the results of this meta-analysis have shown that balance training is beneficial to improve the daily living and sports ability of CAI patients, as well as the dynamic stability of the ankle joint on the posterior side. However, there is still disunity in the training methods, intensity, frequency, and duration of balance training, and there is still no standardized and specific balance training program for CAI patients. The development of a more specific balance training program can be one of the future research directions. Besides, high-quality research with a larger sample size on these issues in the future is needed in the future.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CAI:
-
Chronic ankle instability
- RCTs:
-
Randomized controlled trials
- MD:
-
Mean difference
- CI:
-
Confidence interval
- MeSH:
-
Medical Subject Headings
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- CAIT:
-
Cumberland Ankle Instability Tool
- FAAM-ADL:
-
Foot and Ankle Ability Measure ADL
- FAAM-Sports:
-
Foot and Ankle Ability Measure Sports
- SEBT:
-
Star Excursion Balance Test
References
Tee E, Melbourne J, Sattler L, Hing W. Evidence for rehabilitation interventions after acute lateral ankle sprains in athletes: a scoping review. J Sport Rehabil. 2022;31(4):457–64.
Drakos M, Hansen O, Kukadia S. Ankle instability. Foot Ankle Clin. 2022;27(2):371–84.
Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19(10):653–60.
Gopinath R, Pigott M, Lindsey B, Finney FT, Holmes JR, Walton DM, Talusan PG. Medial ankle instability: review of anatomy, evaluation, and treatment. Foot Ankle Spec. 2022. https://doi.org/10.1177/1938640021992915.
Liu K, Delaney AN, Kaminski TW. A review of the role of lower-leg strength measurements in ankle sprain and chronic ankle instability populations. Sports Biomech. 2022;21(4):562–75.
Chan LYT, Sim YTN, Gan FK, Binabdrazak HR. Effect of chronic ankle instability on lower extremity kinematics, dynamic postural stability, and muscle activity during unilateral jump-landing tasks: a systematic review and meta-analysis. Phys Ther Sport. 2022;55:176–88.
Picot B, Hardy A, Terrier R, Tassignon B, Lopes R, Fourchet F. Which functional tests and self-reported questionnaires can help clinicians make valid return to sport decisions in patients with chronic ankle instability? A narrative review and expert opinion. Front Sports Act Living. 2022;4:902886.
Lin CI, Mayer F, Wippert PM. The prevalence of chronic ankle instability in basketball athletes: a cross-sectional study. BMC Sports Sci Med Rehabil. 2022;14(1):27.
Kim H, Moon S. Effect of joint mobilization in individuals with chronic ankle instability: a systematic review and meta-analysis. J Funct Morphol Kinesiol. 2022;7(3):66.
Goodrich E, Vopat B, Herda A. Treatment of chronic ankle instability in the military population: a systematic review. Foot Ankle Spec. 2022;25:19386400211068239.
Emirzeoglu M, Ulger O. The acute effects of cognitive-based neuromuscular training and game-based training on the dynamic balance and speed performance of healthy young soccer players: a randomized controlled trial. Games Health J. 2021;10(2):121–9.
O’Driscoll J, Delahunt E. Neuromuscular training to enhance sensorimotor and functional deficits in subjects with chronic ankle instability: a systematic review and best evidence synthesis. Sports Med Arthrosc Rehabil Ther Technol. 2011;3:19.
Loudon JK, Santos MJ, Franks L, Liu W. The effectiveness of active exercise as an intervention for functional ankle instability: a systematic review. Sports Med. 2008;38(7):553–63.
Cruz AL, Oliveira R, Silva AG. Exercise-based interventions for physically active individuals with functional ankle instability: a systematic review of the literature. J Sports Med Phys Fitness. 2019;59(4):666–75.
Kim K, Choi B, Lim W. The efficacy of virtual reality assisted versus traditional rehabilitation intervention on individuals with functional ankle instability: a pilot randomized controlled trial. Disabil Rehabil Assist Technol. 2019;14(3):276–80.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Moseley AM, Elkins MR, Van der Wees PJ, Pinheiro MB. Using research to guide practice: The Physiotherapy Evidence Database (PEDro). Braz J Phys Ther. 2020;24(5):384–91.
Pati D, Lorusso LN. How to write a systematic review of the literature. HERD. 2018;11(1):15–30.
Cain MS, Ban RJ, Chen YP, Geil MD, Goerger BM, Linens SW. Four-week ankle-rehabilitation programs in adolescent athletes with chronic ankle instability. J Athl Train. 2020;55(8):801–10.
Cain MS, Garceau SW, Linens SW. Effects of a 4-week biomechanical ankle platform system protocol on balance in high school athletes with chronic ankle instability. J Sport Rehabil. 2017;26(1):1–7.
Cruz-Diaz D, Lomas-Vega R, Osuna-Perez MC, Contreras FH, Martinez-Amat A. Effects of 6 weeks of balance training on chronic ankle instability in athletes: a randomized controlled trial. Int J Sports Med. 2015;36(9):754–60.
Kim KM, Estudillo-Martinez MD, Castellote-Caballero Y, Estepa-Gallego A, Cruz-Diaz D. Short-term effects of balance training with stroboscopic vision for patients with chronic ankle instability: a single-blinded randomized controlled trial. Int J Environ Res Public Health. 2021;18(10):11–4.
Liang Y, Gao M, Wang P. The efficacy of dynamic and static balance training in the treatment of chronic ankle instability. Chinese J Gerontol Rehabil. 2015;1(2):23–7.
Linens SW, Ross SE, Arnold BL. Wobble board rehabilitation for improving balance in ankles with chronic instability. Clin J Sport Med. 2016;26(1):76–82.
Shih YF, Yu HT, Chen WY, Liao KK, Lin HC, Yang YR. The effect of additional joint mobilization on neuromuscular performance in individuals with functional ankle instability. Phys Ther Sport. 2018;30:22–8.
Sierra-Guzman R, Jimenez-Diaz F, Ramirez C, Esteban P, Abian-Vicen J. Whole-body-vibration training and balance in recreational athletes with chronic ankle instability. J Athl Train. 2018;53(4):355–63.
Wright CJ, Linens SW, Cain MS. A randomized controlled trial comparing rehabilitation efficacy in chronic ankle instability. J Sport Rehabil. 2017;26(4):238–49.
Marcori AJ, Monteiro PHM, Oliveira JA, Doumas M, Teixeira LA. Single leg balance training: a systematic review. Percept Mot Skills. 2022;129(2):232–52.
Ziaei Ziabari E, Haghpanahi M, Razi M, Lubberts B, Ashkani-Esfahani S, DiGiovanni CW. The effects of chronic ankle instability on the biomechanics of the uninjured, contralateral ankle during gait. Orthop Surg. 2022;14(9):2238–44.
Nakasa T, Ikuta Y, Sumii J, Nekomoto A, Adachi N. Characteristics of chronic ankle instability requiring both anterior talofibular and calcaneofibular ligament repair. J Foot Ankle Surg. 2022;61(5):1028–33.
Xu Y, Song B, Ming A, Zhang C, Ni G. Chronic ankle instability modifies proximal lower extremity biomechanics during sports maneuvers that may increase the risk of ACL injury: A systematic review. Front Physiol. 2022;13:1036267.
Zarei H, Norasteh AA. Effects of exercise training programs on balance of blind children and adolescents: a systematic review and meta-analysis. J Bodyw Mov Ther. 2022;30:187–95.
Lu Z, Zhou L, Gong W, Chuang S, Wang S, Guo Z, Bao D, Zhang L, Zhou J. The effect of 6-week combined balance and plyometric training on dynamic balance and quickness performance of elite badminton players. Int J Environ Res Public Health. 2022;19(3):1605.
Hiller CE, Refshauge KM, Bundy AC, Herbert RD, Kilbreath SL. The Cumberland ankle instability tool: a report of validity and reliability testing. Arch Phys Med Rehabil. 2006;87(9):1235–41.
Cruz-Diaz D, Hita-Contreras F, Martinez-Amat A, Aibar-Almazan A, Kim KM. Ankle-joint self-mobilization and crossfit training in patients with chronic ankle instability: a randomized controlled trial. J Athl Train. 2020;55(2):159–68.
Kim KM, Estepa-Gallego A, Estudillo-Martinez MD, Castellote-Caballero Y, Cruz-Diaz D. Comparative effects of neuromuscular- and strength-training protocols on pathomechanical, sensory-perceptual, and motor-behavioral impairments in patients with chronic ankle instability: randomized controlled trial. Healthcare (Basel). 2022;10(8):1364.
Forsyth L, Bonacci J, Childs C. A pilot randomised control trial of the efficacy of stability-based training with visualisation for people with chronic ankle instability. Med Biol Eng Comput. 2022;60(4):1199–209.
Driedger MR, Groeschl R, Yohanathan L, Starlinger P, Grotz TE, Smoot RL, Nagorney DM, Cleary SP, Kendrick ML, Truty MJ. Finding the balance: general surgery resident versus fellow training and exposure in hepatobiliary and pancreatic surgery. J Surg Educ. 2021;78(3):875–84.
Martin RL, Irrgang JJ, Burdett RG, Conti SF, Van Swearingen JM. Evidence of validity for the Foot And Ankle Ability Measure (FAAM). Foot Ankle Int. 2005;26(11):968–83.
Eechaute C, Vaes P, Van Aerschot L, Asman S, Duquet W. The clinimetric qualities of patient-assessed instruments for measuring chronic ankle instability: a systematic review. BMC Musculoskelet Disord. 2007;8:6.
Gribble PA, Hertel J, Plisky P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train. 2012;47(3):339–57.
Powden CJ, Dodds TK, Gabriel EH. The reliability of the star excursion balance test and lower quarter Y-balance test in healthy adults: a systematic review. Int J Sports Phys Ther. 2019;14(5):683–94.
Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36(12):911–9.
Gusi N, Carmelo Adsuar J, Corzo H, Del Pozo-Cruz B, Olivares PR, Parraca JA. Balance training reduces fear of falling and improves dynamic balance and isometric strength in institutionalised older people: a randomised trial. J Physiother. 2012;58(2):97–104.
Liu M, Han J, Mei Y, Li Y. Dynamic balance between demand-and-supply of urban taxis over trajectories. Math Biosci Eng. 2022;19(1):1041–57.
Ozmen T, Gunes M, Simsek A, Inceoglu F. Reliability of the modified star excursion balance test in individuals with down syndrome. J Bodyw Mov Ther. 2022;32:171–5.
Sogut B, Harput G, Tunay VB. Star excursion balance test scores under different conditions: effects of arms position and shoe-wear. J Bodyw Mov Ther. 2022;30:17–22.
O’Neil JT, Plummer OR, Raikin SM. Application of computerized adaptive testing to the foot and ankle ability measure. Foot Ankle Int. 2021;42(1):2–7.
Nixon DC, McCormick JJ, Johnson JE, Klein SE. PROMIS pain interference and physical function scores correlate with the Foot and Ankle Ability Measure (FAAM) in patients with hallux valgus. Clin Orthop Relat Res. 2017;475(11):2775–80.
Acknowledgements
None.
Funding
This study was funded by Shanghai Municipal Health Commission Health Industry Clinical Research Special Project (202240250), China Disabled Persons Federation special projects of assistive products for the disabled (2022CDPFAT-15) and Shanghai Municipal Science and Technology Major Project (2021SHZDZX0100).
Author information
Authors and Affiliations
Contributions
TW designed research. YG, TC, ZY, YH, ML, and TW conducted research. YG, TC, and ZY analyzed data. YG and TW wrote the first draft of the manuscript. YG and TW had primary responsibility for the final content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In this study, all methods were performed in accordance with the relevant guidelines and regulations. Ethical approval, consent to participate, and written informed consent were not necessary since our study was a meta-analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, Y., Cheng, T., Yang, Z. et al. A systematic review and meta-analysis of balance training in patients with chronic ankle instability. Syst Rev 13, 64 (2024). https://doi.org/10.1186/s13643-024-02455-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02455-x