
Abstract
Appropriate antibiotic treatment for critically ill patients with serious Gram-negative infections in the intensive care unit is crucial to minimize morbidity and mortality. Several new antibiotics have shown in vitro activity against carbapenem-resistant Enterobacterales (CRE) and difficult-to-treat resistant Pseudomonas aeruginosa. Cefiderocol is the first approved siderophore beta-lactam antibiotic with potent activity against multidrug-resistant, carbapenem-resistant, difficult-to-treat or extensively drug-resistant Gram-negative pathogens, which have limited treatment options. The spectrum of activity of cefiderocol includes drug-resistant strains of Acinetobacter baumannii, P. aeruginosa, Stenotrophomonas maltophilia, Achromobacter spp. and Burkholderia spp. and CRE that produce serine- and/or metallo-carbapenemases. Phase 1 studies established that cefiderocol achieves adequate concentration in the epithelial lining fluid in the lung and requires dosing adjustment for renal function, including patients with augmented renal clearance and continuous renal-replacement therapy (CRRT); no clinically significant drug–drug interactions are expected. The non-inferiority of cefiderocol versus high-dose, extended-infusion meropenem in all-cause mortality (ACM) rates at day 14 was demonstrated in the randomized, double-blind APEKS–NP Phase 3 clinical study in patients with nosocomial pneumonia caused by suspected or confirmed Gram-negative bacteria. Furthermore, the efficacy of cefiderocol was investigated in the randomized, open-label, pathogen-focused, descriptive CREDIBLE–CR Phase 3 clinical study in its target patient population with serious carbapenem-resistant Gram-negative infections, including hospitalized patients with nosocomial pneumonia, bloodstream infection/sepsis, or complicated urinary tract infections. However, a numerically greater ACM rate with cefiderocol compared with BAT led to the inclusion of a warning in US and European prescribing information. Cefiderocol susceptibility results obtained with commercial tests should be carefully evaluated due to current issues regarding their accuracy and reliability. Since its approval, real-world evidence in patients with multidrug-resistant and carbapenem-resistant Gram-negative bacterial infections suggests that cefiderocol can be efficacious in certain critically ill patient groups, such as those requiring mechanical ventilation for COVID-19 pneumonia with subsequently acquired Gram-negative bacterial superinfection, and patients with CRRT and/or extracorporeal membrane oxygenation. In this article, we review the microbiological spectrum, pharmacokinetics/pharmacodynamics, efficacy and safety profiles and real-world evidence for cefiderocol, and look at future considerations for its role in the treatment of critically ill patients with challenging Gram-negative bacterial infections.
Similar content being viewed by others

Introduction
Healthcare-associated infections, including hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), bloodstream infection (BSI), and catheter-associated complicated urinary tract infections (CA-UTI) are leading causes of morbidity and mortality in critically ill patients [1,2,3]. A driving factor in poor outcomes is a delay in the administration of appropriate antibiotics, particularly in patients with serious multidrug-resistant (MDR) infections [4,5,6,7], underlining the importance of recognizing risk factors for MDR pathogens [8]. In critically ill patients, the most concerning MDR pathogens are: carbapenem-resistant (CR) and difficult-to-treat resistant (DTR, i.e., not susceptible to all high-efficacy and low-toxicity antibiotics [4]) Pseudomonas aeruginosa; CR Acinetobacter baumannii; extended-spectrum beta-lactamase (ESBL)-producing and CR Enterobacterales (CRE); and Stenotrophomonas maltophilia [9,10,11,12,13,14,15].
In recent years, several new agents based on combinations of old beta-lactams and new beta-lactamase inhibitors with activity against highly resistant Gram-negative pathogens have been approved (e.g., ceftazidime–avibactam, meropenem–vaborbactam, imipenem–relebactam) [13]. Against this backdrop, we look at the role of the first siderophore cephalosporin antibiotic to be approved, cefiderocol. Developed specifically to target CR Gram-negative bacterial infections [16, 17], cefiderocol binds iron, an essential nutrient for bacterial growth, and enters bacterial cells not only by passive diffusion through porin channels but also through iron transport channels [16, 17]. Cefiderocol is mostly stable against a broad range of serine- and metallo-beta-lactamases (MBLs), although it can be weakly hydrolyzed by certain mutant isoforms of these enzymes [18,19,20,21]. Unlike for carbapenems and other standard-of-care beta-lactam antibiotics, porin loss and efflux pump upregulation mechanisms of antimicrobial resistance in Gram-negative bacteria have limited effect on the overall in vitro activity of cefiderocol [19, 22].
This review summarizes the published literature on the in vitro susceptibility of cefiderocol against highly resistant Gram-negative bacterial isolates across surveillance programs, mechanisms of resistance, pharmacokinetics (PK), PK/pharmacodynamics (PK/PD) in preclinical models of infections, and clinical data. It also discusses the characteristics of cefiderocol relative to recently approved beta-lactam–beta-lactamase inhibitor (BL–BLI) combinations, and covers overlapping and differential potential roles of cefiderocol and BL–BLIs in therapy within the current antibiotic landscape. Finally, consideration is given to future studies that would help to better define the role of cefiderocol relative to recently approved BL–BLIs in the treatment of patients with highly resistant infections.
Microbiology and spectrum of activity of cefiderocol
Cefiderocol has a broad spectrum of activity against aerobic Gram-negative bacteria frequently found in the intensive care unit (ICU), including MDR and CR strains of Enterobacterales, P. aeruginosa, A. baumannii, and S. maltophilia, the latter of which is intrinsically resistant to carbapenems [19, 23]. Cefiderocol has no in vitro activity against Gram-positive bacteria and anaerobes [19]. Clinical breakpoints for interpretation of the results of cefiderocol susceptibility testing are available from Clinical and Laboratory Standards Institute (CLSI), the US Food and Drug Administration (FDA) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) (Table 1) [24,25,26]. The interpretive criteria are not identical, which may result in discrepancies in categorization of isolates of the same species exhibiting the same cefiderocol minimum inhibitory concentration (MIC) values, depending on the breakpoint system adopted.
The in vitro activity of cefiderocol was investigated in large surveillance studies and in smaller independent investigations. Among 800 Gram-negative clinical isolates derived from ICU patients with infections of the lower respiratory tract (LRTI) and urinary tract (UTI), or with wound infection or BSI, cefiderocol MICs were ≤ 4 μg/mL against all isolates, including carbapenem–non-susceptible Enterobacterales, P. aeruginosa, and A. baumannii [27].
The 5-year multinational SIDERO surveillance program, based on CLSI breakpoints for all species, showed that 96.7% of CREs, 99.8% of CR strains of P. aeruginosa, 94.2% of CR strains of A. baumannii, and 98.6% of S. maltophilia were susceptible to cefiderocol [28]. Burkholderia spp. do not have CLSI susceptibility breakpoints; however, cefiderocol MIC90 was 0.5 μg/mL, suggesting low MIC values for most isolates [28]. For carbapenem–non-susceptible Achromobacter spp., the cefiderocol MIC90 was 4 μg/mL in a global collection of isolates [29].
High in vitro activity of cefiderocol against Enterobacterales, P. aeruginosa, A. baumannii, and S. maltophilia was also observed in the 2020 SENTRY multinational surveillance program. In addition, cefiderocol was the most potent antibiotic against the different resistance phenotypes (Table 2) [30]. Overall, 89.2–95.9% of Enterobacterales isolates resistant to imipenem–relebactam, meropenem–vaborbactam, or ceftazidime–avibactam were susceptible to cefiderocol according to CLSI criteria and 54.1–70.7% of the same isolates were susceptible to cefiderocol based on EUCAST criteria (Table 2) [30], reflecting the different breakpoints established by the two committees. Among P. aeruginosa isolates resistant to ceftolozane–tazobactam, imipenem–relebactam, or ceftazidime–avibactam, susceptibility rates of 88.3%, 100%, and 91.6% of isolates, respectively, were reported for cefiderocol by CLSI criteria and of 85%, 100%, and 89.2% of isolates by EUCAST criteria, respectively (Table 2) [30].
Cefiderocol susceptibility testing issues
The mechanism of cefiderocol entry into the bacterial cell requires expression of specific siderophore (iron transport) uptake systems under low iron concentrations encountered in infected tissues in vivo, which accounts for the remarkable spectrum of antimicrobial activity. This implies that the reference broth microdilution (BMD) for cefiderocol susceptibility testing must use iron-depleted medium to avoid misleading results (i.e., false resistance) [31,32,33]. While this prevented an easy addition of cefiderocol to panels used by several antimicrobial susceptibility testing (AST) platforms, some commercial systems for cefiderocol MIC testing have been developed. However, these systems were shown to be affected by accuracy, reproducibility, and bias issues [34,35,36,37]. According to EUCAST, disk diffusion can be used as a starting approach to cefiderocol testing by diagnostic laboratories, but results falling into the area of technical uncertainty (ATU) should either be confirmed by the reference BMD with iron-depleted, cation-adjusted Mueller–Hinton medium or cautionary considered indicative of resistance [37, 38], leading to an overall overestimation of resistance. In fact, it was shown that more than 20% of isolates of MDR Gram-negatives may yield cefiderocol results falling into the ATU when tested by disk diffusion [35]. Moreover, disk diffusion can also be affected by remarkable variability depending on the various combinations of disks and agar media manufacturers [34, 37]. Additional commercial systems for cefiderocol susceptibility testing have recently been developed, and evaluations of the available systems are underway with variable results [39,40,41,42,43].
Pharmacokinetics in healthy subjects and critically ill patients
In two Phase 1 studies in healthy subjects, single and multiple intravenous doses of cefiderocol up to 4000 mg were well-tolerated and exhibited a linear PK profile [44, 45]. Dose-proportional increases in maximum serum concentration (Cmax) and area under the concentration–time curve (AUC0-∞) were observed between 100 to 4000 mg [44, 45]. The mean plasma half-life of cefiderocol was 1.98–2.74 h and the PK of cefiderocol did not change with multiple dosing in healthy subjects [44]. Protein binding was estimated at approximately 58% in healthy subjects and was not significantly altered with renal impairment [46, 47]. Cefiderocol (1 g, 1-h infusion, radio-labeled) was primarily excreted unchanged in the urine, with metabolic pathways providing only minor excretion routes [48]. Following administration of cefiderocol 2 g, in 1-h infusion, the AUC (212.0 to 872.5 µg • h/mL) and half-life (2.8 to 9.6 h) increased and renal clearance decreased (4.7 to 1.1 L/h) in patients with mild, moderate or severe renal impairment (including those patients with or without hemodialysis) compared with subjects with normal renal function [47], suggesting that cefiderocol dose adjustment is needed with renal function. In vitro data demonstrating no interactions of cefiderocol with drug transporter systems have been confirmed in studies using furosemide, metformin, and rosuvastatin in healthy volunteers [49, 50]. In vitro data indicate that cefiderocol may induce CYP3A4 in the liver; thus, patients should be monitored for potential reduced efficacy when substrates of CYP3A4 enzyme are co-administered with cefiderocol [51]. Studies on epithelial lining fluid (ELF) penetration of cefiderocol confirmed its effective tissue penetration into the lung. In healthy volunteers, a single 2 g 1-h infusion resulted in ~ 24% ELF to plasma ratio of free cefiderocol [46].
Data are also available on the PK of cefiderocol in plasma and ELF in critically ill patients. In a small French study in seven ICU patients, mainly with VAP (six patients), the PK profile of cefiderocol at steady state was investigated after multiple dosing of 2 g, 3-h infusions [52]. The mean (± standard deviation [SD]) minimum serum concentration (Cmin) of cefiderocol prior to the start of infusion (C0) was 42.1 ± 20.1 mg/L, the mean Cmax was 77.1 ± 12.9 mg/L, the mean AUC0–8 h was 448 ± 155 mg • h/L and the half-life was 13 ± 11.3 h [52]. In one patient with augmented renal clearance (ARC), the half-life of cefiderocol was lower (1.4 h) than in the rest of the ICU population [52]. The PK of cefiderocol in critically ill patients has also been reported for five patients with septic shock due to MDR Gram-negative bacteria, all of whom had varying degrees of acute renal injury; three required continuous renal replacement therapy (CRRT), one required an additional cytokine adsorber, and two patients also required extracorporeal membrane oxygenation (ECMO) [53]. With a target of 100% for the percentage of time during the dosing period that the free drug concentration in the plasma exceeds the MIC (%fT>1×MIC; overall Cmin > 4 μg/mL), none of the initial or renally adapted dosing regimens were suboptimal. Cmin levels ranged between 25 and 70 μg/mL; however, there was a reduction in Cmin in a patient receiving cytokine adsorber therapy [53]. Cefiderocol half-life was prolonged for at least 8 h in all patients [53]. In a Phase 1b study in hospitalized patients with pneumonia under mechanical ventilation, the ELF penetration at steady state increased to ~ 54% after multiple dosing of cefiderocol 2 g in 3-h infusions [54].
The PK of cefiderocol have been further investigated to support dosing under CRRT and ECMO. A recent ex vivo investigation suggested that the effluent rate was the significant parameter determining the clearance of cefiderocol during CRRT. Based on these findings, dosing recommendations according to the effluent rate were incorporated into the cefiderocol prescribing information [49, 55, 56]. In an ex vivo investigation that compared the PK of cefiderocol relative to baseline conditions, cefiderocol concentrations in blood samples collected post-oxygenation were reduced in a similar trend between closed-loop ECMO circuits and the control chambers without an oxygenator [57]. In another study, samples collected from the ECMO circuit on day 9 suggested < 5% loss of cefiderocol, and plasma and lung trough concentrations also remained above the MIC of P. aeruginosa [58]. Collectively, these data suggest that there was no significant cefiderocol adsorption to the oxygenator membrane in the ECMO circuit and cefiderocol PK is not expected to be altered in patients with ECMO support [57].
Preclinical PK/PD investigations
Dose fractionation in vivo preclinical studies in neutropenic murine thigh and lung infection models demonstrated that the PD parameter most closely correlated with the efficacy of cefiderocol was the time the free concentration remained above the MIC (%fT>MIC) [59]. Based on the efficacy variable of 1-log reduction in bacterial growth, the PD target required to achieve in vivo efficacy differed by bacterial species (i.e., Enterobacterales 64% and 73% [lung, thigh], P. aeruginosa 70% and 72% [lung, thigh], A. baumannii 88% [lung], and S. maltophilia 54% [lung]) [59]. In another series of experiments investigating cefiderocol doses up to 250 mg/kg against P. aeruginosa in the neutropenic murine thigh infection model, in which 32% protein binding was applied to correct for free drug exposure, ~ 76%, 82%, or 88% T>MIC was required to achieve in vivo bacteriostatic effects, 1-log10, or 2-log10 killing, respectively [60].
The neutropenic murine thigh infection model was also used to investigate the potential susceptibility breakpoint for cefiderocol at humanized dosing (replicating exposures of 2 g, 3-h infusion every 8 h in humans) against various Gram-negative bacterial species with cefiderocol MICs of 0.12 to > 256 μg/mL [61]. Over 24 h, among isolates with cefiderocol MIC values up to 4 μg/mL, cefiderocol led to bacterial stasis or ≥ 1-log reduction in colony-forming unit (CFU) in 77% of Enterobacterales, 88% of A. baumannii, and 85% of P. aeruginosa isolates [61]. The suppression of bacterial growth (from stasis to cidal effects [i.e., ≥ 2-log10 reduction in CFU]) was sustained for up to 72 h against a total of four meropenem-susceptible and six meropenem-resistant strains of Enterobacterales, A. baumannii, and P. aeruginosa with cefiderocol MIC values up to 4 μg/mL in another neutropenic murine thigh infection model study [62]. Additional studies in the same model confirmed that sustained in vivo efficacy (up to 72 h) with cefiderocol can be obtained against CR A. baumannii without the emergence of in vivo resistance [63]. Humanized dosing of cefiderocol in this model was also efficacious against P. aeruginosa isolates with cefiderocol MIC values of 0.063–0.5 μg/mL, with a ≥ 2-log10 reduction in CFU at 24 h compared with vehicle-treated controls against all except one isolate [64]. Furthermore, the infusion duration selected for cefiderocol in Phase 3 trials was based on results from an immunocompetent rat respiratory tract infection model, which showed that a 3-h infusion of cefiderocol at humanized dosing showed enhanced efficacy against some isolates of A. baumannii and K. pneumoniae compared with a 1-h infusion of cefiderocol [65].
Synergism between cefiderocol and avibactam, amikacin, meropenem, and ampicillin–sulbactam at concentrations replicating exposures have been observed in an in vitro chemostat infection model against A. baumannii strains that were resistant to cefiderocol [66,67,68]. In a different in vitro study in time-kill curve experiments, against A. baumannii strains with cefiderocol MICs of 16–32 µg/mL, the combination of cefiderocol with generic drugs sulbactam, amikacin, and minocycline also showed synergism in suppression of bacterial growth [68]. In a recent investigation in the neutropenic murine thigh infection model, cefiderocol at humanized dosing in combination with meropenem, ceftazidime–avibactam, or ampicillin–sulbactam was more efficacious against cefiderocol-susceptible A. baumannii isolates (MIC = 2 µg/mL) relative to cefiderocol alone [69].
Dosing and population PK analyses
Based on the preclinical investigations, the standard dosing and infusion time of cefiderocol in patients with normal renal function was modeled as a 2 g, 3-h infusion every 8 h (q8h), which provided > 90% probability of target attainment (PTA) for Gram-negative bacteria with cefiderocol MIC values up to 4 µg/mL [70, 71]. Cefiderocol dosing for patients with renal impairment, initially modeled using PTAs for 75% fT>MIC, are as follows (all as a 3-h intravenous infusion): mild impairment (creatinine clearance [CrCl] estimated using Cockcroft–Gault equation in the final model as 60 to < 90 mL/min), 2 g q8h; moderate impairment (30 to < 60 mL/min), 1.5 g q8h; severe impairment (15 to < 30 mL/min), 1 g q8h; and end-stage renal disease (< 15 mL/min), 0.75 g q12h [70, 71]. Modeling suggests that a dose of 2 g q6h can provide the same PTA for patients with ARC (CrCl > 120 mL/min) as a dose of 2 g q8h in critically ill patients with normal renal function (Table 3) [71].
The abovementioned cefiderocol dosing regimens were utilized in critically ill patients with nosocomial pneumonia (NP), BSI, and cUTI in the randomized Phase 3 APEKS–NP and CREDIBLE–CR studies, the results of which studies are discussed below [72, 73]. In these Phase 3 studies, cefiderocol doses for treatment were based on renal function determined at screening and during therapy on days 3–4 [72, 73]. An analysis of 187 cefiderocol-treated patients, 120 of whom were in the ICU and > 20% of whom had ARC, reported no significant difference in Cmax and daily AUC according to renally adjusted dosing [74]. Geometric means of fCmin and %fT > MIC≤4 μg/mL were > 9 μg/mL and > 93%, respectively, indicating adequate exposure for the treatment of susceptible pathogens based on CLSI breakpoint (i.e., MIC ≤ 4 μg/mL), regardless of renal function, infection site, body size, and disease severity [74].
The PTA for cefiderocol was investigated in a population PK modeling study, developed using data from Phase 1–3 studies [71, 75] and involving 3427 plasma concentrations from 516 subjects (91 patients without infection and 425 patients with infection [i.e., pneumonia, BSI/sepsis, cUTI]) [71]. Cefiderocol plasma concentrations were described by a three-compartment model with a proportional error model for intraindividual variability [71]. The effects of CrCl and infection sites on clearance, body weight on volume of distribution in the central and peripheral compartments, albumin concentration and any infection site on the volume of distribution in the peripheral compartment were included in the final model [71]. CrCl was the most significant covariate on cefiderocol PK. The %fT>MIC was 100% in 97% of patients in both Phase 3 studies and the PTA for 100% fT>MIC was > 90% with MICs of ≤ 4 mg/mL for most infection sites and renal function groups [71]. No PK/PD correlation was found between plasma exposures and clinical outcomes, microbiological outcomes, or vital status, because the exposure level was very high in most patients [71, 75]. For simulated patients with infections caused by pathogens with cefiderocol MICs of ≤ 4 µg/mL, the PTA for 75% fT>MIC was > 95% for all infection sites and renal function groups, while for 100% fT>MIC, the PTA was > 90% for all infection sites and renal function groups, except for patients with BSI and normal renal function, in whom the PTA was 85% [71].
ELF concentrations were also explored in the population PK analysis of the Phase 3 studies. The estimated %fT>MIC,ELF was 100% in 89.3% of patients in CREDIBLE–CR and 97.9% of patients in APEKS–NP [75], supporting the adequacy of cefiderocol ELF concentrations to treat Gram-negative bacterial pneumonia caused by pathogens with a cefiderocol MIC of ≤ 4 mg/L [54, 76]. In Monte Carlo simulations for patients with NP, the PTA in ELF was found as > 99.5% for pathogens with cefiderocol MIC values ≤ 2 µg/mL and > 87% for MIC values of ≤ 4 µg/mL, across all renal function groups [76].
Compatibility and solubility for intravenous infusion
Cefiderocol has shown good compatibility with frequently used intravenous infusions for hospitalized patients, with a compatibility rate of 69% of 91 medicinal products in a Y-site simulated investigation [77]. Where medications (e.g., dobutamine hydrochloride, lorazepam, methylprednisolone acetate, propofol, rocuronium bromide, tobramycin sulfate, vancomycin hydrochloride) are not compatible with cefiderocol, separate intravenous catheter administration should be used [77]. The MINI-BAG Plus Container System and VIAL-MATE Adaptor (Baxter HealthCare Co., Deerfield, IL, USA) are both compatible with the cefiderocol 1 g vial, facilitating cefiderocol ease of use and minimizing the risk of contamination and environmental exposure [78].
Clinical experience
Efficacy
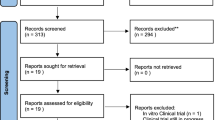
Cefiderocol has demonstrated efficacy in patients with serious infections in one randomized, prospective, Phase 2 (APEKS–cUTI) and two randomized, prospective, active-controlled or parallel-group Phase 3 (APEKS–NP, CREDIBLE–CR) clinical studies in critically ill patients with NP, BSI/sepsis, and cUTI, who were at risk of or were infected by MDR and CR Gram-negative pathogens (Additional file 1: Table S1) [72, 73, 79]. It should be noted that the APEKS–cUTI and APEKS–NP studies excluded patients with pathogens known to be CR at study entry as the comparator agent was a carbapenem. Upon reporting carbapenem resistance in the baseline pathogens by the local laboratory, physicians were permitted to discontinue the blinded treatment if patients did not respond to treatment [72, 79]. De-escalation of therapy was not feasible in the randomized APEKS–cUTI and APEKS–NP studies as patients received monotherapy [72, 79]. In the randomized CREDIBLE–CR study, de-escalation of adjunctive therapy was permitted based on local susceptibility reports; escalation of therapy after the early assessment visit was not permitted and administration of any other agent would be considered as “rescue therapy” for a patient without clinical improvement [73].
APEKS–cUTI
The randomized APEKS–cUTI study was designed to demonstrate the non-inferiority of cefiderocol (2 g, q8h, infused over 1 h) to imipenem–cilastatin (1 g/1 g, q8h, infused over 1 h) in hospitalized patients with complicated urinary tract infection [79]. The enrolled patient population was at risk of being infected by MDR Gram-negative bacteria, including P. aeruginosa. Most patients were aged > 65 years, > 50% of patients had moderate or severe renal impairment, and the study design allowed the enrollment of patients with immunosuppression and renal transplant [79]. The study results showed that cefiderocol treatment was non-inferior to imipenem–cilastatin treatment in the primary endpoint of composite of microbiological eradication and clinical cure at the test-of-cure visit (Additional file 1: Table S1) [79]. Serious adverse events were reported in 5% and 8% of patients in the cefiderocol and imipenem–cilastatin arms, respectively [79].
APEKS–NP
The randomized APEKS–NP study was conducted to demonstrate the non-inferiority of treatment with cefiderocol (2 g, q8h, 3-h infusion, 7–14 days) to high-dose, extended-infusion meropenem (2 g, q8h, 3-h infusion, 7–14 days) in day 14 all-cause mortality (ACM) rates among patients with Gram-negative NP [72]. A large proportion of the 292 patients included were critically ill, as shown by ICU admission (cefiderocol 70%, meropenem 66%), mechanical ventilation (cefiderocol 61%, meropenem 59%), Acute Physiology and Chronic Health Evaluation (APACHE) II scores ≥ 20 (cefiderocol 28%, meropenem 31%), age ≥ 75 years (cefiderocol 28%, meropenem 30%), and CrCl ≤ 50 mL/min (cefiderocol 33%, meropenem 35%) [72].
The study met its primary endpoint, with day 14 ACM rates of 12.4% with cefiderocol and 11.6% with meropenem (adjusted treatment difference 0.8%, 95% confidence interval (CI) –6.6 to 8.2) (Additional file 1: Table S1). In subgroup analyses, day 14 ACM rates were statistically comparable between treatments for patients with VAP, ventilated HAP, high APACHE II score and high Clinical Pulmonary Infection Score (CPIS), and ICU at randomization [72]. Comparable intertreatment-arm ACM rates were also seen at day 28, both overall (cefiderocol 21%, meropenem 21%) and for the most severely ill patients [72]. Furthermore, similar clinical cure and microbiological eradication rates were found between cefiderocol and meropenem arms by baseline Gram-negative pathogen (i.e., K. pneumoniae, P. aeruginosa, A. baumannii [including a proportion of meropenem-resistant isolates] and E. coli) [72].
CREDIBLE–CR
The randomized, open-label, pathogen-focused, descriptive, Phase 3 CREDIBLE–CR study investigated the efficacy of cefiderocol and best available therapy (BAT) in 150 patients with serious infections (NP, BSI/sepsis, or cUTI) caused by CR pathogens, including non-fermenters, such as CR P. aeruginosa or CR A. baumannii [73]. Being designed with relatively few exclusion criteria, the CREDIBLE–CR study was able to enroll patients with underlying conditions who would normally be excluded from randomized, non-inferiority, double-blind Phase 3 studies, such as the APEKS–NP study. The heterogeneous nature of a population comprising different infection types necessitated the use of primary endpoints defined by infection type [73, 80]. The critically ill status of the population was reflected in the rates of ICU admission at randomization (cefiderocol 56%, BAT 43%), mechanical ventilation (cefiderocol 50%, BAT 53%), APACHE II scores ≥ 20 (cefiderocol 29%, BAT 27%), age ≥ 75 years (cefiderocol 29%, BAT 29%), CrCl ≤ 50 mL/min (cefiderocol 43%, BAT 30%), and shock (cefiderocol 19%, BAT 12%) [73]. There was a similarity between the cefiderocol and BAT treatment arms at randomization in CPIS scores among ventilated patients, Sequential Organ Failure Assessment (SOFA) scores, and Charlson Comorbidity Index [73].
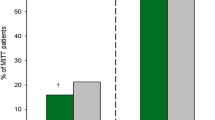
Clinical cure rates, as primary endpoint, at the test-of-cure visit were similar for cefiderocol and BAT in patients with NP (50% and 53%, respectively) and BSI/sepsis (43% in each arm) [73]. The primary endpoint of microbiological eradication rate for baseline pathogen from urine for patients with cUTI was numerically higher in patients treated with cefiderocol (cefiderocol 53%, BAT 20%) [73]. Despite similar rates of clinical and microbiological outcomes between treatment arms, overall mortality rates were numerically higher in the cefiderocol arm than in the BAT arm by day 28 (25% and 18%, respectively) and end of study (34% and 18%, respectively) (Additional file 1: Table S1) [73].
Sensitivity and subgroup analyses of the Phase 3 studies
Due to the higher observed ACM with cefiderocol relative to BAT in the CREDIBLE–CR study, several post-hoc analyses were performed. No single specific mortality risk factor was identified as a significant covariate on logistic regression modeling for the overall population [73]. The higher mortality rate in the cefiderocol arm was most apparent among patients with A. baumannii infections (cefiderocol 38%, BAT 18% at day 28; cefiderocol 50%, BAT 18% at end of study) [73]. Among patients without Acinetobacter spp. at randomization, mortality rates were similar between the cefiderocol and BAT arms at all visits (cefiderocol 15%, BAT 19% at day 28; cefiderocol 22%, BAT 19% at end of study) [73]. It is possible that imbalances in baseline factors within the heterogeneous population, together with limited stratification factors, contributed to the mortality differences between treatment arms [73, 81, 82]. The numerical differences between the treatment arms in ICU admission (cefiderocol 81%, BAT 47%), age ≥ 65 years (cefiderocol 62%, BAT 41%), Charlson Comorbidity Index ≥ 6 (cefiderocol 50%, BAT 35%), moderate or severe renal impairment (cefiderocol 33%, BAT 18%), and ongoing or prior shock (cefiderocol 26%, BAT 6%), point to the inclusion of more severely ill patients with CR Acinetobacter spp. in the cefiderocol arm compared with the BAT arm [73]. Most patients in the cefiderocol arm received monotherapy, while most patients in the BAT arm were treated with a combination of two or three antibiotics [73]. It is notable that the increased mortality rate in the cefiderocol arm was not linked to toxicity; the composite endpoint of survival and no change in antibiotic due to lack of therapeutic efficacy or emerging toxicity was reported in a similar proportion of patients in both treatment arms [73]. Furthermore, the observed mortality rate in the BAT arm for patients with CR A. baumannii infections was relatively low compared with rates in the control arms of previous randomized, controlled studies [82]. A post-hoc analysis of pneumonia patients infected by Acinetobacter spp. with meropenem MIC > 8 µg/mL in the double-blind, randomized APEKS–NP study showed comparable mortality rates at days 14 (cefiderocol: 28%, meropenem: 28%) and 28 (cefiderocol: 33%, meropenem: 39%) between cefiderocol and meropenem arms, respectively [72].
Based on the findings from the CREDIBLE–CR study, a “Warning and Precaution” (i.e., “Increase in all-cause mortality in patients with carbapenem-resistant Gram-negative bacterial infections: an increase in all-cause mortality was observed in cefiderocol-treated patients compared to those treated with best available therapy [BAT]) was added to the US prescribing information for cefiderocol. Although the cause of the increase in mortality has not been established, clinicians are advised to “closely monitor the clinical response to therapy in patients with cUTI and HABP/VABP" [49]. In addition, a special warning was included in the European Summary of Product Characteristics [51].
A subgroup analysis of the randomized APEKS–NP and CREDIBLE–CR studies confirmed the efficacy of cefiderocol in infections caused by CR Gram-negative pathogens harboring MBL enzymes (i.e., clinical cure: 70.8% and microbiological eradication: 58.3%), and no increased mortality was observed in these infections [83]. Among patients treated with comparators, clinical cure (40.0%) and microbiological eradication (30.0%) rates were lower than with cefiderocol [83]. The clinical benefit of cefiderocol treatment was consistent between the APEKS–NP and the CREDIBLE–CR studies [83]. K. pneumoniae harboring OXA-48 oxacillinase enzyme was detected across the CREDIBLE–CR and APEKS–NP studies in ten patients with cUTI, BSI/sepsis or pneumonia treated with cefiderocol [84]. All ten patients survived by day 28 and clinical cure at test of cure was reported for seven patients [84].
Given the role of iron channels in mediating cefiderocol entry into bacterial cells, the impact of patient iron levels on the clinical activity of cefiderocol merits attention. Anemia is not uncommon among critically ill patients and was reported for 8% of patients in each of the Phase 3 studies (see Safety section, below). A subgroup analysis of the APEKS–NP study showed that cefiderocol efficacy in critically ill patients with NP was not compromised by low serum iron levels at randomization [85] or by administration of iron supplementation in the form of blood transfusion or iron medications [85]. Of note, the majority of patients (~ 80%) had low baseline iron levels and this was most frequent among patients with ICU admission at randomization (71.9%) and those who were ventilated (63.2%) [85].
A post-hoc analysis of 84 patients with secondary bacteremia from the APEKS–cUTI, APEKS–NP, CREDIBLE–CR studies suggested that cefiderocol treatment may be an effective treatment in eradication of blood isolates of both carbapenem-susceptible and carbapenem-resistant Gram-negative species with low rates of persistence or recurrence [86].
Safety
As would be expected in a critically ill patient population, rates of treatment-emergent adverse events (TEAEs) were relatively high in both treatment arms in the randomized APEKS–NP and CREDIBLE–CR studies. In the APEKS–NP study, the most common TEAE occurring with cefiderocol among 148 patients in the safety population was cUTI (15.5%), followed by hypokalemia (10.8%), diarrhea (8.8%), anemia (8.1%), pneumonia (7.4%), aspartate aminotransferase increase and pleural effusion (6.8%, each), alanine aminotransferase increase (6.1%), and hypomagnesemia (5.4%). Discontinuation due to drug-related adverse events was rare in both treatment arms [72]. In the CREDIBLE–CR study, nearly all patients had at least one TEAE [73]. The most common TEAEs occurring among 101 patients receiving cefiderocol in the safety population were diarrhea (19%), pyrexia (14%), septic shock and vomiting (13% each), decubitus ulcer (10%), and hypokalemia (9%), with abnormal liver function test, constipation, hypotension, anemia, aspartate aminotransferase increase, and pleural effusion each being reported in 8% of patients, acute kidney injury, dyspnea, nausea, pneumonia, and alanine aminotransferase increase each occurring in 7% of patients, and abdominal pain, hypomagnesemia, thrombocytopenia, and chest pain each being reported in 6% of patients [73]. Three patients (3%) receiving cefiderocol and two patients (4%) receiving BAT discontinued study drug due to drug-related TEAEs [73]. Drug-related serious adverse events occurred in one patient (1%) in the cefiderocol arm and five patients (10%) in the BAT arm [73]. In the cefiderocol arm, 30% of patients had liver-related TEAEs, but many of these patients had confounding factors (e.g., hepatitis) [73].
Across all three clinical studies, seizures were reported in one patient receiving cefiderocol (with a history of epilepsy) in the APEKS–cUTI study, three events (one event of which was deemed a serious adverse event [SAE]) in the cefiderocol arm and two events in the meropenem arm in the APEKS–NP study, and one mild event in the cefiderocol arm and one SAE in the BAT arm in the CREDIBLE–CR study [87]. Clostridioides difficile infection was observed in similar proportions of patients in the cefiderocol and comparator treatment arms in the APEKS–NP study (four patients [3%] in both the cefiderocol and meropenem arms, respectively) [72], in the CREDIBLE–CR study (three patients [3%] in the cefiderocol arm and one patient [2%] in the BAT arm) [87], and in one patient (< 1%) in the cefiderocol arm and five patients (3%) in the imipenem–cilastatin arm of the APEKS–cUTI study [87]. C. difficile SAEs were reported only in the APEKS–cUTI study, in one patient receiving cefiderocol and in two patients receiving imipenem–cilastatin [87].
As well as looking at the role of iron-related parameters in terms of efficacy, as discussed earlier, consideration has been given to their impact on safety. In the CREDIBLE–CR study, 78.4% of the 134 patients randomized who had baseline serum iron data available had low iron levels (cefiderocol 76.2%, BAT 57.1%) [88]. Iron levels did not appear to influence safety. Day 28 ACM rates were similar in the subset of patients who received either blood transfusion or iron supplementation during antibiotic treatment (cefiderocol 23.8%, BAT 27.8%) and did not increase among patients without any supplementation (cefiderocol 25.4%, BAT 12.9%) [89]. In all three randomized clinical trials, safety parameters related to iron homeostasis (i.e., hepcidin, iron, total iron-binding capacity, transferrin saturation) were similar between treatment arms [72, 73, 85, 87, 89].
Real-world evidence
Several cases have been reported in which critically ill patients, often complicated with end-stage renal disease requiring CRRT, respiratory failure requiring ECMO, transplantation, hematological or solid cancer, other forms of immunosuppression, presence of coronavirus disease 2019 (COVID-19), burn wounds, or concurrent bacteremia, were successfully treated with cefiderocol either as monotherapy or in combination treatment (Table 4). Most patients had CR or extensively drug resistant (XDR) A. baumannii, CR or MDR P. aeruginosa, with CR K. pneumoniae and/or S. maltophilia co-infections, and clinical improvement or resolution was reported for the majority of patients. The mortality rates in case series reports (i.e., 23–55%) (Table 4) were similar to those observed in clinical studies [53, 58, 90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115].
The two largest real-world, observational, retrospective studies involved patients with CR A. baumannii infections, who received either cefiderocol or colistin-containing regimens [90, 91] (Table 4). In one of these two studies, 124 patients were diagnosed mainly with BSI (63.7%) and VAP (28.2%), approximately 90% of patients were in the ICU and 40% had COVID-19 pneumonia, and a small percentage required ECMO (~ 15% among cefiderocol-treated patients) or CRRT (~ 12%) during sepsis. Patients receiving cefiderocol had a significantly lower 30-day mortality rate than those receiving colistin therapy (34% versus 55.8%, respectively, p = 0.018). The lower mortality rate with cefiderocol treatment at days 14 and 28 was still significant for patients with BSI, but not for patients with VAP [90]. A multivariate analysis showed that septic shock, higher SOFA score, and age were linked with increased risk, and cefiderocol-containing treatment with lower risk of mortality [90]. The second study included 107 critically ill patients in the ICU with COVID-19 pneumonia requiring mechanical ventilation, who were colonized by CR A. baumannii prior to infection, and had high median SOFA score (cefiderocol 9, colistin-based 8). Patients had LRTI (41%) or BSI (58%). The clinical and microbiological cure rates were similar at day 14 in cefiderocol-treated patients and those receiving other antibiotics [91]. Despite clinical improvement by day 14 as indicated by improvements in SOFA score in both treatment groups, the 14-day and 28-day mortality rates were similar with cefiderocol monotherapy (40% and 55%, respectively) and colistin-based therapy (51% and 58%, respectively) [91].
Further real-world evidence on cefiderocol use and outcomes is provided by the ongoing PROVE retrospective chart review study in US and European hospitals [116, 117]. Among 76 patients with A. baumannii infections recorded as receiving cefiderocol, 18% had at least four major comorbid conditions, 13% had COVID-19 infection during index hospitalization, 54% were in the ICU, and 41% were receiving mechanical ventilation [116]. Altogether, 36% of infections were polymicrobial, with P. aeruginosa as the main accompanying pathogen (33%). Most (96%) A. baumannii isolates tested were CR. Cefiderocol was administered as monotherapy in 55% of patients and following failure on another Gram-negative antibiotic in 11% of patients. The overall clinical cure rate was 63% and the 30-day ACM rate was 21%; among the 76% of patients receiving cefiderocol within the first week of positive culture, the cure rate was 64% and the 30-day ACM rate was 21% [116]. An overall clinical cure rate of 63% and a 30-day ACM rate of 21% were also reported among 120 patients receiving cefiderocol for P. aeruginosa infections caused mainly by CR isolates (97% of 114 isolates tested) [117]. Among 85 (71%) patients receiving cefiderocol within a week of positive culture, the clinical cure and 30-day ACM rates were 65% and 21%, respectively. Of the total cohort of patients with P. aeruginosa infections, one-quarter of patients (23%) had at least four major comorbid conditions, 14% had COVID-19 infection during index hospitalization, 76% were in the ICU, and 55% were receiving mechanical ventilation. Polymicrobial infections were recorded in 36% of cases, mainly with A. baumannii (23%). Cefiderocol was administered mostly as monotherapy (68%) and 12% of patients received it following failure on another Gram-negative antibiotic [117].
Viale et al. conducted a systematic literature review involving 150 cefiderocol-treated patients in the real-world setting from 44 studies/reports [118]. The most frequent clinical diagnosis was pneumonia (22%), and P. aeruginosa and A. baumannii were the two most frequent pathogens [118]. The duration of cefiderocol treatment ranged between 2 weeks and > 6 weeks, although it was not reported for 35% of patients. Across all studies, the overall clinical response, microbiological cure, and mortality rates were 80%, 72%, and 35%, respectively [118].
A case series of patients with VAP and/or BSI caused by A. baumannii aimed to find an association between cefiderocol Cmin/MIC ratio and microbiological outcomes. In this investigation, four patients received ECMO support (one also received CRRT) and had either optimal or quasi-optimal Cmin/MIC ratios. ECMO support did not appear to have an influence on the microbiological result following cefiderocol treatment [94]. In a recent report, one patient without comorbid conditions, who developed VAP and sepsis, received ECMO and was infected by XDR/DTR A. baumannii, New Delhi metallo-beta-lactamase (NDM)-producing K. pneumoniae, and Candida auris. Following cefiderocol treatment with dose adjustment, clinical cure, microbiological cure was reported for the patient with survival at day 30 [112].
Resistance emergence on-therapy
Although clinical cases of resistance emerging during therapy have been reported [90, 101, 105, 119,120,121], resistance to cefiderocol remains relatively uncommon. It is likely that on-therapy resistance requires a variety of concurrently present mechanisms, such as increased expression of specific MBLs (e.g., NDM), mutations in AmpC beta-lactamase, siderophore receptors, and regulators of iron transport channels, and/or target (penicillin-binding protein-3) modifications [122, 123]. Reports indicate that certain mutations in iron-transport genes, which are species specific, do not increase cefiderocol MIC values consistently above the susceptibility breakpoints [19], unless other resistance mechanisms are also present [123]. A cefiderocol-resistant NDM-producing K. pneumoniae strain obtained in vitro and due to functional loss of the iron transporter gene cirA was outcompeted by the parent strain in vitro, thus showing a fitness defect that suggests this resistance mechanism has low propensity to disseminate in the absence of strong selective pressure [124]. However, an outbreak of highly cefiderocol-resistant NDM-producing K. pneumoniae causing clinical infections, and due mainly to clonal expansion of a mutant with an inactivated cirA gene, has recently been observed in the absence of strong selective pressure [125].
Increases of ≥ four-fold in the MICs emerged in similar proportions of patients receiving cefiderocol and comparator antibiotics in both the randomized CREDIBLE–CR study (cefiderocol 15% [A. baumannii, K. pneumoniae, P. aeruginosa and S. maltophilia] and BAT 13% [K. pneumoniae, A. baumannii, E. coli]) and the randomized APEKS–NP study (cefiderocol 5% [Enterobacter aerogenes, K. pneumoniae, E. cloacae and S. marcescens] and meropenem 4% [K. pneumoniae, P. aeruginosa and C. freundii]), although in most cases the elevated cefiderocol MIC did not reach resistance [72, 73, 126]. To date in real-world cases, on-therapy resistance during or after cefiderocol treatment were reported for two patients with CR P. aeruginosa infections [101, 105], three patients with CRE infections [119, 120, 127], and five patients with CR or XDR A. baumannii infections [90, 121]. Regular monitoring of resistance emergence is needed for clinical use of cefiderocol.
Role of cefiderocol in the ICU
Overall, published data indicate that cefiderocol is a useful addition to the antibiotic armamentarium against CRE, DTR-P. aeruginosa, CR A. baumannii, and rare species, such as Achromobacter spp., S. maltophilia or Burkholderia spp. [13, 14, 19, 23, 30, 72, 73]. Preclinical studies confirm that standard dosing leads to bactericidal activity of cefiderocol and population PK analyses show adequate exposure in plasma and ELF for the treatment of infections with cefiderocol MIC values up to 4 µg/mL across all renal function groups [71, 76]. Phase 3 clinical studies showed similar or statistically comparable efficacy in critically ill patients between cefiderocol and comparator antibiotics at standard and renal function-adjusted doses, including patients with ARC [72, 73]. In addition, clinical studies and real-world case reports in critically ill patients also confirm the similar safety of cefiderocol to other beta-lactams, and that an increase in ACM rates in the cefiderocol arm of the randomized CREDIBLE–CR study was not due to toxicity. In the randomized CREDIBLE–CR study, notable baseline imbalances were observed between the two treatment arms among patients with CR A. baumannii infections, making interpretation of efficacy and ACM findings difficult [73]. This is further complicated by the finding that ACM among patients in the BAT arm with CR A. baumannii infections was substantially lower relative to the rates observed with other treatments in previous randomized, controlled studies [82]. Further studies are required to clarify the role of cefiderocol treatment for the patient population in which it is intended to be used.
Comparative clinical data with cefiderocol and other newer beta-lactam antibiotics are scarce. Surveillance studies have demonstrated that a large proportion of Gram-negative isolates are susceptible to cefiderocol even if they are non-susceptible to the newer BL–BLI agents (Table 2) [28, 30]. Cross-resistance between cefiderocol and the new BL–BLIs has been observed to be rare. Pathogens are also likely to remain susceptible to cefiderocol when the isolates carry an MBL gene or porin mutations [19]. Furthermore, cefiderocol is the only beta-lactam antibiotic that has activity against most clinically relevant, problematic non-fermenter species such as P. aeruginosa, A. baumannii complex, S. maltophilia, Achromobacter spp., and B. cepacia complex frequently encountered in the ICU or in certain patient groups (e.g., colonization in patients with cystic fibrosis [CF]) [19, 28]. Against P. aeruginosa resistant or not susceptible to a range of common antipseudomonal antibiotics, cefiderocol MICs ranged between ≤ 0.06 and 4 μg/mL for 98.3% of all isolates, and susceptibility rates were 97.4% and 97.9% against XDR and MDR isolates, respectively [128]. Thus, cefiderocol has the broadest spectrum in terms of species and resistance mechanisms present in CR Gram-negative pathogens (Table 5) [13, 19, 28, 30].
Positioning within expert guidelines is another useful way to assess the relative merits of newer and established agents [129,130,131,132,133,134]. The European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines [129] reviewed all available clinical evidence for each antibiotic through PICO questions (i.e., patients, intervention, comparator, outcome). However, because current recommendations by ESCMID for or against newer antibiotics in the treatment of severe CRE infections, DTR P. aeruginosa, and CR A. baumannii infections are often supported by low-quality evidence, the role of some of the newer antibiotics remains unclear [129]. Gatti et al. have developed different treatment algorithms based on types of resistance mechanism and infection [132,133,134]. These Italian recommendations are aligned in general with the ESCMID guidelines in that the recommendations for cefiderocol are cautious and its use in critically ill patients should be targeted to CRE, CR P. aeruginosa, and CR A. baumannii infections with certain resistance mechanisms when in vitro activity is confirmed [132,133,134]. The two Infectious Diseases Society of America (IDSA) guidances are based on anatomical infection site, resistance mechanisms, and species [130, 131]. Cefiderocol is recommended as an alternative treatment option for patients with complicated UTIs caused by CRE, for infections outside the urinary tract caused by MBL-producing CRE, or as an alternative agent for CRE infections outside the urinary tract due to KPC-producers [130]. In UTIs caused by DTR P. aeruginosa, cefiderocol is one of the preferred treatment options, and for infections outside the urinary tract, cefiderocol is an alternative option [130]. For the treatment of CR A. baumannii and moderate/severe S. maltophilia infections, cefiderocol is recommended in combination with other agents [131].
Consistent with best antibiotic stewardship practices, cefiderocol use should be considered as an early targeted treatment option in patients in whom an XDR, DTR, CR, or MDR infection is highly suspected or documented given the deleterious outcomes associated with delayed receipt of effective therapy [99]. However, susceptibility testing even for cefiderocol is highly recommended to ensure treatment of susceptible pathogens [99, 100]. Among the testing methods that have been developed, currently, the BMD method with iron-depleted medium provides consistently accurate susceptibility results for cefiderocol [24, 26]. Patients with an increased likelihood of MDR Gram-negative bacterial infection include those with prior hospitalization, prior antibiotic use within 90 days, previous infection or colonization with a drug-resistant bacteria in the gut, urinary tract or respiratory tract, age > 70 years, diabetes mellitus, chronic obstructive pulmonary disease, or malignancy; poor infection control in hospital, travel to endemic areas, and high rate of local antimicrobial resistance are also contributing factors [9, 10, 135, 136]. For ICU-acquired pneumonia or VAP, individual patient factors such as septic shock at the time of VAP, acute respiratory distress syndrome or acute renal replacement therapy prior to VAP, and chronic liver disease are also linked with increased risk of MDR infections [9, 10, 136, 137]. Real-world data show that over 10% of critically ill patients in the ICU with A. baumannii and P. aeruginosa infections, in whom cefiderocol is expected to also be an appropriate antibiotic choice [28, 30], currently receive cefiderocol as a last-resort antibiotic [116, 117]. Because cefiderocol susceptibility testing may lengthen times to obtain MIC results, the initiation of therapy in some clinical settings should not be delayed given the high susceptibility rates among most Gram-negative pathogens, which could be followed by de-escalation of therapy. Further clinical experience is needed to explore whether cefiderocol treatment, administered to at-risk patients prior to treatment failure with other antibiotics, is associated with improved outcomes.
Like other antibiotics for patients with VAP, optimal duration of cefiderocol merits further investigation. In the randomized APEKS–NP and CREDIBLE–CR Phase 3 studies, patients with pneumonia and BSI/sepsis received cefiderocol treatment on average of 10–11 days [72, 73]. However, data are conflicting on the optimal duration of therapy for patients with VAP. According to the ATS/IDSA guidelines, a 7-day treatment is recommended for patients with HAP or VAP when improvement in signs and symptoms can be detected early. However, prolonged treatment should be considered for patients without clinical improvement or for those complicated with secondary bacteremia [138]. In a prospective controlled study in France, the non-inferiority of short-term (8 days) versus long-term (15 days) antibiotic treatment could not be established in patients with VAP caused by P. aeruginosa, and the study was stopped early due to slow enrolment. A tendency was seen towards a more frequent recurrence among patients receiving a short-term treatment, but no impact was found on 28-day mortality rate, length of ICU stay, and duration of mechanical ventilation [139]. In contrast, in a meta-analysis of randomized clinical studies comparing the outcomes after short-term and long-term antibiotic treatment courses in patients with VAP, and specifically in the subgroup of patients with non-fermenting Gram-negative bacteria, no significant differences in the rates of recurrence or relapse were found [140]. However, delay in appropriate antibiotics is known to impact mortality rates in such at-risk patient populations. A recent study has shown that improvement in identification of MDR Gram-negative pathogens with specific resistance profile through a streamlined microbiology workflow shortens the time to select appropriate antibiotics [141]. Such intervention, combined with shorter treatment duration, potentially can have a favorable impact on patient outcomes and may result in equal rates of overall clinical and microbiological response as longer treatment duration. However, after end of antibiotic treatment, monitoring of patients is warranted to detect any relapse or superinfection that would require additional courses of antibiotic treatment, particularly among patients with risk factors for drug-resistant pathogens [138].
Future directions
Future studies are needed to better define the clinical role of cefiderocol for critically ill patients with highly resistant Gram-negative infections. One area concerns combination therapy. Despite limited randomized Phase 3 clinical trial data (with cefiderocol being delivered exclusively as monotherapy in APEKS–NP and mainly as monotherapy [70–80%] in CREDIBLE–CR [72, 73]), real-world evidence supports the use of cefiderocol both as monotherapy and in combination [53, 58, 90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117]. This needs to be further investigated in clinical trials and optimal combination partners should be determined. Previous work with the in vitro chemostat model and the in vivo murine infection models point to the use of avibactam, amikacin and ampicillin/sulbactam [66,67,68,69].
Accurate systems for easy and ready-to-use susceptibility testing of cefiderocol by diagnostic laboratories are needed for improving drug prescription practice for definitive chemotherapy of infections caused by Gram-negative pathogens with limited treatment options. While initial testing by disk diffusion followed by confirmation of uncertain results by reference BMD with iron-depleted medium can be an acceptable option, evaluations of novel commercial testing systems will eventually indicate reliable alternatives in the future.
The need for routine therapeutic drug monitoring (TDM) in the ICU is still being debated [142,143,144,145]. Data from more than 500 patients in the Phase 1–3 clinical studies and population PK modeling suggest that in general routine TDM is not essential, because the current cefiderocol dosing recommendations are likely to achieve the PD target predicted by preclinical animal studies with very high probability in all infection types [70, 71, 76]. However, certain patient groups, such as those requiring CRRT and/or ECMO, may benefit from routine TDM [145], particularly when beta-lactam antibiotics are used for their treatment [142, 143]. Currently, data from cefiderocol TDM studies for cefiderocol are sparse [94, 97] and the contribution of host factors to outcomes cannot be discounted [94]. Two ongoing Phase 1 clinical studies (clinicaltrials.gov NCT04995835 and NCT05373615) may clarify dosing needs for these specific patient populations.
The emergence of resistance in clinical practice is a consideration for all new antibiotics. While the current level of non-susceptibility to cefiderocol based on CLSI breakpoints is very low (i.e., CRE 1.8%, XDR P. aeruginosa 2.8%, CR A. baumannii 4.2%) [30], resistant isolates may develop and spread [121]. On-therapy resistance development should be monitored, especially for patients with recurrent infections or for non-responders. Rapid diagnostic testing to identify the causative pathogen and underlying carbapenem resistance mechanisms [8] should be more widely adopted and used together with risk factor assessment to ensure an appropriate targeted approach in patient populations for whom timing of appropriate antibiotic treatment is critical.
Future clinical trials are required to help refine the role of cefiderocol in the management of seriously ill patients with CR Gram-negative bacterial infections. For example, the ongoing phase 2 GAMECHANGER trial is investigating the efficacy of cefiderocol versus investigator-determined BAT (within 48 h of the index blood culture) for patients with healthcare-associated and hospital-acquired Gram-negative BSI [146]. The trial is due to be completed in the first quarter of 2023. Additional information will also be provided by ongoing PK studies in patients with CF and pulmonary exacerbation (NCT05314764), as well as critically ill patients requiring ECMO (NCT04995835) or CRRT (NCT05373615). Finally, it will be essential to continue to monitor the benefits of cefiderocol opposite newer antibiotics as they enter the clinical arena.
Conclusions
Based on the reviewed clinical evidence, dosing recommendations, including for patients with severe renal impairment, CRRT or ARC, as well as PK/PD and safety profiles, cefiderocol can be regarded as one of the treatment options available for CR Gram-negative infections in critically ill patients in the ICU, either as monotherapy or in combination. Consideration should be given to the severity of illness and/or the potential for resistance emergence. Risk factors associated with mortality should be carefully considered when antibiotic treatment, including cefiderocol, is selected for patients in the ICU.
Availability of data and materials
Not applicable.
Abbreviations
- ACM:
-
All-cause mortality
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- ARC:
-
Augmented renal clearance
- AST:
-
Antimicrobial susceptibility testing
- ATU:
-
Area of technical uncertainty
- AUC:
-
Area under the concentration–time curve
- BAT:
-
Best available therapy
- BL–BLI:
-
Beta-lactam–beta-lactamase inhibitor
- BMD:
-
Broth microdilution
- BSI:
-
Bloodstream infection
- CAP:
-
Community-acquired pneumonia
- CA-UTI:
-
Catheter-associated complicated urinary tract infection
- CF:
-
Cystic fibrosis
- CFU:
-
Colony-forming unit
- CI:
-
Confidence interval
- CLSI:
-
Clinical and Laboratory Standards Institute
- Cmax :
-
Maximum serum concentration
- Cmin :
-
Minimum serum concentration
- COVID-19:
-
Coronavirus disease 2019
- CPIS:
-
Clinical Pulmonary Infection Score
- CR:
-
Carbapenem resistant
- CrCl:
-
Creatinine clearance
- CRE:
-
Carbapenem-resistant Enterobacterales
- CRRT:
-
Continuous renal replacement therapy
- cUTI:
-
Complicated urinary tract infection
- DTR:
-
Difficult-to-treat resistant
- ECMO:
-
Extracorporeal membrane oxygenation
- eGFR:
-
Estimated glomerular filtration rate
- ELF:
-
Epithelial lining fluid
- ESBL:
-
Extended-spectrum beta-lactamase
- ESCMID:
-
European Society of Clinical Microbiology and Infectious Diseases
- EUCAST:
-
European Committee on Antimicrobial Susceptibility Testing
- FDA:
-
US Food and Drug Administration
- %fT>MIC :
-
Percentage of time during the dosing period that the free drug concentration in the plasma exceeds the MIC
- HABP:
-
Hospital-acquired bacterial pneumonia
- HAP:
-
Hospital-acquired pneumonia
- HCAP:
-
Healthcare-associated pneumonia
- ICU:
-
Intensive care unit
- IDSA:
-
Infectious Diseases Society of America
- IQR:
-
Interquartile range
- IV:
-
Intravenous
- LRTI:
-
Lower respiratory tract infection
- MBL:
-
Metallo-beta-lactamase
- MDR:
-
Multidrug resistant
- MIC:
-
Minimum inhibitory concentration
- NDM:
-
New Delhi metallo-beta-lactamase
- NP:
-
Nosocomial pneumonia
- OXA:
-
Oxacillinase
- PD:
-
Pharmacodynamics
- PDR:
-
Pandrug resistant
- PICO:
-
Patients, Intervention, Comparator, Outcome
- PK:
-
Pharmacokinetic
- PTA:
-
Probability of target attainment
- q8h:
-
Every 8 h
- SAE:
-
Serious adverse event
- SARS-CoV-2:
-
Severe Acute Respiratory Syndrome coronavirus-2
- SD:
-
Standard deviation
- SOFA:
-
Sequential organ failure assessment
- TDM:
-
Therapeutic drug monitoring
- TEAE:
-
Treatment-emergent adverse events
- TOC:
-
Test of cure
- UTI:
-
Urinary tract infection
- VABP:
-
Ventilator-associated bacterial pneumonia
- VAP:
-
Ventilator-associated pneumonia
- XDR:
-
Extensively drug resistant
References
Esperatti M, Ferrer M, Giunta V, Ranzani OT, Saucedo LM, Li Bassi G, et al. Validation of predictors of adverse outcomes in hospital-acquired pneumonia in the ICU. Crit Care Med. 2013;41:2151–61.
Cai B, Echols R, Magee G, Arjona Ferreira JC, Morgan G, Ariyasu M, et al. Prevalence of carbapenem-resistant Gram-negative infections in the United States predominated by Acinetobacter baumannii and Pseudomonas aeruginosa. Open Forum Infect Dis. 2017;4:ofx76.
Rosenthal VD, Yin R, Valderrama-Beltran SL, Gualtero SM, Linares CY, Aguirre-Avalos G, et al. Multinational prospective cohort study of mortality risk factors in 198 ICUs of 12 Latin American countries over 24 years: the effects of healthcare-associated infections. J Epidemiol Glob Health. 2022;12:504–15.
Kadri SS, Adjemian J, Lai YL, Spaulding AB, Ricotta E, Prevots DR, et al.; National Institutes of Health Antimicrobial Resistance Outcomes Research Initiative (NIH–ARORI). Difficult-to-treat resistance in Gram-negative bacteremia at 173 US hospitals: retrospective cohort analysis of prevalence, predictors, and outcome of resistance to all first-line agents. Clin Infect Dis. 2018;67:1803–14.
Bonine NG, Berger A, Altincatal A, Wang R, Bhagnani T, Gillard P, et al. Impact of delayed appropriate antibiotic therapy on patient outcomes by antibiotic resistance status from serious Gram-negative bacterial infections. Am J Med Sci. 2019;357:103–10.
Lodise TP, Berger A, Altincatal A, Wang R, Bhagnani T, Gillard P, et al. Antimicrobial resistance or delayed appropriate therapy—does one influence outcomes more than the other among patients with serious infections due to carbapenem-resistant versus carbapenem-susceptible Enterobacteriaceae? Open Forum Infect Dis. 2019;6:ofz194.
Kollef MH, Shorr AF, Bassetti M, Timsit JF, Micek ST, Michelson AP, et al. Timing of antibiotic therapy in the ICU. Crit Care. 2021;25:360.
Bassetti M, Kanj SS, Kiratisin P, Rodrigues C, Van Duin D, Villegas MV, et al. Early appropriate diagnostics and treatment of MDR Gram-negative infections. JAC Antimicrob Resist. 2022;4:dlac089.
Fernández-Barat L, Ferrer M, De Rosa F, Gabarrús A, Esperatti M, Terraneo S, et al. Intensive care unit-acquired pneumonia due to Pseudomonas aeruginosa with and without multidrug resistance. J Infect. 2017;74:142–52.
Bassetti M, Righi E, Vena A, Graziano E, Russo A, Peghin M. Risk stratification and treatment of ICU-acquired pneumonia caused by multidrug-resistant/extensively drug-resistant/pandrug-resistant bacteria. Curr Opin Crit Care. 2018;24:385–93.
Strich JR, Kadri SS. Difficult-to-treat antibiotic-resistant Gram-negative pathogens in the intensive care unit: epidemiology, outcomes, and treatment. Semin Respir Crit Care Med. 2019;40:419–34.
Vincent JL, Sakr Y, Singer M, Martin-Loeches I, Machado FR, Marshall JC, et al.; EPIC III Investigators. Prevalence and outcomes of infection among patients in intensive care units in 2017. JAMA. 2020;323:1478–87.
Karvouniaris M, Pontikis K, Nitsotolis T, Poulakou G. New perspectives in the antibiotic treatment of mechanically ventilated patients with infections from Gram-negatives. Expert Rev Anti Infect Ther. 2021;19:825–44.
Niederman MS, Baron RM, Bouadma L, Calandra T, Daneman N, De Waele J, et al. Initial antimicrobial management of sepsis. Crit Care. 2021;25:307.
Tacconelli E, Carrara E, Savoldi A, Harbarth S, Mendelson M, Monnet DL, et al.; WHO Pathogens Priority List Working Group. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18:318–27.
Ito A, Nishikawa T, Matsumoto S, Yoshizawa H, Sato T, Nakamura R, et al. Siderophore cephalosporin cefiderocol utilizes ferric iron transporter systems for antibacterial activity against Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2016;60:7396–401.
Aoki T, Yoshizawa H, Yamawaki K, Yokoo K, Sato J, Hisakawa S, et al. Cefiderocol (S-649266), a new siderophore cephalosporin exhibiting potent activities against Pseudomonas aeruginosa and other gram-negative pathogens including multi-drug resistant bacteria: structure activity relationship. Eur J Med Chem. 2018;155:847–68.
Ito-Horiyama T, Ishii Y, Ito A, Sato T, Nakamura R, Fukuhara N, et al. Stability of novel siderophore cephalosporin S-649266 against clinically relevant carbapenemases. Antimicrob Agents Chemother. 2016;60:4384–6.
Ito A, Sato T, Ota M, Takemura M, Nishikawa T, Toba S, et al. In vitro antibacterial properties of cefiderocol, a novel siderophore cephalosporin, against Gram-negative bacteria. Antimicrob Agents Chemother. 2017;62:e01454-e1517.
Ito A, Nishikawa T, Ota M, Ito Horiyama T, Ishibashi N, Sato T, et al. Stability and low induction propensity of cefiderocol against chromosomal AmpC β-lactamases of Pseudomonas aeruginosa and Enterobacter cloacae (Erratum in J Antimicrob Chemother. 2019;74:539). J Antimicrob Chemother. 2018;73:3049–52.
Poirel L, Sadek M, Nordmann P. Contribution of PER-type and NDM-type β-lactamases to cefiderocol resistance in Acinetobacter baumannii. Antimicrob Agents Chemother. 2021;65: e0087721.
David S, Wong JLC, Sanchez-Garrido J, Kwong HS, Low WW, Morecchiato F, et al. Widespread emergence of OmpK36 loop 3 insertions among multidrug-resistant clones of Klebsiella pneumoniae. PLoS Pathog. 2022;18: e1010334.
Sato T, Yamawaki K. Cefiderocol: discovery, chemistry, and in vivo profiles of a novel siderophore cephalosporin. Clin Infect Dis. 2019;69(Suppl. 7):S538–43.
Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 32nd ed. CLSI Supplement M100. Wayne, PA: 2022.
Food and Drug Administration. FDA-Recognized Antimicrobial Susceptibility Test Interpretive Criteria. Cefiderocol injection. 2021. https://www.fda.gov/drugs/development-resources/cefiderocol-injection. Accessed 23 Sept 2022.
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 13.0, 2023. http://www.eucast.org.
Golden AR, Adam HJ, Baxter M, Walkty A, Lagacé-Wiens P, Karlowsky JA, et al. In vitro activity of cefiderocol, a novel siderophore cephalosporin, against Gram-negative bacilli isolated from patients in Canadian intensive care units. Diagn Microbiol Infect Dis. 2020;97: 115012.
Karlowsky JA, Hackel MA, Takemura M, Yamano Y, Echols R, Sahm DF. In vitro susceptibility of Gram-negative pathogens to cefiderocol in five consecutive annual multinational SIDERO-WT surveillance studies, 2014 to 2019. Antimicrob Agents Chemother. 2022;66: e0199021.
Nakai R, Makino A, Hama H, Yoshitomi T, Nakamura R, Hackel M, et al. In vitro and in vivo antimicrobial activity of cefiderocol and comparators against Achromobacter spp. Open Forum Infect Dis. 2021;8(Suppl. 1):S625–6.
Shortridge D, Streit JM, Mendes R, Castanheira M. In vitro activity of cefiderocol against U.S. and European Gram-negative clinical isolates collected in 2020 as part of the SENTRY Antimicrobial Surveillance Program. Microbiol Spectr. 2022;10(2):e0271221.
Hackel MA, Tsuji M, Yamano Y, Echols R, Karlowsky JA, Sahm DF. Reproducibility of broth microdilution MICs for the novel siderophore cephalosporin, cefiderocol, determined using iron-depleted cation-adjusted Mueller-Hinton broth. Diagn Microbiol Infect Dis. 2019;94:321–5.
European Committee on Antimicrobial Susceptibility Testing. Guidance document on broth microdilution testing of cefiderocol BMD. 2020. www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Guidance_documents/Cefiderocol_MIC_testing_EUCAST_guidance_document_201217.pdf
Marchetti P, Sanchez C, Echegorry M, Olivieri L, Ramirez MS, Faccone D, et al. Comparison of iron-depleted (ID) versus cation-adjusted Mueller-Hinton broth (CAMHB) media for cefiderocol susceptibility among carbapenemase-producing Enterobacterales (CPEs). Presented at 33rd European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark. 15–18 April 2023; P0388.
Devoos L, Biguenet A, Rousselot J, Bour M, Plésiat P, Fournier D, et al. Performance of discs, sensititre EUMDROXF microplates and MTS gradient strips for the determination of the susceptibility of multidrug-resistant Pseudomonas aeruginosa to cefiderocol. Clin Microbiol Infect. 2023;29(5): 652.e1-652.e8. https://doi.org/10.1016/j.cmi.2022.12.021.
Bonnin RA, Emeraud C, Jousset AB, Naas T, Dortet L. Comparison of disk diffusion, MIC test strip and broth microdilution methods for cefiderocol susceptibility testing on carbapenem-resistant Enterobacterales. Clin Microbiol Infect. 2022;28:1156.e1-1156.e5.
Bovo F, Lazzarotto T, Ambretti S, Gaibani P. Comparison of broth microdilution, disk diffusion and strip test methods for cefiderocol antimicrobial susceptibility testing on KPC-producing Klebsiella pneumoniae. Antibiotics (Basel). 2023;12:614.
European Committee on Antimicrobial Susceptibility Testing. EUCAST warnings concerning antimicrobial susceptibility testing products or procedures. https://www.eucast.org/ast-of-bacteria/warnings. Accessed 14 Apr 2023.
Matuschek E, Longshaw C, Takemura M, Yamano Y, Kahlmeter G. Cefiderocol: EUCAST criteria for disc diffusion and broth microdilution for antimicrobial susceptibility testing. J Antimicrob Chemother. 2022;77:1662–9.
Asensio Gallego S, Lopez Cerero L, Portillo Calderon I, Delgado Valverde M, Pascual A. Difficulties with cefiderocol susceptibility testing: assessment of commercial available methods with carbapenem resistant Gram-negative bacteria. Presented at 33rd European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark. 15–18 April 2023; P0327.
Dortet L, Niccolai C, Pfennigwerth N, Frisch S, Gonzalez C, Antonelli A, et al. Performance evaluation of the UMIC cefiderocol to determine MIC in Gram-negative bacteria. Presented at 33rd European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark. 15–18 April 2023; O0964.
Merino Garcia P, Barrio B, Culebras E, Rios E, Delgado-Iribarren A, Rodriguez-Avial I. In vitro activity of cefiderocol against carbapenem-resistant Gram-negative bacilli: comparative evaluation of broth microdilution, agar dilution prepared with iron depleted Mueller-Hinton broth, disk diffusion and UMIC Cefiderocol®. Presented at 33rd European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark. 15–18 April 2023; P0352.
Mezcord V, Wong O, Lopez C, Georgeos N, Fua V, Ozuna A, et al. Comparison of methods to determine Acinetobacter cefiderocol (CFD) susceptibility: are the results comparable between the different assays? Presented at 33rd European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark. 15–18 April 2023; P0380.
Bianco G, Boattini M, Comini S, Banche G, Cavallo R, Costa C. Disc diffusion and ComASP® cefiderocol microdilution panel to overcome the challenge of cefiderocol susceptibility testing in clinical laboratory routine. Antibiotics (Basel). 2023;12:604.
Saisho Y, Katsube T, White S, Fukase H, Shimada J. Pharmacokinetics, safety, and tolerability of cefiderocol, a novel siderophore cephalosporin for Gram-negative bacteria, in healthy subjects. Antimicrob Agents Chemother. 2018;62:e02163-e2217.
Sanabria C, Migoya E, Mason JW, Stanworth SH, Katsube T, Machida M, et al. Effect of cefiderocol, a siderophore cephalosporin, on QT/QTc interval in healthy adult subjects. Clin Ther. 2019;41:1724-36.e4.
Katsube T, Saisho Y, Shimada J, Furuie H. Intrapulmonary pharmacokinetics of cefiderocol, a novel siderophore cephalosporin, in healthy adult subjects. J Antimicrob Chemother. 2019;74:1971–4.
Katsube T, Echols R, Arjona Ferreira JC, Krenz HK, Berg JK, Galloway C. Cefiderocol, a siderophore cephalosporin for Gram-negative bacterial infections: pharmacokinetics and safety in subjects with renal impairment. J Clin Pharmacol. 2017;57:584–91.
Miyazaki S, Katsube T, Shen H, Tomek C, Narukawa Y. Metabolism, excretion, and pharmacokinetics of [14 C]-cefiderocol (S-649266), a siderophore cephalosporin, in healthy subjects following intravenous administration. J Clin Pharmacol. 2019;59:958–67.
Fetroja. Cefiderocol for injection for intravenous use. Prescribing Information. Shionogi Inc., Florham Park, NJ 07932, USA. 2021.
Katsube T, Miyazaki S, Narukawa Y, Hernandez-Illas M, Wajima T. Drug-drug interaction of cefiderocol, a siderophore cephalosporin, via human drug transporters. Eur J Clin Pharmacol. 2018;74:931–8.
Fetcroja. Cefiderocol (1 g powder for concentrate for solution for infusion). Summary of Product Characteristics. Shionogi B.V., 151 Kingsfordweg, 1043GR Amsterdam, The Netherlands. 2020.
Llopis B, Bleibtreu A, Jacquet P, Selves A, Rohaut B, Junot H, et al. Pharmacokinetic study of cefiderocol in intensive care unit patients. ECCMID 2020. Abstract 9857. https://www.escmid.org/guidelines_publications/eccmid_2020_abstract_book. Accessed 23 Sep 2022.
König C, Both A, Rohde H, Kluge S, Frey OR, Röhr AC, et al. Cefiderocol in critically ill patients with multi-drug resistant pathogens: real-life data on pharmacokinetics and microbiological surveillance (Erratum in: Antibiotics (Basel). 2021;10:1230). Antibiotics (Basel). 2021;10:649.
Katsube T, Nicolau DP, Rodvold KA, Wunderink RG, Echols R, Matsunaga Y, et al. Intrapulmonary pharmacokinetic profile of cefiderocol in mechanically ventilated patients with pneumonia (Erratum in: J Antimicrob Chemother. 2021; 76:3069). J Antimicrob Chemother. 2021;76:2902–5.
Wenzler E, Butler D, Tan X, Katsube T, Wajima T. Pharmacokinetics, pharmacodynamics, and dose optimization of cefiderocol during continuous renal replacement therapy (Erratum in: Clin Pharmacokinet. 2022;61:1069). Clin Pharmacokinet. 2022;61:539–52.
Wei X, Naseer S, Weinstein EA, Iarikov D, Nambiar S, Reynolds KS, et al. Cefiderocol dosing for patients receiving continuous renal replacement therapy. Clin Pharmacol Ther. 2022;112(5):1004–7. https://doi.org/10.1002/cpt.2703.
Berry AV, Cornelius A, Gluck JA, Nicolau DP, Kuti JL. Cefiderocol is not sequestered in an ex vivo extracorporeal membrane oxygenation (ECMO) circuit. Open Forum Infect Dis. 2022;9(Suppl2): ofac492.652.
Riera J, Domenech L, García S, Pau A, Sosa M, Domenech J, et al. Pharmacokinetics of cefiderocol during extracorporeal membrane oxygenation: a case report. Perfusion. 2023;28:2676591231160462. https://doi.org/10.1177/02676591231160462.
Nakamura R, Ito-Horiyama T, Takemura M, Toba S, Matsumoto S, Ikehara T, et al. In vivo pharmacodynamic study of cefiderocol, a novel parenteral siderophore cephalosporin, in murine thigh and lung infection models. Antimicrob Agents Chemother. 2019;63:e02031-e2118.
Ghazi IM, Monogue ML, Tsuji M, Nicolau DP. Pharmacodynamics of cefiderocol, a novel siderophore cephalosporin, in a Pseudomonas aeruginosa neutropenic murine thigh model. Int J Antimicrob Agents. 2018;51(2):206–12.
Monogue ML, Tsuji M, Yamano Y, Echols R, Nicolau DP. Efficacy of humanized exposures of cefiderocol (S-649266) against a diverse population of Gram-negative bacteria in a murine thigh infection model. Antimicrob Agents Chemother. 2017;61:e01022-e1117.
Stainton SM, Monogue ML, Tsuji M, Yamano Y, Echols R, Nicolau DP. Efficacy of humanized cefiderocol exposures over 72 hours against a diverse group of Gram-negative isolates in the neutropenic murine thigh infection model. Antimicrob Agents Chemother. 2019;63:e01040-e1118.
Gill CM, Abdelraouf K, Oota M, Nakamura R, Kuroiwa M, Ishioka Y, et al. Assessment of sustained efficacy and resistance emergence under human-simulated exposure of cefiderocol against Acinetobacter baumannii using in vitro chemostat and in vivo murine infection models. JAC Antimicrob Resist. 2022;4:dlac047.
Ghazi IM, Monogue ML, Tsuji M, Nicolau DP. Humanized exposures of cefiderocol, a siderophore cephalosporin, display sustained in vivo activity against siderophore-resistant Pseudomonas aeruginosa. Pharmacology. 2018;101:278–84.
Matsumoto S, Singley CM, Hoover J, Nakamura R, Echols R, Rittenhouse S, et al. Efficacy of cefiderocol against carbapenem-resistant Gram-negative bacilli in immunocompetent-rat respiratory tract infection models recreating human plasma pharmacokinetics. Antimicrob Agents Chemother. 2017;61:e00700-e717.
Yamano Y, Takemura M, Anan N, Nakamura R, Echols R. Synergistic effect of cefiderocol with other antibiotics against PER-producing Acinetobacter baumannii isolates from the multinational SIDERO-WT studies. Open Forum Infect Dis. 2020;7(Suppl 1):S805 Poster 1626.
Yamano Y, Ishibashi N, Kuroiwa M, Takemura M, Sheng WH, Hsueh PR. Characterisation of cefiderocol-non-susceptible Acinetobacter baumannii isolates from Taiwan. J Glob Antimicrob Resist. 2022;28:120–4.
Abdul-Mutakabbir JC, Nguyen L, Maassen PT, Stamper KC, Kebriaei R, Kaye KS, et al. In vitro antibacterial activity of cefiderocol against multidrug-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2021;65: e0264620.
Gill CM, Santini D, Takemura M, Longshaw C, Yamano Y, Echols R, et al. In vivo efficacy of human simulated exposures of cefiderocol (FDC) in combination with ceftazidime/avibactam (CZA) or meropenem (MEM) using in a 72 hour murine thigh infection model. Open Forum Infect Dis. 2022;9(Suppl 2): ofac492.661. Poster 609.
Katsube T, Wajima T, Ishibashi T, Arjona Ferreira JC, Echols R. Pharmacokinetic/ pharmacodynamic modeling and simulation of cefiderocol, a parenteral siderophore cephalosporin, for dose adjustment based on renal function. Antimicrob Agents Chemother. 2017;61:e01381-e1416.
Kawaguchi N, Katsube T, Echols R, Wajima T. Population pharmacokinetic and pharmacokinetic/pharmacodynamic analyses of cefiderocol, a parenteral siderophore cephalosporin, in patients with pneumonia, bloodstream infection/sepsis, or complicated urinary tract infection. Antimicrob Agents Chemother. 2021;65:e01437-e1520.
Wunderink RG, Matsunaga Y, Ariyasu M, Clevenbergh P, Echols R, Kaye KS, et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): a randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2021;21:213–25.
Bassetti M, Echols R, Matsunaga Y, Ariyasu M, Doi Y, Ferrer R, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect Dis. 2021;21:226–40.
Katsube T, Echols R, Wajima T. Evaluation of cefiderocol exposure based on pharmacokinetic and pharmacokinetic/pharmacodynamic parameters in critically-ill patients. Presented at: 31st European Congress of Clinical Microbiology & Infectious Diseases (ECCMID); Virtual congress. 9–12 July 2021; Poster 1244.
Katsube T, Kawaguchi N, Matsunaga Y, Ariyasu M, Nagata TD, Portsmouth S, et al. Pharmacokinetic/pharmacodynamic analyses of cefiderocol in critically ill patients. Open Forum Infect Dis. 2020;7(Suppl. 1):S669–70.
Kawaguchi N, Katsube T, Echols R, Wajima T, Nicolau DP. Intrapulmonary pharmacokinetic modeling and simulation of cefiderocol, a parenteral siderophore cephalosporin, in patients with pneumonia and healthy subjects. J Clin Pharmacol. 2022;62:670–80.
Lu J, Liu Q, Kupiec TC, Vail H, Lynch LR, Fam DS, et al. Physical compatibility of cefiderocol with selected intravenous drugs during simulated Y-site administration. Int J Pharm Compd. 2021;25:52–61.
Lynch L, Rathod D, Manrodt R, Chen Z, Fam D, Slover C, et al. Cefiderocol for injection compatibility testing using the MINI-BAG Plus Container System and the VIAL-MATE Adaptor. 2021 ASHP Midyear Congress Virtual Meeting; December 5–9, 2021. Poster 1077024.
Portsmouth S, van Veenhuyzen D, Echols R, Machida M, Ferreira JCA, Ariyasu M, et al. Cefiderocol versus imipenem-cilastatin for the treatment of complicated urinary tract infections caused by Gram-negative uropathogens: a phase 2, randomised, double-blind, non-inferiority trial. Lancet Infect Dis. 2018;18:1319–28.
Bassetti M, Ariyasu M, Binkowitz B, Nagata TD, Echols RM, Matsunaga Y, et al. Designing a pathogen-focused study to address the high unmet medical need represented by carbapenem-resistant Gram-negative pathogens—the international, multicenter, randomized, open-label, phase 3 CREDIBLE-CR study. Infect Drug Resist. 2019;12:3607–23.
O’Donnell JN, Putra V, Lodise TP. Treatment of patients with serious infections due to carbapenem-resistant Acinetobacter baumannii: how viable are the current options? Pharmacotherapy. 2021;41:762–80.
Lodise TP, Bassetti M, Ferrer R, Naas T, Niki Y, Paterson DL, et al. All-cause mortality rates in adults with carbapenem-resistant Gram-negative bacterial infections: a comprehensive review of pathogen-focused, prospective, randomized, interventional clinical studies. Expert Rev Anti Infect Ther. 2022;20:707–19.
Timsit JF, Paul M, Shields RK, Echols R, Baba T, Yamano Y, et al. Cefiderocol for the treatment of infections due to metallo-beta-lactamase-producing pathogens in the CREDIBLE-CR and APEKS-NP phase 3 randomized studies. Clin Infect Dis. 2022;75(6):1081–4. https://doi.org/10.1093/cid/ciac078.
Longshaw C, Roger E, Santerre Henriksen A, Baba T, Nguyen S, Yamano Y. Evidence for efficacy of cefiderocol against OXA-48-containing isolates from the APEKS-NP and CREDIBLE-CR trials. Antimicrob Agents Chemother. 2022;66: e0110022.
Skaar EP, Echols R, Matsunaga Y, Menon A, Portsmouth S. Iron serum levels and iron homeostasis parameters in patients with nosocomial pneumonia treated with cefiderocol: post hoc analysis of the APEKS-NP study. Eur J Clin Microbiol Infect Dis. 2022;41:467–76.
Paterson DL, Kinoshita M, Baba T, Echols R, Portsmouth S. Outcomes with cefiderocol treatment in patients with bacteraemia enrolled into prospective Phase 2 and Phase 3 randomised clinical studies. Infect Dis Ther. 2022;11:853–70.
Matsunaga Y, Sonoyama T, Casanova L, Nagata TD, Echols R, De Gregorio F, Ogura E, Portsmouth S. Safety profile of the novel siderophore cephalosporin cefiderocol in randomized phase 2 and phase 3 clinical studies of serious Gram-negative infections. Open Forum Infect Dis. 2020;7(Suppl 1):S661–2.
Longshaw C, Weiss G, Skaar EP, Zeitlinger M, Baba T, Matsunaga Y, et al. Effects of iron supplementation on the efficacy of cefiderocol in patients with carbapenem-resistant infections in the pathogen-focused CREDIBLE-CR study. Crit Care. 2021;25(Suppl. 1):P124.
Longshaw C, Weiss G, Skaar EP, Zeitlinger M, Baba T, Matsunaga Y, et al. Impact of cefiderocol treatment on iron homeostasis and anaemia in critically ill patients with carbapenem-resistant infections in the CREDIBLE-CR study. Crit Care. 2021;25(Suppl. 1):P123.
Falcone M, Tiseo G, Leonildi A, Della Sala L, Vecchione A, Barnini S, et al. Cefiderocol-compared to colistin-based regimens for the treatment of severe infections caused by carbapenem-resistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2022;66: e0214221.
Pascale R, Pasquini Z, Bartoletti M, Caiazzo L, Fornaro G, Bussini L, et al. Cefiderocol treatment for carbapenem-resistant Acinetobacter baumannii infection in the ICU during the COVID-19 pandemic: a multicentre cohort study. JAC Antimicrob Resist. 2021;3:dlab174.
Rando E, Segala FV, Vargas J, Seguiti C, De Pascale G, Murri R, et al. Cefiderocol for severe carbapenem-resistant A. baumannii pneumonia: towards the comprehension of its place in therapy. Antibiotics (Basel). 2021;11:3.
Meschiari M, Volpi S, Faltoni M, Dolci G, Orlando G, Franceschini E, et al. Real-life experience with compassionate use of cefiderocol for difficult-to-treat resistant Pseudomonas aeruginosa (DTR-P) infections. JAC Antimicrob Resist. 2021;3:dlab188.
Gatti M, Bartoletti M, Cojutti PG, Gaibani P, Conti M, Giannella M, et al. A descriptive case series of pharmacokinetic/pharmacodynamic target attainment and microbiological outcome in critically ill patients with documented severe extensively drug-resistant Acinetobacter baumannii bloodstream infection and/or ventilator-associated pneumonia treated with cefiderocol. J Glob Antimicrob Resist. 2021;27:294–8.
Borghesi L, Viaggi V, Franzetti M, Montoli M, Mauri C, Moioli G, et al. Successful prolonged cefiderocol treatment of a chronic left pleural empyema caused by Pseudomonas aeruginosa in a patient affected by COVID-19: a case report. J Glob Antimicrob Resist. 2021;27:157–9.
Zaidan N, Hornak JP, Reynoso D. Extensively drug-resistant Acinetobacter baumannii nosocomial pneumonia successfully treated with a novel antibiotic combination. Antimicrob Agents Chemother. 2021;65: e0092421.
Kobic E, Gill CM, Mochon AB, Nicolasora NP, Nicolau DP. Cefiderocol pharmacokinetics in a patient receiving continuous venovenous hemodiafiltration. Open Forum Infect Dis. 2021;8:ofab252.
Kobic E, Abouelhassan Y, Singaravelu K, Nicolau DP. Pharmacokinetic analysis and in vitro synergy evaluation of cefiderocol, sulbactam, and tigecycline in an extensively drug-resistant Acinetobacter baumannii pneumonia patient receiving continuous venovenous hemodiafiltration. Open Forum Infect Dis. 2022;9(10):ofac484. https://doi.org/10.1093/ofid/ofac484.
Gavaghan V, Miller JL, Dela-Pena J. Case series of cefiderocol for salvage therapy in carbapenem-resistant Gram-negative infections. Infection. 2023;51(2):475–82. https://doi.org/10.1007/s15010-022-01933-5.
Bleibtreu A, Dortet L, Bonnin RA, Wyplosz B, Sacleux SC, Mihaila L, et al.; The Cefiderocol French Study Group OBO. Susceptibility testing is key for the success of cefiderocol treatment: a retrospective cohort study. Microorganisms. 2021;9:282.
Grande Perez C, Maillart E, Miendje Deyi VY, Huang TD, Kamgang P, Dernier Y, et al. Compassionate use of cefiderocol in a pancreatic abscess and emergence of resistance. Infect Dis Now. 2021;51:399–401.
Oliva A, Ceccarelli G, De Angelis M, Sacco F, Miele MC, Mastroianni CM, et al. Cefiderocol for compassionate use in the treatment of complicated infections caused by extensively and pan-resistant Acinetobacter baumannii. J Glob Antimicrob Resist. 2020;23:292–6.
Falcone M, Tiseo G, Nicastro M, Leonildi A, Vecchione A, Casella C, et al. Cefiderocol as rescue therapy for Acinetobacter baumannii and other Carbapenem-resistant Gram-negative infections in intensive care unit patients. Clin Infect Dis. 2021;72:2021–4.
Gainey AB, Burch AK, Brownstein MJ, Brown DE, Fackler J, Horne B, et al. Combining bacteriophages with cefiderocol and meropenem/vaborbactam to treat a pan-drug resistant Achromobacter species infection in a pediatric cystic fibrosis patient. Pediatr Pulmonol. 2020;55:2990–4.
Kufel WD, Steele JM, Riddell SW, Jones Z, Shakeraneh P, Endy TP. Cefiderocol for treatment of an empyema due to extensively drug-resistant Pseudomonas aeruginosa: clinical observations and susceptibility testing considerations. IDCases. 2020;21: e00863.
Zingg S, Nicoletti GJ, Kuster S, Junker M, Widmer A, Egli A, et al. Cefiderocol for extensively drug-resistant Gram-negative bacterial infections: real-world experience from a case series and review of the literature. Open Forum Infect Dis. 2020;7:ofaa185.
Stevens RW, Clancy M. Compassionate use of cefiderocol in the treatment of an intraabdominal infection due to multidrug-resistant Pseudomonas aeruginosa: a case report. Pharmacotherapy. 2019;39:1113–8.
Contreras DA, Fitzwater SP, Nanayakkara DD, Schaenman J, Aldrovandi GM, Garner OB, et al. Coinfections of two strains of NDM-1- and OXA-232-coproducing Klebsiella pneumoniae in a kidney transplant patient. Antimicrob Agents Chemother. 2020;64:e00948-e1019.
Trecarichi EM, Quirino A, Scaglione V, Longhini F, Garofalo E, Bruni A, et al.; IMAGES Group. Successful treatment with cefiderocol for compassionate use in a critically ill patient with XDR Acinetobacter baumannii and KPC-producing Klebsiella pneumoniae: a case report. J Antimicrob Chemother. 2019;74:3399–401.
Edgeworth JD, Merante D, Patel S, Young C, Jones P, Vithlani S, et al. Compassionate use of cefiderocol as adjunctive treatment of native aortic valve endocarditis due to extremely drug-resistant Pseudomonas aeruginosa. Clin Infect Dis. 2019;68:1932–4.
Bavaro DF, Belati A, Diella L, Stufano M, Romanelli F, Scalone L, et al. Cefiderocol-based combination therapy for “difficult-to-treat” Gram-negative severe infections: real-life case series and future perspectives. Antibiotics (Basel). 2021;10:652.
Fendian ÁM, Albanell-Fernández M, Tuset M, Pitart C, Castro P, Soy D, et al. Real-life data on the effectiveness and safety of cefiderocol in severely infected patients: a case series. Infect Dis Ther. 2023;21:1–12. https://doi.org/10.1007/s40121-023-00776-3.
Mornese Pinna S, Corcione S, De Nicolò A, Montrucchio G, Scabini S, Vita D, et al. Pharmacokinetic of cefiderocol in critically ill patients receiving renal replacement therapy: a case series. Antibiotics (Basel). 2022;11:1830.
La Bella G, Salvato F, Minafra GA, Bottalico IF, Rollo T, Barbera L, et al. Successful treatment of aortic endocarditis by Achromobacter xylosoxidans with cefiderocol combination therapy in a non-Hodgkin lymphoma patient: case report and literature review. Antibiotics (Basel). 2022;11:1686.
Hoellinger B, Simand C, Jeannot K, Garijo C, Cristinar M, Reisz F, et al. Real-world clinical outcome of cefiderocol for treatment of multidrug-resistant non-fermenting, gram negative bacilli infections: a case series. Clin Microbiol Infect. 2023;29:393–5.
Marcella S, Kobic E, Carr AL, Georgiades B, Margiotta C. Outcomes using cefiderocol for the treatment of Acinetobacter baumannii infections from the PROVE (real-world evidence) study. Open Forum Infect Dis. 2022;9(Suppl 2): ofac492.718. Poster 666.
Marcella S, Carr AL, Kobic E, Nguyen S, Zhou A. Real-world experience of cefiderocol with Pseudomonas aeruginosa in the PROVE (retrospective cefiderocol chart review) study. Open Forum Infect Dis. 2022;9(Suppl 2): ofac492.719. Poster 667.
Viale P, Tascini D, Dinh A, Longshaw C, Fitzgerald A, Wood H, et al. Systematic review of the early use experience of cefiderocol in real world practice. Open Forum Infect Dis. 2022;9(Suppl 2): ofac492.729. Poster 1265727.
Klein S, Boutin S, Kocer K, Fiedler MO, Störzinger D, Weigand MA, et al. Rapid development of cefiderocol resistance in carbapenem-resistant Enterobacter cloacae during therapy is associated with heterogeneous mutations in the catecholate siderophore receptor cirA. Clin Infect Dis. 2022;74:905–8.
Simner PJ, Mostafa HH, Bergman Y, Ante M, Tekle T, Adebayo A, et al. Progressive development of cefiderocol resistance in Escherichia coli during therapy is associated with an increase in blaNDM-5 copy number and gene expression. Clin Infect Dis. 2022;75:47–54.
Smoke SM, Brophy A, Reveron S, Iovleva A, Kline EG, Marano M, et al. Evolution and transmission of cefiderocol-resistant Acinetobacter baumannii during an outbreak in the burn intensive care unit. Clin Infect Dis. 2023;76(3):e1261-e1265. https://doi.org/10.1093/cid/ciac647.
Karakonstantis S, Rousaki M, Kritsotakis EI. Cefiderocol: systematic review of mechanisms of resistance, heteroresistance and in vivo emergence of resistance. Antibiotics (Basel). 2022;11:723.
Simner PJ, Beisken S, Bergman Y, Ante M, Posch AE, Tamma PD. Defining baseline mechanisms of cefiderocol resistance in the Enterobacterales. Microb Drug Resist. 2022;28:161–70.
McElheny CL, Fowler EL, Iovleva A, Shields RK, Doi Y. In vitro evolution of cefiderocol resistance in an NDM-producing Klebsiella pneumoniae due to functional loss of cirA. Microbiol Spectr. 2021;9(3): e0177921. https://doi.org/10.1128/Spectrum.01779-21.
Coppi M, Antonelli A, Niccolai C, Bartolini A, Bartolini L, Grazzini M, et al. Nosocomial outbreak by NDM-1-producing Klebsiella pneumoniae highly resistant to cefiderocol, Florence, Italy, August 2021 to June 2022. Euro Surveill. 2022;27:2200795.
Nordmann P, Shields RK, Doi Y, Takemura M, Echols R, Matsunaga Y, et al. Mechanisms of reduced susceptibility to cefiderocol among isolates from the CREDIBLE-CR and APEKS-NP clinical trials. Microb Drug Resist. 2022;28:398–407.
Jousset AB, Poignon C, Yilmaz S, Bleibtreu A, Emeraud C, Girlich D, et al. Rapid selection of a cefiderocol-resistant Escherichia coli producing NDM-5 associated with a single amino acid substitution in the CirA siderophore receptor. J Antimicrob Chemother. 2023;78(4):1125–7.
Karlowsky JA, Walkty AJ, Baxter MR, Adam HJ, Lagacé-Wiens PRS, Schweizer F, et al. In vitro activity of cefiderocol against extensively drug-resistant Pseudomonas aeruginosa: CANWARD, 2007 to 2019. Microbiol Spectr. 2022;10(4): e0172422.
Paul M, Carrara E, Retamar P, Tängdén T, Bitterman R, Bonomo RA, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European Society of Intensive Care Medicine). Clin Microbiol Infect. 2022;28:521–47.
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2022 guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75:187–212.
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America guidance on the treatment of ampc β-lactamase-producing Enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clin Infect Dis. 2022;74:2089–114.
Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused at creating algorithms for targeted therapy of infection-related ventilator associated complications (IVACs) caused by Enterobacterales in critically ill adult patients. Expert Rev Anti Infect Ther. 2022;20:331–52.
Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused at creating algorithms for targeted therapy of BSIs, cUTIs, and cIAIs caused by Enterobacterales in critically ill adult patients. Infect Drug Resist. 2021;14:2461–98.
Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused on creating algorithms for targeted therapy of infection-related ventilator-associated complications (IVACs) caused by Pseudomonas aeruginosa and Acinetobacter baumannii in critically ill adult patients. Antibiotics (Basel). 2022;11:33.
Bassetti M, Vena A, Giacobbe DR, Castaldo N. Management of infections caused by multidrug-resistant Gram-negative pathogens: recent advances and future directions. Arch Med Res. 2021;52:817–27.
Cillóniz C, Dominedò C, Torres A. An overview of guidelines for the management of hospital-acquired and ventilator-associated pneumonia caused by multidrug-resistant Gram-negative bacteria. Curr Opin Infect Dis. 2019;32:656–62.
Zaragoza R, Vidal-Cortés P, Aguilar G, Borges M, Diaz E, Ferrer R, et al. Update of the treatment of nosocomial pneumonia in the ICU. Crit Care. 2020;24:383.
Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61–e111. Erratum in: Clin Infect Dis. 2017;64:1298. Erratum in: Clin Infect Dis. 2017;65:1435.
Bouglé A, Tuffet S, Federici L, Leone M, Monsel A, Dessalle T, et al; iDIAPASON Trial Investigators. Comparison of 8 versus 15 days of antibiotic therapy for Pseudomonas aeruginosa ventilator-associated pneumonia in adults: a randomized, controlled, open-label trial. Intensive Care Med. 2022;48:841–9.
Daghmouri MA, Dudoignon E, Chaouch MA, Baekgaard J, Bougle A, Leone M, et al. Comparison of a short versus long-course antibiotic therapy for ventilator-associated pneumonia: a systematic review and meta-analysis of randomized controlled trials. EClinicalMedicine. 2023;58: 101880.
McCrink KA, DeRonde KJ, Jimenez A, Rosello G, Natori Y, Claeys KC, et al. Impact of a real-time diagnostic and antimicrobial stewardship workflow on time-to-appropriate therapy for infections caused by multidrug-resistant Gram-negative organisms. Int J Antimicrob Agents. 2023;61(6):106811. https://doi.org/10.1016/j.ijantimicag.2023.106811.
Abdul-Aziz MH, Alffenaar JC, Bassetti M, Bracht H, Dimopoulos G, Marriott D, et al.; Infection Section of European Society of Intensive Care Medicine (ESICM); Pharmacokinetic/pharmacodynamic and Critically Ill Patient Study Groups of European Society of Clinical Microbiology and Infectious Diseases (ESCMID); Infectious Diseases Group of International Association of Therapeutic Drug Monitoring and Clinical Toxicology (IATDMCT); Infections in the ICU and Sepsis Working Group of International Society of Antimicrobial Chemotherapy (ISAC). Antimicrobial therapeutic drug monitoring in critically ill adult patients: a Position Paper. Intensive Care Med. 2020;46:1127–53.
Abdulla A, Dijkstra A, Hunfeld NGM, Endeman H, Bahmany S, Ewoldt TMJ, et al. Failure of target attainment of beta-lactam antibiotics in critically ill patients and associated risk factors: a two-center prospective study (EXPAT). Crit Care. 2020;24:558.
Barreto EF, Webb AJ, Pais GM, Rule AD, Jannetto PJ, Scheetz MH. Setting the beta-lactam therapeutic range for critically ill patients: is there a floor or even a ceiling? Crit Care Explor. 2021;3: e0446.
Dilworth TJ, Schulz LT, Micek ST, Kollef MH, Rose WE. β-lactam therapeutic drug monitoring in critically ill patients: weighing the challenges and opportunities to assess clinical value. Crit Care Explor. 2022;4: e0726.
Wright H, Harris PNA, Chatfield MD, Lye D, Henderson A, Harris-Brown T, et al. Investigator-driven randomised controlled trial of cefiderocol versus standard therapy for healthcare-associated and hospital-acquired Gram-negative bloodstream infection: study protocol (the GAME CHANGER trial): study protocol for an open-label, randomised controlled trial. Trials. 2021;22:889.
Oota M, Hama H, Yoshitomi T, Nakamura R, Takemura M, Yamano Y, et al. In vitro and in vivo antibacterial activity of cefiderocol against Burkholderia spp. Open Forum Infect Dis. 2021;8(Suppl. 1):S621.
Avycaz (ceftazidime-avibactam for injection for intravenous use). Prescribing Information. Allergan USA, Inc., Madison, NJ 07940, USA. 2020.
Zavicefta. Ceftazidime-avibactam (2 g/0.5 g powder for concentrate for solution for infusion). Summary of Product Characteristics. Pfizer Ireland Pharmaceuticals Operations Support Group. Ringaskiddy, County Cork, Ireland. 2021.
Zerbaxa. Ceftolozane-tazobactam for injection for intravenous use. Prescribing Information. Merck & Co., Inc. Whitehouse Stations, NJ 08889, USA. 2020.
Zerbaxa. Ceftolozane-tazobactam (1 g/0.5 g powder for solution for infusion). Summary of Product Characteristics. Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, The Netherlands. 2020.
Recarbrio (imipenem-cilastatin-relebactam for injection for intravenous use). Prescribing Information. Merck & Co., Inc. Whitehouse Station, NJ 08889, USA. 2020.
Recarbrio. Imipenem-cilastatin-relebactam (500 mg/500 mg/250 mg powder for solution for infusion). Summary of Product Characteristics. Merck Sharp & Dohme B.V. Waarderweg 39, 2031 BN Haarlem, The Netherlands. 2020.
Vabomere (meropenem and vaborbactam for injection, for intravenous use). Prescribing Information. Melinta Therapeutics, LLC, Lincolnshire, IL 60069, USA. 2020.
Vaborem (meropenem/vaborbactam 1 g/1 g powder for concentrate for solution for infusion). Summary of Product Characteristics. Menarini International Operations Luxembourg S.A.; 1 Avenue de la Gare, L-1611, Luxembourg. 2021.
Acknowledgements
Editorial and medical writing support was provided by Adrienn Kis, PhD, and Joanne Shrewsbury-Gee, PhD, Highfield, Oxford, UK, and this support was funded by Shionogi & Co., Ltd., Osaka, Japan. Shionogi reviewed this manuscript from a medical, legal, and regulatory perspective.
Funding
The open access for this manuscript was funded by Shionogi & Co., Ltd., Osaka, Japan.
Author information
Authors and Affiliations
Contributions
All authors participated in the conception, drafting and revisions of the manuscript, and read and approved the final version for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
PLV has no conflict of interest. CES has received consultancy fees from Shionogi, Paratek, Abbvie, Pfizer. He is on the speaker bureau for Shionogi, Abbvie, Paratek, Merck. He has been involved in clinical trials from Pleurostem, Jansen, Pfizer, Merck, and Abbive. PR has no conflict of interest. GMR has received consultancy fees from Menarini, MSD, Pfizer, and Zambon. He has participated in speakers’ bureau for Angelini, Menarini, MSD, Pfizer, and Shionogi. GMR has also received grant support for laboratory work from Angelini, Menarini, MSD, Nordic Pharma, Shionogi, VenatorX, and Zambon, all outside of the submitted work. TPL has received consultancy fees from AbbVie, Cidara, Ferring, Genentech, IPCD, Johnson and Johnson, Melinta, Merck, Paratek, Roche, Shionogi, Spero, and VenatorX. He has received grants or research support from BioFire Diagnostics, Entasis, Merck, and Wockhardt. He has participated in speakers’ bureau for Ferring and Shionogi.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Summary of randomized clinical trial evidence for cefiderocol in the APEKS–cUTI, APEKS–NP and CREDIBLE–CR studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Viale, P., Sandrock, C.E., Ramirez, P. et al. Treatment of critically ill patients with cefiderocol for infections caused by multidrug-resistant pathogens: review of the evidence. Ann. Intensive Care 13, 52 (2023). https://doi.org/10.1186/s13613-023-01146-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-023-01146-5