
Abstract
Background
Understanding the barriers and facilitators to behaviour change by primary care practitioners (PCPs) is vital to inform the design and implementation of successful Behaviour Change Interventions (BCIs), embed evidence-based medicine into routine clinical practice, and improve quality of care and population health outcomes.
Methods
A theory-led systematic review of reviews examining barriers and facilitators to clinical behaviour change by PCPs in high-income primary care contexts using PRISMA. Embase, MEDLINE, PsychInfo, HMIC and Cochrane Library were searched. Content and framework analysis was used to map reported barriers and facilitators to the Theoretical Domains Framework (TDF) and describe emergent themes. Intervention functions and policy categories to change behaviour associated with these domains were identified using the COM-B Model and Behaviour Change Wheel (BCW).
Results
Four thousand three hundred eighty-eight reviews were identified. Nineteen were included. The average quality score was 7.5/11. Reviews infrequently used theory to structure their methods or interpret their findings. Barriers and facilitators most frequently identified as important were principally related to ‘Knowledge’, ‘Environmental context and resources’ and ‘Social influences’ TDF domains. These fall under the ‘Capability’ and ‘Opportunity’ domains of COM-B, and are linked with interventions related to education, training, restriction, environmental restructuring and enablement. From this, three key areas for policy change include guidelines, regulation and legislation. Factors least frequently identified as important were related to ‘Motivation’ and other psychological aspects of ‘Capability’ of COM-B. Based on this, BCW intervention functions of persuasion, incentivisation, coercion and modelling may be perceived as less relevant by PCPs to change behaviour.
Conclusions
PCPs commonly perceive barriers and facilitators to behaviour change related to the ‘Capability’ and ‘Opportunity’ domains of COM-B. PCPs may lack insight into the role that ‘Motivation’ and aspects of psychological ‘Capability’ have in behaviour change and/or that research methods have been inadequate to capture their function. Future research should apply theory-based frameworks and appropriate design methods to explore these factors. With no ‘one size fits all’ intervention, these findings provide general, transferable insights into how to approach changing clinical behaviour by PCPs, based on their own views on the barriers and facilitators to behaviour change.
Systematic review registration
A protocol was submitted to the London School of Hygiene and Tropical Medicine via the Ethics and CARE form submission on 16.4.2020, ref number 21478 (available on request). The project was not registered on PROSPERO.
Similar content being viewed by others


Background
Known as the “second translational gap” [1], a gap in translation between evidence-based interventions and everyday clinical practice has been shown across different clinical areas and international settings [2,3,4], with numerous organisational and individual factors influencing clinical behaviour. Existing literature has shown that there is particularly wide variation in clinical behaviour in the primary care setting, which cannot be explained by case mix and clinical factors alone [5, 6]. This variation is of particular concern, as it is widely accepted that primary care is the cornerstone of a strong healthcare system [7], and stronger primary care systems are generally associated with better and more equitable population health outcomes [8,9,10,11]. With an ageing population and unique evolving challenges faced in primary care, understanding the contextual barriers and facilitators to successful behaviour change by primary care practitioners (PCPs) is vital to inform the design and implementation of successful behaviour change interventions (BCIs), and is likely to offer the greatest potential improvement in quality of care and population health outcomes.
Behaviour change interventions
Changing behaviour of healthcare professionals is not easy, but has been shown to be easier when evidence-based theory informs intervention development [12]. BCIs aimed at healthcare professionals have traditionally been related to incentivisation schemes, guidelines, educational outreach, audit and feedback, printed materials and reminders [13, 14]. These have often emerged from approaches to understanding behaviour change, focused on individual attitude-intention processes [15] and theories emphasising self-interest [16, 17]. However, the impact of these interventions on changing clinicians’ behaviour has been found to variable [18]. Within the context of primary care, attitude-intention processes may not fully explain (lack of) behaviour change, where PCPs face competing pressures, such as caring for multiple patients with limited time, identifying pathology among undifferentiated symptoms, coping with emotional situations, managing uncertainty and keeping up-to-date with substantial volumes of new evidence. Similarly, theories of self-interest may not fully translate to PCPs. BCIs are often implemented through collective action across teams or based on financial levers [19,20,21]; however, the organisational context where PCPs work can vary from a single or group community-based practices with variable payment systems [22]. Therefore, while other healthcare professionals, patients and carers are likely to offer valuable insights, understanding PCPs’ own perspectives on the barriers and facilitators to behaviour change by PCPs is a vital starting point.
Theoretical Domains Framework and Behaviour Change Wheel
The Theoretical Domains Framework (TDF) of behaviour change [23] simplifies and integrates 33 theories and 128 key theoretical constructs related to behaviour change into a single framework for use across multiple disciplines. Theoretical constructs are grouped into 14 domains in the final paper by Michie et al. [24], encompassing individual, social and environmental factors, with the majority relating to individual motivation and capability factors [25] (Fig. 1). Skills can be subcategorised into cognitive and interpersonal, and physical, although cognitive and inter-personal skills are more relevant to primary care (Table 1).

The TDF has been widely used to examine clinical behaviour change in healthcare settings [25, 27,28,29,30,31,32,33,34]. Key advantages of the TDF include a comprehensive range of domains useful for synthesising large amounts of data [24] and the domains can be used to identify the types of interventions and policy strategies necessary to change those mechanisms of behaviour, using the Behaviour Change Wheel (BCW) [26]. Developed by Michie et al., the BCW can be used to characterise interventions by their “functions” and link these to behavioural targets, categorised in terms of capability (individual capacity to engage in the activity concerned), opportunity (all the factors that lie outside the individual that make the behaviour possible or prompt it) and motivation (brain processes that energize and direct behaviour), known as the COM-B System. Capability encompasses not only individual physical capability, but also psychological capability, defined as the capacity to engage in the necessary thought processes using comprehension, reasoning etc. Strategies to modify behaviour can be identified based on salient TDF and COM-B domains [35].
The evidence gap
Never having been done before, the aims of this systematic review of reviews were to:
-
1)
Identify barriers and facilitators to clinical behaviour change by PCPs through the theoretical lenses of the TDF and BCW, from the perspective of PCPs.
-
2)
Help inform the future development and implementation of theory-led BCIs, to embed EBM into routine clinical practice, improve quality of care and population health outcomes.
A systematic review of reviews was deemed an appropriate method to address these aims, as the literature is substantial and heterogeneous. Existing reviews of reviews have looked at different types of effective BCIs, both in primary care [36, 37] and in healthcare in general [18], however none have looked at barriers and facilitators to PCPs’ behaviour change, using both the TDF and BCW models as a theoretical basis.
We aimed to answer the following questions:
-
1)
Which TDF domains are most frequently identified as important by PCPs when barriers and facilitators to clinical behaviour change by PCPs are mapped to the TDF framework?
-
2)
What important themes emerge within these TDF domains?
-
3)
What intervention functions and policy strategies from the COM-B Model and BCW link to these TDF domains, and what are the implication of this?
Methods
Guidance presented in the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis [38] was used as methodological guidance to conduct the review, which provides guidance for umbrella reviews synthesising qualitative and quantitative data on topics other than intervention effectiveness. This guidance, alongside a modified version of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [39], were used for reporting (Additional file 1).
Searches
A comprehensive database search strategy was devised by MM with assistance from a librarian from LSHTM. The search was conducted by MM on April 16th 2020 without date restriction, using the following databases: Embase (1947 to 2020 April 14), MEDLINE (1946 to April week 1 2020), PsychInfo (1806 to April week 1 2020), Health Management Information Consortium (HMIC) (1979 to March 2020) and Cochrane Library (inception to April 2020). The full search strategies are shown in Additional file 2.
In addition, grey literature was hand-searched by MM on the following websites: Public Health England [40], the University College London (UCL) Centre for Behaviour Change [41] and the National Institute for Health and Care Excellence (NICE) Evidence Search [42]. After screening and selection, reference lists of the included reviews were screened for additional relevant reviews.
Inclusion and exclusion criteria
To be included, articles had to be reviews of qualitative, quantitative or mixed methods empirical studies examining barriers and facilitators to clinical behaviour change by PCPs. Inclusion and exclusion criteria were defined using the PICo framework (Population, phenomena of Interest, Context) [43], to enable transparency and reproducibility. The element of ‘types of studies’ was added to specify types of evidence included (Table 2).
Rationale
Population
In most HIC settings, general practitioners/family doctors are the main providers of primary care, however often included a mix of PCPs (healthcare professionals working in primary care).
Context
PCPs usually provide the mainstay of care in high-income settings. Common barriers and facilitators across a wide range of high-income settings provides stronger evidence for context-specific recommendations.
Types of studies:
-
The inclusion of all types of reviews (including but not limited to narrative and realist reviews, meta-ethnography and meta-aggregation) allows for a broader review of available literature and they are not bound by the specificity of systematic reviews [44, 45].
-
Only reviews published in English were included.
Screening and selection
Results from database searches were exported to EndNote X9 software and deduplicated. Titles and abstracts were screened independently by two reviewers (MM and SN). If the abstract contained insufficient information to determine eligibility, a copy of the full text was obtained. The full texts of articles meeting the inclusion criteria were obtained and reviewed. A standardised form including elements of the PICo framework was used at the full text review stage to identify relevant articles in a consistent way. Articles which could not be accessed online were obtained by contacting authors. Authors were also contacted to obtain clarification where eligibility was unclear. Reference lists of included articles were hand searched by MM and SN to identify additional relevant articles, subject to the same screening and selection processes described.
Quality appraisal
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Systematic Reviews and Research Syntheses [38] was used for quality appraisal, conducted independently by MM and SN. This tool was applicable to reviews of observational studies, which constituted the majority of the included articles; therefore, all reviews, regardless of their type, were subject to quality appraisal using the JBI checklist. This also allowed for consistency in scoring and easier comparison between the reviews. A scoring system was pre-defined using a small sample of five articles and guidance in the JBI Manual for Evidence Synthesis [38]. Some articles fulfilled some but not all of the criteria for each question, which was believed to be reasonable, therefore an additional ‘partial yes’ response was added to reflect this (Additional file 3). With a maximum score of 11, scores were used to indicate low (≤ 4 points), moderate (> 4 and < 8 points) and high (≥ 8 points) quality. As outlined by Pope and Mays [46], the value of specific pieces of qualitative research may only emerge during the synthesis process and may still offer valuable insights despite low quality. No articles were therefore excluded on the basis of low quality scores.
Data extraction
The JBI Data Extraction Form for Reviews of Systematic Reviews and Research Syntheses [38] was adapted to extract relevant data from included reviews. A citation matrix was created to map the included empirical studies of each review and identify duplicate references.
Data analysis and synthesis
Data analysis was conducted independently by MM and SN. Previously reported analysis methods [25, 47] were used to guide data analysis and synthesis methods. A combination of content and framework analysis was used, described in five steps:
-
1)
Data extraction: full-text versions of the included articles were imported into NVivo software and data were extracted from results and discussion sections and supplementary files. Data included barriers, facilitators and factors which could be both barriers and facilitators.
-
2)
Deductive analysis: extracted barriers, facilitators and factors were mapped to relevant TDF domains using component constructs of each domain, outlined by Cane et al. [24]. Almost all reported barriers and facilitators related to skills were cognitive and interpersonal, therefore the TDF domain ‘skills: physical’ was removed.
-
3)
Counts were used to identify the most frequently-reported TDF domains. Owing to the vast amount of information across the included reviews, counts were also used to identify the TDF domains most frequently reported as important by authors. This was done in three ways: where authors explicitly stated they were important or salient, where they were most frequently reported where authors used frequency counts, and where authors highlighted or focused on them in the discussion section to draw main conclusions.
-
4)
Inductive analysis: thematic analysis was conducted to identify emergent themes within the TDF domains most frequently identified as important to provide context to the role each barrier, facilitator and factor plays in hindering or facilitating clinical behaviour change. Owing to the vast amount of information across the included reviews, themes reported as important or salient by five or more reviews were labelled as important overall.
-
5)
TDF domains most frequently identified as important were mapped to the COM-B model of the BCW to identify the associated intervention functions and policy categories.
Discrepancies between reviewers at the screening, selection, quality appraisal and analysis stages were discussed until a consensus was reached.
Results
Search results and selection
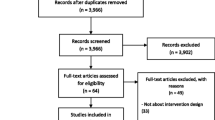
Database searches identified 6308 records. After duplicates were removed, there were 4374 records remaining. An additional 14 articles were identified from grey literature and reference list searches. The vast majority of these articles were either not a review of empirical studies, or they did not focus on behaviour change. Where they did focus on behaviour change, they focused on patient behaviour change, rather than that of PCPs. One hundred and nine full-text articles were assessed for eligibility. Clarification was sought from 19 authors on participant roles, search strategies and synthesis methods, and was obtained from 11 authors. Nineteen reviews [33, 48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65] were included in the data synthesis (Fig. 2).

Flow chart [66] of review process
Characteristics of included reviews
Of the 19 included reviews, 17 [48,49,50,51,52,53,54,55,56,57,58,59,60,61,62, 64, 65] were systematic reviews and 2 [33, 63] were narrative reviews. The reviews were all published between 2005 and 2020. Four hundred and one empirical studies were included in total across a wide range of settings and healthcare systems. Almost all studies were conducted in high-income countries, the majority of which were conducted in Europe, USA, Canada, Australia and New Zealand. Five studies (1%) were conducted in upper-middle-income countries, including Jordan, Turkey, South Africa and Bosnia and Herzegovina. Seven reviews [48,49,50,51,52,53, 65] only included qualitative studies, two [54, 55] only included quantitative studies, and 10 [33, 56,57,58,59,60,61,62,63,64] included qualitative, quantitative and/or mixed methods studies. Most studies were observational, utilising qualitative interviews and/or focus groups, or cross-sectional surveys. A minority of observational studies from six [55, 58, 59, 62,63,64] reviews were part of larger intervention studies.
More than 72,000 PCPs were included in total. Seven [33, 48, 49, 52, 55, 63, 64] reviews only reported general practitioner (GP) or family physician (FP) data and 12 [50, 51, 53, 54, 56,57,58,59,60,61,62, 65] reported a mix of PCP data, the majority of which were GPs, FPs, and community paediatrics and obstetrics and gynaecology physicians. Of these, five reviews [51, 56, 60, 62, 65] included primary care non-physicians, including nurse practitioners (NPs) and physician assistants. Seven reviews [50, 52, 53, 56, 58, 61, 65] examined behaviour related to clinical management of a range of topics, of which three specifically examined prescribing behaviour; four reviews [33, 51, 59, 63] examined diagnostic processes; two [49, 54] examined prevention; two [55, 57] examined communication and engagement with patients; two [48, 64] examined the practice of EBM in general; one [62] examined collaborative practice; and one [60] examined service provision. Eighteen studies were referenced by two reviews each due to overlapping phenomena of interest. The most common data synthesis methods were thematic/narrative synthesis and meta-ethnography, used by 13 reviews [48,49,50,51,52,53, 55, 56, 58, 60,61,62, 65]. Six reviews [33, 54, 57, 59, 63, 64] used framework synthesis; only three reviews [33, 59, 64] used existing theoretical frameworks or models, such as the TDF and COM-B. A summary of review characteristics is shown in Table 3. Additional information is shown in Additional file 4.
Quality appraisal
Quality of empirical studies
Three reviews [33, 55, 63] did not conduct quality appraisal, two of which [33, 63] were narrative reviews. The remaining reviews used a wide range of appraisal tools to suit the type of data they included, which were primarily existing tools in their original or adapted forms. Five reviews [56, 57, 60, 62, 64] used more than one tool. The most common appraisal tools used were CASP (Critical Appraisal Skills Programme) Checklists [67] for qualitative and quantitative research, used by seven reviews [48, 52, 53, 56, 57, 59, 65]. There was large variation in how authors used the appraisal tools, therefore quality of studies could not be reliably compared between reviews. Detailed information is shown in Additional file 3.
Quality of reviews
Ten reviews were of high quality, seven were of moderate-quality and two were of low quality using the JBI checklist. The highest score was 10.5/11 and the lowest was 3/11. The average score was 7.5/11, which is considered moderate quality. Reviews generally included well-evidenced recommendations for policy and practice and appropriate directives for future research. On validity, reviews scored highest on appropriate inclusion criteria for the review question, and appropriate methods used to combine studies. Reviews scored poorly on using an appropriate search strategy and assessing for publication bias. Most reviews did not justify search limits and/or did not provide evidence of a search strategy. Scores for each of the criteria are shown in Additional file 3.
Main findings
A large number of barriers, facilitators and factors were identified by authors, often interacting with each other in a complex way (Table 4). As a result, some barriers and facilitators were mapped to more than one TDF domain. All TDF domains were identified. All reviews identified ‘environmental context and resources’ as important, and all but two reviews identified ‘knowledge’ and ‘social influences’ as important. TDF domains identified least frequently as important were ‘goals’, ‘intentions’ and ‘optimism’. Although ‘social/professional role and identity’, ‘skills’ and ‘emotion’ TDF domains were frequently identified, they were less frequently highlighted as important by authors. Table 4 shows how each TDF domain and COM-B domains were mapped to each of the included reviews, as well as which domains were identified as important.
Forty-two themes were identified in total across all TDF domains, 12 of which were labelled as important overall. A theme was labelled as important overall if five or more reviews identified it as important or salient. Within the ‘Knowledge’, ‘Environmental context and resources’, and ‘Social influences’ TDF domains, nine important themes emerged, of which the most frequently cited as important were ‘knowledge, awareness and uncertainty’ and ‘time, workload and general resources’. Across the remaining TDF domains, other important themes included ‘skills and competence’, ‘roles and responsibilities’, and ‘confidence in own ability’. Additional file 5 shows how themes were mapped to each TDF domain and each review, with corresponding quotes.
Capability: psychological (COM-B domain)
Knowledge (TDF domain)
Knowledge, awareness and uncertainty (theme)
Identified as important by 13 reviews [33, 50,51,52, 54, 55, 58,59,60,61,62,63, 65] (average quality score 7.2/11).
Inadequate knowledge and awareness and uncertainty were identified as important barriers to depression diagnosis and management [51, 56], recognition of insomnia [33], antibiotic prescribing in childhood infections [50] and acute respiratory tract infections (ARTIs) [65], engagement in cancer care [58], integration of genetics services [60], discussing smoking cessation [55], collaborative practice [62], management of multimorbidity [52], breast and colorectal screening in older adults [54] and chlamydia testing [59, 63]. This varied from a lack of knowledge of the topic as a whole, to more specific skills or outcomes. For example, PCPs reported a lack of knowledge around the epidemiology and presentation of chlamydia, benefits of testing, how to take specimens, and treatment options [59]. When prescribing antibiotics for childhood infections and ARTIs, PCPs reported they tend to prescribe “just in case” when they are uncertain of the consequences of not prescribing, such as when the diagnosis is unclear, or where there is no established doctor-patient relationship [50, 65]. There was widespread lack of knowledge within the field of genetics, including uncertainty around cancer genetics, genetic testing, genetic discrimination legislation, and local genetics service provision [60]. As well as a lack of knowledge of national guidelines and strategy [60, 63], inadequate guidelines were reported to exacerbate a lack of knowledge. For example, a lack of attention in guidelines on how social problems affect response to depression management was reported to exacerbate PCPs’ uncertainty around their role in managing depression [56]. Lack of knowledge and uncertainty were frequently reported to cause discomfort, low confidence, and reluctance to fill certain roles.
Opportunity: physical (COM-B domain)
Environmental context and resources (TDF domain)
Time, workload and general resources (theme)
Identified as important by 13 reviews [33, 48, 50, 51, 53,54,55, 58,59,60,61, 63, 64] (average quality score 7.3/11).
A lack of time to implement a variety of different tasks and clinical behaviours was reported, compounded by a large and complex workload and lack of general resources. A prominent barrier was time-pressured consultations, where PCPs reported difficulty in ensuring the clinician and parents are satisfied with the outcome when treating childhood infections [50], offering alternative interventions [53], listening to patients with depression [56], discussing emotions in cancer care [58] or smoking cessation with patients [55], introducing chlamydia testing and addressing sexual health-related concerns [63], recognising, diagnosing and managing child and adolescent mental health problems [61], and negotiating with patients [48]. PCPs also reported a lack of time to read and assess evidence and guidelines and reflect on their own practice [48, 64].
Guidelines, evidence and decision-making tools (theme)
Identified as important by five reviews [48, 52, 58, 64, 65] (average quality score 7.8/11).
Guidelines were a common factor reported to affect clinical behaviour, including a lack of guidelines/guidance, questionable evidence-base, and a disjunction between guidelines and personal experience. For example, PCPs reported difficulty in adapting recommendations to individual patient circumstances and practical constraints of the consultation [48, 51, 52]. PCPs felt that some guidelines lack the necessary flexibility when taking patient preferences and multi-morbidity into account, which can add to complexity and even cause harm in some cases [52, 64]. PCPs questioned the evidence-base of the guidelines due to low generalisability and narrow inclusion criteria of trials [48, 64] and potential biased sources of research, such as pharmaceutical companies [64]. The validity of criteria used for depression diagnosis was also questioned, with national guideline criteria defining depressive disorders using symptom counts, as opposed to viewing it as a syndrome requiring aetiological and conceptual thinking [51]. For non-English PCPs, access to evidence and guidelines in their native language was reported as a major barrier to implementing EBM [64].
Financial resources and insurance coverage (theme)
Identified as important by 6 reviews [49, 54, 58, 61, 62, 64] (average quality score 8/11).
Poor remuneration and increasing costs were common barriers reported in areas such as PCP involvement in cancer care [58], child and adolescent mental health [61] and use of EBM [64]. A major barrier to recognition and management of child and adolescent mental health problems and cancer in older adults was inadequate insurance coverage, including inadequate coverage of screening tests [54], restrictions on the number of funded therapy visits, and lack of psychiatrists [61]. As a result, increased reimbursement was identified as a potential facilitator that could increase child and adolescent mental health diagnoses [61].
Education and training (theme)
Identified as important by five reviews [33, 59, 63,64,65] (average quality score 5.7/11).
A lack of education and training was highlighted as an important barrier to chlamydia testing [59, 63], recognition of insomnia [33], antibiotic prescribing [65], and use of EBM [64]. PCPs reported that undergraduate sexual health teaching is inadequate [63] and that they have a lack of appropriate training and skills to discuss sexual health, take a sexual history, offer a test, manage treatment and notify partners. This has led to a reduction in knowledge and confidence to offer testing and discuss sexual health [59]. More education and training for PCPs and undergraduate students was frequently cited as a facilitator, as PCPs felt this would increase knowledge and confidence to change behaviour. Older male PCPs were identified as potentially in need of specific education on sexual health due to cultural differences with some patients receiving chlamydia testing [59]. Some PCPs reported that trustworthy and knowledgeable educational sources are important for PCPs to feel added value, with peer-led educational meetings given as an example [65].
Opportunity: social (COM-B domain)
Social influences (TDF domain)
PCP-patient relationship and patient-centred care (theme)
Identified as important by nine reviews [48, 49, 51,52,53, 57,58,59, 65] (average quality score 8.2/11).
Some PCPs reported that preservation of the PCP-patient relationship is prioritised over adherence to guidelines, particularly if guidelines recommend rationing services, or if PCPs feel empathetic towards anxious patients [48]. This dilemma was described as unpleasant and against the principles of patient-centred medicine, but sometimes necessary to avoid the potential litigation that rationing might bring [48] and loss of patients to other practices [53]. Similarly, the desire to maintain a good relationship is sometimes in competition with the PCP’s rationing role, leading some PCPs to give patients a “quick fix” when prescribing benzodiazepines [53]. Although not always reported as important, sensitive and emotive areas of medicine appear to be particularly affected, with PCPs reporting a concern for depriving patients of hope and/or damaging the relationship if they engage in the process of ACP [57], cancer care [58], or offer chlamydia testing [63]. Specifically, PCPs worried about appearing discriminatory and judgemental towards patients by offering chlamydia testing [63], and being too intrusive and paternalistic in recommending behaviour change to patients to prevent CVD [49]. This appears to be compounded by different religious and cultural norms between the PCP and patient, particularly if patients are of non-heteronormative orientation [63].
Establishing a rapport with patients and developing a long-standing, trusting doctor-patient relationship was identified as a facilitator for information-sharing, depression diagnosis [51], multimorbidity management [52], changing prescribing behaviour of benzodiazepines [53] and PCP engagement in ACP [57].
Patient/carer characteristics (theme)
Identified as important by eight reviews [49, 50, 53, 54, 56, 59, 64, 65] (average quality score 8/11).
The majority of reviews identified perceptions of patient/carer perceived ideas, concerns, expectations and motivations as important barriers to preventing CVD [49], prescribing antibiotics [50, 65] and benzodiazepines [53], chlamydia testing [59], cancer screening in older adults [54], and implementing EBM [64]. Attitudes were often born from stigma towards patients with mental health problems, and cultural diversity between the PCP and patient. For example, PCPs were found to have ambivalent attitudes towards working with depressed people, with some PCPs describing them as “burdens” and “people who bore you” [56]. Ethnic minorities were also felt to somatise their depression, and patients with social problems were seen to be avoiding work or seeking to medicalise their problems. This was compounded by a perception that management of patients presenting with social problems is complex. These beliefs were considered alongside other complex external factors, such as perceived pressure from parents to prescribe antibiotics [50], patient expectations different from the evidence [64], and a reluctance to medicalise unhealthy lifestyles [49].
Collaboration and communication with other health professionals (theme)
Identified as important by seven reviews [49, 52, 58, 59, 61, 62, 65] (average quality score 7.8/11).
Poor communication and uncoordinated care between PCPs and specialists were reported to hinder medication overviews, creating a feeling of uncertainty around the role of the PCP [52]. This was compounded by the perception of hierarchy between doctors and nurses [62] and negative attitudes towards handing over power [59]. Co-management with specialists was identified as an important facilitator in CVD prevention, to reinforce specialist advice and strengthen cohesive care [49]. Specialist input was desired by some PCPs to improve the awareness of the complexity of multimorbidity among specialists and ensure all doctors ‘speak with one voice’ to avoid provoking distrust [52]. Discussion with peers and personal or local prescribing feedback were identified as important facilitators to changing antibiotic prescribing [65]. Multiple facilitators to collaboration between nurse and medical practitioners in primary care were also identified [62]. These ranged from knowing the practitioner and having a good working relationship, reciprocity without hierarchy and control, effective communication including the use of technology, mutual trust and respect, shared responsibility and support from medical practitioners.
Norms, stigma and attitudes (theme)
Identified as important by five reviews [56, 59, 60, 63, 65] (average quality score 6.6/11).
The belief that patients would feel stigmatised or embarrassed was identified as an important barrier to depression diagnosis [56], chlamydia testing [59, 63], discussing family history and genetics [60] and antibiotic prescribing for ARTIs [65]. Stigma towards depression was seen as an important barrier to addressing psychosocial aspects of depression and commencing treatment amongst patients from the Caribbean and South Asia [56]. Stigmatising attitudes towards depressed, obese and elderly people was also reported to impact clinical decision-making [49, 56] (see ‘Patient and carer characteristics’ section). A major facilitator to reduce stigma and raise awareness was the normalisation of chlamydia testing [63]. This may include formal policy, guidelines or government programmes, feedback on testing rates, different methods of testing such as urine samples, and the use of non-heteronormative terminology.
BCW intervention functions and policy categories
COM-B components and intervention functions linked to the three TDF domains most frequently identified as important are shown in Table 5. Based on this, five intervention functions from the BCW were identified as most likely to be successful in changing clinical behaviour by PCPs. Associated with improving ‘capability’ are education (increasing knowledge or understanding), training (imparting skills) and enablement (promoting collective action across networks to overcome barriers, such as behavioural support for smoking cessation) interventions. Associated with improving social and physical ‘Opportunity’ are restriction (using rules to engage in the target behaviour), environmental restructuring (changing the physical or social context) and enablement interventions. The TDF domains ‘intentions’, ‘goals’ and ‘optimism’, which all map to the ‘motivation’ domain of the COM-B, were perceived as the least influential on clinical behaviour change by PCPs. As a result, BCW intervention functions including persuasion, incentivisation, coercion and modelling may be perceived as less relevant by PCPs to change behaviour.
Using the BCW, the three policy categories most commonly associated with supporting the delivery of the five intervention functions identified include guidelines (creating documents that recommend or mandate practice, including all changes to service provision), regulation (establishing rules or principles of behaviour or practice, such as establishing voluntary agreements on advertising), and legislation (making or changing laws, such as prohibiting sale or use) (Table 5).
Discussion
Summary of main results
Evidence across all reviews was heterogeneous, examining 16 different clinical behaviours across a range of primary care settings and healthcare systems. Most reviews were of moderate-to-high quality. All themes identified from the included reviews could be mapped to at least one domain from the TDF. Barriers, facilitators and factors most commonly reported by PCPs were related to ‘knowledge’, ‘environmental context and resources’ and ‘social influences’. Within these domains, ‘knowledge, awareness and uncertainty’ and ‘time, workload and general resources’ were by far the most important themes. Not only did factors affect various clinical behaviours such as diagnosis, management, and communication and collaboration with patients and other healthcare professionals, factors were also linked to each other in a complex way, often exacerbating each other in specific contexts and circumstances. For example, a lack of knowledge and uncertainty amongst PCPs is exacerbated by a poor or unestablished PCP-patient relationship, lack of time and resources, as well as patient characteristics, such as comorbidities and social problems.
Five out of nine intervention functions from the BCW (education, training, restriction, environmental restructuring and enablement) can be linked to the three TDF domains reported as most important by PCPs to help change clinical behaviour. These can be delivered through all seven policy categories of the BCW, although those most frequently associated policy categories with all five intervention categories are guidelines, regulation and legislation.
The TDF domains ‘intentions’, ‘goals’ and ‘optimism’, which all map to the ‘motivation’ domain of the COM-B, were perceived as the least influential on clinical behaviour change by PCPs. The TDF domains ‘behavioural regulation’, ‘memory, attention and decision processes’, ‘emotion’, ‘beliefs about consequences’, ‘reinforcement’, and ‘beliefs about capabilities’ were also perceived by PCPs as less important barriers or facilitators to behaviour change. ‘Behavioural regulation’, and ‘memory, attention and decision processes’ relate to the psychological aspect of ‘capability’ and the others, again, relate to the ‘Motivation’ domain of COM-B. This is a surprising finding, as the central premise of the TDF model is that domains linked to all three areas of the COM-B (capability, opportunity and motivation) model should interact to produce behaviour [25].
Linked to the automatic and reflective ‘motivation’ domain of COM-B are BCW interventions related to incentivisation, persuasion, coercion and modelling. It is therefore also surprising to find that PCPs did not identify these as important barriers and/or facilitators as substantial evidence exists regarding the widespread use of interventions associated with incentives (e.g. financial pay for performance or reputational league tables—albeit with mixed effects, and those which may utilise persuasion, modelling and even coercion (e.g. peer-to-peer outreach or public reporting) to change aspects of PCP behaviour [14, 68,69,70].
The limited frequency and importance given to aspects of psychological ‘Capability’ and ‘Motivation’ raises questions as to whether PCPs may have less insight into these areas or less desire to identify them as barriers or facilitator. It is possible they may be neglecting the role of brain processes involved in developing psychological capabilities, i.e. the capacity to engage in the necessary thought processes using comprehension and reasoning, and those that energize or direct behaviour, such as habitual processes, emotional responding and automatic decision-making. With most studies using qualitative interviews or cross-sectional surveys, questions may also have focused on domains researchers and BCI designers believed to be relevant, such as external factors including time, guidelines and patients.
Key policy implications
Based on our findings, three TDF domains were most commonly reported across the majority of reviews, regardless of the type of behaviour change and context. This suggests that addressing these common factors through associated BCW intervention functions of education, training, restriction, environmental restructuring and enablement, and applying associated policy categories—namely guidelines, regulation and legislation, if not already addressed, could be prioritised to encourage PCPs to change clinical practice where needed across most clinical behaviours and settings.
Strengths and limitations
The robustness of our findings is supported by several features. A broad, sensitive search strategy maximised the number of eligible reviews identified. Although the extent to which findings are applicable to a specific healthcare system or clinical context is unclear, reviews meeting the inclusion criteria focused on 16 types of clinical behaviours across a breadth of healthcare systems and included over 72,000 PCPs, providing a good starting point to identify commonalities across PCPs from a variety of different primary care settings.
Large amounts of heterogeneous data was summarised in a clear way using two evidence-based frameworks, however precise mapping of barriers, facilitators and factors to the TDF proved challenging, owing to the complex interplay between factors and interpretation of the authors of where they fitted. The integration of the TDF and BCW means important barriers and facilitators can be linked to practical strategies to address them, which does, however, rely on the validity of the frameworks themselves.
Future research
Only a minority of reviews utilised a theory-based framework to synthesise evidence. To maximise the likelihood of intervention success and encourage the use of common terminology and understanding, future research should synthesise evidence using theory-informed frameworks, such as the TDF, paying particular attention to barriers and facilitators to behaviour change associated with PCPs’ own automatic and reflective motivation, and other aspects of psychological capability related to behaviour change. Methods exploring PCP motivation and aspects of psychological capability, as well as methods less reliant on PCPs’ insight, such as direct observation, may provide more valid conclusions.
Conclusions
To the best of our knowledge, this is the first theory-led systematic review of reviews examining barriers and facilitators to clinical behaviour change by PCPs across a variety of primary care settings using the TDF and BCW. From the evidence available, PCPs perceive that factors related to knowledge, environmental context and resources and social influences are influential across a variety of primary care contexts, often interacting with each other in a complex way. It is vital that future research utilises theory-based frameworks and appropriate design methods to explore factors relating to automatic and reflective motivation, such as habitual processes, emotional responding and automatic decision-making that energize or direct behaviour, as well as psychological capability of PCPs, including the capacity to engage in the necessary thought processes using comprehension, reasoning etc. With no ‘one size fits all’ intervention, these findings go some way to offering general, transferable lessons in how to approach changing clinical behaviour by PCPs and improve quality of care and population health outcomes.
Availability of data and materials
All data analysed during this study are included in this published article and its additional information files.
Abbreviations
- ARTI:
-
Acute respiratory tract infection
- BCI:
-
Behaviour Change Intervention
- BCW:
-
Behaviour Change Wheel
- CASP:
-
Critical Appraisal Skills Programme
- COM-B:
-
Capability Opportunity Motivation Behaviour
- CVD:
-
Cardiovascular disease
- EBM:
-
Evidence-based medicine
- FP:
-
Family physician
- GP:
-
General practitioner
- HMIC:
-
Health Management Information Consortium
- JBI:
-
Joanna Briggs Institute
- NICE:
-
National Institute for Health and Care Excellence
- NP:
-
Nurse practitioner
- PCP:
-
Primary care practitioner
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- TDF:
-
Theoretical Domains Framework
References
Woolf SH. The meaning of translational research and why it matters. JAMA. 2008;299(2):211–3.
Sederer LI. Science to practice: making what we know what we actually do. Schizophr Bull. 2009;35(4):714–8.
Runciman WB, Hunt TD, Hannaford NA, Hibbert PD, Westbrook JI, Coiera EW, et al. CareTrack: assessing the appropriateness of health care delivery in Australia. Med J Aust. 2012;197(2):100–5.
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–30.
Brookes-Howell L, Hood K, Cooper L, Little P, Verheij T, Coenen S, et al. Understanding variation in primary medical care: a nine-country qualitative study of clinicians’ accounts of the non-clinical factors that shape antibiotic prescribing decisions for lower respiratory tract infection. BMJ Open. 2012;2(4):e000796.
Jaramillo E, Tan A, Yang L, Kuo Y-F, Goodwin JS. Variation among primary care physicians in prostate-specific antigen screening of older men. JAMA. 2013;310(15):1622–4.
Shi L. The impact of primary care: a focused review. Scientifica. 2012;2012:432892.
Starfield B. Policy relevant determinants of health: an international perspective. Health Policy. 2002;60:201–18.
Macinko J, Starfield B, Shi L. The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970-1998. Health Serv Res. 2003;38(3):831–65.
Niti M, Ng TP. Avoidable hospitalisation rates in Singapore, 1991–1998: assessing trends and inequities of quality in primary care. J Epidemiol Community Health. 2003;57(1):17–22.
Starfield B. Primary care and health: a cross-national comparison. In: Isaacs SL, Knickman JR, editors. Generalist medicine and the US health system, Chapter 11. Princeton: Robert Wood Johnson; 2004. p. 187–96.
Abraham C, Kelly MP, West R, Michie S. The UK National Institute for Health and Clinical Excellence public health guidance on behaviour change: a brief introduction. Psychol Health Med. 2009;14(1):1–8.
Grimshaw JMSL, Thomas R, et al. Changing provider behavior: an overview of systematic reviews of interventions. Med Care. 2001;39(8):II2–45.
Ahmed K, Hashim S, Khankhara M, Said I, Shandakumar AT, Zaman S, et al. What drives general practitioners in the UK to improve the quality of care? A systematic literature review. BMJ Open Qual. 2021;10(1):e001127.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211.
Laffont JJ, Martimort D. The theory of incentives: the principal-agent model. Princeton: Princeton University Press; 2009.
Becker G. The economic approach to human behavior. Chicago: University of Chicago Press; 1976.
Johnson MJ, May CR. Promoting professional behaviour change in healthcare: what interventions work, and why? A theory-led overview of systematic reviews. BMJ Open. 2015;5(9):e008592.
Thornton PH, Ocasio W, Lounsbury M. The institutional logics perspective: a new approach to culture, structure and process. Oxford: Oxford University Press; 2012. p. 248.
Hernes T. A process theory of organization. Oxford: Oxford University Press; 2014.
Czarniawska B. A theory of organizing. Cheltenham: Edward Elgar Publishing Ltd; 2008.
Berenson RA, Rich EC. US approaches to physician payment: the deconstruction of primary care. J Gen Intern Med. 2010;25(6):613–8.
Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33.
Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37.
Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Michie S, Pilling S, Garety P, Whitty P, Eccles MP, Johnston M, et al. Difficulties implementing a mental health guideline: an exploratory investigation using psychological theory. Implement Sci. 2007;2(1):8.
Islam R, Tinmouth AT, Francis JJ, Brehaut JC, Born J, Stockton C, et al. A cross-country comparison of intensive care physicians’ beliefs about their transfusion behaviour: a qualitative study using the Theoretical Domains Framework. Implement Sci. 2012;7:93.
McSherry LA, Dombrowski SU, Francis JJ, Murphy J, Martin CM, O’Leary JJ, et al. ‘It’s a can of worms’: understanding primary care practitioners’ behaviours in relation to HPV using the theoretical domains framework. Implement Sci. 2012;7(1):73.
Duncan EM, Francis JJ, Johnston M, Davey P, Maxwell S, McKay GA, et al. Learning curves, taking instructions, and patient safety: using a theoretical domains framework in an interview study to investigate prescribing errors among trainee doctors. Implement Sci. 2012;7:86.
Bussières AE, Patey AM, Francis JJ, Sales AE, Grimshaw JM, the Canada PPT. Identifying factors likely to influence compliance with diagnostic imaging guideline recommendations for spine disorders among chiropractors in North America: a focus group study using the Theoretical Domains Framework. Implement Sci. 2012;7(1):82.
Murphy K, O’Connor DA, Browning CJ, French SD, Michie S, Francis JJ, et al. Understanding diagnosis and management of dementia and guideline implementation in general practice: a qualitative study using the theoretical domains framework. Implement Sci. 2014;9(1):31.
Ogeil RP, Chakraborty SP, Young AC, Lubman DI. Clinician and patient barriers to the recognition of insomnia in family practice: a narrative summary of reported literature analysed using the theoretical domains framework. BMC Fam Pract. 2020;21(1):1.
Craig LE, McInnes E, Taylor N, Grimley R, Cadilhac DA, Considine J, et al. Identifying the barriers and enablers for a triage, treatment, and transfer clinical intervention to manage acute stroke patients in the emergency department: a systematic review using the theoretical domains framework (TDF). Implement Sci. 2016;11(1):157.
Richardson M, Khouja CL, Sutcliffe K, Thomas J. Using the theoretical domains framework and the behavioural change wheel in an overarching synthesis of systematic reviews. BMJ Open. 2019;9(6):e024950.
Chauhan BF, Jeyaraman MM, Mann AS, Lys J, Skidmore B, Sibley KM, et al. Behavior change interventions and policies influencing primary healthcare professionals' practice-an overview of reviews. Implement Sci. 2017;12(1):3.
Lau R, Stevenson F, Ong BN, Dziedzic K, Treweek S, Eldridge S, et al. Achieving change in primary care—causes of the evidence to practice gap: systematic reviews of reviews. Implement Sci. 2016;11(1):40.
Aromataris E, Fernandez R, Godfrey C, Holly C, Khalil H, Tungpunkom P. Chapter 10: Umbrella reviews. In: Aromataris E, Munn Z, editors. JBI manual for evidence synthesis; 2020.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 2020. Available from: http://www.prisma-statement.org/. Accessed 1 June 2020.
PHE. Public Health England (PHE). https://www.gov.uk/government/organisations/public-health-england. Accessed 16 Apr 2020.
Change UCfB. UCL centre for behaviour change. https://www.ucl.ac.uk/behaviour-change/. Accessed 16 Apr 2020.
NICE. National Institute for Health and Care Excellence (NICE) evidence search: https://www.evidence.nhs.uk/search. Accessed 16 Apr 2020.
Stern C, Jordan Z, McArthur A. Developing the review question and inclusion criteria. Am J Nurs. 2014;114(4):53–6.
Collins JA, Fauser BCJM. Balancing the strengths of systematic and narrative reviews. Hum Reprod Update. 2005;11(2):103–4.
Rycroft-Malone J, McCormack B, Hutchinson AM, DeCorby K, Bucknall TK, Kent B, et al. Realist synthesis: illustrating the method for implementation research. Implement Sci. 2012;7(1):33.
Pope C, Mays N. Qualitative research in health care. Hoboken: Wiley; 2013.
Graham-Rowe E, Lorencatto F, Lawrenson JG, Burr JM, Grimshaw JM, Ivers NM, et al. Barriers to and enablers of diabetic retinopathy screening attendance: a systematic review of published and grey literature. Diabet Med. 2018;35(10):1308–19.
Carlsen B, Glenton C, Pope C. Thou shalt versus thou shalt not: a meta-synthesis of GPs’ attitudes to clinical practice guidelines. Br J Gen Pract. 2007;57(545):971–8.
Ju I, Banks E, Calabria B, Ju A, Agostino J, Korda RJ, et al. General practitioners’ perspectives on the prevention of cardiovascular disease: systematic review and thematic synthesis of qualitative studies. BMJ Open. 2018;8(11):e021137.
Lucas PJ, Cabral C, Hay AD, Horwood J. A systematic review of parent and clinician views and perceptions that influence prescribing decisions in relation to acute childhood infections in primary care. Scand J Prim Health Care. 2015;33(1):11–20.
Schumann I. Physicians’ attitudes, diagnostic process and barriers regarding depression diagnosis in primary care: a systematic review of qualitative studies; 2012.
Sinnott C, McHugh S, Browne J, Bradley C. GPs’ perspectives on the management of patients with multimorbidity: systematic review and synthesis of qualitative research. BMJ Open. 2013;3(9):e003610.
Sirdifield C, Anthierens S, Creupelandt H, Chipchase SY, Christiaens T, Siriwardena AN. General practitioners’ experiences and perceptions of benzodiazepine prescribing: systematic review and meta-synthesis. BMC Fam Pract. 2013;14:191.
Vedel I, Puts MTE, Monette M, Monette J, Bergman H. Barriers and facilitators to breast and colorectal cancer screening of older adults in primary care: a systematic review. J Geriatr Oncol. 2011;2(2):85–98.
Vogt F, Hall S, Marteau TM. General practitioners’ and family physicians’ negative beliefs and attitudes towards discussing smoking cessation with patients: a systematic review. Addiction. 2005;100(10):1423–31.
Barley EA, Murray J, Walters P, Tylee A. Managing depression in primary care: a meta-synthesis of qualitative and quantitative research from the UK to identify barriers and facilitators. BMC Fam Pract. 2011;12:47.
De Vleminck A, Houttekier D, Pardon K, Deschepper R, van Audenhove C, Stichele RV, et al. Barriers and facilitators for general practitioners to engage in advance care planning: a systematic review. Scand J Prim Health Care. 2013;31(4):215–26.
Lawrence RA, McLoone JK, Wakefield CE, Cohn RJ. Primary care physicians’ perspectives of their role in cancer care: a systematic review. J Gen Intern Med. 2016;31(10):1222–36.
McDonagh LK, Saunders JM, Cassell J, Curtis T, Bastaki H, Hartney T, et al. Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: a systematic review. Implement Sci. 2018;13(1):130.
Mikat-Stevens NA, Larson IA, Tarini BA. Primary-care providers’ perceived barriers to integration of genetics services: a systematic review of the literature. Genet Med. 2015;17(3):169–76.
O'Brien D, Harvey K, Howse J, Reardon T, Creswell C. Barriers to managing child and adolescent mental health problems: a systematic review of primary care practitioners’ perceptions. Br J Gen Pract. 2016;66(651):e693–707.
Schadewaldt V, McInnes E, Hiller JE, Gardner A. Views and experiences of nurse practitioners and medical practitioners with collaborative practice in primary health care - an integrative review. BMC Fam Pract. 2013;14:132.
Yeung A, Temple-Smith M, Fairley C, Hocking J. Narrative review of the barriers and facilitators to chlamydia testing in general practice. Aust J Prim Health. 2015;21(2):139–47.
Zwolsman S, te Pas E, Hooft L, Wieringa-de Waard M, van Dijk N. Barriers to GPs’ use of evidence-based medicine: a systematic review. Br J Gen Pract. 2012;62(600):e511–21.
Tonkin-Crine S, Yardley L, Little P. Antibiotic prescribing for acute respiratory tract infections in primary care: a systematic review and meta-ethnography. J Antimicrob Chemother. 2011;66(10):2215–23.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
CASP. Critical Appraisal Skills Programme (CASP) appraisal checklists. Available from: https://casp-uk.net/casp-tools-checklists/. Accessed 1 June 2020.
Khan N, Rudoler D, McDiarmid M, Peckham S. A pay for performance scheme in primary care: Meta-synthesis of qualitative studies on the provider experiences of the quality and outcomes framework in the UK. BMC Fam Pract. 2020;21(1):142.
Eijkenaar F, Emmert M, Scheppach M, Schoffski O. Effects of pay for performance in health care: A systematic review of systematic reviews. Health Policy. 2013;110(2-3):115–30.
Campanella P, Vukovic V, Parente P, Sulejmani A, Ricciardi W, Specchia ML. The impact of public reporting on clinical outcomes: a systematic review and meta-analysis. BMC Health Serv Res. 2016;16:296.
Acknowledgements
LP is funded by a National Institute for Health Research (NIHR) Doctoral Research Fellowship. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
This review was led by MM as her Master’s in Public Health thesis at the London School of Hygiene and Tropical Medicine (LSHTM), no funding was received for this. LP is funded by a NIHR Doctoral Research Fellowship. No funding was received by SN.
Author information
Authors and Affiliations
Contributions
MM co-designed the project title and methods, conducted the searches, screening, selection, quality appraisal, data extraction, data analysis and synthesis, and drafted the report. LP co-designed the project title and methods and revised the draft. SN conducted screening, selection, quality appraisal, data extraction and data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA checklist.
Additional file 2.
Search strategy. Search concepts, keywords and MeSH terms used to derive search strategies. Search strategy.
Additional file 3.
Quality appraisal. Adapted scoring system for the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Systematic Reviews and Research Syntheses. Quality of empirical studies: appraisal instruments and quality scores. Quality appraisal criteria.
Additional file 4.
Additional data. Characteristics of included reviews.
Additional file 5.
Evidence mapping. Mapping of emergent themes to the Theoretical Domains Framework (TDF). Evidence table.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mather, M., Pettigrew, L.M. & Navaratnam, S. Barriers and facilitators to clinical behaviour change by primary care practitioners: a theory-informed systematic review of reviews using the Theoretical Domains Framework and Behaviour Change Wheel. Syst Rev 11, 180 (2022). https://doi.org/10.1186/s13643-022-02030-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-02030-2