
Abstract
Background
Dual-task training has been a popular intervention for individuals with balance impairments. However, the effects of dual-task training on chronic ankle instability (CAI) have not been comprehensively analyzed and reliable clinical evidence is scarce. The purpose of this systematic review and meta-analysis is to evaluate the effectiveness of dual-task training on postural stability and functional ability in individuals with CAI.
Methods
PubMed, Web of Science, EBSCO, Cochrane Library, Physiotherapy Evidence Database (PEDro), and China National Knowledge Infrastructure (CNKI) were researched from inception to November 2022. This study was conducted by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two reviewers assessed the studies for inclusion and extracted data. The Cochrane Risk of Bias list was used to assess the risk of bias in included studies. Mean differences (MD) with a 95% confidence interval (CI) were calculated with the RevMan 5.3 software.
Results
A total of 7 randomized controlled trials with 192 CAI met the inclusion criteria. The meta-analysis results showed that compared with the control group, dual-task training significantly improved the Y-balance test (MD = 1.60, 95% CI: −0.00 to 3.21, P = 0.050) and reduced COP-area (MD = − 0.94, 95% CI: −1.62 to − 0.26, P = 0.007) in individuals with CAI. However, there is no significant difference between dual-task training and the control group on COP-velocity (MD = − 0.26, 95% CI: −0.70 to 0.17, P = 0.240), hop test (MD = − 0.20, 95% CI: −0.66 to 0.26, P = 0.386) and BESS (MD = − 1.24, 95% CI: −2.95 to 0.48, P = 0.157) in individuals with CAI.
Conclusion
This meta-analysis showed that dual-task training may be effective in improving static and dynamic postural stability. However, more high-quality randomized controlled trials are needed to verify the short and long-term effectiveness of dual-task training on CAI.
Similar content being viewed by others

Introduction
Chronic ankle instability (CAI) is categorized into functional (FAI) and mechanical (MAI) instability and is characterized by symptoms of giving way, pain, and recurrent sprains. Following their first ankle sprain, 40% of people will develop CAI, which can result in static or dynamic postural instability and dysfunction [1]. Both automatic and cognitive control are involved in the process of postural stability and functional ability [2]. According to research, any reduction in conscious-controlled attention toward postural control increases the possibility of disturbing coordination and stability, presumably as a result of movement-specific reinvestment. Based on the notion of reinvestment, control movement performance might be affected by attention distraction [3]. Meanwhile, a theory based on the competition for cross-domain resources hypothesizes that limited cognitive resources are available for the management of maintaining postural stability and performing cognitive tasks, potentially resulting in a decline in postural stability, cognitive task performance, or both, when the two tasks are performed at the same time [4,5,6]. The constrained action hypothesis postulates that attentional shifts might enable motor systems to operate automatically, leading to more efficient performance [7]. Some studies [8, 9] found that dual-task training improved balance and functional performance in CAI. Nevertheless, no significant differential effect of dual-task training was observed in the study by Taghavi et al. [10]. Previous review studies indicated that dual-task training is safe and beneficial for postural stability in stroke patients and elderly individuals [11,12,13]. However, the effects of dual-task training on postural stability and functional ability in CAI have not been comprehensively analyzed, and reliable clinical evidence is scarce. Assessing whether dual-task training affects stability and functional ability may modify rehabilitation paradigms for CAI. We therefore performed a systematic review and meta-analysis of studies published on this individual. Our results can help healthcare providers decide whether dual-task training should be included in the rehabilitation program for CAI.
The purpose of this systematic review and meta-analysis was to investigate the effect of dual-task training on postural stability and functional ability in individuals with CAI.
Methods
Protocol and registration
This meta-analysis met the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [14]. This study was registered on PROSPERO as CRD42022356421. To increase the reliability of the meta-analysis results, only the randomized controlled trials (RCTs) were included and the effects of dual-task training on CAI were investigated, which were modified from the registered protocol.
Search strategy
The search was performed in PubMed, Web of Science, EBSCO, Cochrane Library, Physiotherapy Evidence Database (PEDro), China National Knowledge Infrastructure (CNKI) from inception to November 2022 with no restriction on language. The search strategy for each database is shown in Appendix 1. The search terms used were chronic ankle instability OR functional ankle instability OR mechanical ankle instability OR ankle sprain OR ankle instability AND dual task OR cognitive OR motor OR divided attention OR multi task OR combined OR concurrent. We also screened the reference lists of the papers identified in database searches.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) individuals: individuals with chronic ankle instability; (2) intervention: dual-task training; (3) comparisons: no restrictions; (4) outcome measures: static and dynamic postural stability or functional tests; (5) study design: randomized controlled trials (RCTs). We excluded studies: (1) if they were conducted in animals, in vitro, cadavers, or simulators; (2) if the articles were not RCTs or not published as peer-reviewed journal articles, including book chapters and conference abstracts; (3) studies whose full text or data are not available.
Study selection
Titles, abstracts, and full texts of the retrieved studies were screened by two independent reviewers (LW and GY) based on the inclusion and exclusion criteria. Disagreements were resolved by a third reviewer (YPC).
Data extraction
Two researchers (LW and GY) independently extracted the data: characteristics of the publications (authors, year of publication, etc.); details of study design (sample size, etc.); individuals (age, gender, number of individuals, etc.); interventions (type of dual-task training, frequency, duration of the session, etc.); and outcomes (assessment methods, etc.). Disagreements were resolved by a third reviewer (YPC).
Risk of bias assessment
The risk of bias of the included studies was assessed independently by two researchers (LW and GY) according to the Cochrane Risk of Bias list. The associated risks were divided into unclear, low, and high. Any disagreement was resolved by discussion until consensus was reached or by consulting a third author (YPC).
Statistical analysis
Review Manager5.3 (Cochrane Collaboration, Oxford, UK) was used to analyze the outcomes. Continuous data were presented as mean difference (MD) and 95% confidence interval (95% CI). The I2 statistic was used to measure the heterogeneity across the included studies. The fixed effect model was applied to analyze data with low heterogeneity (P ≥ 0.1, I²<50%). For data with high heterogeneity (P < 0.1, I²>50%), the source of the heterogeneity was investigated. After the reduction of heterogeneity by subgroup analysis or sensitivity analysis, the fixed effect model was adopted. While the random effect model was used to analyze data with high heterogeneity. Publication bias was not performed as there were no more than 10 included studies for each outcome. P ≤ 0.05 was considered significant.
Results
Study identification
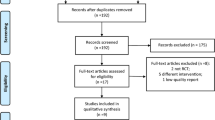
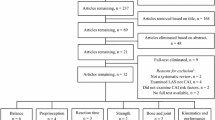
A total of 72 articles were identified after duplicates were removed and titles and abstracts were screened from the initial search result (Fig. 1). In the end, seven studies [8,9,10, 15,16,17,18] with 192 individuals were included in this systematic review. Of which, six studies [9, 10, 15,16,17,18] were included in the meta-analysis statistical comparison. One study [8] was excluded from the meta-analysis because their outcome measurements could not be merged.

Flow diagram showing selection process of articles following PRISMA guidelines
Characteristics of included studies
The characteristics of the included studies are shown in Table 1. The five RCTs included a total of 54 FAI and 138 CAI. Five studies performed the single task with the balance training [8, 10, 15, 16, 18], one study with the proprioceptive exercises [9], and one study [17] with no intervention in the control group. The dual-task training performed with dual tasks of backwards counting (BC) [10, 15], random number generation (RNG) [8, 15], backward digit span task [9], catching thrown balls [16], kicking balls [17] and active video games [18]. The duration of the intervention ranged from 1 session to 5 weeks. No follow-up effect was investigated in the included studies.
Study bias
The bias of the graph and summary of the included studies are shown in Figs. 2 and 3.

Risk of bias graph

Risk of bias summary
Blinding of individuals and personnel in 2 studies [17, 18] was considered high-risk. In 2 studies [10, 17], the risk of bias associated with blinding outcome assessment was deemed low. In 1 study [10], the risk of bias from allocation concealment was found to be low. Other bias in the included studies was deemed unclear.
Synthesis of results
Four studies [9, 10, 15, 18] with 87 individuals reported the effects of dual-task training on the Y-balance test. A fixed-effect model was used (I2 = 0%, P = 0.860). The synthesized data showed marginally significant differences between dual-task training and single-task training in Y-balance (MD = 1.60, 95% CI: −0.00 to 3.21, P = 0.050). (Fig. 4).

Forest plots demonstrated the effect of dual-task training on Y-balance in individuals with CAI.
Three studies [9, 15, 17] with 97 individuals reported the effects of dual-task training on center of pressure-area (COP-area) with high heterogeneity (I2 = 78%, P = 0.011). After excluding one study [15] by sensitivity analysis, heterogeneity among the studies was small (I2 = 0%, P = 0.897). A fixed-effect model was used for analysis, and the synthesized data showed a significant decrease in COP-are in the dual-task training group (MD = − 0.94, 95% CI: −1.62 to − 0.26, P = 0.007) in CAI. (Fig. 5).

Forest plots demonstrated the effect of dual-task training on COP-area in individuals with CAI.
Two studies [9, 15] with 53 individuals reported the effects of dual-task training on COP- velocity. The synthesized data showed no significant differences between dual-task training and single-task training in COP-velocity (MD = − 0.26, 95% CI: −0.70 to 0.17, P = 0.240) in CAI. And a random-effect model was used because of substantial heterogeneity for COP-velocity (I2 = 58%, P = 0.122) (Fig. 6).

Forest plots demonstrated the effect of dual-task training on COP-velocity in individuals with CAI.
Two studies [9, 16] with 50 individuals reported the effects of dual-task training on figure-of-8 hop test in CAI. No significant difference was found between dual-task training and single-task training (MD = − 0.20, 95% CI: −0.66 to 0.26, P = 0.386). A fixed-effect model was used (I2 = 9%, P = 0.296) (Fig. 7).

Forest plots demonstrated the effect of dual-task training on figure-of-8 hop tests in individuals with CAI.
Two studies [10, 18] with 34 individuals reported the effects of dual-task training on balance error scoring system (BESS) score in CAI. No significant difference was found between dual-task training and single-task training (MD = − 1.24, 95% CI: −2.95 to 0.48, P = 0.157). A fixed-effect model was used (I2 = 0%, P = 0.531) (Fig. 8).

Forest plots demonstrated the effect of dual-task training on BESS scores in individuals with CAI.
Discussion
This meta-analysis summarizes the effects of dual-task training on postural stability and functional ability among CAI groups. The results showed that compared with single task training or no intervention, dual-task training can improve Y-balance and COP-area in individuals with CAI.
Y-balance test
This meta-analysis showed that dual-task training had a marginally significant advantage over the control group on the Y-balance test in CAI. Similar results were obtained for dynamic balance performance in older adults [19] and in multiple sclerosis [20]. Several studies have shown that the process controlling the postural changes required to maintain stability requires attention [21, 22]. In the CAI group, a higher level of gait disturbance was reported to be required to cause a change, such as reducing stride time variability in walking, compared to healthy individuals, which may indicate lower adaptability of the sensorimotor system, reducing the ability of the central nervous system to adjust to different task demands [23]. Higher ankle inversion and frontal plane movement variability were detected in the FAI group compared to the healthy controls group during cognitive load walking, which may enhance the risk of ankle instability. Furthermore, the considerably lower mean stride velocity and cognitive performance in both groups imply that walking requires attention, and central processing requires attention to collect and integrate sensory information [24]. The cross-domain resource competition hypothesis states that both maintenances of postural stability and performance on cognitive tasks draw from a finite pool of cognitive resources for their regulation, potentially leading to a decrease in postural stability and/or cognitive tasks performance, when the two activities are performed simultaneously [25]. Nevertheless, some studies [26,27,28,29] examining individuals with CAI have shown positive effects of using two tasks, including improvements in postural control. The authors hypothesized that this could be due to increased attention to postural control [27]. Another study [30] confirmed the benefits of dual-task training for the task integration hypothesis, which states that task coordination skills improve when two activities are practiced simultaneously. Similar benefits were shown for variable priority training compared to fixed priority training in a study by Kramer et al. [31], which also demonstrated that individuals can learn to coordinate between two activities during training under variable priority settings. In addition, one study [32] found radiological evidence that cerebral hemodynamics of the dorsolateral prefrontal cortex improved in the dual-task training group, which was related to the increase in performance. However, some studies showed no significant difference between the dual-task training group and the control group in the dynamic postural control of stability indices [8] and Y-balance test [9, 10, 15, 18] in individuals with CAI. This may be due to the different intervention protocols included in the studies.
COP
The meta-analysis showed that dual-task training had a significant advantage over the control group in COP-area. It is consistent with previous studies, which found that a dual-task training group significantly improved static balance of anterior-posterior and medio-lateral balance [16] in CAI. During dual-task, individuals need to divide attention between two tasks (capacity sharing theory) [33]. Improvements in attention by dual-task training could affect balance [34]. In addition, dual-task training might improve integration and coordination skills while performing two tasks simultaneously [35]. However, there is no significant difference between dual-task training group and the control group on COP-velocity in CAI. The choice of outcome measurement may influence the results of the study since youths demonstrated low reliability in terms of COP-velocity [36]. The selection of more sensitive indices could make this assessment more accurate. Population may also be the reason for the negative results in this study. The sensitivity to dual-task training increased in the elderly and neurological diseases [37,38,39]. CAI population with younger age and better health conditions might have better adaptive capacity to dual tasks. The heterogeneity in COP-are and COP-velocity may be explained by the different use of dual-task training like the backward digit span task [9], RNG plus BC [15] and kicking balls [17]. Further research suggested that the degree of difficulty of the postural task and the complexity of the dual tasks both had an impact on stability performance [12, 40]. When the cognitive task is more complicated, more attentional resources may be required, depleting the resources available for postural stability. With increased balancing difficulty, attentional demand for postural control has been found to rise [4]. Even relatively straightforward dual tasks may have a detrimental effect on postural stability [11].
Hop-test
According to this meta-analysis, the dual-task training group had no significant advantage over the control group on the hop test in CAI, supporting previous findings [9, 41]. During dual-task, postural control appeared to take priority over cognitive processing [42]. It is unlikely that the cognitive task will have any impact on the postural control test if it is insufficient [43]. And it is interesting to note that, given the fact that the intervention program comprised dual tasks, we might have found higher improvement in the dual-task training group compared to the balance training group if the evaluation method had been dual-task [8]. Nevertheless, Kwak et al. [16] found that the dual-task training group improved significantly more than the control group in the up-down hop test. In this study, the motor task was part of the dual task. Motor task training may be more effective than cognitive task training for enhancing postural control, because motor tasks like throwing, catching, and kicking involve complex interactions of the somatosensory, visual, and vestibular systems to manage relationships between the body and external environment [44]. Further research is needed to confirm this.
BESS
BESS is a reliable and inexpensive tool for measuring the static balance of standing in people with CAI. Based on this meta-analysis, dual-task training had no significant effect over the control group on BESS in CAI. This is confirmed by a previous study [45], which stated that performing cognitive tasks with balance training simultaneously did not improve static balance while standing compared to balance training alone. Attentional demands are closely associated with postural control [46]. Quiet standing, which requires less attention because it is a basic ability that individuals have mastered [29], could explain why there is no significant difference in BESS between dual-task training and the control group in CAI.
Limitations of the study
There are several limitations in this study. (1) The included studies varied in the type and degree of difficulty of dual-task training, which added to the heterogeneity. (2) The duration of dual-task training’s therapeutic impact on CAI is unknown due to the absence of follow-up investigations. (3) Due to the small number of RCTs and limited studies in each category after sensitivity analysis, there was a potential risk of bias. (4) The majority of the studies that were included had small sample sizes, which increases the likelihood of a type II error [47].
Future perspectives
Maintaining posture is a simultaneous task in a variety of daily living activities, athletic pursuits, and leisure activities. Training protocols for individuals with CAI should be developed as dual-task training in the future to help the sensorimotor system become more automatic and perform its activities subconsciously [10]. Additionally, balance training strategies that divert attention away from postural control (i.e., external focus of attention) are more successful than those that concentrate on postural control (i.e., internal focus of attention) [48, 49]. Balance protocols that shift focus away from postural control are recommended in future studies. Besides, we might have found higher improvement in the dual-task training group compared to the balance-training group if the evaluation method had been dual-task. Outcome measurements involving dual-task performance were suggested to assess the effects of dual-task training on individuals.
Conclusion
Dual-task training may be effective in improving static and dynamic postural stability. However, more high-quality randomized controlled trials are needed to verify the short and long-term effectiveness of dual-task training on CAI.
Data Availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- CAI:
-
Chronic ankle instability
- FAI:
-
Functional ankle instability
- MAI:
-
Mechanical ankle instability
- PEDro:
-
Physiotherapy evidence database
- CNKI:
-
China national knowledge infrastructure
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- MD:
-
Mean differences
- CI:
-
Confidence Interval
- RCTs:
-
Randomized controlled trials
- BC:
-
Backwards counting
- RNG:
-
Random number generation
- COP:
-
Center of pressure
- BESS:
-
Balance error scoring system
- EG:
-
Experimental group
- CG:
-
Control group
- OSI:
-
Overall stability index
- APSI:
-
Anterior-posterior stability index
- MLSI:
-
Medial-lateral indices stability index
- TTB:
-
Time to boundary
References
Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54(6):572–88.
Takakusaki K. Functional neuroanatomy for posture and gait control. J Mov Disord. 2017;10(1):1–17.
Masters R, Maxwell J. The theory of reinvestment. Int Rev Sport Exerc Psychol. 2008;1(2):160–83.
Lajoie Y, Teasdale N, Bard C, Fleury M. Attentional demands for static and dynamic equilibrium. Exp Brain Res. 1993;97(1):139–44.
Papegaaij S, Hortobagyi T, Godde B, Kaan WA, Erhard P, Voelcker-Rehage C. Neural correlates of motor-cognitive dual-tasking in young and old adults. PLoS ONE. 2017;12(12):e0189025.
Lanzarin M, Parizzoto P, Libardoni TC, Sinhorim L, Tavares GMS, Santos GM. The influence of dual-tasking on postural control in young adults. Fisioterapia E Pesquisa. 2015;22:61–8.
Wulf G, McNevin N, Shea CH. The automaticity of complex motor skill learning as a function of attentional focus. Q J Exp Psychol Soc A. 2001;54(4):1143–54.
Onegh A, Akbari A, Ghiasi F, Hosseinifar M, Asgari A. The effect of dual-task training on dynamic postural control in the subjects with functional ankle instability. J Biotechnol. 2020;11(3):115–22.
Chae J-S, Choe Y-W, Kim M-K. The effects of proprioceptive exercise combined with cognitive task on the balance and ankle function of chronic ankle instability adults. J Korean Phys Soc. 2020;15(1):65–76.
Taghavi Asl A, Shojaedin SS, Hadadnezhad M. Comparison of effect of wobble board training with and without cognitive intervention on balance, ankle proprioception and jump landing kinetic parameters of men with chronic ankle instability: a randomized control trial. BMC Musculoskelet Disord. 2022;23(1):888.
Salihu AT, Hill KD, Jaberzadeh S. Effect of cognitive task complexity on dual task postural stability: a systematic review and meta-analysis. Exp Brain Res. 2022:1–29.
Ghai S, Ghai I, Effenberg AO. Effects of dual tasks and dual-task training on postural stability: a systematic review and meta-analysis. Clin Interv Aging. 2017;12:557–77.
Smith E, Cusack T, Blake C. The effect of a dual task on gait speed in community dwelling older adults: a systematic review and meta-analysis. Gait Posture. 2016;44:250–8.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Gonzales JM. Effects of a 4-week balance training and cognitive loading program in subjects with chronic ankle instability. The University of North Carolina at Charlotte; 2017.
Kwak K-I, Choi B-J. Effects of dual task training on balance and functional performance in high school soccer players with functional ankle instability. J Korean Phys Soc. 2016;28(4):254–8.
Conceição JS, Schaefer de Araújo FG, Santos GM, Keighley J, Dos Santos MJ. Changes in postural control after a ball-kicking balance exercise in individuals with chronic ankle instability. J Athl Train. 2016;51(6):480–90.
Maresh N. Effects of active video games in the rehabilitation of ankle sprains and chronic ankle instability. The University of Wisconsin-Milwaukee; 2014.
Li KZH, Roudaia E, Lussier M, Bherer L, Leroux A, McKinley PA. Benefits of cognitive dual-task training on balance performance in healthy older adults. J Gerontol A. 2010;65A(12):1344–52.
Martino Cinnera A, Bisirri A, Leone E, Morone G, Gaeta A. Effect of dual-task training on balance in patients with multiple sclerosis: a systematic review and meta-analysis. Clin Rehabil. 2021;35(10):1399–412.
Drijkoningen D, Leunissen I, Caeyenberghs K, Hoogkamer W, Sunaert S, Duysens J, et al. Regional volumes in brain stem and cerebellum are associated with postural impairments in young brain-injured patients. Hum Brain Mapp. 2015;36(12):4897–909.
Boisgontier MP, Cheval B, Chalavi S, van Ruitenbeek P, Leunissen I, Levin O, et al. Individual differences in brainstem and basal ganglia structure predict postural control and balance loss in young and older adults. Neurobiol Aging. 2017;50:47–59.
Springer S, Gottlieb U. Effects of dual-task and walking speed on gait variability in people with chronic ankle instability: a cross-sectional study. BMC Musculoskelet Disord. 2017;18(1):316.
Tavakoli S, Forghany S, Nester C. The effect of dual tasking on foot kinematics in people with functional ankle instability. Gait Posture. 2016;49:364–70.
Wollesen B, Voelcker-Rehage C, Regenbrecht T, Mattes K. Influence of a visual–verbal Stroop test on standing and walking performance of older adults. Neuroscience. 2016;318:166–77.
Mohamadi S, Ebrahimi I, Salavati M, Dadgoo M, Jafarpisheh AS, Rezaeian ZS. Attentional demands of postural control in chronic ankle instability, copers and healthy controls: a controlled cross-sectional study. Gait Posture. 2020;79:183–8.
McGrath ML, Yentes JM, Rosen AB. Cognitive loading produces similar change in postural stability in patients with chronic ankle instability and controls. Athl Train Sports Health Care. 2020;12(6):249–56.
Burcal CJ, Wikstrom EA. Cognitive loading-induced sway alterations are similar in those with chronic ankle instability and uninjured controls. Gait Posture. 2016;48:95–8.
Shiravi Z, Talebian Moghadam S, Hadian MR, Olyaei G. Effect of cognitive task on postural control of the patients with chronic ankle instability during single and double leg standing. J Bodyw Mov Ther. 2017;21(1):58–62.
Silsupadol P, Shumway-Cook A, Lugade V, van Donkelaar P, Chou LS, Mayr U, et al. Effects of single-task versus dual-task training on balance performance in older adults: a double-blind, randomized controlled trial. Arch Phys Med Rehabil. 2009;90(3):381–7.
Kramer AF, Larish JF, Strayer DL. Training for attentional control in dual task settings: a comparison of young and old adults. J Exp Psychol Appl. 1995;1:50–76.
Erickson KI, Colcombe SJ, Wadhwa R, Bherer L, Peterson MS, Scalf PE, et al. Training-induced functional activation changes in dual-task processing: an FMRI study. Cereb Cortex. 2007;17(1):192–204.
Pashler H. Dual-task interference in simple tasks: data and theory. Psychol Bull. 1994;116(2):220–44.
Kim D, Ko J, Woo Y. Effects of dual task training with visual restriction and an unstable base on the balance and attention of Stroke patients. J Phys Ther Sci. 2013;25(12):1579–82.
Liepelt R, Strobach T, Frensch P, Schubert T. Improved intertask coordination after extensive dual-task practice. Q J Exp Psychol. 2011;64(7):1251–72.
Lo PY, Su BL, You YL, Yen CW, Wang ST, Guo LY. Measuring the reliability of postural sway measurements for a static standing task: the effect of age. Front Physiol. 2022;13:850707.
Dorfman M, Herman T, Brozgol M, Shema S, Weiss A, Hausdorff JM, et al. Dual-task training on a treadmill to improve gait and cognitive function in elderly idiopathic fallers. J Neurol Phys Ther. 2014;38(4):246–53.
Choi JH, Kim BR, Han EY, Kim SM. The effect of dual-task training on balance and cognition in patients with subacute post-stroke. Ann Rehabil Med. 2015;39(1):81–90.
Fritz NE, Cheek FM, Nichols-Larsen DS. Motor-cognitive dual-task training in persons with neurologic disorders: a systematic review. J Neurol Phys Ther. 2015;39(3):142–53.
Burcal CJ, Needle AR, Custer L, Rosen AB. The effects of cognitive loading on motor behavior in injured individuals: a systematic review. Sports Med. 2019;49(8):1233–53.
Nakagawa K, Hamada K, Inokuma H, Chiba N, Okazaki S. Short-term intervention effects of dual-task training on injury and disability rates in young soccer players. Int J Phys Ther Rehab. 2017;3(135):2.
Resch JE, May B, Tomporowski PD, Ferrara MS. Balance performance with a cognitive task: a continuation of the dual-task testing paradigm. J Athl Train. 2011;46(2):170–5.
Jono Y, Kanai S, Goto T, Harada RYO, Hujitaka Y, Daniide Y, et al. Effect of dual task interference between motor task and cognitive task. Japanese J Health Promot Phys Ther. 2013;3(2):47–51.
Thomas E, Battaglia G, Patti A, Brusa J, Leonardi V, Palma A, et al. Physical activity programs for balance and fall prevention in elderly: a systematic review. Med (Baltimore). 2019;98(27):e16218.
Hiyamizu M, Morioka S, Shomoto K, Shimada T. Effects of dual task balance training on dual task performance in elderly people: a randomized controlled trial. Clin Rehabil. 2012;26(1):58–67.
Shumway-Cook A, Woollacott M. Attentional demands and postural control: the effect of sensorycontext. J Gerontol A. 2000;55(1):M10–M6.
Freiman JA, Chalmers TC, Smith H Jr., Kuebler RR. The importance of beta, the type II error and sample size in the design and interpretation of the randomized control trial. Survey of 71 negative trials. N Engl J Med. 1978;299(13):690–4.
Laufer Y, Rotem-Lehrer N, Ronen Z, Khayutin G, Rozenberg I. Effect of attention focus on acquisition and retention of postural control following ankle sprain. Arch Phys Med Rehabil. 2007;88(1):105–8.
Kang T, Chang H, Lee S. O27 a comparison of attentional focus with balance trainging between external and internal focus in chronic ankle instability on postural control: double blinded randomised control trial. Br J Sports Med. 2017;51:A1–A31.
Acknowledgements
Not applicable.
Funding
The study did not receive any specific funding from funding agencies in the public, commercial or non-profit sectors.
Author information
Authors and Affiliations
Contributions
L.W. contributed to the study concept and design. L.W. and G.Y. conducted the literature search, study selection, and quality assessment, and Y.C. resolved any disagreement. L.W. and G.Y. contributed to data synthesis and analysis and drafted the paper. All authors revised and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, L., Yu, G. & Chen, Y. Effects of dual-task training on chronic ankle instability: a systematic review and meta-analysis. BMC Musculoskelet Disord 24, 814 (2023). https://doi.org/10.1186/s12891-023-06944-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06944-3